Randomized controlled trial of intraosseous access vs. intravenous access in traumatic hemorrhagic shock: Effects on inflammation, hematopoiesis, and coagulation
Gaorong Deng, Lang Jiang, Xin Miao, Yuying Dong, Xiang Gao, Zongfang Li

TL;DR
This study compares intraosseous and intravenous access in traumatic hemorrhagic shock patients, finding that intraosseous access may worsen inflammation, hematopoiesis, and coagulation.
Contribution
The study provides clinical evidence on the effects of intraosseous access in traumatic hemorrhagic shock, highlighting its potential adverse impacts on inflammation and coagulation.
Findings
Intraosseous access led to higher inflammatory markers and oxidative stress compared to intravenous access.
Hematopoietic function was impaired in the intraosseous group with reduced CD34+ cells and colony formation.
Intraosseous access was associated with worse coagulation profiles and tissue hypoxia indicators.
Abstract
This study aimed to evaluate the impact of intraosseous (IO) access on inflammatory mediators, hematopoietic cell function, and coagulation-metabolic disturbances in patients presenting with emergency traumatic hemorrhagic shock (THS), thereby providing clinical evidence to refine IO resuscitation protocols in emergency settings. We conducted a randomized controlled trial involving 84 THS patients admitted between February 2024 and February 2025. Participants were allocated equally into two groups: the IO group (n= 42), where vascular access was established via humeral or proximal tibial puncture, and the intravenous (IV) group (n= 42), where conventional peripheral or central venous access was prioritized. Serial measurements were performed at baseline (T0), 24 hours (T1), and 72 hours (T2) post-intervention to assess: (1) inflammatory mediators (IL-1 b, IL-6, IL-10, HMGB1, MDA); (2)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
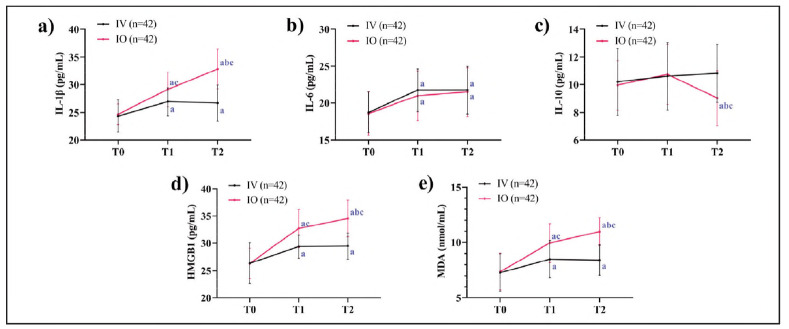 Figure 1
Figure 1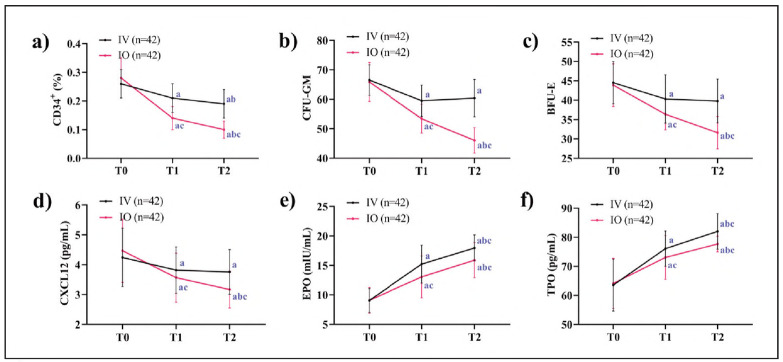 Figure 2
Figure 2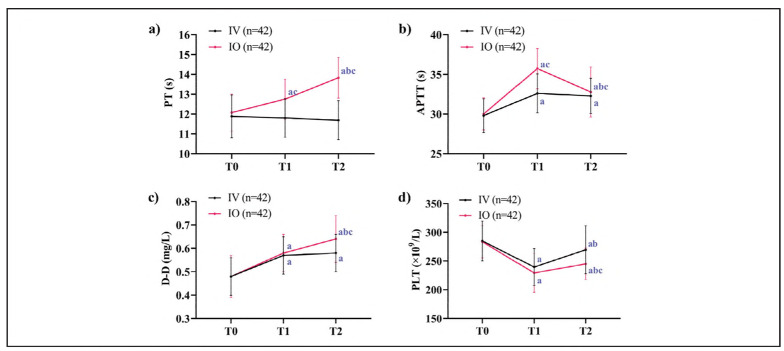 Figure 3
Figure 3| Projects | IV group (n= 42 ) | IO group (n= 42 ) | t (or χ2) | P |
|---|---|---|---|---|
| Age | 43.93 ±11.81 | 43.17±10.80 | 0.389 | 0.759 |
| Sex | 0.474 | 0.491 | ||
| male | 26 (61.90) | 29 (69.05) | ||
| female | 16 (38.10) | 13 (30.95) | ||
| BMI (kg/m2) | 23.24±3.07 | 22.57±3.39 | 0.948 | 0.346 |
| DBP (mmHg) | 77.90±10.40 | 76.10±9.70 | 0.825 | 0.412 |
| SBP (mmHg) | 111.43±12.66 | 112.40±10.47 | 0.385 | 0.701 |
| Types of injuries | 0.957 | 0.916 | ||
| traffic accident | 22 (52.38) | 19 (45.24) | ||
| fall | 8 (19.05) | 7 (16.67) | ||
| crush | 5 (11.90) | 7 (16.67) | ||
| blunt/sharp force injuries | 6 (14.29) | 5 (11.90) | ||
| Other | 1 (2.38) | 4 (9.52) | ||
| Puncture site | ||||
| proximal humerus | - | 29 (69.05) | ||
| proximal tibia | - | 13 (30.95) | ||
| First-attempt success | 27 (64.29) | 36 (85.71) | 5.143 | 0.023 |
| Puncture time (s) | 121.07±58.31 | 85.76±13.34 | 3.826 | <0.001 |
| Infusion time (min) | 30.52±2.36 | 15.76±3.42 | 23.024 | <0.001 |
| Infusion rate (m L/min) | 40.29±3.68 | 122.67±16.00 | 32.521 | <0.001 |
| Groups | Blood lactate (mmol/L) | 24-hour lactate <br>clearance rate (%) | ||
|---|---|---|---|---|
| T0 | T1 | T2 | ||
| IV group (n=42 ) | 1.32±0.42 | 0.90±0.08a | 0.78±0.09ab | 23.36±29.89 |
| IO group (n 42 ) | 1.32±0.30 | 1.11± 0.17a | 0.87± 0.17ab | 12.41±22.08 |
| t (or χ2) | 0.070 | 7.322 | 3.116 | 2.003 |
|
| 0.944 | <0.001 | 0.003 | 0.049 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma, Hemostasis, Coagulopathy, Resuscitation · Trauma and Emergency Care Studies · Traumatic Brain Injury and Neurovascular Disturbances
Introduction
Traumatic hemorrhagic shock (THS), a life-threatening condition frequently encountered in emergency medicine, is characterized by massive blood loss leading to reduced effective circulating blood volume, impaired tissue perfusion, cellular metabolic dysfunction, and subsequent organ failure [1]. This complex clinical syndrome, typically resulting from high-energy trauma such as motor vehicle collisions or catastrophic injuries, presents with complex, severe, and urgent conditions [2]. In emergency medicine, establishing rapid vascular access for fluid resuscitation constitutes the cornerstone of THS management [3]. The intraosseous (IO) access offers a unique advantage in circulatory collapse as the medullary venous plexus remains patent, creating a non-collapsible conduit to the central circulation with excellent bioavailability of administered fluids and medications [4]. Current resuscitation guidelines accordingly recommend IO access as the primary alternative when peripheral venous cannulation fails, with subsequent conversion to central venous access once hemodynamic stability is achieved [5]. Numerous studies have validated the procedural efficiency and high success rates of IO access in critical settings, making it the preferred alternative when intravenous (IV) access is difficult, as recommended by international guidelines [6]. Current resuscitation guidelines primarily emphasize the procedural efficiency of IO access (e.g., puncture time, first-attempt success rate) [7] [8], yet lack clinical evidence regarding its systemic impact on the bone marrow microenvironment. This knowledge gap may lead to underestimation of IO's effects on immune homeostasis and hematopoietic recovery, ultimately influencing long-term outcomes. In the era of precision medicine, these conventional metrics, which focus predominantly on technical success and immediate hemodynamic stabilization, present notable limitations. A more comprehensive evaluation should incorporate deeper insights into the underlying pathophysiology of shock, moving beyond simplistic procedural outcomes.
Emerging evidence from basic science research reveals that traumatic insult induces mitochondrial dysfunction in bone marrow mesenchymal stem cells, activating pro-inflammatory cascades through the TLR4/NF- B signaling pathway [9]. Of particular concern is the bone marrow cavity - the central microenvironment for hematopoietic cell differentiation and development - where the potential mechanical or biochemical perturbations induced by direct IO infusion of large volumes of hypothermic fluids or hyperosmotic agents remain systematically uninvestigated. Such disturbances could disrupt local inflammatory mediator release and impair hematopoietic reconstitution, yet this knowledge gap risks clinical underestimation of IO's impact on immune homeostasis recovery and marrow compensatory capacity, ultimately skewing prognostic assessments [10].
To address these critical questions, our prospective study investigates the temporal dynamics of inflammatory mediators during the first 72 hours post-IO access in emergency THS patients, concurrently evaluating functional changes in hematopoietic progenitor cells through colony-forming assays and analyzing alterations in the CXCL12-CXCR4 chemokine axis. By deciphering how IO influences inflammatory networks and hematopoietic recovery in shock states, this research aims to provide molecular biological evidence for refining IO resuscitation protocols.
Materials and methods
Study population
Inclusion criteria: (1) Diagnosis of THS; (2) Clinical signs including altered mental status, tachycardia, cold/pale extremities, hypotension, or other perfusion deficits; (3) Shock index (SI) > 1.0 with stage III-IV shock (per ATLS criteria: SBP<90 mmHg, anuria, or GCS<12). Exclusion criteria: (1) Patient/family declined participation; (2) Pregnancy; (3) Fracture or infection at potential access sites; (4) Other forms of shock (e.g., septic, cardiogenic); (5) Injury Severity Score (ISS) (10) <25 to ensure injury homogeneity.
From February 2024 to February 2025, we enrolled 84 consecutive THS patients (55 males and 29 females; mean age 43.55 ± 11.25 years). Injury mechanisms included motor vehicle collisions (n=41), falls from height (n = 15), crush injuries (n = 12), blunt/sharp force injuries (n = 11), and other (n = 5). Written informed consent was obtained from all participants or their legal representatives after full disclosure of study risks. The institutional ethics committee approved the protocol (No. 20240551).
Study protocol
Patients were randomly allocated to either IV (n=42) or IO (n = 42) groups for IV access and IO access, respectively. Sample size was calculated based on IL-6 differences in pilot data (mean Δ = 15 pg/mL, SD=8.5). With α=0.05, β=0.1, and 20% attrition, 42 patients per group provided 90% power. Randomization was performed using computer-generated random numbers with block randomization (block size=4). Allocation concealment was ensured via sequentially numbered, opaque sealed envelopes opened after patient enrollment. All resuscitations were supervised by senior emergency physicians at or above the attending physician level, and advanced trauma life support was provided for severe trauma patients. Operators (attending-level emergency physicians) received standardized 2-hour training on IO device placement and maintenance prior to study initiation, including instructional videos and hands-on practice.
Methods
In the IV group, peripheral venous access was initially attempted. If the puncture attempt exceeded 2 minutes without success, central venous access was promptly established. For the IO group, the proximal humerus puncture site was identified at the most prominent aspect of the greater tuberosity, approximately 1-2 cm above the surgical neck. For IO access, puncture site (proximal humerus vs. tibia) was randomly assigned using sealed envelopes to control site-specific confounding. The proximal tibia puncture site was located about 3 cm inferior to the patella and 2 cm medial to the tibial midline on its flat surface. Following standard skin disinfection, the IO needle was advanced perpendicular to the bone until the marrow cavity was entered. The stylet was then withdrawn, and correct placement was confirmed by aspirating bone marrow using a syringe. The needle was then secured, and the IO catheter was flushed with 5-10 mL of 0.9% isotonic saline to maintain patency. Both groups received 30 mL/kg of lactated Ringer's solution at room temperature (22-25°C) infused under 300 mmHg pressure. The intraosseous device was maintained for no more than 24 hours, whereas the central venous line was retained for up to 30 days.
Laboratory tests
Venous blood samples were collected from patients at 0 hours (T0), 24 hours (T1), and 72 hours (T2) after puncture establishment. The following indicators were analyzed: IL-1β (DLB50), IL-6 (D6050B), IL-10 (D1000B), HMGB1 (IC1690G), CXCL12 (MAB310), EPO (DEPRU0), and TPO (BAF288): These markers were quantified using enzyme-linked immunosorbent assay (ELISA) with commercially available kits (R&D Systems). Malondialdehyde (MDA): Levels were determined via the thiobarbituric acid (TBA) colorimetric method using assay kits (Nanjing Jiancheng Bioengineering Institute). CD34^+^ cell enumeration: Flow cytometric analysis was performed (FACSCanto II, BD Biosciences) using CD34-FITC and CD45-APC antibody staining to identify and quantify CD34^+^ hematopoietic progenitor cells. Compensation was set using UltraComp eBeads^TM^ (Invitrogen), with daily CS&T calibration (BD Biosciences). CD34^+^ gate was defined per ISHAGE protocol. Colony-forming unit assays (CFU-GM) and burst-forming unit-erythroid (BFU-E): Isolated bone marrow mononuclear cells (BMNCs) were cultured in methylcellulose-based semi-solid media (Metho-Cult™, STEMCELL Technologies) supplemented with lineage-specific growth factors (GM-CSF and IL-3 for CFU-GM; EPO and SCF for BFU-E). After 7-14 days of incubation (37°C, 5% CO_2_), colonies containing ≥50 cells were microscopically enumerated. PT, APTT, and D-dimer: These were assessed using an automated coagulation analyzer (Sysmex CS-2500).
Additionally, paired arterial samples were obtained for lactate measurement. Heparinized blood was analyzed via enzymatic electrode methodology (e.g., Radiometer ABL90 blood gas analyzer). The 24-hour lactate clearance rate was computed as: Lactate clearance (%) = (initial l actate-24h l actate)/initial lactatex100.
None of the sample collectors or laboratory technicians knew the patients' groupings.
Statistical analysis
The data were analyzed using SPSS22.0. Continuous variables are presented as mean ± standard deviation (χ±s) and were compared between groups using independent samples t-tests. Categorical variables were analyzed using chi-square tests or Fisher's exact tests. Longitudinal data were analyzed using repeated-measures ANOVA with post-hoc Bonferroni tests for within-group comparisons, supplemented by independent t-tests for between-group differences at each time point. A P-value of less than 0.05 was considered statistically significant.
Results
Comparison of baseline characteristics
As shown in Table 1, the two groups did not differ significantly in baseline clinical characteristics, including age, sex, and BMI (P>0.05), confirming their comparability. In the IO group, access was established in the proximal humerus in 29 cases and in the proximal tibia in 13 cases, with a first-attempt success rate of 85.71%. In the IV group, 5 patients required a switch from peripheral to central venous access, and the first-attempt success rate was 64.29%. The IO group demonstrated a significantly higher first-attempt success rate than the IV group (P<0.05). Additionally, compared with the IV group, the IO group exhibited shorter puncture time, less infusion time, and faster infusion speed (P<0.05).
Dynamic changes in inflammatory mediators
At T0, no statistical inter-group differences were observed in serum inflammatory mediator levels (P>0.05). By T1, the IO group exhibited significantly elevated levels of IL-1β, HMGB1, and MDA compared to the IV group (P<0.05), whereas IL-6 and IL-10 levels remained comparable (P>0.05). These findings suggest that the IO route may amplify the release of tissue injury-associated mediators and intensify oxidative stress due to localized mechanical stimulation. At T2, the IO group maintained higher expression of HMGB1, IL-1β, and MDA (P<0.05), while IL-10 levels were significantly suppressed (P<0.05), indicating an inadequate compensatory anti-inflammatory response (Figure 1).
Dynamic changes in inflammatory mediators. a) Comparison of changes in IL-1β, b) Comparison of changes in IL-6, c) Comparison of changes in IL-10, d) Comparison of changes in HMGB1, e) Comparison of changes in MDA. Note: 'a' indicates P < 0.05 compared with T0, 'b' indicates comparison with T1, and 'c' indicates P < 0.05 compared with the IV group at the same time.
Impairment of hematopoietic function
Compared to T0, the IO group demonstrated progressive declines in CD34^+^ cells, CFU-GM, BFU-E, and CXCL12 at both T1 and T2, with values significantly lower than those in the IV group (P<0.05). This suggests a disruption in the bone marrow hematopoietic niche's chemotactic support capacity. Furthermore, although EPO and TPO levels in the IO group were elevated at T1 and T2, they remained lower than in the IV group (P<0.05), likely due to diminished responsiveness of growth factors secondary to localized bone marrow injury (Figure 2).
Impairment of hematopoietic function. a) Comparison of changes in CD34+, b) Comparison of changes in CFU-GM, c) Comparison of changes in BFU-E, d) Comparison of changes in CXCL12, e) Comparison of changes in EPO, f) Comparison of changes in TPO. Note: 'a' indicates P < 0.05 compared with T0, 'b' indicates comparison with T1, and 'c' indicates P < 0.05 compared with the IV group at the same time.
Tissue perfusion and metabolic alterations
Blood lactate levels were significantly higher in the IO group than in the IV group at both T1 and T2 (P<0.05). Additionally, the 24-hour lactate clearance rate was reduced in the IO group versus the IV group (P<0.05), reflecting impaired restoration of tissue perfusion (Table 2).
Table 2: Tissue perfusion and metabolic alterations.Note: 'a' indicates P<0.05 compared with T0, 'b' indicates comparison with T1.
Coagulation dysregulation
At T1, the IO group displayed prolonged PT and APTT compared to the IV group (P<0.01). By T2, PT remained prolonged in the IO group, and D-dimer levels were significantly elevated compared to the IV group (P<0.05). Additionally, PLT decreased in both groups at T1 compared to T0 but recovered by T2, though the IO group's PLT remained lower than that of the IV group (P<0.05) (Figure 3).
Coagulation dysregulation. a) Comparison of changes in PT, b) Comparison of changes in APTT, c) Comparison of changes in D-D, d) Comparison of changes in PLT. Note: 'a' indicates P < 0.05 compared with TO, 'b' indicates comparison with T1, and 'c' indicates P < 0.05 compared with the IV group at the same time.
Discussion
While IO infusion has been increasingly reported in the management of THS, its systemic effects on objective laboratory parameters remain underexplored. Our study comprehensively evaluated the impact of IO access on inflammatory mediators, hematopoietic function, tissue perfusion, and metabolism and coagulation function in THS patients, yielding several key findings:
Regarding inflammatory responses, we demonstrated that IO puncture-induced intramedullary pressure fluctuations and periosteal injury robustly activate inflammatory cascades, particularly elevating IL-1β and HMGB1 levels. This aligns with the mechanistic work by Ibrahim N et al. [11] in animal models, where mechanical stress from marrow puncture was shown to trigger TLR4-dependent IL-iβ secretion. The observed HMGB1 surge is particularly noteworthy, as this damage-associated molecular pattern engages RAGE receptors to amplify systemic inflammation [12] [13]. These results align with previous observations by Deng C et al. [14], who identified a significant association between elevated HMGB1 levels and increased risk of organ failure in trauma populations. Notably, IO infusion of non-warmed fluids may trigger a sudden drop in temperature in the bone marrow microenvironment, leading to mitochondrial dysfunction and excessive reactive oxygen species (ROS) production, evidenced by the characteristic tandem of elevated MDA and depressed SOD activity (oxidative/antioxidant imbalance), collectively exacerbating tissue damage. These findings corroborate experimental data from Stern M et al. [15], where hypothermic fluid resuscitation exacerbated oxidative damage in hemorrhagic shock models through similar mechanisms, manifested by increased MDA and decreased mitochondrial membrane potential. The temporal dynamics of IL-10 regulation presented another critical insight. The marked decline in this anti-inflammatory cytokine at 72 hours post-intervention suggests monocyte functional exhaustion under persistent inflammatory pressure, resulting in an imbalance between pro- and anti-inflammatory networks and creating a »second-hit« effect [16]. This phenomenon provides clinical validation for the »inflammatory exhaustion« hypothesis [Gao Z et al. [17]], demonstrating how sustained inflammatory activation can ultimately deplete the host's capacity to mount appropriate anti-inflammatory responses through cytokine synthesis impairment.
For hematopoietic function, the decline in CXCL12 suggests bone marrow stromal damage impairs hematopoietic stem cell homing, leading to reduced CD34^+^ cells and colony-forming capacity. Additionally, although compensatory increases in EPO and TPO were detected, their upregulation was less pronounced than in the IV group. This attenuated response implies that localized bone marrow injury - potentially mediated by oxidative stress or inflammatory cytokine suppression - may reduce growth factor receptor sensitivity, thereby hindering efficient hematopoietic recovery. Supporting this notion, Asker ME et al. [18] demonstrated in a bone marrow injury model that an inflammatory microenvironment down-regulates EPO receptor expression, blunting erythropoietic responses. Furthermore, the »osmotic shock« hypothesis proposed by Liu Y et al. [19] suggests that hypertonic conditions can induce mitochondrial permeability transition pore opening in hematopoietic stem cells, triggering apoptosis. Given this mechanism, we speculate that hypertonic fluids administered via IO infusion may potentially alter bone marrow interstitial osmolarity, contributing to hematopoietic progenitor cell dysfunction.
Finally, the elevated blood lactate levels and reduced lactate clearance observed in the IO group indicate persistent tissue hypoxia, which may contribute to a self-perpetuating cycle of inflammation and coagulation dysfunction through the following mechanisms: (1) Lactate-mediated hypoxia exacerbation: The accumulation of lactate activates HIF-1α, leading to increased HMGB1 release [20]. HMGB1, in turn, further suppresses mitochondrial respiratory chain activity, worsening hypoxia. (2) Coagulation abnormalities: The prolonged PT/APTT and elevated D-dimer levels suggest concurrent excessive thrombin generation and hyperfibrinolysis in the IO group, which may be driven by IL-6, which promotes tissue factor expression while accelerating platelet consumption. Supporting this, a study by Ueno T et al. demonstrated a significant correlation between IL-6 levels and coagulopathy severity in infectious shock patients [21].
Based on the above findings, we recommend that the following key points be prioritized in future IO procedures: (1) All infused fluids should be prewarmed to 37°C to prevent hypothermia-induced damage to the bone marrow microenvironment. (2) The initial perfusion rate should be carefully regulated (e.g., maintained at 50 mL/min) to minimize mechanical stress on the bone marrow cavity. (3) To mitigate oxidative and inflammatory injury, N-acetyl-cysteine (NAC) should be administered intravenously within 24 hours post-IO resuscitation to counteract MDA-mediated oxidative stress. Alternatively, low-dose corticosteroids (e.g., hydrocortisone at 50 mg/day) or HMGB1 monoclonal antibodies may be considered to suppress excessive inflammatory cascades.
This research has several limitations that should be acknowledged. First, the single-center, small-sample design may limit the statistical power and generalizability of the findings. Second, the 72-hour observation window was insufficient to assess long-term hematopoietic recovery. Third, potential confounding factors, such as the type of resuscitation fluid used, were not evaluated. Fourth, the observed reduction in CXCL12 levels and its association with mechanical IO stimulation require further validation through animal studies or in vitro bone marrow models to establish causality. Future studies should address these limitations to strengthen the evidence base and refine clinical protocols for IO procedures. Fifth, we did not record blood transfusion volumes, surgical intervention timelines, or injury severity scores (e.g., ISS), which may confound inflammatory and coagulation markers.
While IO access exacerbates inflammatory and hematopoietic disturbances, its time advantage in achieving hemodynamic stabilization remains critical when IV access fails. We recommend reserving IO for scenarios where peripheral venous cannulation is impractical, while implementing mitigation strategies (e.g., fluid warming, rate control) to minimize adverse effects.
Conclusion
Through comprehensive multidimensional monitoring, this study elucidates the dualistic role of IO access in THS resuscitation. The IO approach demonstrates clinically valuable advantages, including high procedural success rates and rapid fluid administration, making it a critical intervention for early hemodynamic stabilization. However, our findings reveal that IO access concurrently potentiates multiple pathological cascades - exacerbating systemic inflammatory dysregulation, impairing hematopoietic recovery, and aggravating coagulation-metabolic disturbances - through mechanistically distinct pathways involving direct mechanical stimulation, hypothermic fluid effects, and oxidative stress-mediated damage. Therefore, when IV access is achievable within 2 minutes, it should be prioritized. If IO is required, mitigation strategies (e.g., fluid warming, rate control) are essential.
Dodatak
Consent to publish
All authors gave final approval of the version to be published.
Availability of data and materials
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgements
Not applicable
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1344435443202110.1097/tme.0000000000000376 Jones A R Miller J L Jansen J O Wang H E Adv Emerg Nurs J Whole Blood for Resuscitation of Traumatic Hemorrhagic Shock in Adults 34699424 PMC 8555430 · doi ↗ · pubmed ↗
- 222S 13132202210.1111/vec.13126 Kuo K Palmer L J Vet Emerg Crit Care (San Antonio)Pathophysiology of hemorrhagic shock 35044060 · doi ↗ · pubmed ↗
- 399901113202310.3389/fphys.2022.999011 Dufour-Gaume F Frescaline N Cardona V Prat N J Front Physiol Danger signals in traumatic hemorrhagic shock and new lines for clinical applications 36726379 PMC 9884701 · doi ↗ · pubmed ↗
- 44715547202110.1007/s 00068-020-01327-y Tyler J A Perkins Z De'Ath H D Eur J Trauma Emerg Surg Intraosseous access in the resuscitation of trauma patients: a literature review 32078703 · doi ↗ · pubmed ↗
- 519199193115202310.4240/wjgs.v 15.i 9.1919 Liu B C Cheng M R Lang L Li L Si Y H Li A J Xu Q Zhang H World J Gastrointest Surg Autologous bone marrow infusion via portal vein combined with splenectomy for decompensated liver cirrhosis: A retrospective study 37901728 PMC 10600764 · doi ↗ · pubmed ↗
- 6In. Stat Pearls. Treasure Island (FL) ineligible companies. Disclosure: Jesse Kellar declares no relevant financial relationships with ineligible companies 2025 Dornhofer P Kellar J Z Intraosseous Vascular Access
- 711076112146202210.1111/aor.14170 Takase B Higashimura Y Asahina H Masaki N Kinoshita M Sakai H Artificial organs Intraosseous infusion of liposome-encapsulated hemoglobin (Hb V) acutely prevents hemorrhagic anemia-induced lethal arrhythmias, and its efficacy persists with preventing proarrhythmic side effects in the subacute phase of severe hemodilution model 35006625 · doi ↗ · pubmed ↗
- 817118202310.1186/s 13017-023-00487-7 Wang D Deng L Zhang R Zhou Y Zeng J Jiang H World J Emerg Surg Efficacy of intraosseous access for trauma resuscitation: a systematic review and meta-analysis 36918947 PMC 10012735 · doi ↗ · pubmed ↗