T-Cell Receptor Excision Circle/Kappa-Deleting Recombination Excision Circle-Based Newborn Screening Program for Severe Combined Immunodeficiency in Kumamoto, Japan
Yuya Kinoshita, Jun Kido, Takaaki Sawada, Keishin Sugawara, Fumiko Nozaki, Tomoyuki Mizukami, Madoka Nishimura, Shinichiro Yoshida, Ryutaro Tsuru, Kimitoshi Nakamura

TL;DR
This study evaluates a new screening program in Japan using TREC and KREC measurements to detect severe immunodeficiencies in newborns.
Contribution
The study introduces a combined TREC/KREC-based newborn screening program for detecting T- and B-cell immunodeficiencies.
Findings
Three newborns (0.007%) were diagnosed with T-cell lymphopenia using TREC-based screening.
One newborn (0.008%) was diagnosed with X-linked agammaglobulinemia using combined TREC/KREC screening.
Maternal azathioprine exposure and low birth weight were found to affect TREC/KREC levels.
Abstract
Severe combined immunodeficiency (SCID) is a life-threatening hereditary disorder that requires early diagnosis and intervention. Therefore, this study aimed to evaluate the utility of T-cell receptor excision circle (TREC) and kappa-deleting recombination excision circle (KREC) measurements in newborn screening (NBS) for SCID and other primary immunodeficiencies in Kumamoto Prefecture, Japan. In a TREC-based NBS program (February 2019–March 2022, N = 43,658), six newborns (0.014%) underwent immunological testing, and three (0.007%) were diagnosed with T-cell lymphopenia. In a subsequent combined TREC/KREC-based NBS program (April 2022–March 2023, N = 12,335), eight newborns (0.065%) required further testing, and one (0.008%) was diagnosed with X-linked agammaglobulinemia. Decreased KREC levels were observed in two newborns exposed to maternal azathioprine (AZP). The TREC levels tended…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
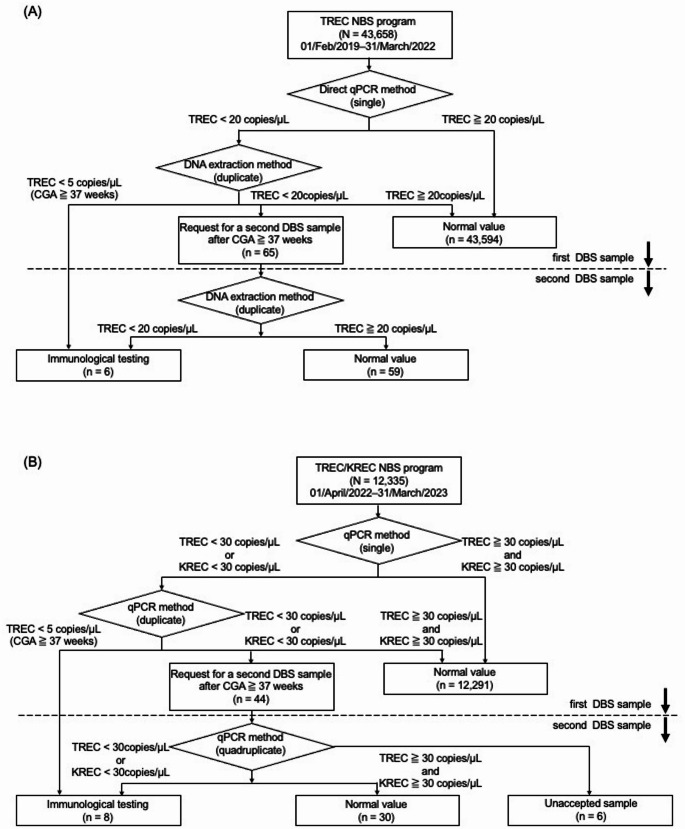 Figure 1
Figure 1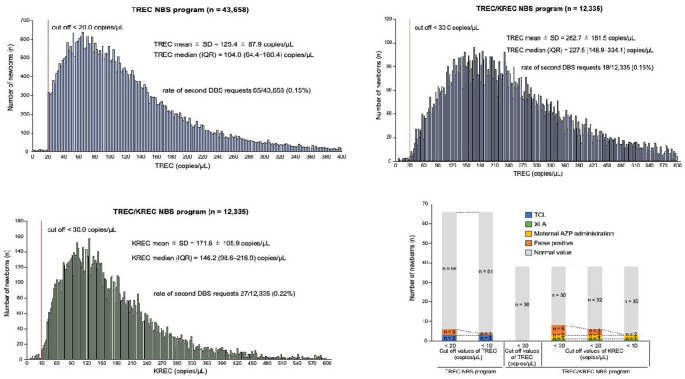 Figure 2
Figure 2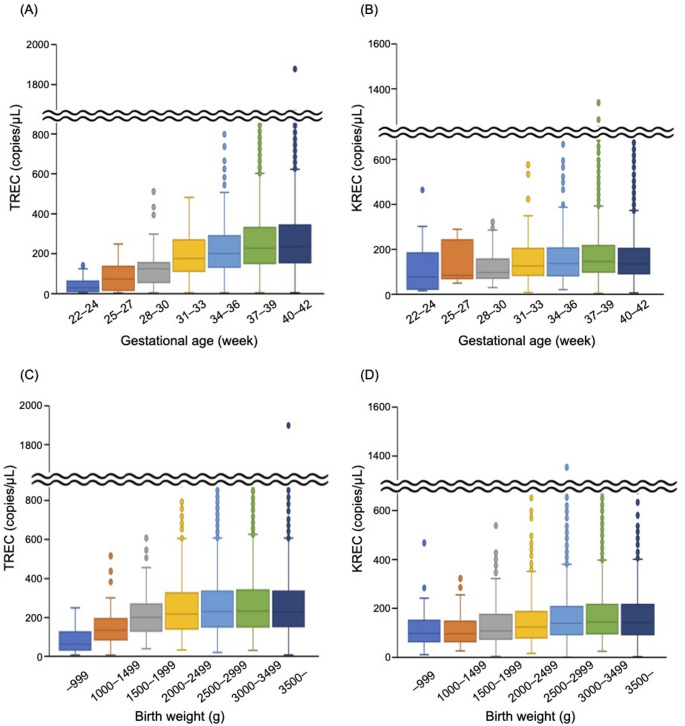 Figure 3
Figure 3- —Kumamoto University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmunodeficiency and Autoimmune Disorders · Congenital Ear and Nasal Anomalies · Blood disorders and treatments
Introduction
Severe combined immunodeficiency (SCID) is a life-threatening hereditary immunodeficiency disorder that typically occurs during early infancy. Although affected neonates may appear healthy at birth, severe opportunistic infections often develop during early infancy, and failure to thrive is frequently observed. Adverse outcomes, including secondary infections from live vaccines, have also been reported [1].
SCID arises from various genetic mutations, such as defects in the interleukin-2 receptor gamma chain, adenosine deaminase, and recombination-activating genes 1 and 2. These defects primarily result in T-cell dysfunction and, in some cases, may also impair B-cell or natural killer (NK) cell function [2]. Approximately two decades ago, the incidence of SCID was estimated to be about 1 in 100,000 live births [1]. More recently, Wakamatsu et al. identified two patients with SCID among the 137,484 live births in Aichi Prefecture, Japan, between April 2017 and December 2021 [3].
Hematopoietic stem cell transplantation (HSCT) remains the most effective treatment for SCID. Survival is significantly improved when HSCT is performed before the onset of infections, highlighting the critical importance of early diagnosis and intervention [4, 5]. In recent years, gene therapy has emerged as a viable treatment option for X-linked SCID, with improved vector safety compared with previous trials [2]. Newborn screening (NBS) programs for SCID have been introduced in several countries [6–13].
Globally, the T-cell receptor excision circle (TREC)—a circular DNA fragment generated during T-cell receptor gene rearrangement in thymocytes—is widely used as a marker in SCID NBS programs [1]. TREC levels reflect the output of newly formed T lymphocytes, and significantly reduced TREC levels indicate impaired T-cell production. In addition to TREC, the kappa-deleting recombination excision circle (KREC)—a byproduct of immunoglobulin kappa light-chain gene rearrangement in developing B lymphocytes—has been incorporated in some SCID NBS protocols [14].
KREC-based screening facilitates the detection of B lymphocytopenia; however, its application remains controversial due to higher false-positive rates [15].
Since October 2020, the attenuated live rotavirus vaccine has been included in Japan’s routine immunization schedule and is administered to infants between 6 and 14 weeks of age [16]. The administration of attenuated live rotavirus vaccines to patients with SCID may lead to chronic gastroenteritis, resulting in severe stunting and wasting, and poses a significant risk of life-threatening complications despite intensive medical care [17, 18]. Considering this risk, the Japanese government has acknowledged the necessity of incorporating SCID into the NBS program [19, 20] and has announced substantial increases in funding to support NBS expansion and enhance follow-up care [21].
Therefore, this study aimed to evaluate the utility of a TREC-based NBS program conducted between February 2019 and March 2022, followed by a combined TREC/KREC-based program from April 2022 to March 2023. We also aim to present the results of our SCID NBS program and discuss its feasibility and characteristics.
Materials and Methods
NBS Program
In 2019, Japan’s NBS program included more than 20 disorders, primarily involving amino acid, organic acid, and fatty acid metabolism disorders, as well as endocrine conditions such as congenital hypothyroidism and congenital adrenal hyperplasia [22, 23]. In this program, blood samples were collected from the heel of newborns between days 4 and 6 of life. As an expanded screening initiative in Kumamoto Prefecture, Japan, TREC- and TREC/KREC-based NBS programs were conducted from February 1, 2019, to March 31, 2022, and from April 1, 2022, to March 31, 2023, respectively. Kumamoto Prefecture has a population of approximately 1.7 million (Fig. 1A–B). Prior to the initiation of the TREC-based NBS program, NBS for lysosomal storage disorders had already been implemented in the prefecture [24–27]. Both the TREC- and TREC/KREC-based NBS programs were performed voluntarily with parental cooperation. Written informed consent was obtained from the parents and legal guardians of all participating newborns. The consent rates were 96.5% for the TREC-based program and 96.1% for the TREC/KREC-based program. Fig. 1Summary of the TREC- and TREC/KREC-based NBS programs. Flowcharts of the (A) TREC- and (B) TREC/KREC-based NBS programs. In the TREC-based NBS program, the TREC cutoff was set at 20 copies/µL. In the TREC/KREC-based NBS program, both the TREC and KREC cutoff values were set at 30 copies/µL. For samples collected from newborns with a corrected gestational age (CGA) of ≥ 37 weeks, the emergency TREC cutoff was set at 5 copies/µL TREC, T-cell receptor excision circle; KREC, kappa-deleting recombination excision circle; NBS, newborn screening; qPCR, quantitative polymerase chain reaction; CGA, corrected gestational age
TREC Measurement
TREC values were measured using dried blood spots (DBSs) collected for routine public mass-screening tests. Discs measuring 1.2 mm in diameter were punched from each DBSs and placed into a 96-well PCR plate (Watson Co., Ltd., Tokyo, Japan). Each well was filled with 20 µL of 0.4 M potassium chloride in phosphate-buffered saline, heated at 50℃ for 3 min, and centrifuged. The supernatant was subsequently discarded, and 20 µL of reaction mixture was added to each well. This mixture contained amplification primers, a reporter dye/quencher-labeled probe, and BIOTAQ™ HS DNA polymerase in Ampdirect^®^ Plus (Shimadzu Co., Kyoto, Japan) (Additional file 1). Quantitative polymerase chain reaction (qPCR) was performed using a QuantStudio^Ⓡ^5 system (Thermo Fisher Scientific K.K., Tokyo, Japan) with the following program: 95℃ for 10 min, followed by 45 cycles of 94℃ for 30 s and 60℃ for 1 min. TREC values were quantified using a TREC copy number standard prepared by a contract laboratory (Nihon Gene Research Laboratories Inc., Sendai, Japan). This qPCR protocol without DNA extraction is referred to as the “direct PCR method.” A preliminary study determined that the cutoff value of 30 copies/µL for TREC was too high; therefore, the threshold was set at 20 copies/µL. If the TREC value obtained using the direct PCR method fell below 20 copies/µL, a 3.2-mm disc was punched from the same DBS, and genomic DNA was extracted using the NucleoSpin Tissue XS kit (TAKARA Bio Inc., Shiga, Japan). The TREC levels were remeasured by qPCR (DNA extraction method). Although the primary cutoff was set at 20 copies/µL, immediate immunological testing was promptly performed if the TREC value was < 5 copies/µL in samples obtained from newborns with a corrected (CGA) of ≥ 37 weeks. This emergency criterion was introduced midway through the program. If the TREC value was < 20 copies/µL, a second DBS sample was requested after the newborn reached a CGA of 37 weeks to reduce false-positive results. Immunological testing was required if the TREC values remained < 20 copies/µL in the second DBS sample.
TREC/KREC Measurement
TREC and KREC values were similarly measured from DBSs collected for other routine screening tests using mass spectrometry. Discs measuring 1.5 mm in diameter were punched from each DBS, and analysis was performed using the NeoSMAAT TREC/KREC^®^ T/K/S kit (Sekisui Medical Co., Ltd., Tokyo, Japan), which is also applicable for NBS for spinal muscular atrophy [28, 29]. Measurements were initially obtained by qPCR using a single test per sample in accordance with the manufacturer’s instructions. A preliminary study demonstrated that the previous cutoff of 20 copies/µL for TREC corresponded to 30 copies/µL with the new TREC/KREC method, resulting in equivalent second DBS request rates of 0.15%. Accordingly, the TREC cutoff was set at 30 copies/µL (Fig. 2A and B). The initial cutoff for KREC was tentatively set at 30 copies/µL, with adjustments planned during program operation if necessary. If the TREC or KREC value was < 30 copies/µL, qPCR was repeated in duplicate. Immediate immunological testing was performed when the TREC value was < 5 copies/µL in the samples obtained from newborns with a CGA of ≥ 37 weeks. When either TREC or KREC values were < 30 copies/µL, a second DBS sample was requested after the newborn reached a CGA of 37 weeks, and measurements were repeated in quadruplicate to reduce false-positive results. Immunological testing was required if either the TREC or KREC values in the second DBS sample remained < 30 copies/µL.
Fig. 2 TREC and KREC distributions and cutoff evaluation in NBS programs. (A) Histogram of TREC levels in the TREC- and (B) TREC/KREC-based NBS programs. (C) Histogram of KREC levels in the TREC/KREC-based NBS program. (D) Results from the second DBS samples in the TREC- and TREC/KREC-based NBS programs TREC, T-cell receptor excision circle; KREC, kappa-deleting recombination excision circle; NBS, newborn screening; IQR, interquartile range; TCL, T-cell lymphopenia; XLA, X-linked agammaglobulinemia; AZP, azathioprine
Immunological testing
Newborns who met the criteria for immunological testing underwent flow cytometric analysis in addition to routine blood tests. The cluster of differentiation (CD) 3+, CD4+, CD8+, CD19+, CD45+, CD56+, and CD45RA+ naïve T-cells were evaluated. Genetic analyses were performed for patients with T-cell lymphopenia (TCL) or B-cell deficiency (BCD), except in those with known underlying disorders such as 22q11.2 deletion syndrome or secondary causes such as postoperative chylothorax. Initial genetic screening was conducted using targeted next-generation sequencing (NGS) panels for SCID-related genes (20 genes) or BCD genes. If no pathogenic variants were identified, extended panels covering approximately 400 immune-related genes or whole-exome sequencing (WES) were performed.
SCID was defined based on the classification established by the Primary Immune Deficiency Treatment Consortium [30]. TCL was defined as a T-cell count of < 1,500/µL [31]. Complete DiGeorge syndrome (cDGS), a non-SCID primary immunodeficiency, was defined as a condition with a CD3^+^ or naïve T-cell count of < 50/µL resulting from severe thymic hypoplasia or aplasia [32]. BCD was defined as a CD19^+^ cell count of < 2% of the total lymphocytes, and X-linked agammaglobulinemia (XLA) was diagnosed by confirming a BTK mutation via genetic testing [33].
Flow Cytometric Analysis
Flow cytometric analysis was performed using a BD FACSCanto™ Ⅱ flow cytometer (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) to quantify the absolute counts of CD3^+^ T-cells, CD4^+^ T-cells, CD8^+^ T-cells, CD45RA^+^ T-cells (naïve T-cells), CD19^+^ B-cells, and CD56^+^ NK cells. Two reagent kits were used in accordance with the manufacturer’s instructions: the BD Multitest™ 6-Color TBNK Kit (cat. no. 662967; BD Biosciences, San Jose, CA, USA) and BD Multitest™ Anti-Human CD45RA FITC/CD45RO PE/CD3 PerCP/CD4 APC (cat. no. 340751; BD Biosciences, San Jose, CA, USA).
Statistical Analysis
Statistical significance was evaluated using the Mann–Whitney U test. All analyses were performed using GraphPad Prism (GraphPad Software Inc., San Diego, CA, USA). Box-and-whisker plots were generated in Microsoft Excel, with boxes representing the interquartile range (IQR) between the 25th and 75th percentiles and horizontal lines indicating the median. Whiskers extended to the smallest and largest data points within 1.5 × IQR below the 25th percentile or above the 75th percentile, excluding outliers. Data points beyond the whiskers were considered outliers and were plotted individually. Values reported as < 6.7 copies/µL were assigned a value of 6.7 copies/µL for statistical analyses and plotting.
Ethics Statements
This study’s was approved by the Ethics Committee of Kumamoto University (approval no. 2018; approval date: August 18, 2015). Written informed consent was obtained from the parents or legal guardians of all participating newborns.
Results
Setting of the TREC- and TREC/KREC-based NBS Programs
Histograms of TREC levels from the TREC-based (N = 43,658) and TREC/KREC-based (N = 12,335) NBS programs were plotted to evaluate TREC distributions (Fig. 2A–C). In the TREC-based NBS program, the TREC level (mean ± standard deviation (SD)) and median (IQR) were 125.4 ± 87.9 and 104.0 (64.4–160.4) copies/µL, respectively. With a TREC cutoff set at 20.0 copies/µL, second blood samples were requested for 65 of 43,658 newborns (0.15%).
In the TREC/KREC-based NBS program, the TREC level (mean ± SD) and median (IQR) were 262.7 ± 161.5 and 227.5 (148.9–334.1) copies/µL, respectively. With a TREC cutoff of 30.0 copies/µL, second DBS samples were requested for 18 of 12,335 newborns (0.15%). Meanwhile, the KREC level (mean ± SD) and median (IQR) were 171.6 ± 105.9 and 146.2 (98.6–216.9) copies/µL, respectively. Using a KREC cutoff of 30.0 copies/µL, second DBS samples were requested for 27 of 12,335 newborns (0.22%). As this program combined TREC and KREC screening, the overall second DBSs were requested for 44 of 12,335 newborns (0.36%). Although the two programs applied different TREC cutoff values owing to methodological differences, the second DBS sampling rates were nearly identical. The median TREC levels in the TREC/KREC-based NBS program were nearly twice as high as those observed in the TREC-based NBS program.
TREC-based NBS Program
In the TREC-based NBS program (Fig. 1A), 65 newborns (0.15%) exhibited low TREC levels (< 20 copies/µL) in their DBSs. Upon repeat testing using the same DBSs, six newborns (0.014%) continued to show consistently abnormal TREC levels and subsequently underwent immunological evaluation. Of these, three had immunological abnormalities (Table 1).
Table 1. Summary of Newborns Who Underwent Immunological Testing as Part of the TREC NBS ProgramPatient No.GenderInformation at the time of initial blood samplingNBS TREC(copies/µL)underlying diseaseCD3^+^T cellCD4^+^ T cellCD8^+^ T cellNaïve T cellImmunological diagnosisLive vaccineoutcome BW (g)
CAG (weeks)
1st
2nd
(/µL)
(/µL)
(/µL)
(/µL) T1Female2,6124115.511.7Miller-Dieker Syndrome2,3951,7895371,327no abnormalitiesEligibleCompletion of follow-upT2Male2,802382.5NDnothing504250135204TCL (c.42 C > A, p.C14*, homozygous )contraindicatedIVIG therapy Oral TMP-SMX therapyT3Male3712317.515.9ELBW CLD2,9991,8918891,233no abnormalitieseligibleCompletion of follow-upT4Male2,4823913.37.0nothing4,3391,7782,2711,197no abnormalitieseligibleCompletion of follow-upT5Male2,388401.71.1DORV VSD PS3191909597TCL due to chylothoraxcontraindicatedUndergoing treatment at another hospitalT6Female2,31237ND-CHARGE syndrome8010CHARGE/cDGS (c.2527 C > T, p.R858*, heterozygous)contraindicatedHSCTTREC T-cell receptor excision circle; NBS newborn screening; BW body weight; CAG corrected gestational age; ND no data; ELBW extremely low birth weight; CLD chronic lung disease; DORV double outlet right ventricle; VSD ventricular septal defect; PS pulmonary stenosis; TCL T-cell lymphopenia; cDGS complete DiGeorge syndrome; IVIG intravenous immunoglobulin; TMP-SMX trimethoprim-sulfamethoxazole; HSCT hematopoietic stem cell transplantation
- Patient T2 presented with 504 CD3^+^, 250 CD4^+^, 135 CD8^+^, and 204 naïve T-cells/µL, leading to the diagnosis of TCL. A homozygous nonsense mutation in the PTCRA gene (c.42 C > A, p.C14*) was identified through genetic analysis [34]. Live vaccines were contraindicated, and the patient received intravenous immunoglobulin and oral trimethoprim-sulfamethoxazole.
- Patient T5 had an underlying congenital heart disease (CHD), including double-outlet right ventricle, ventricular septal defect, and pulmonary stenosis. Immunological testing revealed 319 CD3^+^, 190 CD4^+^, 95 CD8^+^, and 97 naïve T-cells/µL, confirming TCL. Postoperative chylothorax following CHD surgery was identified as the cause of TCL. Live vaccines were contraindicated, and the patient continued CHD management at another hospital.
- Patient T6 had only 8 CD3^+^, 0 CD4^+^, 1 CD8^+^, and 0 naïve T-cells/µL. The patient presented with CHD, coloboma, choanal atresia, growth retardation, external ear hypoplasia, and hearing loss. Sanger sequencing identified a heterozygous pathogenic variant c.2527 C > T (p.R858*) in CHD7, confirming the diagnosis of CHARGE syndrome. Additional findings included hypoparathyroidism, thymic aplasia, and TCL, consistent with cDGS. Live vaccines were contraindicated, and the patient subsequently underwent successful HSCT [35].
TREC/KREC-based NBS Program
In the TREC/KREC-based NBS program (Fig. 1B), 44 newborns (0.36%) exhibited low TREC (< 30 copies/µL) or KREC (< 30 copies/µL) levels. Repeat testing using the same DBSs identified eight newborns (0.065%) with persistently abnormal KREC levels, who subsequently underwent immunological testing. Among these, one was diagnosed with a BCD (Table 2).
Table 2. Summary of Newborns Who Underwent Immunological Testing as Part of the TREC/KREC NBS ProgramPatient No.GenderInformation at the time of initial blood samplingNBS TREC(copies/µL)NBS KREC (copies/µL)underlying diseaseCD3^+^T cellCD4^+^ T cellCD8^+^ T cellNaïve T cellCD19(+)B cellImmunological diagnosisLive vaccineoutcome BW (g)
CAG (weeks)
1st
2nd
1st
2nd
(/µL)
(/µL)
(/µL)
(/µL)
(/µL)
(%) TK1Female2,56038133.9171.92.93.2Maternal AZP administration for scleroderma4,4443,1949093,095117819.7no abnormalitieseligibleCompletion of follow-upTK2Male3,48238349.5852.14.64nothing6,0454,6221,1704,49370.1XLA-MTS (c.201_1800del)contraindicatedSCIG therapyTK3Female2,66841371.7316.416.414nothing9,2046,4122,6086,2844714.1no abnormalitieseligibleCompletion of follow-upTK4Male2,65639250.1214.317.119.7nothing4,9733,8261,0283,7761922.9no abnormalitieseligibleCompletion of follow-upTK5Male3,51040129.1200.124.322.2nothing4,3193,1221,0633,0102455.1no abnormalitieseligibleCompletion of follow-upTK6Male2,2453665.3112.922.428.621 trisomy2,9452,0198891,9851023.1no abnormalitieseligibleCompletion of follow-upTK7Male3,2774020.350.6180.113.4APVR3,4691,9661,4301,83863711.4no abnormalitieseligiblefollow-upTK8Female2,7444088.8112.66.93.3Maternal AZP administration for UC2,7701,9657291,94969518.2no abnormalitieseligiblefollow-upTREC T-cell receptor excision circle; KREC kappa-deleting recombination excision circle; NBS newborn screening; BW body weight; CAG corrected gestational age; AZP azathioprine; UC ulcerative colitis; XLA X-Linked Agammaglobulinemia; MTS Mohr-Tranebjaerg syndrome; SCIG subcutaneous immunoglobulin
- Patient TK2 demonstrated a markedly reduced CD19^+^ B-cell count (7/µL, accounting for 0.1% of lymphocytes) with undetectable serum immunoglobulin A (< 2 mg/dL) and M (< 3 mg/dL) levels. Genetic analysis revealed a gross deletion involving BTK and TIMM8A, consistent with XLA and Mohr–Tranebjaerg syndrome. Live vaccines were contraindicated, and the patient received subcutaneous immunoglobulin replacement therapy.
- Among the remaining seven newborns, two were born to two mothers who received azathioprine (AZP) therapy during pregnancy for scleroderma and ulcerative colitis. None of the newborns exhibited BCD, and both demonstrated spontaneous recovery of B-cell ratios over time.
Re-evaluation of Cutoff Levels in the Second Measurement Using the DNA Extraction Method
Cutoff levels were re-evaluated to assess false-positive rates in the second measurement using the DNA extraction method (Fig. 2D). In the TREC-based NBS program, the false-positive rate was 3/65 (4.62%). This rate would have decreased to 1/65 (1.54%) without missing any TCL cases if the TREC cutoff had been lowered from 20 to 10 copies/µL. In the TREC/KREC-based NBS program, the false-positive rate for TREC was 0/38 (0%). However, the TREC cutoff could not be fully validated as no abnormal TREC levels or TCL cases were detected.
The total false-positive rate for KREC was 5/38 (13.2%). Notably, this system successfully identified a patient with decreased KREC levels associated with maternal AZP administration. If the KREC cutoff had been lowered from 30 to 20 copies/µL or 10 copies/µL, the false-positive rates would have decreased to 3/38 (7.9%) and 0/38 (0%), respectively, without missing any XLA cases and maternal AZP-associated reduced KREC levels.
Change in TREC and KREC Levels Based on Gestational Age or Birth Weight
The TREC and KREC levels in the TREC/KREC-based NBS program were analyzed based on GA to determine the optimal timing for retesting (Fig. 3A and B). The TREC levels were generally lower in more premature infants, with significant differences (Table 3). By contrast, no clear correlation was identified between KREC levels and GA; however, the KREC levels at a GA of 28–30 weeks were significantly lower than those at a GA of 40–42 weeks. The relationship between TREC/KREC levels and birth weight was also examined (Fig. 3C and D). Both the TREC and KREC levels were generally lower in newborns with low birth weights. Specifically, levels in newborns weighing < 2,000 g were significantly lower than those in newborns weighing > 3,000 g (p < 0.001, respectively).
Fig. 3 TREC and KREC levels based on gestational age and birth weight in the NBS program. Box-and-whisker plots of (A) TREC and (B) KREC levels by gestational age. Box-and-whisker plots of (C) TREC and (D) KREC levels by birth weight TREC, T-cell receptor excision circle; KREC, kappa-deleting recombination excision circle; NBS, newborn screening
Table 3. Results of TREC/KREC NBS Program in Relation to Variables Gestational Age and Birth Weight N (%)TREC (copies/µL) p KREC (copies/µL) p Gestational age (weeks)22–24100.0828.95 [12.93–58.95]< 0.000180.20 [35.35–139.30]n.s.25–27150.1269.80 [32.75–134.45]< 0.000188.10 [72.35–221.55]n.s.28–30510.41125.10 [60.60–153.85]< 0.0001100.30 [76.55–159.35]0.001831–33710.58179.70 [123.30–268.40]< 0.0001129.30 [92.95–208.90]n.s.34–364143.36200.00 [132.10–290.05]< 0.0001141.10 [86.40–211.40]n.s.37–39735759.77227.50 [148.40–331.70]0.0013150.90 [102.20–222.00]< 0.000140–42439035.67234.30 [154.20–344.85]1139.80 [95.00–209.15]1 Birth weight (g) –999320.2661.60 [33.10–123.60]< 0.0001104.10 [71.73–155.23]< 0.00011000–1499610.50133.40 [84.30–192.60]< 0.0001101.90 [70.50–145.30]< 0.00011500–19991311.06199.90 [129.35–266.70]0.0005114.40 [81.10–181.10]< 0.00012000–24997796.32217.50 [140.20–324.75]0.0415129.70 [85.05–193.70]< 0.00012500–2999447636.34229.45 [151.50–333.55]n.s.144.90 [98.38–214.00]n.s.3000–3499526642.75231.10 [151.30–340.50]n.s.151.10 [101.73–222.65]n.s.3500–157312.77227.40 [151.90–333.20]1148.90 [99.50–223.20]1The p values were calculated by comparing with newborns whose gestational age 40–42 weeks or birth weight 3500 g or moreTREC, T-cell receptor excision circle; KREC, kappa-deleting recombination excision circle; NBS, newborn screening
Discussion
A TREC-based NBS program and a combined TREC/KREC-based NBS program were implemented as part of the NBS system for the detection of SCID. Accordingly, three newborns with TCL were identified in the TREC-based NBS program, and one with XLA was identified in the TREC/KREC-based NBS program. Live vaccines were contraindicated in four newborns, which enabled the prevention of potentially severe complications and early medical interventions. Similar to SCID, both TCL and XLA require early diagnosis and treatment owing to the high susceptibility of affected individuals to infections. Therefore, the NBS programs proved useful in the early detection and management of these conditions.
The economic advantages of SCID NBS programs, in addition to their clinical benefits, have been reported in other countries [7, 12]. Based on the present findings, SCID NBS programs are both clinically practical and economically beneficial.
The false-positive rates of the screening programs were notably low: 0.007% (3/45,658) and 0.06% (5/12,335) in the TREC-based NBS program and TREC/KREC-based NBS program. One newborn with trisomy 21 (Patient TK6 in Table 2) was identified. Consistent with previous SCID NBS studies, many patients with chromosomal abnormalities—such as trisomy 2—exhibit TREC levels below the cutoff threshold [3, 6]. As illustrated in Fig. 2D, the false-positive rate could potentially be reduced by adjusting the cutoff values for TREC and KREC without overlooking true immunodeficiency cases. However, appropriate adjustment is essential as cutoff levels may vary depending on the assay method. The median TREC levels observed in the TREC/KREC-based NBS program were nearly twice those measured in the TREC-based NBS program. To confirm that this difference was due to assay variability rather than differences in the screened population, TREC levels were compared in an identical set of samples (n = 413) analyzed using both assay systems. The average TREC value measured by the TREC-only assay was 149.1 copies/µL, whereas the corresponding value measured by the combined TREC/KREC assay was 239.8 copies/µL. These findings confirm that the observed difference in TREC values is attributable to the differences in the measurement systems rather than variations in the screened population.
In our study, two newborns (TK1 and TK8) exhibited low KREC levels but normal TREC levels due to maternal AZP administration. Two studies reported low KREC levels but normal TREC levels, which normalized upon follow-up, in newborns exposed to maternal AZP [15, 36]. Conversely, other studies have described AZP-exposed newborns with low TREC levels (KREC data unavailable), which subsequently normalized [37, 38]. These findings suggest that maternal AZP exposure during pregnancy may impair fetal TREC and/or KREC production, particularly in fetuses with low thiopurine S-methyltransferase activity—the enzyme responsible for metabolizing AZP [39, 40]. In vitro studies have indicated that B-cells are highly sensitive to AZP, whereas helper T-cells are relatively resistant [41]. This differential sensitivity may account for the observed discrepancies between TREC and KREC levels.
Some previous TREC/KREC-based NBS programs that incorporated KREC measurement did not identify any patient with immunodeficiency based solely on KREC abnormalities [3, 14]. By contrast, the TREC/KREC-based NBS program in Seville (Spain) detected two patients with XLA who had normal TREC levels, and the program in the Czech Republic identified 10 patients with agammaglobulinemia who also had normal TREC levels [36, 42]. In our program, one patient with XLA was diagnosed based on an isolated KREC abnormality despite normal TREC levels. These findings indicate that TREC/KREC measurement can facilitate the early detection of XLA as well as other immunodeficiencies, including non-XLA hypogammaglobulinemia, Nijmegen breakage syndrome, late-onset adenosine deaminase deficiency, and IKZF-related combined immunodeficiency [43–46]. Therefore, the combined evaluation of TREC and KREC represents a valuable approach in NBS programs.
A second DBS sample was requested from infants with a GA of ≥ 37 weeks, in accordance with the previous studies reporting lower TREC levels in preterm neonates [11, 47–50]. Although birth weight was not employed as a criterion for retesting, infants with low birth weight in this study exhibited lower TREC levels, consistent with a previous study [50]. The relationship between KREC levels and GA or birth weight has not yet been fully elucidated. Two studies reported that KREC levels tended to be lower in more premature and low birth weight infants [36, 51]. The present study demonstrated that TREC levels were generally lower in more premature infants and those with low birth weight, whereas KREC levels were significantly lower in infants with low birth weight compared with those with normal birth weight, with no clear correlation between KREC levels and GA. These findings suggest that birth weight may be more closely associated with KREC levels compared with GA.
In conclusion, a large-scale TREC- and TREC/KREC-based NBS program was implemented in Japan, resulting in the identification of three patients with TCL and one with XLA. The TREC/KREC-based NBS program represents a powerful tool for detecting immunodeficiencies affecting T- or B-cell function. However, careful interpretation is warranted when evaluating these biomarkers in newborn DBS samples, as factors such as maternal AZP administration, low GA, and low birth weight may influence TREC and/or KREC copy numbers.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ministry of Health. (2024). Routine immunization of rotavirus vaccine. Ministry of Health, Labour and Welfare.
- 2Ministry of Health (2024). Guidelines for the demonstration project on newborn mass screening tests. Tokyo. Retrieved from chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.cfa.go.jp/assets/contents/node/basic_page/field_ref_resources/d 4a 9b 67b-acbd-4e 2a-a 27a-7e 8f 2d 6106 dd/bc 621dc 0/20240625_policies_boshihoken_tsuuchi_2024_52.pdf
- 3Ministry of Health (2024). Application guidelines for the demonstration project on newborn mass screening tests. Retrieved April 13, 2025, from chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.cfa.go.jp/assets/contents/node/basic_page/field_ref_resources/d 4a 9b 67b-acbd-4e 2a-a 27a-7e 8f 2d 6106 dd/765d 9d 3f/20240625_policies_boshihoken_tsuuchi_2024_50.pdf
- 4Ministry of Health (2025). Overview of the fiscal year 2025 budget for maternal and child health measures. Retrieved April 13, 2025, from chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.cfa.go.jp/assets/contents/node/basic_page/field_ref_resources/ff 38becb-bbd 1-41f 3-a 95e-3a 22ddac 09d 8/ee 8603 e 9/20250401_policies_boshihoken_156.pdf
- 5Japanese Society for Neonatal Screening (2013). Overview of the National Newborn Mass Screening Program (Results of a Health and Labour Sciences Research Grant) [in Japanese]. Japanese Society for Neonatal Screening. Retrieved July 24, 2025, from https://www.jsms.gr.jp/download/14_1_20131028.pdf
- 6Japanese Society for Neonatal Screening (2013). Diseases Detectable by Tandem Mass Spectrometry (Results of a Health and Labour Sciences Research Grant) [in Japanese]. Japanese Society for Neonatal Screening. Retrieved July 24, 2025, from https://www.jsms.gr.jp/download/14_3_1_20131028.pdf
- 7Smith, et al. (2024). X-linked agammaglobulinemia. In Gene Reviews® [Internet]. University of Washington.