Predictive value of biochemical markers CRP, WBC, and total cholesterol for postoperative dry eye syndrome following phacoemulsification cataract surgery
Yenan Wang, Xizhe Wang, Zhen Li, Huiqing Yang, Xuxiang Zhang

TL;DR
This study shows that blood markers CRP, WBC, and cholesterol can predict dry eye syndrome after cataract surgery, with combined testing being most accurate.
Contribution
The study demonstrates that combining CRP, WBC, and total cholesterol improves prediction of postoperative dry eye syndrome.
Findings
CRP, WBC, and TC levels were significantly higher in patients who developed dry eye syndrome.
CRP, WBC, and TC were identified as independent predictors of dry eye syndrome.
The combined model of CRP, WBC, and TC achieved an AUC of 0.936, outperforming individual markers.
Abstract
Dry eye syndrome is a common complication following phacoemulsification cataract surgery, potentially influenced by systemic biochemical factors. This study aimed to evaluate the predictive efficiency of three routinely measured biochemical markers - C-reactive protein (CRP), white blood cell count (WBC), and total cholesterol (TC) - in identifying patients at risk for postoperative dry eye syndrome. A total of 87 patients undergoing phacoemulsification between January 2024 and February 2025 were enrolled and categorized into dry eye (n=49) and non-dry eye (n=38) groups. Blood samples were collected preoperatively to assess CRP, WBC, and TC levels using standard laboratory protocols. Baseline characteristics were compared, and multivariate logistic regression was conducted to identify independent risk factors. Receiver operating characteristic (ROC) curves were generated to determine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
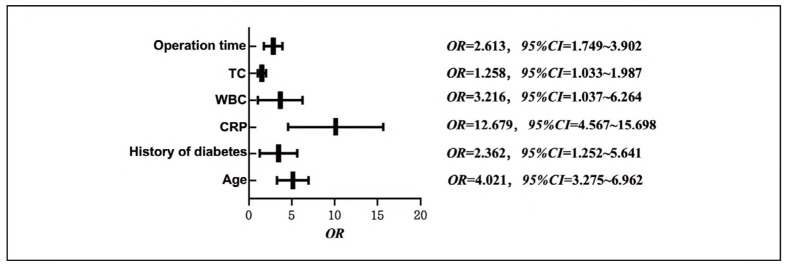 Figure 1
Figure 1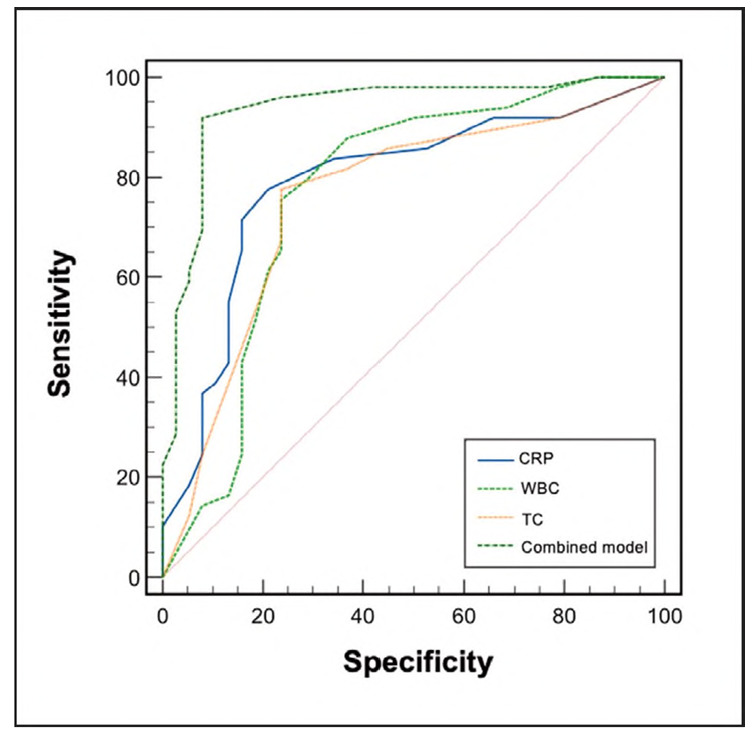 Figure 2
Figure 2| Factor | Dry Eye Group (n = 49) | Non-Dry Eye Group (n = 38) | t (χ2) / P |
|---|---|---|---|
| Age (years, x̄±s) | 62.06 ± 8.68 | 57.68 ± 8.65 | 12.178 / <0.001 |
| Male (n, %) | 34 (69.39%) | 25 (65.79%) | 0.127 / 0.722 |
| BMI (kg/m2, x̄±s) | 24.18 ± 2.46 | 24.29 ± 2.34 | -0.204 / 0.839 |
| Smoking history (n, %) | 11 (22.45%) | 10 (26.32%) | 0.175 / 0.676 |
| Alcohol consumption (n, %) | 10 (20.41%) | 9 (23.68%) | 0.135 / 0.714 |
| Hypertension history (n, %) | 13 (26.53%) | 12 (31.58%) | 0.266 / 0.606 |
| Diabetes history (n, %) | 32 (65.31%) | 10 (26.32%) | 13.030 / <0.001 |
| Duration of surgery (min, x̄±s) | 11.94 ± 1.75 | 9.89 ± 1.35 | 5.954 / <0.001 |
| Group | CRP (mg/L) | WBC (X10 /L ) | TC (mmol/L) |
|---|---|---|---|
| Dry Eye Group (n = 49) | 18.45 ± 1.11 | 6.90 ± 2.68 | 6.94 ± 2.38 |
| Non-Dry Eye Group (n = 38) | 10.50 ± 5.99 | 3.53 ± 1.50 | 4.40 ± 2.46 |
| t/P | 5.535 / <0.001 | 4.921 / <0.001 | 4.883 / <0.001 |
| Factor | Variable | Assignment |
|---|---|---|
| Age | X1 | Entered as original value |
| History of diabetes | X2 | Yes = 1, No = 0 |
| Duration of surgery | X3 | Entered as original value |
| CRP | X4 | Entered as original value |
| WBC | X5 | Entered as original value |
| TC | X6 | Entered as original value |
| Postoperative dry eye syndrome<br>after phacoemulsification | Y | Yes = 1, No = 0 |
| Variable | β | S.E. | Wald | P | OR | 95% CI |
|---|---|---|---|---|---|---|
| Age | 1.649 | 0.457 | 3.608 | <0.001 | 4.021 | 3.275-6.962 |
| History of diabetes | 2.109 | 0.506 | 4.168 | 0.006 | 2.362 | 1.252-5.641 |
| Duration of surgery | 0.960 | 0.205 | 22.011 | <0.001 | 2.613 | 1.749-3.902 |
| CRP | 1.336 | 0.418 | 3.196 | <0.001 | 12.679 | 4.567-15.698 |
| WBC | 1.862 | 0.463 | 4.022 | <0.001 | 3.216 | 1.037-6.264 |
| TC | 2.175 | 0.527 | 4.127 | <0.001 | 1.258 | 1.033-1.987 |
| Indicator | AUC | S.E. | 95%CI | Sensitivity | Specificity | Cut-off Value |
|---|---|---|---|---|---|---|
| CRP | 0.791 | 0.051 | 0.690~0.870 | 77.55 | 78.95 | >10 |
| WBC | 0.770 | 0.056 | 0.667~0.853 | 75.51 | 76.32 | >9 |
| TC | 0.757 | 0.054 | 0.653~0.843 | 77.55 | 76.32 | >5 |
| Combined Model | 0.936 | 0.029 | 0.863~0.977 | 91.84 | 92.11 | - |
| Z/PCombined Detection/CRP | 2.979/0.003 | - | - | - | - | - |
| Z/PCombined Detection/W BC | 2.761/0.006 | - | - | - | - | - |
| Z/PCombined DetectionAC | 2.746/0.006 | - | - | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Surface and Contact Lens · Glaucoma and retinal disorders · Retinal Diseases and Treatments
Introduction
Cataract ranks among the leading causes of blindness worldwide. Clinically, phacoemulsification is the primary treatment modality, characterized by small incisions, rapid recovery, and high safety. However, postoperative complications remain a significant factor affecting patients' visual quality and overall quality of life. Among these complications, dry eye syndrome is particularly common, with a short-term incidence ranging from 30% to 60% and a long-term incidence still reaching 10% to 30% [1] [2]. Dry eye syndrome not only causes ocular surface discomfort and reduced visual quality but may also delay corneal healing, increase the risk of infection, and severely impact surgical outcomes [3].
C-reactive protein (CRP) is a sensitive marker of systemic inflammation and a common acute-phase reactant. White blood cell count (WBC) reflects immune defense and infection status, while total cholesterol (TC) is closely associated with lipid metabolism and vascular endothelial function [4] [5] [6]. Previous studies have shown that elevated levels of CRP and WBC are associated with chronic inflammation of the ocular surface, and abnormal TC levels may contribute to the development of dry eye syndrome by affecting meibomian gland lipid secretion [7]. However, the predictive value of combined CRP WBC, and TC levels for postoperative dry eye syndrome following phacoemulsification remains unclear. Based on the above, this study aims to explore the predictive efficacy of combined detection of CRP, WBC, and TC by observing their dynamic changes after surgery, providing a theoretical basis for early identification of high-risk patients and the development of individualized intervention strategies.
Materials and methods
General information
A total of 87 patients who underwent phacoemulsification at our hospital between January 2024 and February 2025 were included. Inclusion criteria: (1) age >18 years; (2) diagnosis of cataract according to the World Health Organization (WHO) criteria [1], confirmed by slit-lamp examination, fundus examination, and ocular ultrasound, with all patients having Grade III lens nuclear hardness; (3) eligibility for phacoemulsification surgery with no contraindications; (4) no prior diagnosis of dry eye syndrome; (5) no autoimmune diseases, and no medications affecting CRP WBC, or TC levels within the past three months. Exclusion criteria: (1) concurrent serious ocular diseases such as uveitis or glaucoma, or a history of previous ocular surgery; (2) use of anti-inflammatory or immunomodulatory drugs within the past three months; (3) pregnant or lactating women; (4) mental disorders.
Based on the development of dry eye syndrome postoperatively, patients were divided into a dry eye group (n = 49) and a non-dry eye group (n = 38). Written informed consent was obtained from all participants and their families before the study.
Methods
Baseline data, including age, sex, and medical history, were obtained from the hospital's electronic medical records. Levels of CRP WBC, and TC were measured using standardized procedures. After an overnight fast and adequate rest, 5 mL of venous blood was collected from each patient. For CRP and WBC testing, EDTA anticoagulant tubes were used; for TC testing, plain serum tubes were used. CRP and TC were measured using Automatic Biochemical Analyzer with enzymatic colorimetric assay kits. WBC counts were analyzed using the impedance and flow cytometry technology. All samples were processed within 2 hours after collection. The laboratory participated in external quality assessment programs and implemented strict internal quality control using commercial control materials. Daily calibration and routine maintenance were conducted in accordance with the manufacturers' guidelines to ensure the precision and accuracy of all measurements.
Observation indicators
(1) Comparison of baseline characteristics between the dry eye and non-dry eye groups.
(2) Comparison of CRP WBC, and TC levels between the two groups.
(3) Multivariate logistic regression analysis of factors influencing the development of dry eye syndrome post-phacoemulsification.
(4) Receiver operating characteristic (ROC) curves and area under the curve (AUC) calculations to evaluate the predictive value of CRP, WBC, and TC for postoperative dry eye syndrome.
Statistical analysis
Data were analyzed using Statistic Package for Social Science (SPSS) 27.0 (IBM, Armonk, NY, USA). Measurement data were expressed as mean ± standard deviation (x̄ ± s), and independent samples t-tests were used for between-group comparisons. Categorical data were expressed as numbers and percentages (n (%)), and compared using the chi-square (χ^2^) test. ROC curves were plotted to assess the predictive value of CRP WBC, and TC. Multivariate logistic regression was conducted to identify risk factors for postoperative dry eye syndrome. A P-value < 0.05 was considered statistically significant.
Results
Comparison of baseline characteristics between the two groups
The dry eye group had significantly higher age, longer surgical duration, and a greater proportion of patients with a history of diabetes compared to the non-dry eye group (all P < 0.01). No statistically significant differences were observed in other baseline variables (P > 0.05). See Table 1.
Comparison of CRP, WBC, and TC levels between the two groups
The levels of CRP WBC, and TC in the dry eye group were significantly higher than those in the non-dry eye group (all P < 0.001). See Table 2.
Multivariate logistic regression analysis of risk factors for dry eye syndrome after phacoemulsification
Dry eye syndrome after phacoemulsification was set as the dependent variable, and variables with P < 0.05 in univariate analysis were included as independent variables. The assignment of variables is shown in Table 3.
Multivariate logistic regression analysis revealed that age, history of diabetes, duration of surgery, CRP, WBC, and TC were all risk factors for postoperative dry eye syndrome (OR = 4.021, 2.362, 2.613, 12.679, 3.216, 1.258; 95% CI = 1.033-15.698). See Table 4 and Figure 1.
Multivariate logistic regression analysis of risk factors for dry eye syndrome after phacoemulsification.
Predictive Value of CRP, WBC, and TC levels for postoperative dry eye syndrome after phacoemulsification
ROC curve analysis showed that CRP, WBC, and TC levels had relatively high predictive value for dry eye syndrome after phacoemulsification (AUC: 0.791, 0.770, and 0.757, respectively). The combined detection model yielded a significantly higher AUC (0.936) than any single indicator (all P < 0.05). See Table 5 and Figure 2.
Predictive value of CRP WBC, and TC levels for postoperative dry eye syndrome after phacoemulsification.
Discussion
The surgical incision in phacoemulsification can damage corneal nerves and reduce corneal sensitivity, thereby decreasing reflex tear secretion and blink frequency. A reduced blink rate not only impairs meibomian gland lipid secretion and accelerates tear evaporation, but also induces inflammatory responses and disrupts ocular surface structure. These multiple factors contribute to a vicious cycle of excessive tear evaporation, ultimately leading to dry eye syndrome [8] [9].
In this study, data showed that patients who developed dry eye syndrome postoperatively had significantly higher age, longer surgical duration, elevated CRP, WBC, and TC levels, as well as a higher proportion of diabetes history compared with those without dry eye. Multivariate logistic regression analysis confirmed these factors as independent risk factors for postoperative dry eye syndrome. Nur Faizah H et al. [10] reported a higher incidence of dry eye syndrome after phacoemulsification in cataract patients with diabetes. Bu Li et al. [11] suggested that elevated levels of inflammatory markers such as CRP in diabetic cataract patients may increase the risk of postoperative complications, including dry eye syndrome, supporting the rationale of the present study.
The underlying mechanisms may be as follows: With increasing age, lacrimal gland function declines, leading to decreased tear secretion and weakened repair capacity, thereby increasing dry eye risk [12]. Longer surgical duration prolongs ocular surface exposure, exacerbates corneal epithelial damage, and accumulates thermal injury due to phacoemulsification energy, compromising corneal nerves and tear film stability [13]. Chronic hyperglycemia induces corneal nerve degeneration and endothelial dysfunction, inhibits tear secretion, delays corneal epithelial healing, and further raises dry eye risk [14]. Elevated CRP and WBC levels indicate systemic inflammation, where inflammatory mediators can activate immune cells on the ocular surface, damaging corneal and conjunctival epithelial cells, impairing tear secretion, and aggravating tear film inflammation [15]. Hypercholesterolemia disrupts lipid metabolism and interferes with meibomian gland lipid secretion and composition. Abnormal lipid layers in the tear film accelerate tear evaporation and contribute to dry eye development [16].
Our results demonstrate that CRF, WBC, and TC each have a good predictive value for dry eye syndrome following phacoemulsification, with combined detection outperforming individual indicators. The likely reason is that CRP, as a sensitive marker of inflammation, reflects systemic inflammatory cascade activation and the upregulation of intercellular adhesion molecule-1 (ICAM-1), which promotes immune cell infiltration, damaging ocular surface tissues and disrupting tear film homeostasis. WBC count reflects immune defense status; increased neutrophils can release proteases and reactive oxygen species that harm corneal epithelial and goblet cells, affecting both tear secretion and tear film stability [17] [18]. Abnormal TC levels, linked to lipid metabolism disorders, may alter meibomian gland lipid composition, reducing tear film lipid layer fluidity and stability, thus accelerating tear evaporation [19].
The advantage of combined detection lies in the complementary nature of each biomarker: CRP identifies inflammatory activity, WBC quantifies immune response intensity, and TC reveals lipid metabolism abnormalities. This multi-parameter approach enables earlier detection of inflammation, assessment of immune-mediated tissue damage, and evaluation of tear film structure abnormalities, providing more precise identification of high-risk patients and a multidimensional basis for clinical early intervention.
This study is limited by its single-center design and relatively small sample size, which may affect the generalizability of the findings. Additionally, only short-term postoperative outcomes were evaluated, with no data on long-term follow-up. Future research should include larger, multicenter cohorts to enhance the robustness and applicability of the results. Extending the follow-up period will also provide a more comprehensive understanding of the temporal evolution and underlying mechanisms involved.
In conclusion, age, surgical duration, CRP, WBC, TC levels, and history of diabetes may all influence the development of postoperative dry eye syndrome after phacoemulsification. Among them, CRP, WBC, and TC demonstrate predictive value, with combined detection offering superior performance over single indicators. These factors may serve as a basis for early clinical prevention.
Dodatak
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 127131342023 Bhandari S Chew E Y Curr Opin Ophthalmol Cataract surgery and the risk of progression of macular degeneration 3648420710.1097/ICU.0000000000000909 PMC 9752199 · doi ↗ · pubmed ↗
- 2591459942202310.5937/jomb 0-37338 Wang X Zhang Z Ge Y Q Wu X Ma Y C J Med Biochem The effect of calcium dobesilate combined with hypoglycemic drugs in the treatment of cataract NPDR and its effect on fundus microcirculation and blood ICAM-1, MCP-1 and MIF levels 38084239 PMC 10710796 · doi ↗ · pubmed ↗
- 3101141017261202310.1007/s 00417-022-05880-7 Chen N Zhang J S Zhang T X Fan B L Ning Y Graef Arch Clin Exp The effect of sodium hyaluronate on tear film stability in patients with dry eye syndrome after cataract surgery 36378338 · doi ↗ · pubmed ↗
- 415409154561202310.1515/cclm-2023-0086 Plebani M Clin Chem Lab Med Why C-reactive protein is one of the most requested tests in clinical laboratories?36745137 · doi ↗ · pubmed ↗
- 5537253947202410.1038/s 41440-023-01528-z Tsuda K Hypertens Res A link between white blood cell count and blood pressure levels 38001165 · doi ↗ · pubmed ↗
- 6CD 01377522202310.1002/14651858.cd 013775.pub 2 Perais J Agarwal R Evans J R Loveman E Colquitt J L Owens D et al Cochrane Db Syst Rev Prognostic factors for the development and progression of proliferative diabetic retinopathy in people with diabetic retinopathy PMC 994391836815723 · doi ↗ · pubmed ↗
- 7671221202110.1007/s 11892-021-01418-z Go J A Mamalis C A Khandelwal S S Curr Diabetes Rep Cataract Surgery Considerations for Diabetic Patients 34967932 · doi ↗ · pubmed ↗
- 818125202510.1186/s 12886-024-03841-8 Ta H Mc Cann P Xiao M Lien T Abbott K Gregory D G et al Bmc Ophthalmol Dry eye post-cataract surgery: a systematic review and meta-analysis 39806338 PMC 11726945 · doi ↗ · pubmed ↗