Candida species distribution, antifungal susceptibility and trends causing candidemia: a 10-year observation in eastern China
Peishan Cong, Biao Wang, Huiyang Qi, Guiming Zhang, Zhongjun Wang

TL;DR
This study analyzed 10 years of candidemia cases in eastern China, finding rising incidence and species-specific antifungal resistance trends.
Contribution
The study provides updated insights into candidemia trends, species distribution, and risk factors in eastern China over a decade.
Findings
Candida parapsilosis was the most prevalent species in candidemia cases.
Candida tropicalis and Nakaseomyces glabratus showed higher resistance to itraconazole and fluconazole.
Multiple clinical factors like diabetes, ICU admission, and surgery were identified as independent risk factors for candidemia.
Abstract
Candidemia is a major global public health problem due to the high mortality rates and increasing antifungal resistance. This study investigated the epidemiology and risk factors of candidemia in eastern China over the past 10 years. A descriptive, cross-sectional study was conducted from January 2015 to December 2024 in the Affiliated Hospital of Qingdao University to investigate the possible routes and risk factors of candidemia. Antifungal susceptibility was determined using broth microdilution method. The incidence of candidemia increased from 0.98% to 1.69% over the past 10 years. In total 276 candidemia cases, Candida parapsilosis was the most prevalent species (32.2%), followed by Candida albicans (31.9%) and Candida tropicalis (21.5%). C. albicans and C. parapsilosis were susceptible to antifungal agents (resistance rate <7%). Candida tropicalis and Nakaseomyces glabratus…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
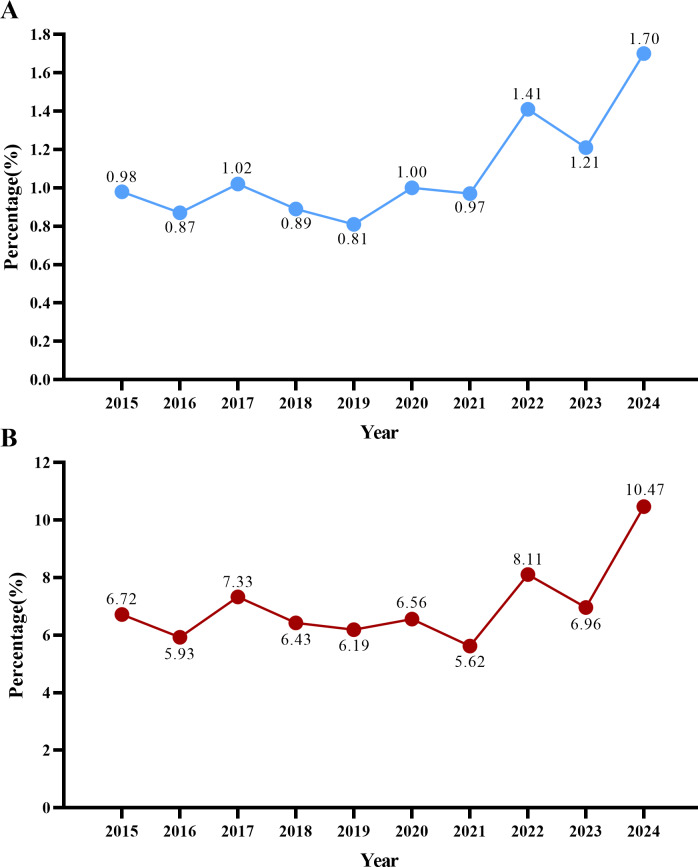 Figure 1
Figure 1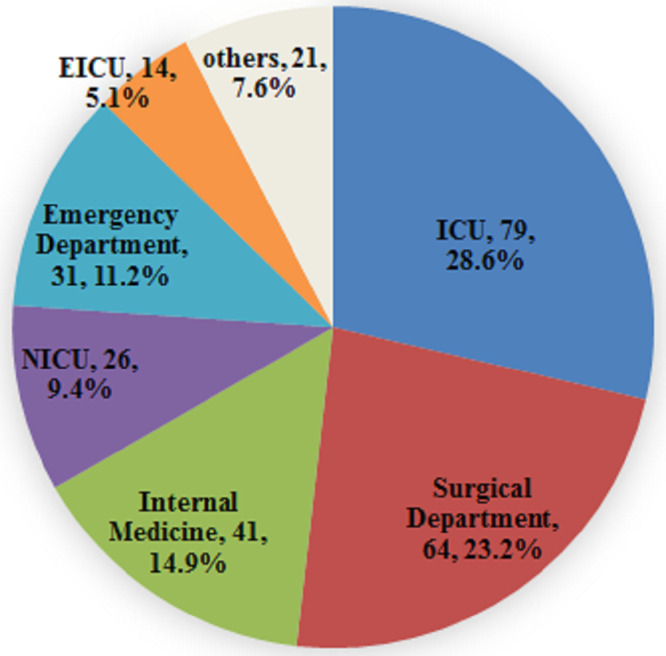 Figure 2
Figure 2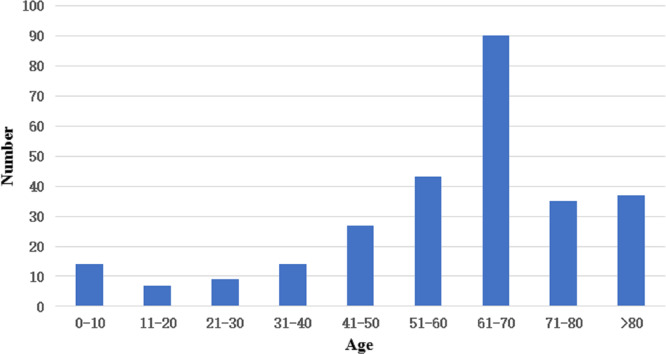 Figure 3
Figure 3- —The Young Scientist Foundation of the Affiliated Hospital of Qingdao University (no. 5201)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Antibiotic Resistance in Bacteria · Reproductive tract infections research
Introduction
The Candida genus is part of the body’s normal microbiota and primarily colonizes the skin, respiratory, gastrointestinal, and genital tracts. However, prolonged use of broad-spectrum antibiotics not only disrupts the integrity of the intestinal barrier but, when combined with corticosteroid-induced immunosuppression, creates a permissive microenvironment that facilitates Candida translocation into the bloodstream, increasing the risk of invasive candidiasis. Fungal pathogens and infections have become a growing global public health concern, and candidemia—specifically recognized as a life-threatening form of these infections—imposes a heavy burden of high mortality rates and hospital costs (Adam et al., 2021). An upward trend in candidemia infections has been noted due to the widespread use of broad-spectrum antibiotics, corticosteroids, immunosuppressants, anticancer therapy, and invasive devices, as well as solid organ transplantation (Thompson et al., 2024). In addition, tracheal intubation or tracheotomy and prior intensive care unit (ICU) hospitalizations could also increase the infection risk (Bassetti et al., 2017; Carbia et al., 2023).
The distribution of species causing invasive Candida infections varies among populations and geographical regions. Moreover, noticeable differences were observed in the proportions of Candida infections across hospital wards (Guinea, 2014). Candidemia caused by Candida albicans was the most frequently isolated (Pfaller et al., 2005). In addition, non-albicans Candida species, such as Candida parapsilosis, Candida tropicalis, and Nakaseomyces glabratus (formerly Candida glabrata), are increasingly being isolated from cases of candidemia, with growing antifungal resistance (Qiao et al., 2023). In 2022, the World Health Organization (WHO) released the “WHO Fungal Priority Pathogens List: Guidance on Research, Development and Public Health Actions” to systematically prioritize fungal pathogens, taking into account their unmet research and development needs and their significance in public health. As specified in the list, Candida auris (Sakaguchia auris, proposed) and C. albicans fall into the Critical Priority Group; N. glabrata, C. tropicalis, and C. parapsilosis are categorized under the High Priority Group; and C. krusei belongs to the Medium Priority Group (World Health Organization, 2022). The susceptibility of each Candida species to antifungal drugs varies. C. albicans harbors susceptibility to various antifungal drugs, while N. glabratus and C. tropicalis present reduced susceptibility to azoles. C. krusei is inherently resistant to fluconazole (FLC) (Tortorano et al., 2021; Boonsilp et al., 2021) C. auris is resistance to numerous antifungal drugs elevated the mortality risk and led to outbreaks in Brazil (Hou et al., 2017; De Almeida et al., 2021).
The fungal resistance intensifies the challenges in the clinical treatment of invasive Candida infections (Cetinkaya et al., 2023). Azoles, as first-line antifungal drugs, are widely used in clinical treatment. Nonetheless, the efficacy of azoles is compromised in the treatment of N. glabratus and C. tropicalis due to their reduced susceptibility. C. krusei was increasingly resistant to fluconazole, too (Bilal et al., 2022). Hence, numerous clinical guidelines have recommended echinocandins as the first-line antifungal agents (Tortorano et al., 2021). The emergence of fluconazole-resistant C. parapsilosis, fluconazole-, voriconazole (VRC)- and echinocandin-resistant N. glabratus strains, and the multi-antifungal-resistant Candida auris (Sakaguchia auris, proposed) poses formidable challenges to the effective clinical management of Candida infections (Pfaller et al., 2019; Castanheira et al., 2020). Despite improvements in disease diagnosis and the introduction of new antifungal drugs, the incidence of candidemia continues to rise (Domán et al., 2024).
Candidemia is a severe infection caused by the Candida genus and may cause multi-organ dysfunction. In recent years, the incidence rate of candidemia has gradually increased (Bilal et al., 2022). Consequently, quantifying serum BDG levels can predict the presence of invasive Candida spp*.* infection. The advantage of BDG-guided preemptive therapy is significant in reducing unnecessary antifungal treatments, which not only helps avoid adverse effects but also limits the development of drug resistance. Given an approximately 54% BDG diagnostic positivity rate for invasive fungal infections, further validation across different clinical settings is important to refine its role in clinical practice (Rouzé, Estella & Timsit, 2022).
In this study, we collected Candida strains isolated from clinical bloodstream infections at the Affiliated Hospital of Qingdao University between January 2015 and December 2024. We analyzed the species distribution, antifungal drug susceptibility, associated risk factors, morbidity rates, and the diagnostic value of the BDG test for candidemia. This research aims to provide a foundation for effective treatment strategies for candidemia and to support efforts in preventing the spread of drug-resistant Candida.
Materials & Methods
Ethics statement
This project was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University (QYFY WZLL 29011). All participants provided written informed consent to participate.
Isolates collection and study design
Between January 2015 and December 2024, a total of 3,838 bloodstream infections were recorded at the Affiliated Hospital of Qingdao University. During the same period, 276 non-duplicate Candida isolates were collected from patients diagnosed with candidemia. A retrospective analysis was conducted to identify these cases across ward distribution, the Candida species distribution, antifungal susceptibility profiles, and the changes in BDG assay results throughout the therapeutic course.
Blood culture and Candida spp. identification
Blood cultures were performed using the BACTEC™ FX Automated Blood Culture System (BD Biosciences, Franklin Lakes, NJ, USA). Following a positive culture result, the culture bottle was removed, and the liquid medium was smeared for Gram staining. The medium was then inoculated onto 5% sheep blood agar, MacConkey agar, and chocolate agar plates. When yeast was observed microscopically on the smear, the blood culture bottles were further inoculated onto Sabouraud dextrose agar. Cultures were incubated at 35 °C for 24–48 h. Species identification of isolated colonies was performed using MALDI-TOF mass spectrometry (Bruker Daltonics, Bremen, Germany).
Additionally, clinical data, including age, sex, and ward information for these patients, were recorded.
Antifungal susceptibility testing
The broth microdilution method (BMD) was employed for Candida susceptibility testing according to the Clinical and Laboratory Standards Institute (CLSI). Clinical breakpoints (CBPs) and epidemiological cutoff values (ECVs) were determined according to CLSI guidelines and are presented in Supplement 1; they were applied as described. Quality control strains, including C. albicans ATCC 90028, C. parapsilosis ATCC 22019, and C. krusei ATCC 6258, were used, with quality control for susceptibility and species identification performed weekly. Sabouraud dextrose agar and Columbia blood agar plates were acquired from Zhengzhou Antobio Co., Ltd. (Zhengzhou, China), while Candida chromogenic medium was obtained from Jinan Babio Co., Ltd. (Jinan, China).
(1,3)-β-D-glucan (BDG) assay
BDG levels in patients’ serum were measured using the BDG assay kit (Zhanjiang A & C Biological LTD., Zhanjiang, China), by photometric analysis. The BDG assay was performed strictly according to the instructions provided in the BDG test kit manual. The cutoff value was 100.5 pg/mL, as recommended by the manufacturer.
Statistical analysis
SPSS 22.0 software (IBM, Armonk, NY, USA) was used for statistical analysis. The association between categorical variables and group data was analyzed using the chi-square test. For non-normally distributed quantitative data, results were presented as medians with interquartile ranges. Variables related to bloodstream infections that were significant in the univariate analysis were entered into a multivariate logistic regression to identify independent risk factors. P-values less than 0.05 were considered statistically significant.
Results
Incidence trend of candidemia
In 2015, 22 Candida spp. isolates separated from 2,245 blood culture samples, showing a positivity rate of 0.98% (22/2,245). In the subsequent years, the incidence continued to increase, reaching approximately 1.69% (50/2,959) by 2024. In 2015, a total of 327 pathogens were isolated from blood cultures, of which 22 were Candida strains, accounting for 6.72% (22/327). In recent years, the proportion of Candida spp. among blood culture-isolated pathogens has increased steadily, reaching nearly 11% by 2024 (Table 1, Fig. 1).
Table 1: The positive rate of Candida spp in blood culture.
The positive rate of Candida. spp. (A) The positive rate of Candida spp. separating from bloodstream infections, (B) the proportion of Candida spp. in pathogens isolated from blood culture.
Distribution of Candida species isolated from blood cultures
Between January 2015 and December 2024, a total of 3,838 positive blood culture cases were recorded at our hospital, of which 276 non-duplicate Candida isolates were extracted, accounting for 7.2% of all blood culture-positive cases (Table 1). C. parapsilosis was the most frequently isolated species (89 isolates, 32.2%), followed by C. albicans (88 isolates, 31.9%), and C. tropicalis (59 isolates, 21.5%). N. glabratus ranked fourth (23 isolates, 8.3%). Other isolates included C. famata (n = 6, 2.2%), Meyerozyma guilliermondii (n = 4, 1.4%), C. rugosa (n = 2, 0.7%), C. krusei (n = 2, 0.7%), C. intermedia (n = 1, 0.4%), C. dubliniensis (n = 1, 0.4%), and C. norvegensis (n = 1, 0.4%). The details are presented in Table 2.
Of the 276 cases of Candida infections identified through blood culture, isolates from the ICU accounted for 28.6% (79/276), followed by the Surgical Department (64 cases, 23.2%), Internal Medicine (41 cases, 14.9%), and the Emergency Department (31 cases, 11.2%). The Neurological ICU and Emergency ICU contributed 9.4% (26/276) and 5.1% (14/276), respectively. The remaining cases from other wards comprised 7.6% (21/276) (Fig. 2). Among the 276 patients with candidemia, 177 were male (64.1%), and 99 were female (35.9%). Candidemia occurred across a wide age range, from 20 days to 91 years, with a median age of 62 years (interquartile range, 50.5–72 years). Notably, 74.3% of patients were aged 50 years or older (Fig. 3).
Table 2: Univariate analysis of the factors influencing candidemia.
Distribution of candidemia patients by clinical service.
Distribution of candidemia patients by age.
Analysis of risk factors for Candidemia
Hypertension (64.9%), surgery (62.0%), chronic pulmonary disease (38.8%), and cardiovascular disease (35.5%) were the most common underlying diseases in candidemia patients. It is worth noting that 89.1% of patients had received antibiotics prior to developing candidemia, and 69.2% had been admitted to the ICU for at least 15 days before the blood culture results became positive. Surgical treatments had been performed in 171 (62.0%) patients. 169 (61.2%) patients used intravascular catheters, and 60.1% required mechanical ventilation. Nearly half of the patients with candidemia (43.5%) needed total parenteral nutrition. Additionally, 31.5% suffered from a solid organ tumor (Table 3).
Table 3: Distribution and antifungal susceptibility of Candida species causing candidemia.
A comparative analysis of risk factors for candidemia was conducted. The infection group included patients with candidemia, while the control group consisted of patients from the same wards who did not develop candidemia. The results revealed that hypertension (P < 0.001), chronic pulmonary diseases (P = 0.021), hematological malignancy (P = 0.012), solid organ tumor (P = 0.031), surgery (P < 0.001), prior antibiotic administration >15 days (P < 0.001), and the use of intravascular catheters (P = 0.03), ICU admission (P < 0.001), mechanical ventilation (P = 0.02) and total parenteral nutrition (P < 0.001) were significantly more common in the infection group than in the control group. In contrast, no significant differences were observed in other factors (P > 0.05) (Table 2).
Antifungal susceptibility testing results
The results of the antifungal susceptibility testing revealed that Amphotericin B (AMB) showed strong activity against common Candida isolates, with the rate of non-wild-type (nWT) or resistance being less than 2%. Except for one N. glabrata strain showing intermediate susceptibility to caspofungin (CAS), and one C. parapsilosis strain exhibiting intermediate susceptibility to both caspofungin (CAS) and micafungin (MCF), all other common Candida species were susceptible to echinocandins. Compared with C. parapsilosis and C. albicans, C. tropicalis and N. glabratus showed significantly higher resistance rates to voriconazole (8.5%, 21.7% vs 2.3%, 2.3%) and fluconazole (18.6%, 30.4% vs 5.6%, 2.3%), respectively. The resistance rates of C. tropicalis and N. glabratus to itraconazole (ITC) were also notable, at 18.6% (11/59) and 13.0% (1/23), respectively. For C. parapsilosis, the overall itraconazole nWT rate was only 6.7% (6/89) (Table 3).
Outcomes of BDG assay in patients with candidemia
Among the 276 patients with candidemia, BDG assays were conducted on 118 patients (42.8%), within 7 days before to 14 days after the onset of symptoms. The assay yielded positive results in 84 cases, yielding a sensitivity of 71.2% and a specificity of 90%. Dynamic monitoring of BDG was implemented on 15 of the 49 positive individuals, revealing that antifungal therapy led to a marked decrease in BDG levels in 10 patients. This decrease was accompanied by improvement in clinical symptoms, indicating the effectiveness of the antifungal treatment and a favorable prognosis, leading to successful discharge. Conversely, five patients whose BDG levels initially decreased post-antifungal treatment but subsequently increased and remained elevated, presented a poor prognosis. These findings highlight the significant value of BDG assays for dynamic monitoring and for assessing the therapeutic outcomes in candidemia.
Discussion
Our study found that the prevalence of candidemia has been steadily increasing over the years. The incidence rose from 0.98% in 2015 to 1.69% in 2024, which is slightly lower than the data in previous studies (Carbia et al., 2023). A study in Japan reported a candidemia incidence of 0.84% across over 2,000 hospitals between 2010 and 2019, which is marginally lower than our findings. This difference may be due to regional differences, hospital infection control strategies, and so on (Kajihara et al., 2022). The increase in candidemia incidences in recent years can be attributed to advances in diagnostic and therapeutic technologies, more invasive procedures, widespread use of broad-spectrum antibiotics, and immunocompromise caused by various underlying diseases (Tsay et al., 2017). Given the challenges in early diagnosis and the high mortality rate of candidemia, understanding the distribution of Candida species and their resistance patterns can provide essential guidance for empirical antifungal therapy.
In this study, we observed that non-albicans Candida, with C. parapsilosis surpassing C. albicans, emerged as the most prevalent species in bloodstream infections. This result is similar to the findings of several recent studies (Puig-Asensio et al., 2014a; Mamali et al., 2022). Conversely, a retrospective study spanning over 16 years at a center in Lebanon found that C. albicans had the highest isolation rate in bloodstream infections, followed by C. tropicalis. This finding was consistent with research data from the USA (Zakhem et al., 2021). A study from a hospital in China found that C. tropicalis accounted for the highest proportion of isolates (Li et al., 2015). Variation in species distribution may be attributed to differences in geographic regions, hospital settings, the patients studied, and the study time frames. Further analysis of species distribution across age groups showed that C. parapsilosis was particularly prevalent in patients under 18 years (Adam et al., 2021). Li et al. (2015) suggested that the increased isolation of non-albicans Candida might be associated with the widespread use of antifungal drugs. However, we did not find a significant association between antifungal use and species distribution. Future research should evaluate the impact of antifungal therapy on the incidence and species distribution of candidemia.
A majority (276) of Candida isolates collected in this study originated from the ICU, the Surgical Department, Internal Medicine, and the Emergency Department. The highest incidence of candidemia patients was observed in the ICU, potentially due to the severity of patients’ conditions, prolonged hospital stays, complex underlying diseases, frequent need for mechanical ventilation, extended use of broad-spectrum antibiotics, and intravenous catheterization. A previous study on 236 candidemia patients, with 172 cases (72.9%) being post-surgical, reported a significantly higher incidence of C. parapsilosis (Zhang et al., 2014). Similarly, the analysis of patients with post-surgical candidemia at our hospital revealed that C. parapsilosis was the dominant isolate (49.0% (50/102)). Patients with hematology, particularly those receiving immunosuppressive therapy or chemotherapy, are at heightened risk of candidemia. Moreover, C. tropicalis was the most commonly isolated species in the Hematology department (55.6% (15/27)), which is consistent with the findings in Brazil (Bergamasco et al., 2013). Our data further reveal that candidemia is more prevalent among the older population, especially those aged > 50 years, and is more common in males than in females. These findings align with the results of the CHIF-NET survey in China. Xiao et al. (2020) and other recent global studies (Pinto-Magalhaes et al., 2019; Aguilar et al., 2020). Notably, 89.1% of patients had received antibiotics prior to candidemia, and more than half of the patients suffered from hypertension and underwent surgery. Over 60% of patients had used intravascular catheters and were admitted to the ICU before developing a Candida-positive blood culture. Overall, the study shows that the well-established risk factors for candidemia include total parenteral nutrition, antibiotic exposure, intravascular catheters, mechanical ventilation, ICU admission, hematological malignancies, solid organ tumors, and surgery.
Regarding antifungal susceptibility, the present study evaluated six antifungal agents and found that C. parapsilosis and C. albicans were highly susceptible to all tested drugs. However, our results demonstrated that C. tropicalis and N. glabratus displayed reduced susceptibility to azoles. The susceptibility of C. tropicalis to fluconazole and itraconazole (78.0% and 81.4%, respectively) was consistent with the recently reported from CHIF-NET. However, its susceptibility to voriconazole (74.6%) was higher than that reported (49.2%) (Farmakiotis & Kontoyiannis, 2017). Bassetti et al. (2020) reported lower fluconazole resistance rates in C. tropicalis isolates from Latin America and North America, with rates of 1.1% and 5.5%, respectively (Bassetti et al., 2020). The resistance rates in other regions, such as China, were higher. The resistance rate of C. tropicalis to fluconazole was 22.2%, and it also showed 90.4% cross-resistance to voriconazole (Tan et al., 2016). Reports from Europe, such as those from Norway (Hesstvedt et al., 2015) and Switzerland, showed lower resistance rates to voriconazole (6.2% and 9%, respectively). These results suggest that the spread of azole-resistant C. tropicalis may be limited within the Asia-Pacific region. N. glabratus also exhibited reduced susceptibility to azoles, with 30.4% and 21.7% resistance and nWT to fluconazole and voriconazole, respectively. These findings are consistent with a multicenter study from China (Xiao et al., 2018). The increasing azole resistance among Candida species warrants concern, largely due to the overuse of azole drugs (Brescini et al., 2020). In response to the rising prevalence of azole resistance, the American Infectious Diseases Society (IDSA) recommended echinocandins as first-line agents for the treatment of Candida in 2016 (Pappas et al., 2016). Despite the emergence of echinocandin-resistant strains, it remains highly effective against fungal infections. Amphotericin B, a potent antifungal agent, has long been restricted in clinical application primarily owing to its substantial toxicity, which often manifests as severe nephrotoxicity and infusion-related adverse reactions.
The early symptoms of candidemia lack specificity, making differentiation from bacterial infections difficult. Blood culture is generally used as the gold standard for diagnosis. However, the culture process is time-consuming and may be interfered with by various factors, thus delaying early diagnosis. Given the long treatment durations, high recurrence rates, and elevated mortality associated with Candida infections, timely and accurate non-culturing diagnostic methods are needed. As a key component of fungal cell walls, BDG can be detected in serum and offers valuable assistance in diagnosing various fungal infections. Combining BDG assays with blood culture enhances early diagnostic and therapeutic monitoring capabilities. In this study, BDG testing was performed on 276 patients with candidemia, with a susceptibility of 41.5%. However, Yazdanpanah et al. (2024) reported a BDG test susceptibility rate of more than 90%. The disparity may be attributed to differences in the diagnostic reagents utilized. Similarly, Rouzé, Estella & Timsit (2022) reported a 45% BDG sensitivity in ICU patients, which aligned closely with our findings (Puig-Asensio et al., 2014b). Future studies, including larger sample sizes and additional regions, are needed to assess the diagnostic value of the BDG in candidemia. Though BDG-guided preemptive antifungal therapies did not significantly improve patients’ outcomes, they did contribute to a substantial reduction in antifungal dosages (Yoshida, 2021). Dynamic BDG monitoring in 10 patients showed a progressive decrease in BDG levels, which correlated with favorable clinical outcomes. However, five patients who initially experienced reduced BDG levels later saw levels rise again and had a poor prognosis. These findings highlight the utility of the BDG test in tracking the therapeutic response to antifungal therapy. Another notable observation in this study is that the β-D-glucan (BDG) assay is not useful for predicting the recurrence of dermatophyte foot infection. Superficial fungal infections usually cause fungal foot, while candidemia is an invasive fungal infection. Various factors may influence the sensitivity and specificity of BDG, so a comprehensive diagnostic approach that combines blood culture with clinical systems is necessary.
Conclusions
In conclusion, this study provided valuable insights into the species distribution, risk factors, and antifungal susceptibility of Candida species causing candidemia in our region. It also highlights the potential role of BDG testing in early diagnosis and developing effective empirical treatment strategies for blood candidemia.The incidence of candidemia has increased in recent years, and C. parapsilosis was the most prevalent species. Thus, effective strategies are needed to help reduce morbidity and mortality among patients with candidemia.
Supplemental Information
10.7717/peerj.20832/supp-1Supplemental Information 1Clinical breakpoints (CBPs) and epidemiological cutoff values (ECVs)
10.7717/peerj.20832/supp-2Supplemental Information 2The ITS sequencing results
10.7717/peerj.20832/supp-3Supplemental Information 3Raw data
10.7717/peerj.20832/supp-4Supplemental Information 4The raw data related to the MALDI-TOF identification
10.7717/peerj.20832/supp-5Supplemental Information 5English translation codebook for raw data related to the MALDI-TOF identification
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adam K-M Osthoff M Lamoth F Conen A Erard V Boggian K Schreiber PW Zimmerli S Bochud P-Y Neofytos D Fleury M Fankhauser H Goldenberger D Mühlethaler K Riat A Zbinden R Kronenberg A Quiblier C Marchetti O Khanna N 2021 Trends of the epidemiology of candidemia in Switzerland: a 15-year FUNGINOS survey Open Forum Infectious Diseases 847110.1093/ofid/ofab 471PMC 851417834660836 · doi ↗ · pubmed ↗
- 2Aguilar G Araujo P Lird G Insaurralde S Kawabata A Ayala E Irala J Argüello R Identification and susceptibility profile of Candida species isolated from hemocultures in hospitals in Paraguay Revista Panamericana De Salud Publica-pan American Journal of Public Health 202044 e 3410.26633/RPSP.2020.3432973893 PMC 7498287 · doi ↗ · pubmed ↗
- 3Bassetti M Garnacho-Montero J Calandra T Kullberg B Dimopoulos G Azoulay E Chakrabarti A Kett D Leon C Ostrosky-Zeichner L Sanguinetti M Timsit J-F Richardson MD Shorr A Cornely OA 2017 Intensive care medicine research agenda on invasive fungal infection in critically ill patients Intensive Care Medicine 431225123810.1007/s 00134-017-4731-228255613 · doi ↗ · pubmed ↗
- 4Bassetti M Vena A Bouza E Peghin M Muñoz P Righi E Pea F Lackner M Lass-Flörl C 2020 Antifungal susceptibility testing in Candida, Aspergillus and Cryptococcus infections: are the MI Cs useful for clinicians?Clinical Microbiology and Infection 261024103310.1016/j.cmi.2020.02.01732120042 · doi ↗ · pubmed ↗
- 5Bergamasco MD Garnica M Colombo AL Nucci M 2013 Epidemiology of candidemia in patients with hematologic malignancies and solid tumours in Brazil Mycoses 5625626310.1111/myc.1201323043234 · doi ↗ · pubmed ↗
- 6Bilal H Shafiq M Hou B Islam R Khan MN Khan RU Zeng Y 2022 Distribution and antifungal susceptibility pattern of Candida species from mainland China: a systematic analysis Virulence 131573158910.1080/21505594.2022.212332536120738 PMC 9487756 · doi ↗ · pubmed ↗
- 7Boonsilp S Homkaew A Phumisantiphong U Nutalai D Wongsuk T 2021 Species distribution, antifungal susceptibility, and molecular epidemiology of Candida species causing candidemia in a tertiary care hospital in Bangkok, Thailand Journal of Fungi 757710.3390/jof 707057734356956 PMC 8303137 · doi ↗ · pubmed ↗
- 8Brescini L Mazzanti S Orsetti E Morroni G Masucci A Pocognoli A Barchiesi F 2020 Species distribution and antifungal susceptibilities of bloodstream Candida isolates: a nine-year single-center survey Journal of Chemotherapy 3224425010.1080/1120009 X.2020.178315432580685 · doi ↗ · pubmed ↗