Quantitative anatomy of the fourth ventricle floor: a cadaveric morphometric study
Ufuk Erginoglu, Umid Sulaimanov, Irem Uslu, Cagdas Ataoglu, Abdullah Keles, Abdurrahman Aycan, Mustafa K. Baskaya

TL;DR
This study provides detailed measurements of the fourth ventricle floor in human brainstems to help improve surgical planning.
Contribution
The study is the first to quantitatively define the hypoglossal and vagal trigones on the fourth ventricle floor.
Findings
The facial colliculus divides the floor into symmetrical rostral and caudal segments (~43% each).
The hypoglossal and vagal trigones occupy 25.44% and 12.69% of the caudal floor length.
Lateral recess lengths and striae medullares bundle counts showed statistically significant asymmetry.
Abstract
The floor of the fourth ventricle contains critical surface landmarks overlying brainstem nuclei. Despite advances in microsurgical techniques, detailed morphometric data on these landmarks remain limited. To perform a morphometric analysis of the fourth ventricle floor using cadaveric specimens, with emphasis on dimensions, symmetry, and proportional relationships relevant to surgical planning. Forty formalin-fixed adult human brainstems were used. Sixteen anatomical parameters were assessed, including twelve linear distances and four qualitative observations. Key landmarks—including the facial colliculus, sulcus limitans, striae medullares, and the hypoglossal and vagal trigones—were measured under magnification. Anatomical ratios were calculated, and findings were compared to prior cadaveric studies. The mean floor length and width were 33.58 ± 2.49 mm and 20.0 ± 1.83 mm,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1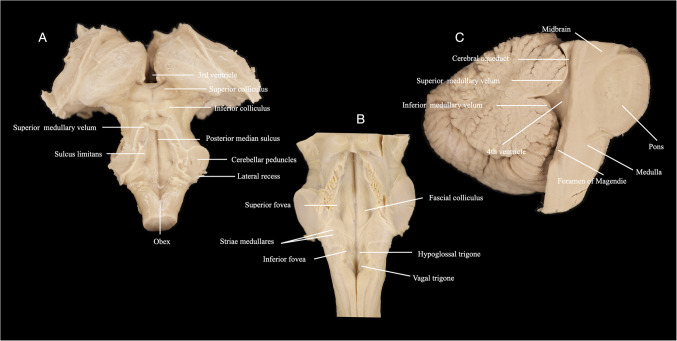 Figure 2
Figure 2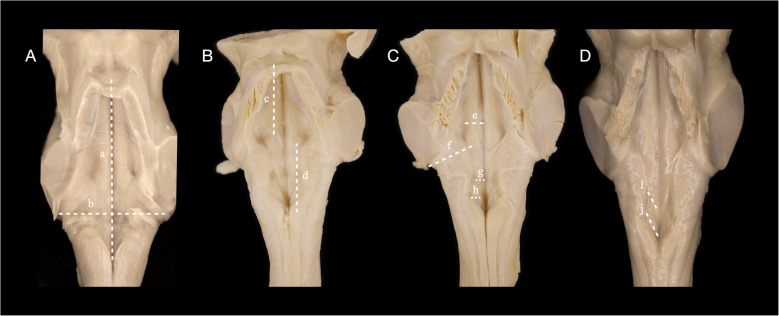 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Thyroid and Parathyroid Surgery · Head and Neck Surgical Oncology
Introduction
The fourth ventricle forms the posterior segment of the ventricular system and lies along the dorsal surface of the brainstem, bordered anteriorly by the pons and medulla and posteriorly by the cerebellum. Its floor, or rhomboid fossa, contains critical surface landmarks overlying cranial nerve nuclei and brainstem pathways. These include the facial colliculus, sulcus limitans, medial eminence, striae medullares, and surface elevations such as the hypoglossal and vagal trigones. Precise knowledge of these anatomical features is essential in neurosurgical procedures involving midline suboccipital or paramedian surgical corridors [1–9].
In light of this anatomical complexity, various surgical corridors have been developed to access fourth ventricular lesions. Among them, telovelar, subtonsillar, and transvermian approaches remain the most widely used. The telovelar and subtonsillar routes utilize natural planes through the cerebellomedullary fissure and beneath the tonsils, preserving midline structures and minimizing cerebellar injury [6, 10, 11]. In contrast, the transvermian approach—historically favored for its direct midline exposure—has declined due to its association with cerebellar mutism and damage to midline structures. More recently, superior transvelar and keyhole techniques have emerged to target rostral or dorsal brainstem lesions through minimally invasive access, though their applicability remains anatomically constrained. Regardless of technique, surgical corridor selection depends on the rostrocaudal level of the lesion, its lateral extension, and relationships to surrounding structures such as the cerebellar peduncles and lateral recesses [1, 3, 6, 8, 12–16].
These approaches are frequently employed to treat diverse pathologies located within or adjacent to the fourth ventricle and brainstem. Typical lesions include ependymomas, subependymomas, medulloblastomas, cavernous malformations, and hemangioblastomas—all of which may distort local anatomy and require careful dissection near regions that contain vital cranial nerve nuclei[13, 14, 16–20]. The median sulcus along the midline floor of the fourth ventricle is often used as a surgical entry point due to its relative distance from critical motor and sensory nuclei, which lie lateral to the sulcus limitans. Various safe entry zones have been proposed in this context, including the suprafacial, infrafacial, and pericollicular triangles [1, 4, 6, 8, 10, 12, 17, 21, 22]. While these strategies are grounded in surface anatomy, they remain limited by a lack of quantitative cadaveric data regarding the true size, symmetry, and spatial relationships of the floor’s key landmarks.
Previous cadaveric studies have reported general morphometry of the fourth ventricle, such as total floor length and transverse width [1–3, 7–9]. However, discrepancies in anatomical definitions—such as variation in the precise aqueductal opening or lateral boundary—have limited their reproducibility. Furthermore, none of these studies have quantitatively characterized the hypoglossal or vagal trigones, despite their role as visible markers of underlying cranial nerve nuclei. Similarly, while sulcus limitans and striae medullares are frequently cited in surgical discussions, their measurable dimensions, symmetry, and variability have not been systematically documented [1, 3, 4].
The aim of this study is to provide a comprehensive morphometric analysis of the floor of the fourth ventricle using formalin-fixed human cadaveric brainstems. We seek to define the dimensions of key anatomical landmarks—including the rostrocaudal length and mediolateral width of the ventricular floor, lateral recesses, sulci, trigones, and surface fibers—and to derive anatomical ratios that reflect their proportional relationships. Although surgical relevance is considered, the primary objective is to establish normative morphometric data that may guide safer planning and interpretation of midline suboccipital approaches to the fourth ventricle. This study offers the first reported cadaveric measurements of the hypoglossal and vagal trigones and provides new insights into the spatial organization of the ventricle floor for neurosurgeons, anatomists, and educators.
Materials and methods
This morphometric study was conducted on 40 formaldehyde-fixed adult human cadavers. Each cadaver contained an intact brainstem, cerebellum, and associated posterior fossa structures, with all cranial bones removed to allow full exposure (Fig. 1). The floor of the fourth ventricle was accessed by carefully removing the cerebellar vermis, overlying lobules, and tela choroidea when necessary. Microdissection was performed under magnification using surgical loupes or a dissecting microscope to ensure precise identification of surface landmarks (Fig. 2). All measurements were obtained under direct visualization using digital calipers.Fig. 1. Macroscopic view of all 40 formaldehyde-fixed adult human cadavers. Some show intact posterior fossa contents—including cerebellum, brainstem, and fourth ventricle—prior to exposure, while others display the fully revealed fourth ventricular floor following removal of the cerebellar vermis, overlying lobules, and tela choroidea. This figure illustrates the anatomical preservation and exposure range across the cadaveric cohort used for morphometric analysisFig. 2Anatomical views of the fourth ventricle in selected cadaveric specimens. (A) Dorsal view showing the superior and inferior colliculi, superior medullary velum, posterior median sulcus, sulcus limitans, cerebellar peduncles, lateral recess, obex, among others. (B) Coronal view of the fourth ventricular floor demonstrating bilateral facial colliculi, hypoglossal and vagal trigones, striae medullares, superior and inferior foveae, among others. (C) Mid-sagittal section showing the cerebral aqueduct, fourth ventricle, superior and inferior medullary vela, and foramen of Magendie, among others, highlighting the rostrocaudal axis of the ventricular system and its relationship to the cerebellum and tectum
Sixteen anatomical parameters were assessed. Twelve were linear distances recorded in millimeters, while four were qualitative or ordinal observations. All measurements were performed in situ, with the brainstem fixed in a neutral position to avoid distortion of surface geometry. The rostrocaudal length of the fourth ventricle floor was measured from the aqueduct opening at the level of the superior medullary velum to the obex. The transverse width was recorded between the right and left foramina of Luschka, marking the lateral extent of the lateral recesses. To divide the ventricular floor into functional zones, the distance from the aqueduct to the superior margin of the facial colliculus was measured to represent the rostral (pontine) floor, and the distance from the inferior margin of the colliculus to the obex defined the caudal (medullary) segment (Fig. 3).Fig. 3. Quantitative morphometric measurements of the fourth ventricular floor. (A) a: rostrocaudal length from the aqueduct opening to the obex. b: transverse width between the foramina of Luschka; (B) c: distance from the aqueduct to the superior margin of the facial colliculus, representing the rostral (pontine) segment, d: distance from the inferior margin of the facial colliculus to the obex, defining the caudal (medullary) segment; (C) e: distance from the median sulcus to the sulcus limitans, f: lateral recess length measured obliquely from the vestibular area, adjacent to the sulcus limitans, to the foramen of Luschka, g: hypoglossal trigone width (transverse axis), h: vagal trigone width (transverse axis); (D) (i) hypoglossal trigone length (rostrocaudal axis), (j) vagal trigone length (rostrocaudal axis)
The lateral recess lengths were measured bilaterally. Each was recorded obliquely from the vestibular area, adjacent to the sulcus limitans, to the foramen of Luschka. Mediolateral dimensions were also recorded. The distance from the median sulcus to the sulcus limitans was measured separately on the right and left sides, at the point where the sulcus limitans was most visible, typically in the mid-pons, where it demarcates the transition from motor to sensory nuclei. The hypoglossal and vagal trigones were evaluated by measuring their maximum width (transverse axis) and length (rostrocaudal axis) on the side where the structure was most clearly distinguishable. These surface elevations correspond to the underlying cranial nerve XII and X nuclei, respectively (Fig. 3).
The presence or absence of the facial colliculi was recorded bilaterally. The number of striae medullares bundles was counted visually on each side using an ordinal 0–4 scale, based on the number of discrete fiber bands identifiable without magnification beyond × 10. No thickness or length measurement was attempted for the striae; only count data were collected. For all paired measurements, both right and left values were recorded independently. In analyses involving structures that could be asymmetric, only the most clearly defined side was included to avoid under- or over-representation (Fig. 2).
Descriptive statistics were calculated for all linear variables, including mean, standard deviation (SD), minimum, and maximum values. The Shapiro–Wilk test was used to evaluate the normality of distribution. Normally distributed paired data (e.g., right vs. left lateral recess length or sulcus limitans width) were compared using the paired t-test. If normality was not met, the Wilcoxon signed-rank test was applied. Comparisons of ordinal data, such as striae count, were also analyzed using the Wilcoxon test. A significance level of p < 0.05 was used for all comparisons (Table 1).Table 1. Descriptive morphometric measurements of the fourth ventricle floor in cadaveric specimens (n = 40)MeasurementRight Side (Mean ± SD)Right Side (Min–Max)Left Side (Mean ± SD)Left Side (Min–Max)p-valueMedian Sulcus → Sulcus Limitans3.09 ± 0.762.0–4.53.03 ± 0.671.5–4.00.49Striae Medullares Count2.07 ± 1.130–41.68 ± 1.010–40.044Lateral Recess Length6.64 ± 1.155.0–8.06.34 ± 1.035.0–8.00.003**Mean ± SDMin–Max-**Fourth Ventricle Length33.58 ± 2.4929.0–39.0-Fourth Ventricle Width20.0 ± 1.8317.0–24.0-Facial Colliculus (Caudal Margin) to Obex14.5 ± 1.6812.0–18.0-Aqueduct Opening to Facial Colliculus (Rostral Margin)14.6 ± 1.9711.0–18.0-Hypoglossal Trigone Width1.92 ± 0.391.5–3.0-Hypoglossal Trigone Length3.65 ± 1.062.0–6.0-Vagal Trigone Length1.83 ± 0.311.0–2.3-Vagal Trigone Width1.56 ± 0.391.0–2.0-This table summarizes morphometric measurements of the fourth ventricle floor based on 40 cadaveric specimensLinear distances are presented as mean ± standard deviation (SD) and range (min–max) in millimetersBilateral structures were compared using a paired t-test or Wilcoxon signed-rank test, depending on normalityP-values < 0.05 were considered statistically significant
Anatomical ratios were then calculated to evaluate the proportional relationships between substructures of the fourth ventricle floor and to derive clinically relevant geometric indices. These ratios included the trigone lengths and widths as a percentage of the corresponding caudal floor segment or ventricle width, the division of the floor into rostral and caudal segments relative to the total floor length, and the ratio of the usable surgical corridor (defined by the sulci limitans) to the entire floor width. All ratios were expressed as percentages and analyzed for normality using the Shapiro–Wilk test. Mean, SD, range, and 95% confidence intervals were reported (Tables 1 and 2).Table 2. Anatomical ratios of fourth ventricle substructures and their clinical relevanceRatioMean ± SD (%)Range (%)95% CI (%)Shapiro–Wilk p-valueNormal DistributionClinical InterpretationHypoglossal Trigone Length/Facial Colliculus to Obex Length25.44 ± 7.6111.76–40.023.08–27.790.43YesExtent of CN XII zone in the caudal floor (medial motor risk)Vagal Trigone Length/Facial Colliculus to Obex Length12.69 ± 2.445.88–16.6711.93–13.440.08YesExtent of CN X zone in the caudal floor (lateral parasympathetic risk)Hypoglossal Trigone Width/Fourth Ventricle Width (Luschka–Luschka)9.66 ± 2.16.25–15.09.01–10.320.14YesProportion of medial floor occupied by CN XII nucleusVagal Trigone Width/Fourth Ventricle Width7.91 ± 1.984.35–11.117.29–8.520.1YesProportion of lateral floor occupied by CN X nucleusFacial Colliculus to Obex Length/Fourth Ventricle Floor Length (Aqueduct to Obex)43.34 ± 5.1730.77–55.1741.73–44.940.75YesProportion of the floor relevant to caudal (medullary) surgical accessAqueduct to Facial Colliculus/Fourth Ventricle Floor Length43.57 ± 5.5731.43–56.6741.79–45.360.77YesProportion of the floor relevant to rostral (pontine) surgical accessFourth Ventricle Width/Fourth Ventricle Floor Length59.71 ± 5.3448.72–75.8658.06–61.370.14YesOverall shape index of floor (transverse vs. longitudinal)Sulcus Limitans-to-Limitans Width/Fourth Ventricle Width30.59 ± 6.1319.44–42.1128.63–32.550.24YesProportion of floor width between sulci limitans usable for midline accessThis table presents key morphometric ratios derived from cadaveric measurements of the fourth ventricle floor (n = 40)Each ratio expresses the proportional relationship between specific substructures (e.g., trigone size, floor width) and major anatomical axes such as the facial colliculus–obex segment or total ventricular floor length. Values are reported as mean ± SD (%), range, and 95% confidence interval (CI). Shapiro–Wilk test p-values were used to assess normality; all ratios followed a normal distribution. The final column summarizes each ratio’s clinical relevance to surgical corridor planning and risk localizationAbbreviations: SD, standard deviation; CI, confidence interval
To place our findings in anatomical and historical context, measurements were compared to previously published cadaveric studies, including those by Antar et al. [3], Umarani et al. [2], Lang et al. [1], and Last and Tompsett [9] (Table 3). In these comparisons, bilateral values in our data were summed when necessary to match single composite values reported in the literature. When previous authors provided means and standard deviations, two-sample t-tests were conducted to assess statistical differences from our findings. In older studies without statistical parameters, comparison was descriptive only.Table 3. Comparison of fourth ventricle floor measurements with published cadaveric studiesMeasurement (mm)This Study (Mean ± SD)Antar et al. [3]Umarani et al. [2]Lang et al. [1]Last &Tompsett [9]p-value (vs. Antar)p-value (vs. Umarani)Fourth Ventricle Length33.58 ± 2.4939.84 ± 4.03M: 41.51 ± 4.88F: 40.38 ± 2.0831.7 (28–38)29 (21–37) < 0.0001 < 0.0001Fourth Ventricle Width20.0 ± 1.8322.51 ± 2.43M: 23.39 ± 2.67F: 24.72 ± 2.0524.0 (21–26)17.0 (12–23) < 0.0001 < 0.0001Facial Colliculus → Obex14.5 ± 1.6820.74 ± 2.13M: 24.74 ± 2.31F: 22.44 ± 1.86–– < 0.0001 < 0.0001Aqueduct → Facial Colliculus14.6 ± 1.9720.54 ± 3.35M: 23.31 ± 3.65F: 24.10 ± 2.88–– < 0.0001 < 0.0001Lateral Recess Length (Right)6.64 ± 1.15––––Lateral Recess Length (Left)6.34 ± 1.03––––0.00490.0343Lateral Recess Length (R + L)12.98 ± 1.7114.83 ± 2.83M: 17.39 ± 3.06F: 16.92 ± 2.21–– < 0.0001 < 0.0001Median Sulcus → Sulcus Limitans (Right)3.09 ± 0.76––––Median Sulcus → Sulcus Limitans (Left)3.03 ± 0.67––––Median Sulcus → Sulcus Limitans (R + L)6.12 ± 1.335.51 ± 0.88M: 6.57 ± 0.98F: 6.42 ± 0.72––0.00490.0343This table compares morphometric measurements from the present study (n = 40 cadavers) with previously reported cadaveric data from Antar et al. (2019), Umarani et al., Lang et al. (1991), and Last & Tompsett (1953)Measurements are presented as mean ± SD or range. Two-sample t-tests were used to compare our values with reported means; all comparisons were statistically significant (p** < 0.001**). Differences may reflect variability in the definitions of anatomical landmarks, measurement techniques, and sample populations across studiesAbbreviations: SD, standard deviation
Results
The mean length of the fourth ventricle floor from the aqueduct opening to the obex was 33.58 ± 2.49 mm (range: 29.0–39.0 mm), and the transverse width from the right to the left foramen of Luschka was 20.0 ± 1.83 mm (range: 17.0–24.0 mm). These two principal axes define the overall shape of the floor, with the longitudinal axis establishing the surgical depth and the transverse axis defining exposure width (Table 1).
Rostrocaudal segmentation of the floor revealed nearly symmetrical division around the facial colliculus. The distance from the aqueduct to the facial colliculus, representing the rostral floor segment, measured 14.6 ± 1.97 mm, while the facial colliculus to obex distance, corresponding to the caudal segment, measured 14.5 ± 1.68 mm. This equal division validates the facial colliculus as a consistent surgical landmark in defining pontine versus medullary approaches (Table 1).
The width from the median sulcus to the sulcus limitans measured 3.09 ± 0.76 mm on the right and 3.03 ± 0.67 mm on the left, with no statistically significant difference (p = 0.49). These mediolateral distances represent the usable midline floor between sensory and motor columns and were highly symmetrical across sides (Table 1). In contrast, the lateral recess lengths showed mild asymmetry: 6.64 ± 1.15 mm on the right versus 6.34 ± 1.03 mm on the left, a statistically significant difference (p = 0.003). Although small in magnitude, this asymmetry may influence lateral corridor exposure in telovelar approaches (Table 1).
The facial colliculus was present bilaterally in all 40 cadavers. The striae medullares were consistently present but varied in number. The right side displayed a mean of 2.07 ± 1.13 bundles, while the left had 1.68 ± 1.01. This difference was statistically significant (p = 0.044), suggesting asymmetry in surface fiber organization. However, correlation analysis between total striae count and fourth ventricle width yielded no significant relationship (ρ = 0.03, p = 0.85), indicating that bundle density does not scale with cavity size (Table 1).
The hypoglossal trigone had a mean width of 1.92 ± 0.39 mm and a length of 3.65 ± 1.06 mm. The vagal trigone was smaller, measuring 1.56 ± 0.39 mm in width and 1.83 ± 0.31 mm in length. To our knowledge, these are the first quantitative measurements of the hypoglossal and vagal trigones based on cadaveric dissection. While prior literature has described these subependymal structures anatomically, no previous study has reported their precise morphometric dimensions in terms of width and length. These values define the anatomical extent of the cranial nerve XII and X zones within the floor of the fourth ventricle (Table 1).
Several anatomical ratios were derived from these measurements to assess spatial relationships. The hypoglossal trigone occupied 25.44 ± 7.61% of the caudal floor (i.e., the facial colliculus to obex segment), while the vagal trigone accounted for 12.69 ± 2.44%. These ratios quantify the rostrocaudal proportions of the motor and parasympathetic danger zones within the medullary floor. Transversely, the hypoglossal and vagal trigones occupied 9.66% and 7.91% of the total ventricular width, respectively, further defining medial and lateral corridor risks. The floor width between sulcus limitans landmarks comprised 30.59 ± 6.13% of the total ventricle width, representing the midline corridor accessible for surgical entry. The ratio of ventricle width to floor length was 59.71 ± 5.34%, indicating a flat floor with a broad working axis. The facial colliculus was positioned near the mid-floor point, with the rostral (aqueduct to colliculus) and caudal (colliculus to obex) floor zones each comprising approximately 43% of the total floor length. All ratios followed normal distribution (Table 2).
Statistical comparisons with previously published cadaveric data demonstrated significant differences across nearly all comparable measurements (p < 0.001; Table 3).
Discussion
Overview of morphometric objectives
This cadaveric study aimed to generate normative morphometric data for the floor of the fourth ventricle, with a direct emphasis on anatomical definition and surgical relevance. While surface structures such as the facial colliculus, sulcus limitans, and striae medullares are routinely described in classical neuroanatomy, few prior investigations have quantitatively characterized their spatial organization or proportions [1–3]. Even fewer studies have defined these features in a way that facilitates neurosurgical planning. Our findings clarify the geometric organization of the rhomboid fossa and provide quantitative context for regions commonly referenced in fourth ventricular and dorsal brainstem surgery [6, 7, 10, 15].
Floor dimensions and surgical segmentation
The rostrocaudal length of the fourth ventricular floor, from the aqueduct opening to the obex, measured 33.58 ± 2.49 mm, while the transverse width, defined by the distance between the foramina of Luschka, was 20.0 ± 1.83 mm. These primary axes delineate the working depth and lateral extent of the surgical field [1–3, 7, 15]. Internally, the floor was nearly symmetrically divided by the facial colliculus into rostral (14.6 ± 1.97 mm) and caudal (14.5 ± 1.68 mm) halves, validating its use as a midpoint reference for distinguishing pontine from medullary zones [6, 8, 11, 15, 21] (Table 1).
Clinically, this symmetric segmentation reinforces the facial colliculus as a structural “equator” of the floor, guiding the use of suprafacial versus infrafacial or pericollicular entry zones [5, 6, 8, 10, 11, 21, 25]. The facial colliculus lies at the junction of motor and sensory transition zones and provides a landmark for orientation during fourth ventricular entry.
Mediolateral corridor and surface fiber patterns
The distance from the median sulcus to the sulcus limitans averaged 3.09 mm (right) and 3.03 mm (left), with no significant asymmetry (p = 0.49) (Table 1). These measurements define a narrow midline corridor that lies medial to both motor and sensory nuclei and is considered relatively safe for dorsal entry [1–4]. Although the region between the median sulcus and sulcus limitans has often been referenced as a potential entry zone, our data support that the true midline—centered on the median sulcus—is preferred to minimize risk to underlying cranial nerve nuclei [6, 8, 10, 15].
The striae medullares were bilaterally visible in all specimens, with significantly more bundles observed on the right (2.07 vs. 1.68, p = 0.044) (Table 1). Although functionally benign, dense or asymmetric striae may obscure key anatomical triangles, particularly in the lower pontine region [1–4]. Notably, there was no significant correlation between total striae count and fourth ventricle width (Spearman’s ρ = 0.03, p = 0.85), suggesting that bundle density does not scale with overall cavity size.
Trigone dimensions and high-risk zones
This is the first cadaveric study to report precise dimensions of the hypoglossal and vagal trigones. The hypoglossal trigone measured 1.92 ± 0.39 mm in width and 3.65 ± 1.06 mm in length, while the vagal trigone measured 1.56 ± 0.39 mm by 1.83 ± 0.31 mm (Table 1 and 2). These surface elevations overlie the nuclei of cranial nerves XII and X and define subependymal surgical caution zones during medullary procedures [1–3].
Collectively, these trigones occupied approximately 40% of the caudal floor, severely limiting the usable entry area in this region (Table 2). Only the most well-defined side was measured to avoid under- or overestimation, consistent with prior anatomic practice [1, 3, 4, 6, 8]. Bilateral measurement was deemed unnecessary given their midline or paramedian location and the predominantly unilateral nature of surgical entry.
Proportional floor ratios and surgical corridor limits
The hypoglossal and vagal trigones occupied 25.44% and 12.69% of the caudal floor length, and 9.66% and 7.91% of the total ventricular width, respectively. In contrast, the usable midline corridor—defined between the sulci limitans—comprised 30.59 ± 6.13% of total floor width (Table 2). These ratios clarify the functional footprint of both surgical caution zones and accessible entry areas [1, 6, 21].
The width-to-length ratio of 59.71% defines the fourth ventricular floor as relatively flat, facilitating microsurgical exposure. The facial colliculus was positioned near the midpoint, with the rostral and caudal segments each comprising approximately 43% of total floor length, reinforcing its landmark utility in planning suprafacial, infrafacial, or pericollicular entry [1, 6, 21].
Lateral recesses and asymmetry
The lateral recesses showed mild but statistically significant asymmetry: 6.64 mm on the right versus 6.34 mm on the left (p = 0.003) (Table 1). This finding may influence side selection for telovelar or subtonsillar approaches, particularly when addressing eccentrically positioned lesions or maximizing lateral exposure. Subtle asymmetry in cerebellomedullary fissure anatomy or foramen of Luschka morphology may underlie these differences [4, 11, 21, 23].
Comparison with prior morphometric studies
Statistical comparisons with previously published cadaveric data revealed significant differences across nearly all comparable measurements. Our fourth ventricle floor length was shorter than that reported by Antar et al. (39.84 mm) and Umarani et al. (41.51 mm in males), likely due to differing definitions of the aqueduct’s superior boundary [2, 3]. Similarly, our ventricle width was smaller than Lang’s et al. (24.0 mm) but greater than that of Last and Tompsett et al. (17.0 mm), reflecting differing measurement landmarks—namely, the lateral recess versus inferior cerebellar peduncle span [1, 9] (Table 1,2,3). The lateral recess and sulcus measurements in our study were presented bilaterally and combined only for cross-study comparisons, whereas prior works did not clarify laterality. All numerical comparisons against Antar and Umarani datasets showed statistically significant differences (p < 0.001), likely due to methodological variation rather than anatomical divergence.
Previous cadaveric studies have documented general dimensions of the fourth ventricle, such as total floor length and transverse cavity width [1–3]. However, these studies vary significantly in their landmark definitions, particularly regarding the location of the aqueduct opening and the lateralmost measurement point for ventricle width. Furthermore, none of these studies have quantitatively characterized the hypoglossal or vagal trigones, despite their importance as surface indicators of cranial nerve nuclei. Similarly, while structures such as the sulcus limitans and striae medullares are routinely referenced in surgical entry discussions, their measurable width, symmetry, and variability remain poorly defined [1, 4].
Surgical applications and corridor selection
Familiarity with normative fourth ventricle anatomy is essential for safe resection of pathologies such as ependymomas, subependymomas, medulloblastomas, hemangioblastomas, cavernous malformations, and intraventricular lymphomas [10–13, 17–20, 22, 24]. Despite technological advances in neuronavigation and diffusion tensor imaging, precise surface anatomy remains fundamental.
The telovelar approach has become the most widely preferred surgical corridor. It utilizes the natural cerebellomedullary fissure to access the fourth ventricle without disrupting the inferior vermis, thereby preserving midline cerebellar structures and minimizing complications such as ataxia and mutism [5, 6, 11, 12]. The subtonsillar variant expands lateral exposure, while the transvermian approach—historically widely used—is now generally avoided due to its association with cerebellar mutism, disequilibrium, and injury to the fastigial and dentate nuclei. However, in select cases with large tumors extending rostrally toward the aqueduct or compressing the fastigium, it may still be considered when telovelar access is insufficient [11, 12, 22].
More recently, keyhole and superior transvelar approaches have gained favor for targeting dorsal brainstem lesions, though their applicability is anatomically constrained and requires high surgical expertise [12, 16].
Clinical relevance and limitations
This study establishes foundational morphometric data for the fourth ventricle floor, emphasizing anatomical clarity and surgical planning. By defining dimensions and ratios of common landmarks, our findings can enhance intraoperative decision-making and reduce the risk of cranial nerve injury.
Limitations include the use of formalin-fixed cadavers, which may contract and differ from in vivo conditions. Pediatric and pathological variants were not included. Future studies may incorporate 3D modeling, high-field imaging, and intraoperative correlation to expand clinical applicability.
Conclusion
The floor of the fourth ventricle demonstrates a consistent geometric organization that can be quantitatively mapped through cadaveric morphometry. Our results define the dimensions and spatial relationships of key subependymal structures, offering a reproducible anatomical framework to support neurosurgical planning, anatomical education, and safer fourth ventricular interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lang J Jr., Ohmachi N, Lang J Sr. (1991) Anatomical landmarks of the rhomboid fossa (floor of the 4th ventricle), its length and its width. Acta Neurochir (Wien) 113:84–90. 10.1007/bf 0140212010.1007/BF 014021201799148 · doi ↗ · pubmed ↗
- 2Mussi AC, Rhoton AL Jr. (2000) Telovelar approach to the fourth ventricle: microsurgical anatomy. J Neurosurg 92:812–823. 10.3171/jns.2000.92.5.081210.3171/jns.2000.92.5.081210794296 · doi ↗ · pubmed ↗
- 3Tanriover N, Ulm AJ, Rhoton AL Jr., Yasuda A (2004) Comparison of the transvermian and telovelar approaches to the fourth ventricle. J Neurosurg 101:484–498. 10.3171/jns.2004.101.3.048410.3171/jns.2004.101.3.048415352607 · doi ↗ · pubmed ↗