Self‐Reported Dysmenorrhea Among Adolescent Girls in the Cape Coast Metropolis: A Cross‐Sectional Study
Amina S. Abugri, Attoh Tetteh, Gabriel P. Kotam, Angele Comlan‐Cataria, Stephen Ocansey, Richard K. D. Ephraim

TL;DR
This study finds that most adolescent girls in Cape Coast, Ghana, experience painful periods, which affects their schoolwork and social life.
Contribution
The study provides new insights into dysmenorrhea prevalence and coping strategies among Ghanaian adolescent girls.
Findings
86.9% of adolescent girls reported experiencing dysmenorrhea.
Dysmenorrhea led to poor concentration, social withdrawal, and absenteeism.
Early menarche was associated with lower odds of severe dysmenorrhea.
Abstract
Dysmenorrhea is a common gynaecological condition among female adolescents and affects students' well‐being in Ghana. This study assessed dysmenorrhea prevalence, effects, and coping mechanisms among adolescent girls in Junior High Schools in the Cape Coast metropolis. A cross‐sectional study was conducted among adolescent girls in three Junior High Schools in the Cape Coast Metropolis. Interviewer‐administered questionnaires were employed to obtain data from 198 postmenarchal adolescents aged 10–19 years. The data were analysed via STATA 15.1. Bivariate and multivariate logistic regression were used to establish the strength of associations between all significant variables, and the results are reported as crude and adjusted odds ratios. Most adolescents (75.6%, n = 149) experienced menarche between the ages of 12 and 13 years; the least common age at menarche was 9. The prevalence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
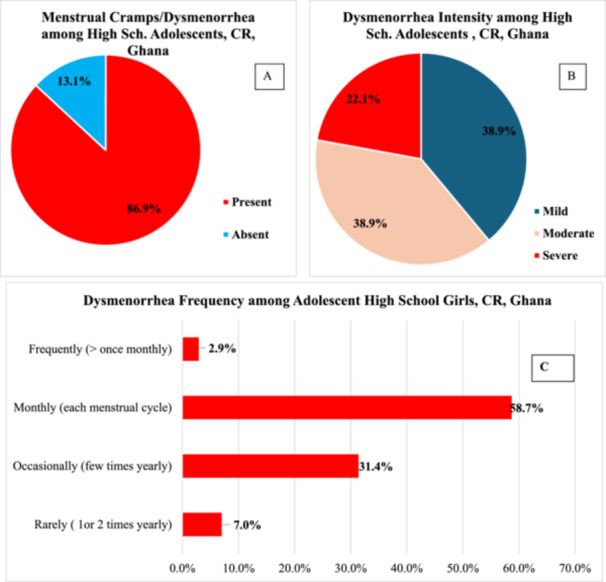 Figure 1
Figure 1| Variable | Frequency ( | Percentage (%) |
|---|---|---|
| Age category (years) [mean ± SD = 14.45 ± 1.22] | ||
| 12–13 years | 47 | 23.74 |
| 14–16 years | 139 | 70.20 |
| 17–18 years | 12 | 6.06 |
| Level/form | ||
| One | 64 | 32.32 |
| Two | 80 | 40.40 |
| Three | 54 | 27.27 |
| Person reside with | ||
| Guardian | 35 | 17.68 |
| Parent | 163 | 82.32 |
| Relationship with person residing with | ||
| Mother | 51 | 25.76 |
| Father | 8 | 4.04 |
| Both mother and father | 103 | 52.02 |
| Auntie/uncle | 17 | 8.59 |
| Grandparents | 16 | 8.08 |
| Sister/step mother | 3 | 1.52 |
| Occupation of guardian | ||
| Government employed | 70 | 35.35 |
| Self‐employed | 119 | 60.10 |
| Unemployed | 9 | 4.55 |
| Level of education of guardian | ||
| No formal education | 24 | 12.12 |
| Formal education | 136 | 68.69 |
| Informal education | 35 | 17.68 |
| Others | 3 | 1.52 |
| Religion | ||
| Christianity | 172 | 86.87 |
| Islam | 26 | 13.13 |
| Ethnicity | ||
| Ashanti | 35 | 17.68 |
| Fante | 117 | 59.09 |
| Northerner | 13 | 6.57 |
| Ga/Ewe/Akuapem/Krobo | 11 | 5.56 |
| Mole Dagbani | 18 | 9.09 |
| Foreigner | 4 | 2.02 |
| Junior High School (JHS) | ||
| I. K. Islamic JHS (Amamoma) | 36 | 18.18 |
| St. Anthony Anglican JHS (Akotokyir) | 64 | 32.32 |
| Kwaprow M/A JHS (Kwaprow) | 98 | 49.49 |
| Variable | Frequency ( | Percentage (%) |
|---|---|---|
| Age or menarche category (years) [mean ± SD = 12.47 ± 1.04] | ||
| 9–11 years | 23 | 11.68 |
| 12–13 years | 149 | 75.63 |
| 14–17 years | 25 | 12.69 |
| Adolescent has regular cycle | ||
| No | 98 | 49.49 |
| Yes | 17 | 8.59 |
| Not sure | 83 | 41.92 |
| Number of days of regular cycle ( | ||
| 20–25 days | 5 | 29.41 |
| 26–28 days | 8 | 47.06 |
| 29–30 days | 4 | 23.53 |
| Duration of blood flow | ||
| 2 days or less | 7 | 3.54 |
| 3–5 days | 116 | 58.59 |
| Greater than 5 days | 75 | 37.88 |
| Number of pads usually used | ||
| Two or less | 96 | 48.48 |
| Three to four | 88 | 44.44 |
| Five or more | 14 | 7.07 |
| Adolescent female circumcised | ||
| No | 192 | 96.97 |
| Yes | 6 | 3.03 |
| Having history of abortion | ||
| No | 195 | 98.48 |
| Yes | 3 | 1.52 |
| Variable | Overall [ | Dysmenorrhea |
| |
|---|---|---|---|---|
| No [ | Yes [ | |||
| Age category (years) [mean ± SD = 14.45 ± 1.22] | 0.190 | |||
| 12–13 years | 47 (23.74) | 9 (34.62) | 38 (22.09) | |
| 14–16 years | 139 (70.20) | 17 (65.38) | 122 (70.93) | |
| 17–18 years | 12 (6.06) | 0 (0.00) | 12 (6.98) | |
| Level/form | 0.077* | |||
| One | 64 (32.32) | 13 (50.00) | 51 (29.65) | |
| Two | 80 (40.40) | 6 (23.08) | 74 (43.02) | |
| Three | 54 (27.27) | 7 (26.92) | 47 (27.33) | |
| Person reside with | 0.497 | |||
| Guardian | 35 (17.68) | 4 (15.38) | 31 (18.02) | |
| Parent | 163 (82.32) | 22 (84.62) | 141 (81.98) | |
| Relationship with person residing with | 0.303 | |||
| Mother | 51 (25.76) | 3 (11.54) | 48 (27.91) | |
| Father | 8 (4.04) | 0 (0.00) | 8 (4.65) | |
| Both mother and father | 103 (52.02) | 19 (73.08) | 84 (48.84) | |
| Auntie/uncle | 17 (8.59) | 2 (7.69) | 15 (8.72) | |
| Grandparents | 16 (8.08) | 2 (7.69) | 14 (8.14) | |
| Sister/step mother | 3 (1.52) | 0 (0.00) | 3 (1.74) | |
| Occupation of guardian | 0.072 | |||
| Government employed | 70 (35.35) | 11 (42.31) | 59 (34.30) | |
| Self‐employed | 119 (60.10) | 12 (46.15) | 107 (62.21) | |
| Unemployed | 9 (4.55) | 3 (11.54) | 6 (3.49) | |
| Religion | 0.300 | |||
| Christianity | 172 (86.87) | 24 (92.31) | 148 (86.05) | |
| Islam | 26 (13.13) | 2 (7.69) | 24 (13.95) | |
| Level of education of guardian | 0.249 | |||
| No formal education | 24 (12.12) | 4 (15.38) | 20 (11.63) | |
| Formal education | 136 (68.69) | 19 (73.08) | 117 (968.02) | |
| Informal education | 35 (17.68) | 2 (7.69) | 33 (19.19) | |
| Others | 3 (1.52) | 1 (3.85) | 2 (1.16) | |
| Ethnicity | 0.328 | |||
| Ashanti | 35 (17.68) | 7 (26.92) | 28 (16.28) | |
| Fante | 117 (59.09) | 11 (42.31) | 106 (61.63) | |
| Northerner | 13 (6.57) | 2 (7.69) | 11 (6.40) | |
| Ga/Ewe/Akuapem/Krobo | 11 (5.56) | 2 (7.69) | 9 (5.23) | |
| Mole Dagbani | 18 (9.09) | 3 (11.54) | 15 (8.72) | |
| Foreigner | 4 (2.02) | 1 (3.85) | 3 (1.74) | |
| Junior High School (JHS) | 0.004 | |||
| I. K. Islamic JHS (Amamoma) | 36 (18.18) | 2 (7.69) | 34 (19.77) | |
| St. Anthony Anglican JHS (Akotokyir) | 64 (32.32) | 16 (61.54) | 48 (27.91) | |
| Kwaprow M/A JHS (Kwaprow) | 98 (49.49) | 8 (30.77) | 90 (52.33) | |
| Variable | Overall [ | Severe dysmenorrhea |
| |
|---|---|---|---|---|
| No [ | Yes [ | |||
| Age (years) [mean ± SD = 14.45 ± 1.22] | 14.28 ± 0.09 | 15.13 ± 0.21 | 0.0001† | |
| Age category (years) [mean ± SD = 14.45 ± 1.22] | 0.001 | |||
| 12–13 years | 47 (23.74) | 45 (95.74) | 2 (4.26) | |
| 14–16 years | 139 (70.20) | 108 (77.70) | 31 (22.30) | |
| 17–18 years | 12 (6.06) | 7 (58.33) | 5 (41.67) | |
| Level/form | 0.799 | |||
| One | 64 (32.32) | 52 (81.25) | 12 (18.75) | |
| Two | 80 (40.40) | 63 (78.75) | 17 (21.25) | |
| Three | 54 (27.27) | 45 (83.33) | 9 (16.67) | |
| Junior High School (JHS) | 0.016 | |||
| I. K. Islamic JHS (Amamoma) | 36 (18.18) | 32 (88.89) | 4 (11.11) | |
| St. Anthony Anglican JHS (Akotokyir) | 64 (32.32) | 44 (68.75) | 20 (31.25) | |
| Kwaprow M/A JHS (Kwaprow) | 98 (49.49) | 84 (85.71) | 14 (14.29) | |
| Person reside with | 0.120 | |||
| Guardian | 35 (17.68) | 25 (71.43) | 10 (28.57) | |
| Parent | 163 (82.32) | 135 (82.82) | 28 (17.18) | |
| Relationship with person residing with | 0.024 | |||
| Mother | 51 (25.76) | 38 (74.51) | 13 (25.49) | |
| Father | 8 (4.04) | 6 (75.00) | 2 (25.00) | |
| Both mother and father | 103 (52.02) | 91 (88.35) | 12 (11.65) | |
| Auntie/uncle | 17 (8.59) | 13 (76,47) | 4 (23.53) | |
| Grandparents | 16 (8.08) | 9 (56.25) | 7 (43.75) | |
| Sister/step mother | 3 (1.52) | 3 (100.00) | 0 (0.00) | |
| Occupation of guardian | 0.215 | |||
| Government employed | 70 (35.35) | 61 (87.14) | 9 (12.86) | |
| Self‐employed | 119 (60.10) | 92 (77.31) | 27 (22.69) | |
| Unemployed | 9 (4.55) | 7 (77.78) | 2 (22.22) | |
| Level of education of guardian | 0.267 | |||
| No formal education | 24 (12.12) | 17 (70.83) | 7 (29.17) | |
| Formal education | 136 (68.69) | 110 (80.88) | 26 (19.12) | |
| Informal education | 35 (17.68) | 31 (88.57) | 4 (11.43) | |
| Others | 3 (1.52) | 2 (66.67) | 1 (33.33) | |
| Religion | 0.283 | |||
| Christianity | 172 (86.87) | 141 (81.98) | 31 (18.02) | |
| Islam | 26 (13.13) | 19 (73.08) | 7 (26.92) | |
| Ethnicity | 0.904 | |||
| Ashanti | 35 (17.68) | 28 (80.00) | 7 (20.00) | |
| Fante | 117 (59.09) | 96 (82.05) | 21 (17.95) | |
| Northerner | 13 (6.57) | 10 (76.92) | 3 (23.08) | |
| Ga/Ewe/Akuapem/Krobo | 11 (5.56) | 8 (72.73) | 3 (27.27) | |
| Mole Dagbani | 18 (9.09) | 15 (83.33) | 3 (16.67) | |
| Foreigner | 4 (2.02) | 3 (75.00) | 1 (25.00) | |
| Variable | Overall [ | Dysmenorrhea |
| |
|---|---|---|---|---|
| No [ | Yes [ | |||
| Age of menarche (years) [mean ± SD = 12.47 ± 1.04] | 12.77 ± 0.99 | 12.43 ± 1.04 | 0.059† | |
| Age or menarche categories | 0.226 | |||
| 9–11 years | 23 (11.68) | 2 (8.70) | 21 (91.30) | |
| 12–13 years | 149 (75.63) | 18 (12.08) | 131 (87.92) | |
| 14–17 years | 25 (12.69) | 6 (24.00) | 19 (76.00) | |
| Adolescent has regular cycle | 0.010 | |||
| No | 98 (49.49) | 6 (6.12) | 92 (93.88) | |
| Yes | 17 (8.59) | 3 (17.65) | 14 (82.35) | |
| Not sure | 83 (41.92) | 17 (20.48) | 66 (79.52) | |
| Number of days of regular cycle ( | 0.065 | |||
| 20–25 days | 5 (29.41) | 1 (20.00) | 4 (80.00) | |
| 26–28 days | 8 (47.06) | 0 (0.00) | 8 (100.00) | |
| 29–30 days | 4 (23.53) | 2 (50.00) | 2 (50.00) | |
| Duration of blood flow | 0.057 | |||
| 2 days or less | 7 (3.54) | 3 (42.86) | 4 (57.14) | |
| 3–5 days | 116 (58.59) | 16 (13.79) | 100 (86.21) | |
| Greater than 5 days | 75 (37.88) | 7 (9.33) | 68 (90.67) | |
| Number of pads usually used | 0.713 | |||
| Two or less | 96 (48.48) | 11 (11.46) | 85 (88.54) | |
| Three to four | 88 (44.44) | 13 (14.77) | 75 (85.23) | |
| Five or more | 14 (7.07) | 2 (14.29) | 12 (85.71) | |
| Adolescent female circumcised | 0.425 | |||
| No | 192 (96.97) | 26 (13.54) | 166 (86.46) | |
| Yes | 6 (3.03) | 0 (0.00) | 6 (100.00) | |
| Having history of abortion | 0.654 | |||
| No | 195 (98.48) | 26 (13.33) | 169 (86.67) | |
| Yes | 3 (1.52) | 0 (0.00) | 3 (100.00) | |
| Variable | Overall [ | Severe dysmenorrhea |
| |
|---|---|---|---|---|
| No [ | Yes [ | |||
| Age of menarche (years) [mean ± SD = 12.47 ± 1.04] | 12.47 ± 0.08 | 12.50 ± 0.21 | 0.855† | |
| Age or menarche categories | 0.787 | |||
| 9–11 years | 23 (11.68) | 19 (82.61) | 4 (17.39) | |
| 12–13 years | 149 (75.63) | 121 (81.21) | 28 (18.79) | |
| 14–17 years | 25 (12.69) | 19 (76.00) | 6 (24.00) | |
| Adolescent has regular cycle | 0.183 | |||
| No | 98 (49.49) | 84 (85.71) | 14 (14.29) | |
| Yes | 17 (8.59) | 12 (70.59) | 5 (29.41) | |
| Not sure | 83 (41.92) | 64 (77.11) | 19 (22.89) | |
| Number of days of regular cycle ( | 1.000 | |||
| 20–25 days | 5 (29.41) | 3 (60.00) | 2 (40.00) | |
| 26–28 days | 8 (47.06) | 6 (75.00) | 2 (25.00) | |
| 29–30 days | 4 (23.53) | 3 (75.00) | 1 925.00) | |
| Duration of blood flow | 0.400 | |||
| 2 days or less | 7 (3.54) | 6 (85.71) | 1 (14.29) | |
| 3–5 days | 116 (58.59) | 97 (83.62) | 19 (16.38) | |
| Greater than 5 days | 75 (37.88) | 57 (76.00) | 18 (24.00) | |
| Crumps frequency ( | 0.002 | |||
| Rarely (1 or 2 times yearly) | 12 (6.98) | 12 (100.00) | 0 (0.00) | |
| Occasionally (few times yearly) | 54 (31.40) | 46 (85.19) | 8 (14.81) | |
| Monthly (each menstrual cycle) | 101 (58.72) | 75 (74.26) | 26 (25.74) | |
| Frequently (> once monthly) | 5 (2.91) | 1 (20.00) | 4 (100.00) | |
| Number of pads usually used | 0.886 | |||
| Two or less | 96 (48.48) | 77 (80.21) | 19 (19.79) | |
| Three to four | 88 (44.44) | 72 (81.82) | 16 (18.18) | |
| Five or more | 14 (7.07) | 11 (78.57) | 3 (21.43) | |
| Pain duration ( | 0.001 | |||
| 2 or less days | 127 (73.84) | 107 (84.25) | 20 (15.75) | |
| 3 days and more | 45 (26.16) | 27 (60.00) | 18 (40.00) | |
| Adolescent female circumcised | 0.086 | |||
| No | 192 (96.97) | 157 (81.770 | 35 (18.23) | |
| Yes | 6 (3.03) | 3 (50.00) | 3 (50.00) | |
| Having history of abortion | 1.000 | |||
| No | 195 (98.48) | 157 (80.51) | 38 (19.49) | |
| Yes | 3 (1.52) | 3 (100.00) | 0 (0.00) | |
| Variable | Overall [ | Dysmenorrhea |
| |
|---|---|---|---|---|
| No [ | Yes [ | |||
|
| ||||
| It restricts me from my normal physical activities | < 0.0001 | |||
| No | 110 (55.56) | 23 (20.91) | 87 (79.09) | |
| Yes | 88 (44.44) | 3 (3.41) | 85 (96.59) | |
| I have poor concentration in both school and home | 0.163* | |||
| No | 120 (60.61) | 19 (15.83) | 101 (84.17) | |
| Yes | 78 (39.39) | 7 (8.97) | 71 (91.03) | |
| Social withdrawal | 0.216* | |||
| No | 115 (58.08) | 18 (15.65) | 97 (84.35) | |
| Yes | 83 (41.92) | 8 (9.64) | 75 (90.36) | |
| Unnecessary irritation | 0.621* | |||
| No | 113 (57.07) | 16 (14.16) | 97 (85.84) | |
| Yes | 85 (42.93) | 10 (11.76) | 75 (88.24) | |
| Decreased academic performance | 0.558 | |||
| No | 168 (84.85) | 21 (12.50) | 147 (87.50) | |
| Yes | 30 (15.15) | 5 (16.67) | 25 (83.33) | |
| I absent myself from school | 0.049 | |||
| No | 175 (88.38) | 26 (14.86) | 149 (85.14) | |
| Yes | 23 (11.62) | 0 (0.00) | 23 (100.00) | |
| Other effects | 1.000 | |||
| No | 193 (97.47) | 26 (13.47) | 167 (86.53) | |
| Yes | 5 (2.53) | 0 (0.00) | 5 (100.00) | |
|
| ||||
| Use of over‐the‐counter medications | 0.234 | |||
| No | 145 (73.23) | 22 (15.17) | 123 (84.83) | |
| Yes | 53 (26.77) | 4 (7.55) | 49 (92.45) | |
| Mostly ignore the pain | 0.527* | |||
| No | 142 (71.72) | 20 (14.08) | 122 (85.92) | |
| Yes | 56 (28.28) | 6 (10.71) | 50 (89.29) | |
| I just rest | 0.380* | |||
| No | 106 (53.54) | 16 (15.09) | 90 (84.91) | |
| Yes | 92 (46.46) | 10 (10.87) | 82 (89.13) | |
| Practice heat therapy | 0.137 | |||
| No | 180 (90.91) | 26 (14.44) | 154 (85.56) | |
| Yes | 18 (9.09) | 0 (0.00) | 18 (100.00) | |
| Consult a physician | 0.365 | |||
| No | 187 (94.44) | 26 (13.90) | 161 (86.10) | |
| Yes | 11 (5.56) | 0 (0.00) | 11 (100.00) | |
| Engage in physical activities | 0.013* | |||
| No | 174 (87.88) | 19 (10.92) | 155 (89.08) | |
| Yes | 24 (12.12) | 7 (29.17) | 17 (70.83) | |
| Herbal remedies/alternative therapies | 0.336 | |||
| No | 189 (95.45) | 24 (12.70) | 165 (87.30) | |
| Yes | 9 (4.55) | 2 (22.22) | 7 (77.78) | |
| Other mechanisms | 0.129 | |||
| No | 193 (97.47) | 24 (12.44) | 169 (87.56) | |
| Yes | 5 (2.23) | 2 (40.00) | 3 (60.00) | |
| Pain medications used ( | 0.693 | |||
| Menstak | 7 (13.21) | 1 (14.29) | 6 (85.71) | |
| Paracetamol | 34 (64.15) | 2 (5.88) | 32 (94.12) | |
| Aspirin/Hyoscine/Ibuprofen | 7 (13.21) | 1 (14.29) | 6 (85.71) | |
| Others (Gebedol/Efpac/Lydia) | 5 (9.43) | 0 (0.00) | 5 (100.00) | |
| Effectiveness of pain medication ( | 0.935 | |||
| Not effective | 5 (9.43) | 0 (0.00) | 5 (100.00) | |
| Poorly effective | 9 (16.98) | 0 (0.00) | 9 (100.00) | |
| Mildly effective | 15 (28.30) | 2 (13.33) | 13 (86.67) | |
| Moderately effective | 10 (18.87) | 1 (10.00) | 9 (90.00) | |
| Highly effective | 14 (26.42) | 1 (7.14) | 13 (92.86) | |
| Variable | OR | 95% CI |
| AOR | 95% CI |
|
|---|---|---|---|---|---|---|
| Junior High School (JHS) | ||||||
| St. Anthony Anglican JHS (Akotokyir) | Ref | Ref | Ref | Ref | Ref | Ref |
| I. K. Islamic JHS (Amamoma) | 5.67 | 1.22–26.28 | 0.027 | 3.82 | 0.72–20.28 | 0.115 |
| Kwaprow M/A JHS (Kwaprow) | 3.75 | 1.50–9.39 | 0.005 | 1.49 | 0.34–6.54 | 0.597 |
| Age of menarche (years) | 0.73 | 0.49–1.09 | 0.120 | 0.51 | 0.28–0.91 | 0.023 |
| Adolescent has regular cycle | ||||||
| Not sure | Ref | Ref | Ref | Ref | Ref | Ref |
| No | 3.95 | 1.48–10.55 | 0.006 | 1.74 | 0.36–8.33 | 0.489 |
| Yes | 1.20 | 0.31–4.67 | 0.790 | 0.36 | 0.06–2.08 | 0.254 |
| It restricts me from my normal physical activities | ||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref |
| Yes | 7.49 | 2.17–25.88 | 0.001 | 11.97 | 2.61–54.93 | 0.001 |
| I absent myself from school | ||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref |
| Yes | Predicts success perfectly | Predicts success perfectly | ||||
| Engage in physical activities | ||||||
| Yes | Ref | Ref | Ref | Ref | Ref | Ref |
| No | 3.36 | 1.23–9.14 | 0.018 | 6.29 | 1.70–23.34 | 0.006 |
| Variable | OR ± SE | 95% CI |
| AOR | 95% CI |
|
|---|---|---|---|---|---|---|
| Junior High School (JHS) | ||||||
| St. Anthony Anglican JHS (Akotokyir) | Ref | Ref | Ref | Ref | Ref | Ref |
| I. K. Islamic JHS (Amamoma) | 0.28 ± 0.16 | 0.09–0.88 | 0.03 | 0.11 ± 0.09 | 0.02–0.52 | 0.006 |
| Kwaprow M/A JHS (Kwaprow) | 0.37 ± 0.14 | 0.17–0.80 | 0.011 | 0.41 ± 0.22 | 0.14–1.15 | 0.091 |
| Age (years) | 1.75 ± 0.27 | 1.30–2.36 | < 0.0001 | 1.46 ± 0.33 | 0.93–2.28 | 0.099 |
| Age category (years) | ||||||
| 12–13 years | Ref | Ref | Ref | Ref | Ref | Ref |
| 14–16 years | 6.45 ± 4.85 | 1.48–28.13 | 0.01 | 4.01 ± 3.35 | 0.78–20.62 | 0.096 |
| 17–18 years | 16.07 ± 14.95 | 2.60–99.48 | 0.003 | 2.92 ± 3.67 | 0.25–34.31 | 0.393 |
| Relationship with person residing with | ||||||
| Both mother and father | Ref | Ref | Ref | Ref | Ref | Ref |
| Mother | 2.59 ± 1.15 | 1.09–6.20 | 0.032 | 3.54 ± 2.07 | 1.13–11.14 | 0.030 |
| Father | 2.53 ± 2.21 | 0.46–13.97 | 0.288 | 4.29 ± 4.86 | 0.46–39.56 | 0.199 |
| Auntie/uncle | 2.33 ± 1.51 | 0.65–8.32 | 0.192 | 2.36 ± 2.16 | 0.39–14.24 | 0.350 |
| Grandparents | 5.90 ± 3.48 | 1.86–18.75 | 0.003 | 8.31 ± 7.10 | 1.56–44.33 | 0.013 |
| Crumps frequency ( | ||||||
| Occasionally (few times yearly) | Ref | Ref | Ref | Ref | Ref | Ref |
| Monthly (each menstrual cycle) | 1.99 ± 0.89 | 0.83–4.77 | 0.122 | 1.64 ± 0.87 | 0.58–4.66 | 0.354 |
| Frequently (> once monthly) | 23.00 ± 27.18 | 2.27–233.19 | 0.008 | 19.12 ± 29.88 | 0.89–409.07 | 0.059 |
| Pain duration ( | ||||||
| 2 or less days | Ref | Ref | Ref | Ref | Ref | Ref |
| 3 days and more | 3.57 ± 1.39 | 1.66–7.65 | 0.001 | 3.92 ± 2.14 | 1.35–11.42 | 0.012 |
| Decreased academic performance | ||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref |
| Yes | 3.64 ± 1.56 | 1.57–8.45 | 0.003 | 3.70 ± 2.41 | 1.03–13.24 | 0.045 |
| Use of over‐the‐counter medications | ||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref |
| Yes | 2.42 ± 0.91 | 1.15–5.07 | 0.020 | 1.63 ± 0.83 | 0.60–4.43 | 0.337 |
| Mostly ignore the pain | ||||||
| Yes | Ref | Ref | Ref | Ref | Ref | Ref |
| No | 3.09 ± 1.57 | 1.14–8.37 | 0.027 | 3.73 ± 2.40 | 1.05–13.20 | 0.042 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMenstrual Health and Disorders · Hypothalamic control of reproductive hormones · Maternal Mental Health During Pregnancy and Postpartum
Introduction
1
Dysmenorrhea refers to painful uterine cramps that occur before or during menstruation [1]. The pain is usually localized in the lower abdomen and can radiate to the back and thighs [2]. Menstruation is associated with increased production of prostaglandins and vasopressin. While prostaglandins cause uterine contractions and pain, vasopressin release enhances uterine contractility and causes ischemic pain by inducing vasoconstriction [3]. Additionally, hormonal fluctuations during the menstrual cycle can cause dysmenorrhea [4]. Stress, diet, menstrual irregularities, menarchal age, and family relationships may influence menstrual pain intensity [5].
Dysmenorrhea is a prevalent gynaecological condition affecting a significant number of adolescent girls during their menstrual cycles. Studies have reported that the prevalence of dysmenorrhea is 60%–93% among adolescents [6]. In a cross‐sectional study among adolescents in the Greater Accra region of Ghana, Acheampong et al. (2019) reported that the prevalence of dysmenorrhea was 68.1% [3]. In a similar study in the northern region of Ghana, a prevalence of 80.9% was reported [7]. These high prevalence rates highlight the widespread nature of dysmenorrhea and raise concerns about its impact on adolescents' health and daily activities.
Dysmenorrhea adversely affects adolescents [8], as usual activities such as sitting, walking, and having a full bladder can cause or intensify menstrual pain [9]. Dysmenorrhea is the primary cause of recurrent short‐term school absenteeism among menstruating adolescents [10, 11]. It affects academic performance through interference with concentration and performance [12, 13]. Pain and discomfort can lead to emotional distress, increased irritability, and decreased participation in social and extracurricular activities [14, 15]. To annul this pain and discomfort associated with dysmenorrhea, adolescents rely on a variety of coping mechanisms, such as ignoring pain [3], heat therapy [16], rest [11], self‐medication [17], and a few consult physicians [3].
Despite its high prevalence and considerable impact on daily activities, dysmenorrhea is often poorly managed and frequently overlooked. Many young females endure pain in silence because of a lack of awareness, social stigma, and the normalization of menstrual discomfort. We used a cross‐sectional study design to collect data on the prevalence, effects, and coping mechanisms of dysmenorrhea among adolescents in the Cape Coast metropolis to provide insights into the burden of dysmenorrhea and to inform preventive and control strategies in the district. To the best of our knowledge, this is the first study among the adolescent population in the Cape Coast Municipality.
Methodology
2
Study Design, Duration, Site, and Sample Size
2.1
This cross‐sectional study was conducted among female adolescents in Junior High Schools (JHSs) in the Cape Coast Municipality. We collected data on the prevalence, effects, and coping mechanisms of dysmenorrhea from 11th July to 14th July 2023. We sent a cover letter and proposal to 10 basic and JHSs in the Cape Coast metropolis and received a positive response from three of the schools. Schools were selected based on the criterion that they had both JHS and primary, as the JHS level typically enrolls girls aged 10–19 years, which aligned with our target audience. Data were collected from Kwaprow M/A JHS (Kwaprow), Imam Khomeini Islamic JHS (Amamoma), and St. Anthony Anglican JHS (Akotokyir). These schools were public JHSs serving broadly similar catchment populations. No formal school‐level or institutional characteristics were collected. An initial form was distributed to participants to collect data on their age, previous intrauterine device use, history of pelvic infections or previous pelvic surgery or trauma and attainment of menarche to assess participants' eligibility. We collected data from 198 postmenarchal adolescent girls between the ages of 10 and 19. Participants were recruited based on their menstrual status, age, and the absence of secondary pelvic conditions.
Eligibility Criteria
2.2
JHS adolescent girls aged 10–19 years who had their first menstrual period were recruited for the study. Adolescents who had not reached menarche; those with mental or physical conditions that could affect their ability to participate in the study; those with pelvic pathologies such as sexually transmitted diseases, endometriosis, and urinary tract infections, which were identified through medical history collection prior to data collection; and those on antidepressants, contraceptives and students who could neither understand English nor Fante, were excluded from the study. The assessment conducted before recruitment revealed that none of the participants used hormonal contraception, and two were excluded because they had a history of pelvic infections.
Data Collection
2.2.1
Pretested, interviewer‐administered paper questionnaires were used to collect data on dysmenorrhea. The questionnaire was divided into four sections: sociodemographics (age, gender, religious affiliation, guardian, relationship with guardian, guardian's educational level), obstetric and gynaecological characteristics, prevalence and impact of dysmenorrhea, and coping mechanisms. The questionnaire was semi‐structured with a combination of closed‐ and open‐ended questions. The questionnaire design aligned with the specific objectives of the study and the population's demographics after a thorough appraisal of the literature [9, 12, 17, 18, 19]. We defined a regular menstrual cycle as a constant 26–32‐day interval during each menstrual cycle [20]. We assessed the severity of dysmenorrhea via the visual analogue scale (VAS). The VAS assesses the female perception of pain and ranges from 0 to 10: no pain to unbearable. The scale was interpreted as mild pain (1–3), moderate pain (4–7), or severe pain (8–10) [7, 21]. Following pretesting and literature‐informed design, no responses were received outside the predefined categories. Accordingly, all responses were coded into the existing categories and analysed quantitatively. Responses were analysed quantitatively, with responses categorized and presented as frequencies and percentages. The questionnaire was administered on paper.
Data Analysis
2.3
The data were initially entered into Microsoft Office Excel (2016), organized and imported into STATA 15.1 (StataCorp LLC, Texas 77845, USA) for analysis. The respondents' sociodemographic, obstetric, and gynaecological data are presented in tables and figures. Continuous data are presented as the means with standard deviations, whereas categorical data are presented as frequencies and percentages. Associations were examined both for the overall prevalence of dysmenorrhea and separately for severe dysmenorrhea. Chi‐square (χ ^2^) analysis was used to explore any associations between severe dysmenorrhea and the sociodemographic, obstetric, and gynaecological characteristics of the adolescents. For all significant variables, bivariate and multivariate logistic regression were used to establish the strength of the associations, and the results are reported as adjusted odds ratios. All analyses were two‐sided, pre‐specified, and performed at a 95% confidence interval, and a p‐value < 0.05 was considered to indicate statistical significance.
Results
3
Among the 198 participants involved in this study, the majority were in their second years (40.4%) of JHS, were Christian (86.9%), and were between the ages of 14 and 16 years (70.2%) (Table 1). Only 52.0% (n = 103) of the participants lived with both parents, and 25.8% (n = 51) lived with only their mothers. The majority of the guardians of these adolescents were self‐employed (60.1%, n = 119) and had no formal education (68.7%, n = 136). We found that most adolescents (75.6%, n = 149) had their first menstrual period between the ages of 12 and 13 years; the least common age at menarche was 9 years, and the maximum was 17 years (Table 2). Only 8.6% (n = 17) of the girls could confirm that they had a regular menstrual cycle, with almost half of the participants (n = 98) without a regular cycle, and 41.9% were unsure if they had regular cycles or not. During their menstrual period, 58.6% (n = 116) of the participants experienced blood flow within 3–5 days, while 37.9% (n = 75) had menses lasting more than 5 days. The reported prevalence of female circumcision was 3.0% (n = 6) among girls. A prior history of abortion was reported by 1.5% (n = 3) of the participants.
The prevalence of dysmenorrhea was 86.9% (n = 172) (Figure 1A). While severe dysmenorrhea was reported by 38 adolescents (22.1%), the rest (77.9%) had either mild (n = 67) or moderate (n = 67) pain during their period of menstruation (Figure 1B). Approximately 26% (n = 45) had pain that lasted 3 days or more. The incidence of dysmenorrhea occurs monthly for most women (58.7%, n = 101), with 31.4% (n = 54) experiencing pain a few times a year (Figure 1C).
Graphs showing the prevalence (A), intensity (B), and frequency (C) of dysmenorrhea among high school adolescents in the Central Region (CR), Ghana.
No significant associations were found between age category (p = 0.2), year of study (p = 0.08), relationship with guardian (p = 0.5), and occupation of guardians (p = 0.07). Age was not significantly associated with the overall prevalence of dysmenorrhea (Table 3); however, increasing age was associated with higher odds of severe dysmenorrhea (Table 4). A significant association was observed between school attendance and dysmenorrhea (χ ^2^ = 11.84, p = 0.004) (Table 3). We found that severe dysmenorrhea was significantly related to different school environments (χ ^2^ = 9.04, p = 0.02), and adolescent relationship with guardian (χ ^2^ = 12.40, *p *= 0.02) (Table 4). There was a significant difference in the ages of those who reported having severe dysmenorrhea (15.1 ± 0.2 years) compared with those who reported otherwise (14.3 ± 0.1 years) (p < 001) (Table 4).
Adolescents with irregular menstrual cycles had significantly higher prevalence of dysmenorrhea compared to those with regular cycles (p = 0.01) (Table 5). Severe dysmenorrhea was significantly associated with the frequency of menstrual cramps (χ ^2^ = 15.59, *p *= 0.002) and the duration of pain (χ ^2^ = 11.35, p = 0.001) (Table 6).
The presence of dysmenorrhea was self‐reported to restrict adolescents from performing their normal physical activities (44.4%, n = 88). It led to poor concentration at school and home (39.4%, n = 78), social withdrawal (41.9%, n = 83), heightened irritability (42.9%, n = 85), a decrease in academic performance (15.2%, n = 30), and absenteeism (11.6%, n = 23) (Table 7). Adolescents with dysmenorrhea were restricted from their normal physical activities (χ ^2^ = 13.13, p < 0.001) (Table 8). Severe dysmenorrhea was associated with a decrease in the academic performance of adolescents. Adolescents who reported dysmenorrhea engaged in few activities as coping mechanisms. Notably, over‐the‐counter medications (26.8%, n = 53), ignoring pain (28.3%, n = 56), and rest (46.5%, n = 92) were mostly practiced while only a few visit the hospital (6.4%). We found a significant association between severe dysmenorrhea and the use of over‐the‐counter medications (χ ^2^ = 5.64, p = 0.02) and ignoring pain (χ ^2^ = 5.30, p = 0.02) as coping mechanisms (Table 9).
Adolescents who experienced early menarche (9–11 years) had significantly lower odds of reporting severe dysmenorrhea compared to those with late menarche (14–17 years) [AOR = 0.51, 95% CI = 0.28–0.91, p = 0.02] (Table 9). Adolescents attending the Islamic JHS (AOR = 0.11 ± 0.09, 95% CI = 0.0–0.5, p = 0.006) and the Kwaprow JHS (OR = 0.37 ± 0.14, 95% CI = 0.2–0.8, p < 0.0001) had higher odds of reporting severe dysmenorrhea (Table 9).
Increasing age was significantly associated with increased odds of having severe dysmenorrhea. Adolescents residing with only their mother had approximately fourfold higher odds of reporting severe dysmenorrhea (AOR = 3.5 ± 2.1, 95% CI = 1.1–11.1, p = 0.03) and an eightfold‐fold increase in the odds of having dysmenorrhea if one resides with her grandparents (AOR = 8.3 ± 7.1, 95% CI = 1.6–44.3, p = 0.01) (Table 9).
Discussion
4
This study assessed the prevalence, effects, and coping mechanisms of dysmenorrhea among adolescent girls in JHSs in the Cape Coast Municipality. The prevalence of dysmenorrhea was 86.9% (n = 172). Approximately half of the participants (n = 98) had irregular menstrual cycles; dysmenorrhea was less likely to occur in adolescents who reported early menarche, and living with grandparents was associated with a higher likelihood of reporting dysmenorrhea. Dysmenorrhea significantly restricted adolescents from their normal physical activities; approximately 30% of the participants relied on over‐the‐counter medications for pain management, whereas only 6.4% consulted a physician.
We found that the prevalence of dysmenorrhea was 86.9%. This is in line with the established prevalence of dysmenorrhea (60%–93%) among the study population [6]. Compared with a similar study among adolescents in the Greater Accra region (prevalence of 68.1%) [3], we found an increased prevalence of dysmenorrhea. Nonetheless, our findings correlate well with studies by Ameade et al. (2018) in the northern region of Ghana [17] and other cross‐sectional studies in Lebanon [7] and Ireland [13].
Approximately half of the participants (n = 98) had irregular cycles, with only 8.6% (n = 17) confirming that they had regular menstrual cycles. This finding is comparable with the findings of studies conducted among adolescents in Ethiopia and among nursing students in Lebanon, which reported prevalence rates of 42.8% and 53.5%, respectively. This figure is high compared with the 25.7% of menstrual irregularities reported by Acheampong et al. [3] in Ghana and the 18.6% reported by Amu and Bamidele [19] in Nigeria. These variations may be attributed to differences in study populations, demographics and sample size. A significant proportion of participants (41.9%) reported uncertainty about their menstrual cycle regularity. This reflects limited menstrual health knowledge among adolescents and the need for heightened menstrual health education in schools. We found a significant relationship between the prevalence of dysmenorrhea and irregular menstrual cycles, which is in line with the findings of previous studies [3, 22]. Irregular menstrual cycles are often characterized by fluctuations in oestrogen and progesterone levels, which affect ovulation and prostaglandin production, leading to intense uterine contractions and pain. While our findings reinforce the association between irregular menstrual cycles and dysmenorrhea, the underlying mechanism remains complex and multifactorial.
Compared to those who had late menarche, adolescents who experienced early menarche were 50% less likely to report dysmenorrhea. In a study among adolescent girls in India, Patel and Barot [2] reported that women who reported early menarche were more likely to experience dysmenorrhea. However, there is some controversial evidence regarding the influence of early and late menarche on dysmenorrhea [23]. De Sanctis et al. [24], in a study among Italian adolescent girls, reported that menarchal age independently does not affect dysmenorrhea. The controversy may lie in the discrepancies in sample sizes and participants' sociodemographics. Given that dysmenorrhea is influenced by a combination of genetic [25], biological [26], environmental [8], and psychosocial factors [5, 27], isolating the effect of menarchal age is challenging. Age was not associated with the overall presence of dysmenorrhea in this study; however, it was associated with the severity of dysmenorrhea among affected adolescents. While dysmenorrhea occurred across all age groups, symptom severity increased with age.
Adolescents who stayed with their grandparents were 8.3 times more at risk of experiencing dysmenorrhea compared with those who stayed with both parents. This aligns with the findings of Acheampong et al. [3], who concluded that adolescents not living with their parents have significantly higher odds of self‐reported dysmenorrhea. Adolescents who do not reside with their parents face a greater risk of experiencing dysmenorrhea due to factors such as parental separation or loss and exposure to domestic conflicts or instability, all of which increase stress levels. Notably, we also found that the school environment influenced the prevalence of dysmenorrhea, with students at Islamic JHS and Kwaprow JHS demonstrating higher odds of reporting the condition. Owing to the already established connection between psychological stressors, environment and dysmenorrhea [5], it is plausible that differences in school community dynamics, menstrual stigma, and socioeconomic background may also contribute may influence dysmenorrhea severity. This merits further investigation with designs better suited to explore school‐level influences.
Dysmenorrhea significantly restricts the normal physical activities of adolescents, as supported by many studies [15, 27]. Nearly half (49.4%) of the participants who reported dysmenorrhea experienced physical activity limitations as a result of their condition. Abreu‐Sánchez et al. [9], in a study among Spanish nursing students, reported that certain daily activities, such as sitting, walking, and having a full bladder, caused or intensified menstrual pain among students with dysmenorrhea. Some studies have demonstrated that regular exercise can significantly reduce the severity and frequency of dysmenorrhea [28, 29]. Engaging in regular exercise induces hormonal changes in the uterine lining, which can alleviate the symptoms associated with dysmenorrhea [30]. Physical activity can increase the production of endorphins, which act as natural painkillers and improve blood flow to the pelvic region. In the current study, only 9.9% of the adolescents used physical activity as a coping mechanism for dysmenorrhea. This is comparable to the findings of Acheampong et al. [3] (14%). Given that physical activity can reduce pain intensity, it is imperative to promote public education on the benefits of exercise as an effective strategy for managing dysmenorrhea.
Dysmenorrhea is the primary cause of recurrent short‐term school absenteeism among menstruating adolescents [10, 11, 15]. This may affect their performance academically due to interference with concentration and performance during their period [12, 13]. We found that 13.4% of the adolescents with dysmenorrhea reported absenteeism, and 41.3% reported poor concentration at home and at school. These findings are consistent with those of previous studies reporting that 5%–14% of adolescents absent themselves from school due to dysmenorrhea [31]. School‐based interventions that provide menstrual health education and support systems to adolescents could significantly enhance their attendance and academic engagements.
Self‐medication, also known as over‐the‐counter medication, is widely practiced in both developed and developing countries, especially among menstruating women [32]. In this study, 29% of the adolescents ignored pain, and 28.4% relied on over‐the‐counter medications for pain management. Menstak, paracetamol, and ibuprofen are among the commonly used drugs. This corresponds with the findings of Acheampong et al. [3], who reported that 34.6% of adolescents relied heavily on self‐medication. Only 6.4% of the adolescents had consulted a physician for their menstrual pain. This aligns with many studies indicating that most adolescents with dysmenorrhea do not seek medical consultation [32]. The reluctance to consult a physician can be attributed to various factors, including the normalization of menstrual pain, lack of awareness about effective treatment options, and stigma surrounding menstrual health issues [33]. This gap in adolescent healthcare access and awareness necessitates initiatives that promote safe pain management practices and improve access to adolescent‐friendly reproductive health services. While over‐the‐counter pain relievers have proven to be effective in providing symptomatic relief for this population [1], increased access to medication also raises concerns about non‐responsible self‐medication [32]. Delays in seeking medical advice when needed, adverse drug–drug interactions, and improper dosages are among the few concerns that can arise from self‐medication [34]. Additionally, some diseases may have presentations similar to those of dysmenorrhea, which may lead to misdiagnosis and, consequently, improper treatment [35].
Limitations
4.1
We used a cross‐sectional design to collect self‐reported data on dysmenorrhea among adolescent girls. This makes our work prone to recall bias. Our sample size of 198 may also limit the generalizability of our findings. The majority of participants had not sought medical evaluation or consulted a healthcare professional, limiting our ability to definitively exclude secondary causes of dysmenorrhea. We did not adjust analyses of age at menarche for gynaecological age, which may influence dysmenorrhea severity.
Conclusion
5
Our study revealed that the incidence of dysmenorrhea is very high among adolescents in the Cape Coast municipality and adversely affects their social and academic lives. With nearly one‐third of adolescents relying on over‐the‐counter drugs and only 6.4% consulting physicians for menstrual pain, there are pervasive concerns of self‐medication. Additionally, this study revealed that psychosocial factors, such as living arrangements and the school environment, play critical roles in the prevalence and severity of dysmenorrhea. These findings highlight significant gaps in healthcare access and important impacts on education, emphasizing the need for better public health strategies.
Author Contributions
Richard K. D. Ephraim and Attoh Tetteh conceived and designed this study. Amina S. Abugri was responsible for data collection and analysis. Gabriel P. Kotam and Angele Comlan‐Cataria drafted the manuscript. Gabriel P. Kotam, Attoh Tetteh, Amina S. Abugri, Stephen Ocansey, and Richard K. D. Ephraim revised the manuscript. Stephen Ocansey and Richard K. D. Ephraim supervised the entire process. All authors read and approved the final version of the manuscript. Gabriel Pezahso Kotam had full access to all of the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors received no specific funding for this work.
Ethics Statement
This study was approved by the Department of Physician Assistant Studies, College of Health and Allied Sciences, University of Cape Coast. The participants were assured of the voluntary nature of the study and their freedom to withdraw at any point during the study if they had any personal reasons to discontinue. Our study protocol conforms to the provisions of the Declaration of Helsinki in 1995 (as revised in Edinburgh 2000).
Consent
Consent was obtained from the Head teachers and guardians of all students recruited for the study.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author, Gabriel P. Kotam, affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. Ghandour , W. Hammoudeh , H. Stigum , R. Giacaman , H. Fjeld , and G. Holmboe‐Ottesen , “The Hidden Burden of Dysmenorrhea Among Adolescent Girls in Palestine Refugee Camps: A Focus on Well‐Being and Academic Performance,” BMC Public Health 24, no. 1 (2024): 726.38448826 10.1186/s 12889-024-18219-0PMC 10918951 · doi ↗ · pubmed ↗
- 2D. Patel and K. Barot , “Prevalence of Dysmenorrhea Among Adolescent Girls in North Gujarat: A Cross Sectional Study,” International Journal of Science and Research (IJSR) 10, no. 6 (2021): 96–100.
- 3K. Acheampong , D. Baffour‐Awuah , D. Ganu , et al., “Prevalence and Predictors of Dysmenorrhea, Its Effect, and Coping Mechanisms Among Adolescents in Shai Osudoku District, Ghana,” Obstetrics and Gynecology International 2019, no. 1 (2019): 1–7.10.1155/2019/5834159 PMC 654578231236112 · doi ↗ · pubmed ↗
- 4J. Jiang , Y. Zhuang , S. Si , et al., “The Association of Reproductive Hormones During the Menstrual Period With Primary Dysmenorrhea,” International Journal of Women's Health 15 (2023): 1501–1514.10.2147/IJWH.S 421950 PMC 1057337937840555 · doi ↗ · pubmed ↗
- 5S. K. Rogers , N. Ahamadeen , C. X. Chen , C. E. Mosher , J. C. Stewart , and K. L. Rand , “Dysmenorrhea and Psychological Distress: A Meta‐Analysis,” Archives of Women's Mental Health 26, no. 6 (2023): 719–735.10.1007/s 00737-023-01365-637632569 · doi ↗ · pubmed ↗
- 6S. Lghoul , M. Loukid , and M. K. Hilali , “Prevalence and Predictors of Dysmenorrhea Among a Population of Adolescent's Schoolgirls (Morocco),” Saudi Journal of Biological Sciences 27, no. 7 (2020): 1737–1742.32565690 10.1016/j.sjbs.2020.05.022PMC 7296472 · doi ↗ · pubmed ↗
- 7S. Karout , L. Soubra , D. Rahme , L. Karout , H. M. J. Khojah , and R. Itani , “Prevalence, Risk Factors, and Management Practices of Primary Dysmenorrhea Among Young Females,” BMC Women's Health 21 (2021): 392.34749716 10.1186/s 12905-021-01532-w PMC 8576974 · doi ↗ · pubmed ↗
- 8E. Fernández‐Martínez , A. Abreu‐Sánchez , J. Pérez‐Corrales , J. Ruiz‐Castillo , J. F. Velarde‐García , and D. Palacios‐Ceña , “Living With Pain and Looking for a Safe Environment: A Qualitative Study Among Nursing Students With Dysmenorrhea,” International Journal of Environmental Research and Public Health 17, no. 18 (2020): 6670.32933209 10.3390/ijerph 17186670 PMC 7558082 · doi ↗ · pubmed ↗