Comparison of neurosurgical and medical management options of space-occupying cerebellar infarction
Cristian D. Mendieta-Barrera, Pavell Dhondt, Anuraag Punukollu, Fabricio Garcia-Torrico, Diana Laura Ochoa-Hernández, Rômulo da Silva Sanglard, Flor Belén Villalobos-Villalobos, Kevin Mamani-Julian, Luciana Rivera-Hurtado, Roel Meeus, Leonardo Rangel-Castilla, Arash Ghaffari-Rafi

TL;DR
This study compares medical and surgical treatments for cerebellar infarctions, finding that surgery, especially a specific combined procedure, improves outcomes for patients with large infarcts or low consciousness.
Contribution
The study identifies specific prognostic thresholds and surgical strategies that improve outcomes for space-occupying cerebellar infarctions.
Findings
Surgical intervention improved outcomes for patients with infarct volumes >51 mL or GCS ≤13.
SDC–N–EVD was the most effective surgical strategy, reducing mortality and hospital stay.
Age and timing within 72 hours did not significantly affect outcomes.
Abstract
Despite space-occupying cerebellar infarctions (SOCIs) carrying a high morbidity and mortality due to mass effect in the posterior fossa, optimal management remains uncertain: particularly regarding patient selection, timing, and surgical technique. We conducted a systematic review and network meta-analysis to compare outcomes between medical versus surgical management, and to identify prognostic thresholds that may guide treatment. A search of PubMed, Embase, and CENTRAL was performed from database inception through October 30, 2024. Studies were included if they reported outcomes in ≥ 10 patients with SOCI treated with medical management and/or surgical interventions, including suboccipital decompressive craniectomy (SDC), external ventricular drainage (EVD), and necrosectomy. Data extraction and risk-of-bias assessment were performed independently by multiple reviewers.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
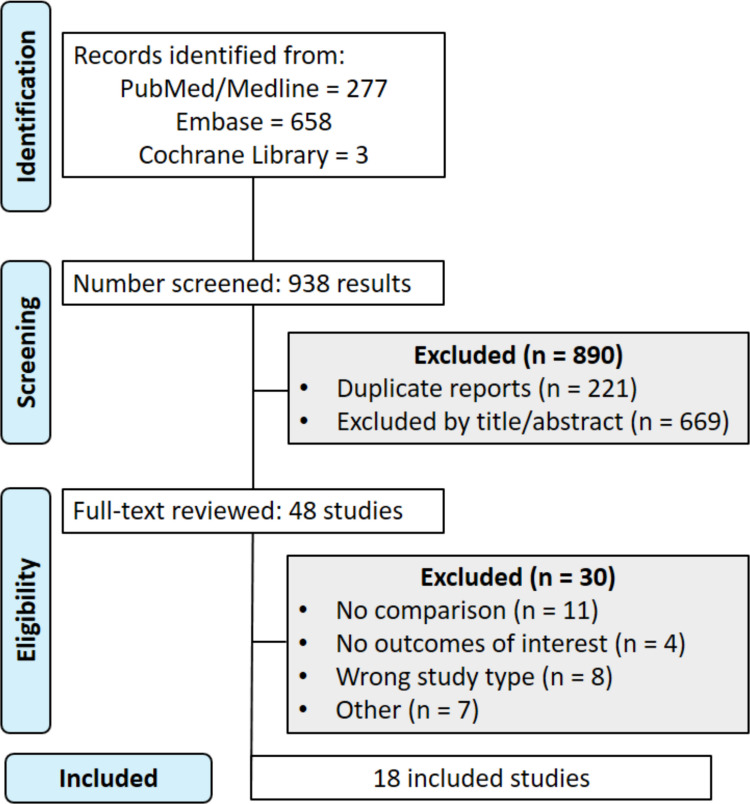 Figure 1
Figure 1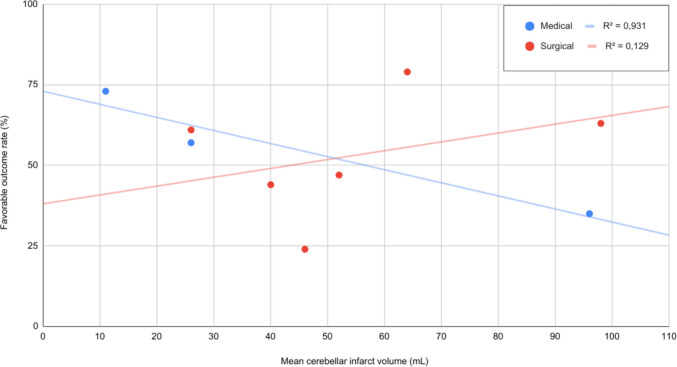 Figure 2
Figure 2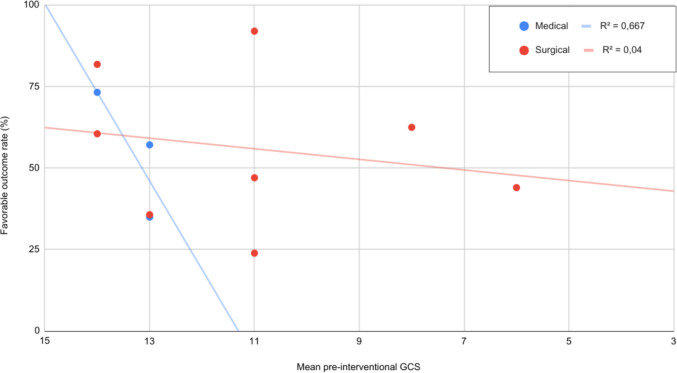 Figure 3
Figure 3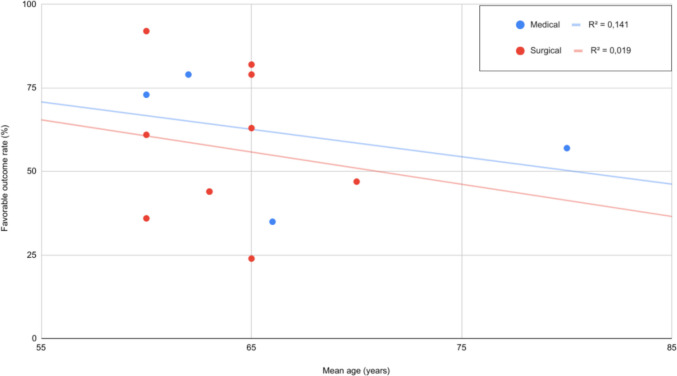 Figure 4
Figure 4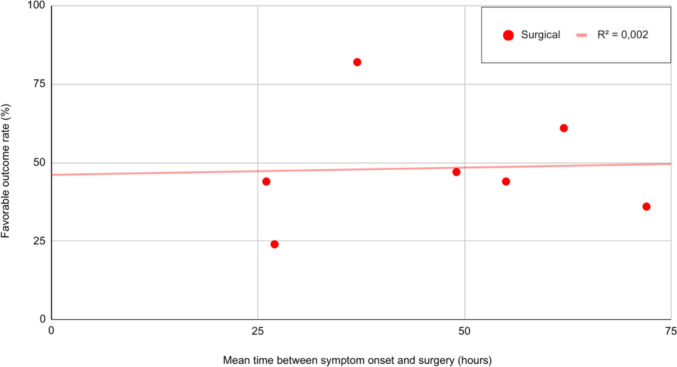 Figure 5
Figure 5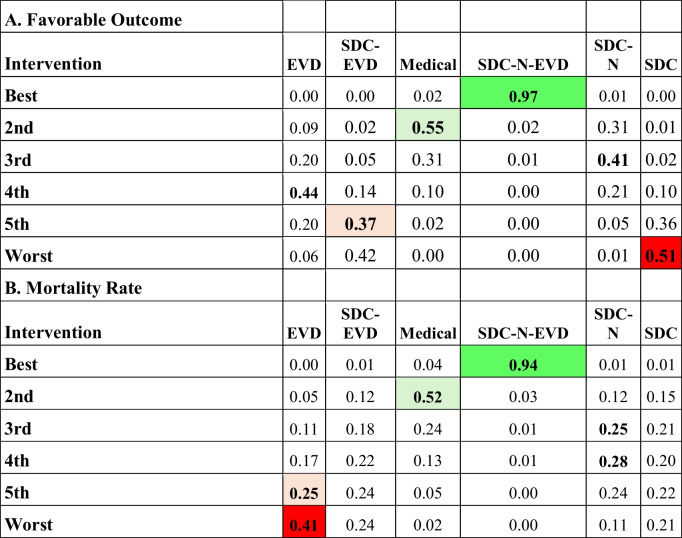 Figure 6
Figure 6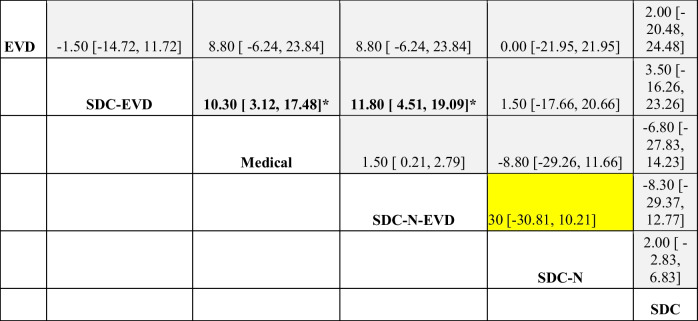 Figure 7
Figure 7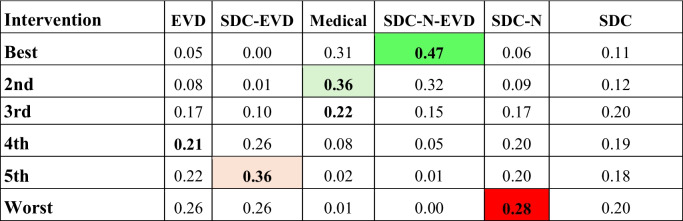 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Vestibular and auditory disorders · Cerebrospinal fluid and hydrocephalus
Introduction
Space-occupying cerebellar infarctions (SOCIs) represent a small proportion of ischemic strokes (1.5–4.2%), yet are associated with disproportionately high morbidity and mortality rates (15–32%), due to the confined anatomy of the posterior fossa [2, 3, 6, 11, 16, 18, 32]. Despite the high risk of life-threatening complications (i.e., obstructive hydrocephalus, brainstem compression, herniation) and death, there remains no consensus on optimal surgical management strategies for SOCIs [11, 16, 18, 24, 29, 32, 38].
Upon diagnosis, initial medical therapy is focused on mitigating cerebral edema and lowering intracranial pressure [8, 24, 35]. However, in the presence of neurological decline or radiographic progression, surgical intervention becomes necessary, including: external ventricular drainage (EVD), suboccipital decompressive craniectomy (SDC), and necrosectomy [1, 8, 14, 15, 24]. Despite widespread use of these surgical interventions, uncertainties remain, regarding their optimal timing, indications, and long-term effectiveness, with no universally accepted treatment algorithm [24, 29]. Crucially, the existing literature often fails to distinguish between specific surgical nuances—such as the added value of necrosectomy or EVD combined with decompression—, leaving a significant gap in knowledge regarding the comparative efficacy of distinct surgical subtypes [1, 8, 14, 15, 24]. Furthermore, while there is literature to suggest that key clinical (pre-interventional Glasgow Coma Scale [GCS] score) and radiographic (infarct volume, presence of hydrocephalus) parameters may guide therapeutic decisions, these findings are tempered by methodological variability, limited sample sizes, and a paucity of randomized controlled trials, which ultimately hinders the development of standardized care pathways [1, 9, 14, 15, 19, 35].
To address these knowledge gaps, we conducted a systematic review and network meta-analysis comparing the efficacy of medical therapy with surgical interventions for SOCI. Unlike traditional pairwise meta-analyses conducted in the literature, our network approach allows for the simultaneous comparison and ranking of multiple treatment strategies [1, 8, 14, 15, 24]. By synthesizing data from diverse clinical settings and intervention strategies, this study aims to clarify treatment outcomes, identify key prognostic indicators, and inform evidence-based recommendations to support individualized, outcome-driven decision-making in the management of SOCI.
Methods
This systematic review and network meta-analysis was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [5, 20, 26].
Literature search
A literature search was performed in MEDLINE (PubMed), Embase, and the Cochrane Central Register for Controlled Trials (CENTRAL) from database inception through October 30, 2024. The search strategy combined keywords and MeSH terms relevant to SOCI and associated interventions, including cerebellar infarction, craniectomy, craniotomy, suboccipital decompressive, and necrosectomy. The full search strategy is provided in Supplementary Methods S1.
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria: involved patients with SOCI; evaluated surgical interventions (e.g., SOC, EVD, or necrosectomy) with or without medical therapy and/or compared different surgical strategies; reported outcomes related to functional status, mortality, or length of stay; included at least 10 patients. Studies were excluded if they were case reports, abstracts, animal studies, reviews, meta-analyses, or not published in English.
Data extraction
Data extraction was performed independently by three reviewers (C.D.M.B., A.P., and P.D.) using a standardized form. Extracted variables included study design, country of origin, patient demographics, pre-interventional GCS scores, comorbidities, infarct volume, time from symptom onset to surgery, type of intervention, follow-up duration, and rate of favorable outcomes. Functional outcomes were recorded as defined in the original studies (e.g., Modified Rankin Scale, Glasgow Outcome Scale, etc.).
Risk of bias assessment
The quality of randomized controlled trials was assessed using the Cochrane Risk of Bias Tool 2.0, while non-randomized studies were evaluated using the Risk Of Bias In Non-randomized Studies of Interventions tool [27, 28]. Highest risk rating across any domain determined the overall study risk. Two reviewers (F.G.T. and C.D.M.B.) independently evaluated each study, with discrepancies resolved through discussion and consensus. Publication bias was evaluated via funnel plots.
Statistical analysis
Linear regression
Associations between favorable outcome rates and pre-interventional variables were explored using linear regression analyses. Independent variables included infarct volume (mL), patient age, pre-interventional GCS score, and time between symptom onset and surgery as independent variables; the dependent variable was favorable outcome rate. The strength of association was assessed using the coefficient of determination (R^2^), and statistical significance was determined using two-tailed p-values. Two-sample z-tests for proportions were applied to evaluate categorical variables.
Meta-analysis
For binary outcomes (favorable outcome and mortality), odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using DerSimonian and Laird random-effects models. Heterogeneity was evaluated using the Cochrane Q test and the I^2^ statistic, with an I^2^ > 40% and a p < 0.10 defining significant heterogeneity. All meta-analyses were performed using R Studio (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria) and Review Manager software (RevMan version 5.4.1; The Cochrane Collaboration, London, United Kingdom).
A frequentist random-effects framework was employed to compare multiple treatment strategies simultaneously. Treatments were ranked based on their estimated probability of being the most effective, using the surface under the cumulative ranking curve [25]. Results were presented as league tables, forest plots, and network diagrams.
Results
Study selection
A total of 938 articles were retrieved from database searches (PubMed: 277; Embase: 658; Cochrane Library: 3). After duplicate removal and abstract screening, 890 articles were excluded, leaving 48 for full-text review. Ultimately, 18 studies met the inclusion criteria (Fig. 1).Fig. 1. Preferred reporting items for systematic reviews and meta-analyses (PRIMSA) flow diagram. The diagram illustrates the study selection process according to the PRISMA guidelines. A total of 938 records were identified across three databases (PubMed, Embase, and Cochrane Library). After removal of duplicates and title/abstract screening, 48 articles were assessed fully for eligibility. Of these, 30 were excluded based on predefined inclusion and exclusion criteria, resulting in 18 studies included in the final qualitative synthesis
Baseline characteristics of cerebellar infarction population
The analysis involved 18 studies published between 1982 and 2024, collectively including 754 patients with SOCI (Germany [N = 4 studies], the United States [N = 4], Japan [N = 4], Italy [N = 2], France [N = 1], United Kingdom [N = 1], Türkiye [N = 1], and Germany-Austria [N = 1]) [4, 10, 15, 21, 29–31, 36, 39]. Sixteen studies were retrospective, one was prospective study, and one was a randomized controlled trial.
The mean patient age was comparable across groups (67.3 years in the medical cohort vs. 67.1 years in the surgical). Reported mean cerebellar infarct volume was smaller volume in the medical group (20.7 mL) than the surgical group (45.7 mL). Pre-interventional GCS scores were higher among medically managed patients (mean: 13.3) than in the surgical cohort (11). Among patients undergoing surgery, the mean time from symptom onset to surgery was 46.9 h Tables 1 and 2. Table 1. Baseline characteristics of included studies. Characteristics include the study type, national origin, intervention type, follow-up time, and outcome measure utilized. EVD: external ventricular drain; SDC: suboccipital decompressive craniectomy; N: necrosectomy; GCS: Glasgow come score; GOS: Glasgow outcome scale; mRS: Modified Rankin Scale; NR: not reported; RCT: randomized clinical trialStudyDesignCountryIntervention (n)Mean Age (Years)Follow-Up (Months)OutcomeMedicalEVDSDCEVD + SDCEVD + SDC + NSDC + NSurgicalMedical Won, 2024 [39] RetrospectiveGermanyNR71NRNRNR7166.3NR12mRS Kapapa, 2024 [10] RetrospectiveGermany21NRNR17NRNR69.580.1NRmRS Hernandez-Duran, 2024 [4] RetrospectiveGermanyNRNR43NRNR49653mRSKumral, 2023Prospective (RCT)Türkiye40NRNRNR32NR64.766.612mRS Wang, 2022 [36] RetrospectiveUnited States112386060NRDischarge Destination Taylor, 2020 [31] RetrospectiveUnited States652NR9NR1258.5NRNR Suyama, 2018RetrospectiveJapanNRNR59NRNR653mRS Tartara, 2018 [30] RetrospectiveItalyNRNR29NRNR64.733.8mRS Mostofi, 2013 [21] RetrospectiveFrance286163NRNR59.762.4NRGCSJuttler, 2009 [9]RetrospectiveUnited StatesNR9NR39NR86036mRS Kudo, 2007 [14] RetrospectiveJapanNR32314362.6NRGOS Raco, 2003 [24]RetrospectiveItaly25845NRNR56NRGOSKoh, 2000RetrospectiveUSA26621NRNRNR16mRS Jauss, 1999 [8] ProspectiveGermany-Austria3614304NRNR58.53mRS Mathew, 1995 [19] RetrospectiveUnited Kingdom3472NRNRNR57NRGOS Hornig, 1994 [6] RetrospectiveGermany16NRNRNRNR3061.2NRmRSAuer, 1986RetrospectiveJapan321NR7NRNR61NRNRTaneda, 1982RetrospectiveJapan5NRNR3NR759NRComplete RecoveryTable 2Baseline characteristics of included studies. Variables included the following: medical comorbidities, cerebellar infarct volume, time to surgery from symptom onset, and pre-interventional GCS. For cells with values separated by a slash, the total patient population was subcategorized by those who received medical therapy versus surgical therapy (the first value represents patient who received medical therapy, the second value for surgical therapy) AF: atrial fibrillation; HTN: arterial hypertension; DM: diabetes mellitus; GCS: Glasgow coma score; NR: not reportedStudyPatients (n)Medical Comorbidities (n)Hydrocephalus (n)Infarct Volume (mL)Time to Surgery (Hours)Pre-Intervention GCSMedical Therapy UtilizedMedicalSurgicalHTNDMDyslipidemiaAFMedicalSurgical Won, 2024 [39] NR142NR/115NR/42NRNR/32NRNR39.926.4NR/10.3NR Kapapa, 2024 [10] 211717/163/7NRNRNR25.852.848.5313.3/10.5Oxygenation, Prophylactic Anticoagulation Hernandez-Duran, 2024 [4] NR92NR/80NR/28NRNR/24NRNR45.527NR/10.5NRKumral, 2023403224/2117/1213/1116/12NR96.498.4NR12.8/8.4Antihypertensives, Anti-Edema Agents, Prophylactic Anticoagulation Wang, 2022 [36] 1123888/2848/1743/1815/8NR11.425.962.414/13.5Anti-Edema Agents Taylor, 2020 [31] 652148/1526/1125/10NR5/112546NR13.3/13Anti-Edema Agents Suyama, 2018NR14NR/9NR/4NRNR/8NR/12NR64.3NRNRNR Tartara, 2018 [30] NR11NRNRNRNRNRNRNR36.8NR/13.6NR Mostofi, 2013 [21] 2216NRNRNRNRNRNRNRNR12.9/11.2Antihypertensives, Anti-Edema Agents, AntiemeticsJuttler, 2009 [9]NR56NRNRNRNRNRNRNR72NR/13NR Kudo, 2007 [14] NR25NRNRNRNRNRNRNR55.2NR/6NR Raco, 2003 [24]2517NRNRNRNRNRNRNRNRNRAnti-Edema Agents, Prophylactic AnticoagulationKoh, 2000269NRNRNRNRNR/9NRNRNRNRAnti-Edema Agents, Hyperventilation Jauss, 1999 [8] 3648NRNRNRNRNRNRNRNRNRAnti-Edema Agents Mathew, 1995 [19] 349NRNRNRNRNRNRNRNR11Anti-Edema Agents Hornig, 1994 [6] 1630NRNRNRNRNRNRNRNRNRAnti-Edema AgentsAuer, 1986328NRNRNRNRNRNRNRNRNRNRTaneda, 1982510NRNRNRNR15NRNRNRNRNR
Variables associated with outcome
Cerebellar infarct volume
In the medical group, larger infarct volume was significantly associated with worse outcomes (estimate = 1.1441, p < 0.0001). In the surgical group, infarct volume (estimate = −0.3570, p = 0.3867) was not significantly associated with outcomes Figure 2.Fig. 2. Cerebellar infarct volume and outcome. For patients with infarcts > 51 mL, surgical intervention (61.48%, 95% CI: 46.06–74.91) was associated with significantly higher rates of favorable outcome compared with medical therapy 35.00%, 95% CI: 20.63, 51.68; p = 0.018). Each dot represents an individual study cohort included in the analysis
Glasgow coma scale score at presentation
In the surgical group, higher pre-interventional GCS showed a non-significant trend towards better outcomes (estimate = 0.0601, p = 0.5724) Figure 3.Fig. 3. Presenting glassgow coma scale score and outcome. Patients with GCS ≤ 13 demonstrated improved outcomes following surgical intervention, relative to medical management alone (p < 0.05). Each dot represents an individual study cohort included in the analysis
Age at presentation
Age was not significantly associated with outcomes in either the medical group (estimate = −0.0399, p = 0.3860) or the surgical group (estimate = −0.0284, p = 0.7495), although point estimates suggest a trend towards worse outcomes with increasing age Figure 4.Fig. 4. Age at presentation and outcome. Increasing age was associated with poorer outcomes across both treatment groups. As age increases, patients consistently experienced worse outcomes with surgical interventions than medical management alone (p < 0.05). Each dot represents an individual study cohort included in the analysis
Time of symptom onset to surgical intervention
Time from symptom onset to surgery in the surgical group had no significant impact on outcomes (estimate = −0.0021, p = 0.7911), indicating no measurable effect of surgical timing Figure 5.Fig. 5. Time to surgery and outcome. Surgery performed within the first 72 h of symptom onset did not significant influence outcome (p = 0.93). Each dot represents an individual study cohort included in the analysis
Favorable outcomes and mortality rate by intervention type
Combination therapy with suboccipital decompressive craniectomy, necrosectomy, and external ventricular drainage (SDC-N-EVD) conferred the greatest benefit. Compared with medical therapy, SDC-N-EVD increased odds of a favorable outcome by 3.1-fold (95% CI: 1.18–8.14; p < 0.05). The only surgical intervention found to statistically reduce odds of favorable outcome, relative to medical management, was a stand-alone SDC (p < 0.05). SDC-N-EVD exhibited improved mortality rates against all other treatment types except medical management Tables 1 and 2.
Treatment-ranking analysis demonstrated that SDC-N-EVD had the highest probability of yielding a favorable outcome, followed by (2) medial management, (3) SDC-N, (4) EVD, (5) SDC-EVD, and (6) SCD. Regarding mortality, SDC-N-EVD ranked first (lowest mortality), with medial management ranking second; while EVD alone afforded the worst mortality rate. In summary, per rank probabilities of all management strategies for SOCI, SDC-N-EVD ranked first for providing the greatest likelihood of resulting in a favorable outcome and reduced mortality Table 3. Table 3(A) Rank probability for favorable outcome. SDC-N-EVD exhibited the highest probability for a favorable outcome, followed by medical management. SDC alone, followed by SDC-EVD exhibited the two worst probabilities for favorable outcome. (B) Rank probability for mortality rate. SDC-N-EVD and medical management exhibited the highest probabilities for reduced mortality rate. EVD: external ventricular drain; N: necrosectomy; SDC: suboccipital decompressive craniectomy. Green shading indicates the intervention with the highest probability of having the most favorable outcome or reduced mortality rate (best rank), while red shading indicates the intervention with the greatest probability of being the worst outcome or greatest mortality rate (worst rank); light green (better rank) and red shading (worse rank) indicate high probabilities for intermediate probabilities
Length of stay by intervention type
SDC-N-EVD was also associated with shorter length of stay compared with other treatment strategies, albeit statistical significance was not consistently met given suspected underpowering of analyses (Table 4). Rank-probability analysis however confirmed SDC-N-EVD as most likely to reduce hospitalization length of stay, followed by medical therapy at second Table 5. Table 4. Length of stay odds per treatment cohort. Network meta-analysis for length of stay by indirect comparison of medical and surgical interventions. Overall, SDC-N-EVD exhibited improved odds of reducing length of stay compared to other treatment modalities, although statistical significance was not reached in each comparison. Odds ratio with 95% CI presented. *indicates statistical significance. EVD: external ventricular drain; N: necrosectomy; SDC: suboccipital decompressive craniectomyTable 5Rank probability for length of stay. SDC-N-EVD, followed by medical management yielded in the highest probability for reducing length of stay. Green shading indicates the intervention with the highest probability of being the most effective (best rank), while red shading indicates the intervention with the greatest probability of being the least effective (worst rank); light green (better rank) and red shading (worse rank) indicate high probabilities for intermediate probabilities of effectiveness. EVD: external ventricular drain; N: necrosectomy; SDC: suboccipital decompressive craniectomy
Discussion
Provided the variability in management strategies for SOCIs, our investigation sought to provide clarity on interventional thresholds and determine whether an optimal treatment strategy exits. Overall, patients with larger infarction volumes derived greater benefit with surgical management—specifically, when managed with the combined approach of SDC-N-EVD. SDC-N-EVD was associated with the highest likelihood of favorable outcomes, lower mortality, and shorter hospitalization. In contrast, the timing of surgery from symptom onset did not significant alter outcomes.
Medical versus surgical management
General comparison between medical and surgical cohorts exhibited no significant differences in outcome, yet when we stratified by intervention type, SDC-N-EVD exhibited a clear advantage over medical therapy. The improved outcomes from utilizing SDC-N-EVD is likely attributed to the combined effects of acutely addressing the hydrocephalus (i.e., lowering intracranial pressure), relieving posterior fossa mass effect, mitigating brainstem compression, and addressing altered cerebrospinal fluid dynamics postoperatively, while the necrosectomy may further attenuate the inflammatory sequelae of infarction [4, 7, 12, 22, 24].
On the contrary, standalone EVD was most likely to yield in mortality. The worse outcome is likely attributed to the risk of upward transtentorial herniation following ventricular decompression, which in turn can exacerbate brainstem compression [7, 12, 22, 24]. These findings underscore the importance of surgical comprehensiveness: interventions that address both mass effect and CSF circulation appear superior to temporizing measures alone.
Infarction volume
Our results highlight infarct volume as a pivotal factor in treatment selection. Favorable outcomes with medical management declined linearly with increasing infarct size, whereas surgical outcomes remained relatively stable. Surgery conferred significant benefit over medical therapy.
Prior investigations have also recognized the critical nature of infarct volume on surgical decision making [10, 39]. For instance, some have suggested even at smaller infarct volumes (35 mL or greater) better outcomes are experienced with surgical decompression than an EVD alone [39]. Although we did not stratify outcomes by infarct volume for each specific surgical modality, our results reinforced the limited role of EVD alone given worse outcomes; one can surmise such a premise, asa suboccipital decompression with necrosectomy directly addresses the culprit (i.e., infarcted swollen cerebellar tissue yielding in mass effect), while an EVD alone simply temporizes the consequences (hydrocephalus) of the underlying problem [10, 39]. Nevertheless, there are considerable nuances in management where a standalone EVD can be considered, depending on patient exam, infarct volume, and radiographic data [10, 39].
Pre-interventional GCS
Neurological status (i.e., clinical exam) remains a cornerstone of surgical decision making [17, 33]. Patients presenting with GCS ≤ 13 were more likely to benefit from surgery, whereas those with preserved consciousness (GCS 14–15) tended to fare better with medical management. Although direct comparisons with prior studies are limited, our results align with the American Heart Association/American Stroke Association guidelines recommending surgical intervention in patients with progressive neurological deterioration [37].
Patient age
While age was inversely correlated with favorable outcome across all treatment modalities, outcomes between surgical versus medical therapy did not differ significantly within age strata. These findings suggest age alone should not preclude surgical intervention when otherwise indicated. Prior literature also supports such a conclusion, as there are reports of acceptable surgical outcomes in older SOCI patients, while parallel data from supratentorial infarctions demonstrates age does not independently dictate treatment benefit [33, 34, 37]. Hence, age can be used to inform discussions on treatment decision-making with patients and family, but alone age should not exclude a patient from an intervention if warranted.
Time to surgery
Consistent with prior literature, our analysis did not identify difference in outcome between early and later surgical intervention—with outcomes equivalent if surgery was performed in the first 72 h [13, 16, 22, 23]. Although some have advocated for earlier decompression, current evidence—including American Heart Association/American Stroke Association guidelines—indicate the outcomes are primarily influenced by neurological status at the time of surgery, rather than precise timing, provided the intervention occurs prior to herniation [37].
Length of stay
Despite being the most invasive strategy, SCD-N-EVD was associated with both improved outcomes and shorter hospitalization. By definitively addressing the cerebellar infarct, such allows for directly alleviating mass effect, reducing hydrocephalus, and preventing further neurologic deterioration, transitioning the disease course towards expedited clinical recovery; whereas conservatively managed patients require graduate stabilization and hence prolonged intensive care unit monitoring [15, 39].
Limitations
There are several important limitations to note. The majority of included studies were retrospective in nature, with only one prospective cohort and a single randomized controlled trial, making the overall evidence base vulnerable to selection bias, incomplete data capture, and unmeasured confounding. Sample sizes were often small, and considerable heterogeneity existed across studies with respect to patient demographics, infarct volume thresholds, timing of intervention, surgical technique, and definitions of favorable outcome. The clinical and methodological diversity poses a challenge to the transitivity assumption required for network meta-analysis. Specifically, the indications for surgical intervention were not standardized; some centers operated prophylactically based on radiological criteria, while others adopted a wait-and-watch approach, reserving surgery for patients with clinical deterioration. Furthermore, variations in neurocritical care protocols—ranging from osmotherapy regimens to sedation strategies across different years and institutions—introduce a layer of clinical heterogeneity that may confound the direct and indirect comparisons between surgical modalities. While random-effects modeling was used to account for the above variability, there will nonetheless be residual heterogeneity in the final analysis.
Outcome reporting was inconsistent, with different studies employing various functional scales such as the Modified Rankin Scale or Glasgow Outcome Scale, and follow-up durations were frequently limited, thereby restricting the ability to assess long-term functional recovery, quality of life, or independence. Furthermore, the timing of surgery was not uniformly defined—some studies measured from symptom onset while others from hospital admission—and procedural details such as the extent of necrosectomy or the size of decompression were inconsistently reported, limiting comparability between surgical modalities. Restricting the analysis to English-language publications may also have introduced language bias, while publication bias remains possible despite funnel plot evaluation. Finally, most of the included studies were conducted in high-resource healthcare settings, which may limit generalizability to regions with fewer neurosurgical resources or different models of stroke care. These limitations highlight the need for larger, multicenter prospective studies and randomized controlled trials with standardized protocols to validate prognostic thresholds and refine treatment algorithms for space-occupying cerebellar infarctions.
Conclusion
In conclusion, our systematic review and meta-analysis suggest surgical intervention is associated with improved outcomes for patients with SOCIs who presented with larger infarct volumes. Among the evaluated surgical strategies, combined SDC–N–EVD exhibited the highest likelihood of favorable outcomes and reduced hospitalization. Age and timing of surgery did not significantly modify outcomes, suggesting that these factors should not serve as absolute contraindications to intervention when clinically indicated—however, these findings must be interpreted in light of the significant heterogenetic amongst included studies. Nevertheless, these findings support the development of standardized, evidence-based treatment algorithms, and underscore the need for prospective multicenter studies to validate prognostic thresholds and optimize patient selection for surgical management of SOCI.
Supplementary Information
Below is the link to the electronic supplementary material.ESM 1Supplementary Material 1 (DOCX 13.5 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Higgins JP et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 10.1136/bmj.d 592810.1136/bmj.d 5928 PMC 319624522008217 · doi ↗ · pubmed ↗
- 2Kumral, Emre and Dorukoğlu, Mesut and Orman, Mehmet and Özgiray, Erkin, Decompressive Craniectomy in Patients with Malignant Cerebellar Infarction a Randomized, Controlled Trial (Demci Trial). Available at SSRN: https://ssrn.com/abstract=4423441, 10.2139/ssrn.4423441
- 3Moher D, Liberati A, Tetzlaff J, Altman DG (2009) PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. P Lo S Med. 6(7):e 1000097. 10.1371/journal.pmed.100009710.1371/journal.pmed.1000097 PMC 270759919621072 · doi ↗ · pubmed ↗
- 4Raco A, Caroli E, Isidori A, Salvati M (2003) Management of acute cerebellar infarction: one institution's experience. Neurosurgery, 53(5), 1061–5. 10.1227/01.neu.0000088766.34559.3e 10.1227/01.neu.0000088766.34559.3e 14580272 · doi ↗ · pubmed ↗