Health-related quality of life in patients with vestibular schwannoma managed with observation, stereotactic radiosurgery or microsurgery: a systematic review and single-arm meta-analysis
Ineke M. J. Pruijn, Frédérique R. L. M. Welie, Wietske Kievit, Henricus P. M. Kunst

TL;DR
This study compares the quality of life for patients with vestibular schwannoma treated with observation, radiosurgery, or surgery, finding no clinically meaningful differences between the approaches.
Contribution
The study provides the first meta-analysis comparing HRQoL outcomes across three major treatment strategies for vestibular schwannoma using the PANQOL questionnaire.
Findings
Pooled PANQOL scores for observation, radiosurgery, and surgery showed no clinically meaningful differences.
Hearing and energy domains had the lowest scores, while facial function and anxiety had the highest.
Substantial heterogeneity across studies suggests a need for standardized, prospective research.
Abstract
Health-related quality of life (HRQoL) is a key outcome in the management of vestibular schwannoma (VS). Although wait-and-scan (W&S), stereotactic radiosurgery (SRS), and microsurgery (MS) are established management strategies, their comparative effects on HRQoL remain unclear. This systematic review and meta-analysis aimed to synthesize HRQoL outcomes using the Penn Acoustic Neuroma Quality of Life (PANQOL) questionnaire and to pool PANQOL scores for W&S, SRS, and MS. A systematic search of PubMed and Embase was conducted up to February 2025. Eligible studies included patients with unilateral sporadic VS managed with W&S, SRS, or MS, with HRQoL assessed by PANQOL at least one year after diagnosis or intervention. Pooled mean PANQOL scores were calculated using single-arm meta-analyses. Minimal clinically important differences (MCIDs) were applied to assess relevance. 16 studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
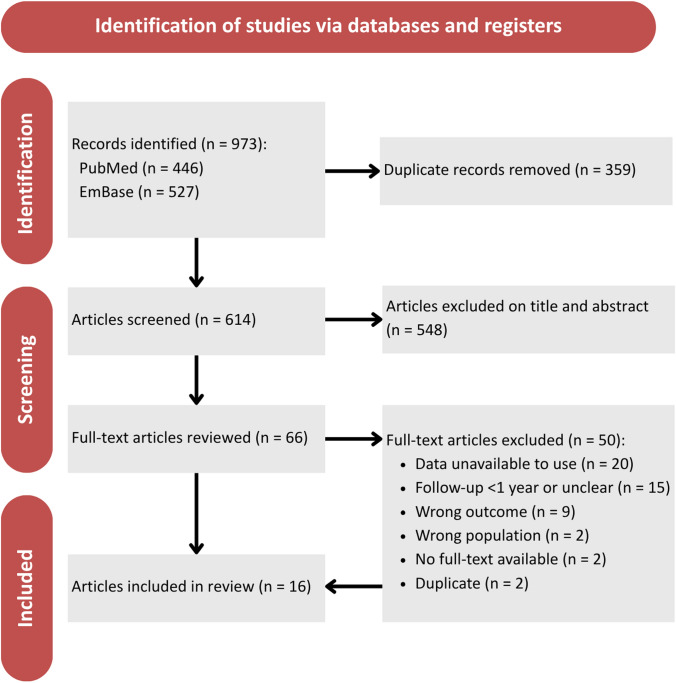 Figure 1
Figure 1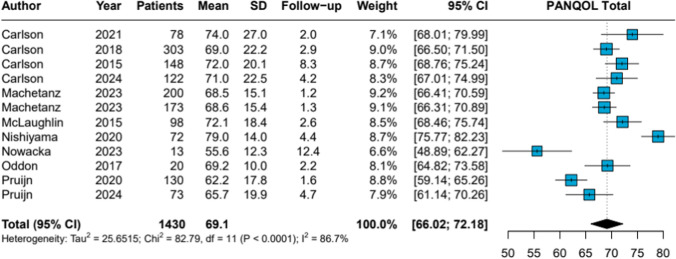 Figure 2
Figure 2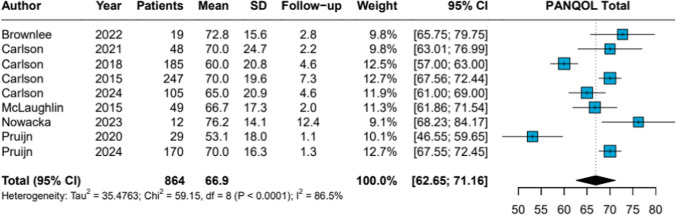 Figure 3
Figure 3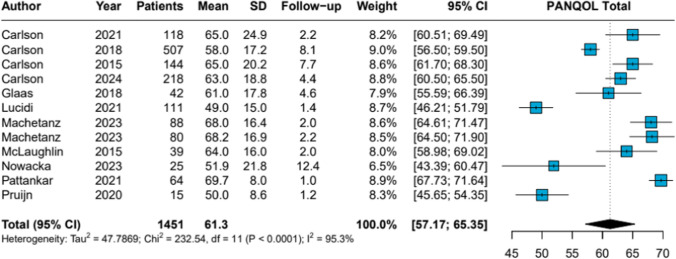 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Vestibular and auditory disorders · Trigeminal Neuralgia and Treatments
Introduction
Quality of life (QoL) has gained an increasing importance in the field of vestibular schwannoma (VS), and as such, has become of paramount importance in the decision-making and evaluation of management strategies. Vestibular schwannomas are the most prevalent tumors in the cerebellopontine angle with an incidence rate of 34 VS/million/year [1]. Patients may be faced with unilateral hearing loss, tinnitus, and balance problems resulting from VS [2]. However, the majority of patients may also suffer from fatigue, lack of energy, anxiety, dizziness, or headaches [2–5]. Both these disease-specific and more general symptoms, either caused by the vestibular schwannoma or initiated management, result in limitations and restrictions in daily life activities and societal participation. This ultimately leads to a deterioration of the health-related quality of life (HRQoL).
Management strategies for VS include a conservative wait-and-scan (W&S) strategy with serial imaging and regular follow-up, or active treatment with either stereotactic radiosurgery (SRS) or microsurgery (MS). Given the benign nature of VS and the generally small- to medium-sized tumors at presentation, there has been increasing attention to management-related morbidity, prompting several studies evaluating the impact of different treatment modalities on HRQoL. However, research in this area has been heterogeneous and sometimes contradictory, with studies drawing differing conclusions on the effects of the same management strategy [6–13].
To provide an overall assessment of management impact on QoL, Gauden et al. [14] published a systematic review in 2011, concluding that methodological limitations—including study design and small sample sizes—precluded firm conclusions. At that time, HRQoL in VS patients was primarily assessed using generic instruments, such as the 36-item Short Form Questionnaire (SF-36) and the Glasgow Benefit Inventory (GBI). In 2010, the disease-specific Penn Acoustic Neuroma Quality of Life (PANQOL) questionnaire was introduced [15], providing a more targeted assessment of patient-reported outcomes. The PANQOL captures the unique functional and psychosocial challenges faced by VS patients—including hearing, balance, facial function, and anxiety—and is more sensitive to clinically meaningful changes than generic instruments. Using the PANQOL, studies can ensure consistency in outcome measurement, enhance comparability across treatment modalities, and allow for more precise evaluation of management-related HRQoL effects.
Building on this methodological advancement, Papatsoutsos et al. [16] published an updated systematic review in 2018, extending the work of Gauden et al. [14], summarizing the literature on the impact of management strategies on HRQoL up to 2016. Their findings indicated that VS diagnosis itself was associated with reduced HRQoL, which further deteriorated after microsurgery and stereotactic radiotherapy [16].
It is important to recognize, however, that the previous evaluations have some limitations. While in the time of Gauden et al. there were no studies yet evaluating HRQoL with the disease-specific PANQOL, Papatsoutos et al. searched the literature up to 2016, missing out on the long-term evaluations of HRQoL using the PANQOL. Additionally, their systematic review included studies that reported changes in HRQoL either through visual indicators (e.g., directional arrows in figures) or numerical values, without providing the original baseline or follow-up measurements [17]. Moreover, several studies on HRQoL were conducted in highly specific patient groups [18, 19], making a comparison of treatment strategies and the generalizability problematic.
Though research on HRQoL and patient-reported outcomes evaluating treatments in patients with VS has taken flight in the past years, the question remains which management modality preserves the highest HRQoL [20]. To aid patient counseling, enhance shared decision-making and evaluation of HRQoL outcomes, the main objective of this systematic review and meta-analysis was to pool PANQOL HRQoL outcomes in patients with VS managed with W&S, SRS or MS and secondary to compare and evaluate the differences.
Materials and methods
This systematic review was performed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and registered at the International Prospective Register of Systematic Reviews (PROSPERO) under number CRD420250651347.
Search strategy
A systematic search of literature in PubMed and Embase was conducted up to February 10, 2025. The search was performed with a restriction on publication date including studies from 2010 onwards as the PANQOL was introduced by Shaffer et al. in 2010. A librarian assisted in drafting and pretesting the search strategy in PubMed which was adapted to the other database. The search strategy comprised the key elements “vestibular schwannoma” or “acoustic neuroma” and equivalents combined with “health-related quality of life” or “quality of life” or “PANQOL” or synonyms. Reference lists of eligible studies were reviewed for potential inclusion. Appendix 1 lists the full electronic search strategy.
Eligibility criteria
We included all original, peer-reviewed studies evaluating at least one management strategy (W&S, SRS or MS) in patients with unilateral sporadic VS, either as investigated population or subpopulation reporting on PANQOL scores as an outcome (total and domain scores). The majority of the patients had to be evaluated with a per protocol analysis. Follow-up time had to be at least one year after diagnosis for W&S management and at least one year after SRS or MS treatment. Articles needed to have full-text availability and be written in English or Dutch. Exclusion criteria were inclusion of patients with neurofibromatosis type II, inclusion of patients with salvage treatment or a combination of treatments, literature or systematic reviews, meta-analyses, case reports, comments, letters to the editor and books. Studies from which the PANQOL data were not extractable from text, tables or supplementary files were also excluded.
Study selection
Two reviewers (IP and FW) independently screened all titles and abstracts for eligibility using the Rayyan platform [21]. Discordance was reconciled with mutual agreement or, if necessary, discussed with a third reviewer (HK) until consensus was reached. The same reviewers (IP and FW) independently assessed all eligible full texts for inclusion and excluded studies with reason, with disagreements resolved by consensus. In cases where multiple studies originated from the same research group and described overlapping patient populations, the publication with the highest number of patients was included.
Outcome
The primary outcome measure was the PANQOL total score for each management strategy. Secondary outcome measures included the PANQOL subdomain scores for Anxiety, Balance, Energy, Face, General, Hearing, and Pain. The PANQOL consists of 26 items across these seven domains, each scored on a 0–100 scale, with higher scores indicating better HRQoL. The PANQOL total score represents the mean of the seven subdomain scores and similarly ranges from 0 to 100. Although the PANQOL was developed as a disease-specific instrument for patients with vestibular schwannoma (VS), data from a Dutch reference sample without VS demonstrated a mean total score of 81.8 (SD 12.6), reflecting that even individuals without VS may experience mild hearing loss, tinnitus, or balance issues [4]. Outcomes were interpreted using the minimal clinically important differences (MCID) defined as the smallest change in a patient-reported outcome that patients perceive as meaningful and clinically relevant [22]. For the PANQOL, established MCID thresholds are 12.5 for the total score, 16.4 for Anxiety, 14 for Balance, 16 for Energy, 25 for Face, 12.9 for General, 13.1 for Hearing, and 20.6 for Pain [22]. These thresholds facilitate the distinction between statistically significant changes and those that are clinically meaningful from the patient’s perspective.
Data extraction
For each management strategy, main study characteristics were extracted from each article on first author, year of publication, country of study conduction, study design, study period, number of patients, tumor size, mean follow-up time, and type of SRS or MS. Additionally, the PANQOL outcomes (means and standard deviations) were extracted from the data. Attempts were made to contact corresponding authors of included studies to obtain essential data. There was no imputation for missing data. Means and standard deviations were calculated from medians and interquartile ranges if necessary, and pooled means and standard deviations were calculated if there were no combined outcomes available in subgroup analysis i.e., separate reporting on men vs. women [23].
Quality assessment
All included studies were either single-arm or nonrandomized comparative designs. Therefore, a critical appraisal was conducted using the Risk Of Bias In Nonrandomized Studies—of Interventions (ROBINS-I) assessment tool. This assessment evaluated seven domains: bias due to confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported results. The overall risk of bias was rated as high when these domains were not adequately addressed or reported, and low when sufficient methodological detail was provided. No studies were excluded based on the results of this appraisal.
Statistical analysis
Pooled results on PANQOL total score and PANQOL domain scores per treatment strategy are shown in a single-arm meta-analysis using forest plots with means and confidence intervals. The proportion of variation across studies owing to heterogeneity rather than chance was assessed with the I^2^ statistic. Statistical analysis was performed with R version 4.3.1 (R Foundation for Statistical Computing).
Results
Study selection
The systematic search strategy identified 973 potentially eligible records. After removal of duplicates, 614 unique articles were screened based on title and abstract. Of these, 66 articles were selected for full-text review, ultimately resulting in the inclusion of 16 studies. [4, 6, 13, 24–36]. A manual search of the reference lists of included studies did not identify any additional eligible publications.
All included studies were either single-arm or nonrandomized comparative designs, which is why a single-arm meta-analysis was performed for each management strategy, enabling pooling of treatment-specific outcomes without relying on assumptions required for indirect comparisons. Two studies were identified with overlapping patient populations, identical follow-up and PANQOL outcomes. Although the most recent publication by Link et al. appeared in 2018 [37], the earlier study by Carlson et al. (2015) [6] included one additional patient in the MS 20–30 mm CPA group (n = 144 vs. n = 143). For this reason, Carlson et al. [6] was included in the single-arm meta-analysis, while Link et al. was excluded [37]. The study selection process is summarized in the PRISMA flow diagram (Fig. 1). Detailed study characteristics and outcome data are provided in Appendix 3 and Appendix 4.Fig. 1PRISMA flow chart
Risk of bias
Of the 16 included studies, 9 studies were categorized as having a moderate risk of bias [4, 6, 13, 25–27, 32, 34, 36] and 7 studies were deemed at serious risk of bias [24, 28–31, 33, 35], primarily due to concerns with missing data and selection of reported results. No studies were excluded based on their bias assessment. See Appendix 2 for the detailed bias assessment.
Wait-and-scan
12 predominantly cross-sectional studies were included in the single-arm meta-analysis for the W&S strategy. Study characteristics are summarized in Appendix 3. In total, PANQOL data from 1430 patients were pooled, with sample sizes ranging from 13 to 303 participants per study. The mean time from diagnosis to PANQOL assessment ranged between 1.28 and 12.4 years. Tumor size was reported either in centimeters [6, 25–27], or using the Koos classification system [4, 30–32, 36]. Overall, most tumors were smaller than 20 mm or classified as Koos grades I–III.
The meta-analysis yielded a pooled PANQOL total score of 69.1 (95% CI 66.02–72.18), accompanied by high heterogeneity (I^2^ = 86.7%, p < 0.0001). The corresponding forest plot is presented in Fig. 2. Pooled subdomain scores were: Anxiety 73.0, Balance 70.0, Energy 67.4, Face 85.8, General 59.2, Hearing 56.2, and Pain 74.5 (Table 1; Forest plots PANQOL subdomain scores in Appendix 5).Fig. 2. Wait-and-Scan Forest Plot PANQOL TotalTable 1Mean PANQOL scores from single-arm meta-analysisW&SSRSMSW&S vs. SRSW&S vs. MSSRS vs. MSMCIDPANQOL anxiety73.073.969.1− 0.93.94.816.4PANQOL balance70.061.058.29.011.82.814.0PANQOL energy67.460.758.16.79.32.616.0PANQOL face85.883.570.62.315.212.925.0PANQOL general59.259.862.3− 0.6− 3.1− 2.512.9PANQOL hearing56.248.950.47.35.8− 1.513.1PANQOL pain74.572.662.01.912.510.620.6PANQOL total69.166.961.32.27.85.612.5
Stereotactic radiosurgery
Nine studies were included in the single-arm meta-analysis of SRS, originating from Ireland [24], the USA [6, 13, 25–27], New Zealand [33], and the Netherlands [4, 36]. Sample sizes ranged from 12 to 247 patients, resulting in a total of 864 individuals. Mean follow-up durations varied from 1.1 to 12.4 years. Tumor sizes ranged from a few millimeters to ≥ 40 mm, corresponding to Koos grades I through IV. The most common type of SRS was the Gamma Knife in five out of nine studies [4, 13, 24, 26, 36]. The other four did not report on the type of SRS.
The pooled PANQOL total score following SRS was 66.9 (95% CI 62.65–71.16), with high heterogeneity (I^2^ = 86.5%, p < 0.0001) (Fig. 3). Pooled subdomain scores were: Anxiety 73.9, Balance 61.0, Energy 60.7, Face 83.5, General 59.8, Hearing 48.9, and Pain 72.6 (Table 1; Forest plots PANQOL subdomain scores in Appendix 6).Fig. 3. Stereotactic Radiosurgery Forest Plot PANQOL Total
Microsurgery
12 studies were included in the single-arm meta-analysis of microsurgical treatment, encompassing 1451 patients. Most underwent treatment using the retrosigmoid approach, which enables hearing preservation [4, 26, 29–31, 35]. PANQOL outcomes were assessed after a mean follow-up ranging from 1 to 12.4 years. Sample sizes varied from 15 to 507 participants per study. Tumor size distribution is detailed in Appendix 3; however, the majority of patients underwent microsurgery for tumors measuring 10–30 mm or classified as Koos grades III–IV.
The pooled PANQOL total score for microsurgical treatment was 61.3 (95% CI 57.17–65.35), with high heterogeneity (I^2^ = 95.3%, p < 0.0001) (Fig. 4). Pooled subdomain scores were: Anxiety 69.1, Balance 58.2, Energy 58.1, Face 70.6, General 62.3, Hearing 50.4, and Pain 62.0 (Table 1; Forest plots PANQOL subdomain scores in Appendix 7).Fig. 4MMicrosurgery Forest Plot PANQOL Total
No pooled PANQOL total or subdomain score differences between the three management strategies (W&S vs. SRS, W&S vs. MS, or SRS vs. MS) exceeded the MCID (Table 1).
Discussion
This systematic review and single-arm meta-analysis pooled PANQOL HRQoL scores for patients with unilateral VS managed with W&S, SRS or MS. Overall, patients managed with W&S had a pooled PANQOL total score of 69.1, those managed with SRS scored 66.9, and patients undergoing MS had a pooled PANQOL total score of 61.3. Importantly, differences in total and subdomain PANQOL scores across W&S, SRS, and MS did not exceed the established MCIDs, indicating no clinically meaningful differences in HRQoL and suggesting that outcomes are broadly comparable across treatment modalities.
However, these findings should be considered in the wider context of tumor management and clinical decision-making, where HRQoL outcomes are only one of several important factors. At first glance, it may appear counterintuitive that W&S yields HRQoL outcomes comparable to those of active interventions, such as SRS and MS. However, this should not be interpreted as a lack of therapeutic benefit of active treatment. PANQOL primarily captures symptom burden and functional impact rather than tumor control. Moreover, treatment decisions should not be based solely on HRQoL scores; rather, they must integrate the effectiveness of each management strategy in terms of tumor control, the risks associated with each treatment, including the risk of mortality, treatment-related morbidities, and the potential long-term impact on HRQoL. A comprehensive evaluation of these factors is essential to ensure that patients receive the most appropriate care. Given the complexity inherent in these decisions, shared decision-making is crucial. Clinicians must engage in thorough, transparent, and individualized counseling with patients, providing them with a clear understanding of the potential benefits and risks of each treatment option. This collaborative process is vital for aligning treatment decisions with the patient’s values, preferences, and clinical circumstances, thereby optimizing the selection of the most suitable therapeutic approach.
Nevertheless, the interpretation of pooled PANQOL scores requires caution, given the substantial heterogeneity observed across studies, with I^2^ values exceeding 75% in all analyses. This heterogeneity is likely explained by several factors. First, many included studies had a cross-sectional or retrospective design, often lacking power calculations, and failing to report the timing or rationale for initiating treatment. These designs also precluded baseline PANQOL scores and the opportunity to evaluate the change in PANQOL scores during follow-up following W&S, SRS, or MS. Second, variability in patient populations—including tumor size, Koos classification, age, comorbidities, and overall health status—and reporting those may have affected both baseline HRQoL and the impact of treatment. Third, patient and clinician preferences, as well as geographic differences in treatment approaches, likely influenced management choice and outcomes [38]. Finally, differences in response rates, influenced by whether questionnaires were administered in-hospital, online, or via post, may have introduced further variability in reported outcomes [39, 40].
Taken together, these sources of heterogeneity highlight the challenges of synthesizing HRQoL outcomes across diverse study designs and populations. Despite this heterogeneity, pooling of PANQOL scores was methodologically warranted using a random-effects model, which accounts for both within- and between-study variability. This approach allows synthesis of treatment-specific PANQOL outcomes, integrating variability in patient populations, tumor characteristics, and management delivery—including surgical approach, radiosurgery protocols, and follow-up schedules—thereby providing pooled estimates that meaningfully reflect the impact of each management strategy on HRQoL despite the observed heterogeneity.
In addition to this variability within the included literature, several methodological considerations also limited the number of studies eligible for inclusion in the meta-analysis. The V-REX study [41], for example, which is a RCT, was excluded because it used an intention-to-treat (ITT) analysis, which is particularly useful in reflecting real-world clinical scenarios. In clinical practice, patients often switch between treatments or discontinue their assigned therapy, and ITT analysis captures this variability by including all patients as initially assigned, regardless of whether they complete the treatment as planned. This allows for a more realistic estimate of the overall effectiveness of the treatments. However, in the context of this meta-analysis, we sought to isolate the effects of the treatments as per protocol, to better understand the specific outcomes of each treatment modality, and to minimize confounding from therapy switching or discontinuation. As nearly half of the patients in the V-REX study (44%) switched from W&S to active treatment, the HRQoL results were difficult to interpret in the context of actual management strategies when viewed through the lens of ITT. Furthermore, multiple studies with larger cohorts and longer follow-up periods could not be included because they did not report, but only visualized, PANQOL scores, and attempts to obtain these data from the authors were unsuccessful. Studies that lacked measures of variability (SD, IQR) or reported PANQOL outcomes stratified according to other factors (for example, hearing) were similarly excluded, further reducing the available evidence base.
A further limitation of the included studies is the absence of PANQOL baseline scores, precluding meaningful assessment of within-group changes in HRQoL over time for each management strategy. Without baseline measurements, it remains unclear whether reported follow-up scores reflect true stability, improvement, or deterioration relative to pretreatment status. In addition, limited reporting on patients lost to follow-up—particularly the reasons for non-response—raises concerns about attrition bias. In patients who may experience greater morbidity as a result of their VS or treatment modality, HRQoL may be more severely impacted, potentially leading to non-completion of questionnaires. Therefore, these patients, who may represent the most clinically relevant cases, are often underrepresented in the final HRQoL scores. This could introduce bias and limit the generalizability of the findings.
Beyond these practical exclusions, there remains a more fundamental question regarding the ability of the current PANQOL instrument to capture true differences between management strategies. One could argue whether there actually are differences to be measured between management strategies, given that pooled PANQOL HRQoL scores show only small variations that do not exceed the MCID. This raises the question whether these differences are truly negligible or simply not captured due to limitations in the PANQOL instrument. The PANQOL equally weights all seven domains in calculating the total score, despite evidence that certain domains—such as energy, anxiety, pain, and balance—contribute more strongly to overall HRQoL than others like hearing or tinnitus [3, 4]. This uniform weighting may obscure clinically meaningful differences between patient groups or treatment modalities. The recently developed Vestibular Schwannoma Quality of Life (VSQOL) index [42], which includes additional domains, such as cognitive function, treatment satisfaction, and broader pain assessment, has been designed to capture a more comprehensive and nuanced view of HRQoL. Given its enhanced sensitivity and psychometric robustness, the VSQOL may be better suited to detect (subtle) clinically relevant differences in patient-reported outcomes that the PANQOL cannot fully reveal. Future studies employing the VSQOL could therefore determine whether subtle but clinically relevant differences exist between treatment strategies, ultimately supporting more informed, patient-centered decision-making.
This naturally leads to the broader issue of how the field can generate higher-level evidence in future. Ultimately, the highest level of evidence regarding HRQoL outcomes in patients with vestibular schwannoma would be obtained from meta-analyses of RCTs or rigorously controlled cohort studies directly comparing management strategies. However, such studies are exceedingly scarce, reflecting both ethical and practical challenges in randomizing patients to distinct treatment modalities in this population. An alternative approach could be a network meta-analysis, in which studies comparing different pairs of interventions—for example, W&S versus SRS and SRS versus MS—are synthesized to enable indirect comparisons across all three strategies. While this method has theoretical appeal, its validity depends on sufficient overlap in baseline patient, tumor and HRQoL characteristics across studies to satisfy the transitivity assumption. Moreover, network meta-analysis fundamentally relies on randomized comparative trials using a common comparator to construct the network, as randomization ensures that patients with similar baseline characteristics could theoretically have been allocated to any treatment arm across studies. Observational studies, including matched cohort designs, do not fully satisfy this assumption and therefore may introduce residual confounding if incorporated into the network. In the context of VS HRQoL research, such comparability is generally lacking, hence the high heterogeneity in this meta-analysis, limiting the interpretability of indirect comparisons. Given these constraints, single-arm meta-analyses remain the most feasible and methodologically defensible approach to synthesize existing data, providing valuable insights into patient-reported outcomes across treatment modalities while transparently acknowledging the limitations imposed by heterogeneity and study design.
Looking forward, strengthening the evidence base will require coordinated efforts to enhance data quality and comparability across studies. Future research should prioritize standardized collection and reporting of HRQoL outcomes, including the consistent use of validated instruments such as the PANQOL or VSQOL at baseline and during follow-up, complete reporting of measures of variability, and stratification according to clinically relevant factors, such as tumor size, treatment indication, and baseline patient, tumor, and HRQoL characteristics. Establishing a national database and fostering international collaboration would facilitate larger and more representative datasets. This, in turn, would enable individual patient data (IPD) meta-analyses, which are widely considered the most methodologically rigorous approach to evidence synthesis. By allowing direct access to raw, patient-level data across centers, IPD meta-analyses enable uniform data harmonization, adjustment for confounding variables, and exploration of subgroup effects that are not possible with aggregate data alone. Such an approach would substantially improve the validity and interpretability of comparative effectiveness research in vestibular schwannoma. Ultimately, the goal of these efforts is to generate high-quality, generalizable evidence that informs shared decision-making, helping patients to weigh the potential impact of different management strategies on their quality of life and to select the treatment that best aligns with their individual preferences and clinical circumstances.
Conclusion
In summary, this systematic review and single-arm meta-analysis demonstrates that patients with unilateral VS managed with W&S, SRS, or MS report broadly comparable HRQoL outcomes, with differences in pooled PANQOL scores not exceeding the corresponding MCIDs. These findings suggest that, from a HRQoL perspective, no management strategy confers a clear advantage over the others. However, these findings should be considered in the wider context of tumor management and clinical decision-making, where HRQoL outcomes are only one of several important factors. Nevertheless, substantial heterogeneity, methodological limitations, and incomplete reporting highlight the need for more rigorous and standardized research. Establishing national databases and fostering international collaboration will be essential to generate sufficiently large and representative datasets, enabling more robust analyses and subgroup explorations. Ultimately, the overarching aim of such efforts is to provide high-quality, generalizable evidence that can support patients and clinicians in making well-informed, individualized treatment decisions.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 14 kb)Supplementary file2 (DOCX 18 kb)Supplementary file3 (DOCX 33 kb)Supplementary file4 (DOCX 42 kb)Supplementary file5 (PDF 186 kb)Supplementary file6 (PDF 102 kb)Supplementary file7 (PDF 140 kb)