Prognostic value of surfactant protein D and biochemical markers in BALF and plasma of ARDS patients undergoing mechanical ventilation
Hu Han, Litao Zhang, Zhangshun Shen, Ranliang Hua, Lingling Li, Hui Guo

TL;DR
This study shows that surfactant protein D levels in lung fluid and blood, along with lactate and pH, can predict survival in ARDS patients on ventilators.
Contribution
The study demonstrates the prognostic value of SP-D in BALF and plasma for ARDS patients.
Findings
SP-D levels in BALF and plasma were significantly higher in non-survivors.
Lactate levels were elevated and pH was lower in the death group.
A combined biomarker model achieved an AUC of 0.883 for predicting 28-day mortality.
Abstract
Surfactant protein D (SP-D) and circulating exosomes have emerged as potential biochemical indicators of lung injury severity in acute respiratory distress syndrome (ARDS). This study aimed to evaluate the prognostic value of SP-D levels and selected biochemical parameters in bronchoalveolar lavage fluid (BALF) and plasma among ARDS patients receiving mechanical ventilation. A total of 103 mechanically ventilated ARDS patients were enrolled between February 2020 and February 2023. Patients were classified into survival (n = 59) and death (n=44) groups based on 28-day mortality. On the day of diagnosis, SP-D and exosome levels in BALF and plasma, along with pH, lactate, and oxygenation-related indices, were measured and analyzed for prognostic relevance. SP-D levels in both BALF and plasma were significantly higher in non-survivors (P < 0.001), while exosome levels did not differ…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
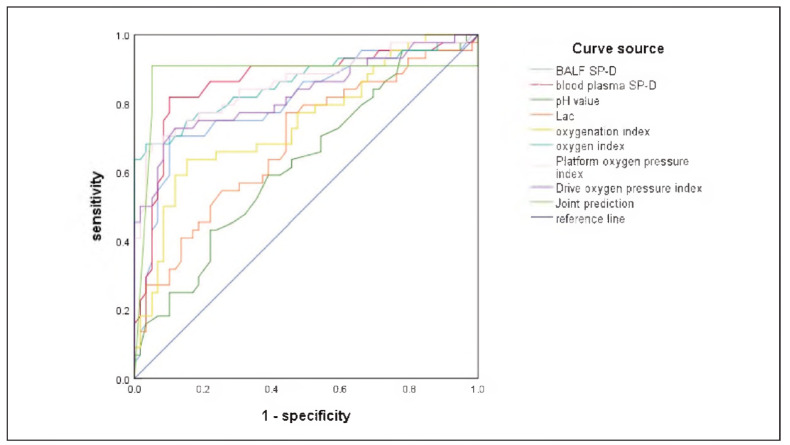 Figure 1
Figure 1| Group | Age (year) | Sex | BMI (kg/m2) | Weight (kg) | |
|---|---|---|---|---|---|
| male | female | ||||
| Survival group<br>(n=59) | 52.15±5.66 | 42 (71.19) | 17 (28.81) | 22.16±3.16 | 62.15±6.45 |
| Death group<br>(m=44) | 51.26±4.98 | 29 (65.91) | 15 (34.09) | 22.23±2.98 | 61.98±7.15 |
|
| 0.830 | 0.328 | -0.114 | 0.126 | |
|
| 0.408 | 0.567 | 0.910 | 0.900 | |
| Group | Basic aetiology | ||||
| Severe pneumonia | Multiple inj'ury | Septic shock | Cerebral apoplexy | Severe pancreatitis | |
| Survival group<br>(n=59) | 10(16.95) | 15(25.42) | 12(20.34) | 5(8.47) | 17(28.81) |
| Death group<br>(m=44) | 12(27.27) | 8(18.18) | 6(13.64) | 4(9.09) | 14(31.82) |
|
| 2.584 | ||||
|
| 0.630 | ||||
| Group | Exosome (mL-1) | SP-D (μmg/mL) |
|---|---|---|
| Survival group (n=59) | 26.78±1.65 | 29.26±2.12 |
| Death group (m=44) | 26.22±1.23 | 94.26±5.46 |
|
| 1.892 | -83.500 |
|
| 0.061 | <0.001 |
| Group | Exosome (mL-1) | SP-D (μg/mL) |
|---|---|---|
| Survival group (n=59) | 25.54±2.12 | 19.26±1.46 |
| Death group (m=44) | 25.03±2.31 | 42.12±6.45 |
|
| 1.162 | -26.373 |
|
| 0.248 | <0.001 |
| Group | pH value | PaO2 (mmHg) | PaCO2 (mmHg) | Lac (mmol/L) |
|---|---|---|---|---|
| Survival group (n=59) | 7.44±0.12 | 83.85±34.12 | 44.45±15.26 | 2.11±1.02 |
| Death group (m=44) | 7.38±0.13 | 78.44±46.26 | 45.11±15.68 | 2.87±1.26 |
|
| 2.422 | 0.683 | -0.215 | -3.381 |
|
| 0.017 | 0.496 | 0.831 | 0.001 |
| Group | Oxygenation index | Oxygen index | Platform oxygen pressure index | Drive oxygen pressure index |
|---|---|---|---|---|
| Survival group (n=59) | 181.55±56.12 | 7.35±2.12 | 12.66±6.12 | 8.77±3.56 |
| Death group (m=44) | 124.62±66.45 | 17.88±5.16 | 28.45±9.26 | 18.44±6.97 |
|
| 4.706 | -14.171 | -10.407 | -9.181 |
|
| <0.001 | <0.001 | <0.001 | <0.001 |
- —A Comparative Study on the Effects of High-Concentration Oxygen Inhalation and Good PEEP Levels on Lung Injury (20170034)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Respiratory Support and Mechanisms · Sepsis Diagnosis and Treatment
Introduction
Acute Respiratory Distress Syndrome (ARDS) is a severe, acute, and progressive pulmonary condition marked by extensive alveolar damage and impaired gas exchange [1] [2] [3]. Epidemiological data indicate that ARDS affects up to 10% of the population and carries a mortality rate ranging from 27% to 37%, posing a significant clinical and public health burden [4] [5]. While mechanical ventilation remains the primary supportive therapy to maintain oxygenation and carbon dioxide elimination, it may also induce ventilator-associated lung injury due to alveolar overdistension or oxygen toxicity, thus complicating prognosis [6] [7]. As a result, there is a pressing need for reliable biomarkers to assess disease severity and guide clinical decision-making in ARDS.
Beyond ventilatory parameters, biochemical indicators are increasingly recognized for their potential prognostic value in ARDS. The oxygenation index (PaO_2_/FiO_2_), a physiological marker widely used in clinical practice, is closely correlated with mortality in critically ill ARDS patients [8]. In parallel, circulating exosomes - nanovesicles carrying proteins, nucleic acids, and lipids - are involved in intercellular communication and may reflect the extent of systemic inflammation and alveolar-capillary barrier disruption during ARDS. Surfactant protein D (SP-D), a pulmonary collectin predominantly secreted by alveolar epithelial cells, plays a critical role in innate immune defense and lung homeostasis. Elevated serum levels of SP-D have been associated with increased disease severity and worse outcomes in ARDS [9].
Given these insights, evaluating SP-D and exosome levels in both plasma and bronchoalveolar lavage fluid (BALF) may offer clinically relevant biochemical markers to predict prognosis in ARDS patients. This study was therefore conducted to explore the relationship between the oxygenation index, SP-D and exosome concentrations in BALF and plasma, and 28-day mortality among mechanically ventilated ARDS patients. The results are reported below.
Materials and methods
General information
This prospective observational study was conducted from February 2020 to February 2023 and included 103 patients diagnosed with acute respiratory distress syndrome (ARDS) who received mechanical ventilation at our hospital. Patients were divided into two groups based on their 28-day survival: the survival group (n = 59) and the death group (n = 44). There were no statistically significant differences in baseline characteristics between the two groups (P > 0.05), as shown in Table 1. The study protocol was approved by the hospital's ethics committee, and written informed consent was obtained from all patients or their legal representatives.
Inclusion criteria:
(1) Diagnosis of ARDS based on the consensus definition of the European and American conferences [10];
(2) Age between 19 and 65 years;
(3) No recent history (within three months) of high-dose antibiotic or immunosuppressant use;
(4) Availability of complete clinical and laboratory data
Exclusion criteria:
(1) Patients who did not complete the entire treatment course at our institution, were transferred to another facility, or discharged prematurely;
(2) Patients with a prior history of respiratory disease treatment or those with recurrent ARDS episodes;
(3) Presence of severe autoimmune diseases;
(4) Diagnosed malignancies;
(5) Death within five days of hospital admission.
Sample collection:
Peripheral venous blood and bronchoalveolar lavage fluid (BALF) were collected from all participants on the day of diagnosis. Venous blood samples were centrifuged at 2,500 rpm (radius 14 cm) for 10 minutes at room temperature, and the resulting serum was harvested for biochemical analysis. BALF was obtained using fiberoptic bronchoscopy under local anesthesia. The bronchoscope was advanced into the right middle lobe bronchus, where 50 mL of sterile 0.9% sodium chloride solution at 37°C was instilled and then aspirated twice. The retrieved lavage fluid was immediately filtered through sterile gauze to remove mucus and debris, followed by centrifugation at 2,500 rpm (radius 14 cm) for 10 minutes. The supernatant was collected and stored for further analysis.
Exosome quantification:
Exosome size distribution and concentration in BALF and plasma were measured using nanoparticle tracking analysis (NTA), which detects particles based on Brownian motion and light scattering. The total concentration of exosomes was expressed as particles/mL, and natural logarithmic transformation was applied to the values for statistical analysis.
SP-D detection:
Surfactant protein D (SP-D) concentrations in both BALF and plasma were quantified using commercially available enzyme-linked immunosorbent assay (ELISA) kits (Roche, Shanghai, China), following the manufacturer's instructions. All samples were measured in duplicate to ensure analytical precision.
Arterial blood gas and derived indices:
Immediately after diagnosis, arterial blood samples were collected and analyzed using an automated blood gas analyzer (Cobas B123, Roche) to measure pH, arterial oxygen partial pressure (PaO_2_), and the fraction of inspired oxygen (FiO_2_). From these parameters, the following ventilatory indices were calculated:
Plateau pressure-oxygenation index: Pplat X 100 X FiO_2_/PaO_2_
Driving pressure-oxygenation index: P X 100 X FiO_2_/PaO_2_
Observation indicators
The primary biochemical indicators assessed on the day of diagnosis included SP-D and exosome levels in both BALF and plasma. In addition, arterial blood gas variables (pH, PaO2, lactate) and mechanical ventilation parameters were recorded. The relationship between these biochemical and physiological parameters and the 28-day prognosis was subsequently analyzed.
Statistical analysis
Data were processed using Statistic Package for Social Science (SPSS) 23.0 software (IBM, Armonk, NY, USA). Categorical variables such as sex and underlying etiology were analyzed by chi-square test. Continuous variables such as age, BMI, exosome content, and SP-D levels were analyzed by t-test. A p-value < 0.05 was considered statistically significant.
Results
Comparison of exosome and SP-D levels in BALF
As shown in Table 2, there was no statistically significant difference in the concentration of exosomes in bronchoalveolar lavage fluid (BALF) between the survival and death groups (P > 0.05). In contrast, BALF SP-D levels were markedly higher in the death group compared to the survival group (P < 0.05), suggesting a potential association between elevated SP-D and adverse clinical outcomes.
Comparison of plasma exosome and SP-D levels
Similarly, no significant differences in plasma exosome levels were observed between the two groups (P > 0.05). However, plasma SP-D concentrations were significantly elevated in the death group relative to the survival group (P < 0.05), as demonstrated in Table 3.
Comparison of arterial blood gas parameters
As shown in Table 4, arterial oxygen partial pressure (PaO_2_) and carbon dioxide partial pressure (PaCO_2_) did not differ significantly between groups (P > 0.05). However, patients in the death group exhibited significantly lower arterial pH values and higher lactate concentrations compared to those in the survival group (P < 0.05), indicating more profound metabolic derangements and tissue hypoxia.
Comparison of mechanical ventilation parameters
Mechanical ventilation parameters are presented in Table 5. Compared with the survival group, the death group showed significantly lower oxygenation index (PaO_2_/FiO_2_) values, alongside increased oxygen index, plateau pressure-oxygenation index, and driving pressure-oxygenation index (all P < 0.05). These findings suggest more severe respiratory impairment and ventilatory dependence in non-survivors.
Predictive value of SP-D, blood gas indicators, and ventilation parameters
Receiver Operating Characteristic (ROC) curve analysis was performed to evaluate the prognostic performance of each parameter. As shown in Table VI and Figure 1, the area under the curve (AUC) for BALF SP-D and plasma SP-D were 0.804 and 0.864, respectively, both indicating strong predictive value. Additional parameters with notable predictive ability included oxygen index (AUC = 0.861), plateau pressure-oxygenation index (AUC = 0.857), and driving pressure-oxygenation index (AUC = 0.828).
Path diagram of mediation analysis. (Note: Figure 1 represents the mediation analysis path diagram of inflammatory factors on the relationship between glycemic abnormalities and disease severity. A-C represent the mediating effects of IL-6, WBC and hs-CRP, respectively).
The combination of these high-performing indicators (AUC > 0.750) yielded an overall AUC of 0.883, surpassing the predictive value of any single parameter. This combined biomarker approach demonstrated high sensitivity (0.909) and specificity (0.849) for predicting 28-day mortality in ARDS patients.
Discussion
Acute Respiratory Distress Syndrome (ARDS) is a life-threatening pulmonary condition typically induced by severe infections, trauma, or exposure to harmful inhalants, leading to diffuse alveolar injury and impaired gas exchange [11] [12]. Although its pathogenesis is multifactorial and not yet fully elucidated, ARDS is largely driven by an exaggerated systemic inflammatory response. This cascade results in the recruitment of inflammatory cells to the lungs, excessive cytokine release, increased alveolar-capillary permeability, and subsequent pulmonary edema [13] [14] [15]. These changes compromise lung compliance and oxygenation capacity, frequently resulting in hypoxemia and multi-organ dysfunction. Mechanical ventilation remains a critical supportive intervention; however, its efficacy varies and may itself contribute to ventilator-induced lung injury. Hence, the identification of reliable biochemical and physiological markers for prognosis is crucial to guide therapeutic strategies and improve patient outcomes.
Among candidate biomarkers, surfactant protein D (SP-D) has gained considerable attention. SP-D is a collagen-containing C-type lectin produced primarily by alveolar epithelial type II cells and plays an integral role in pulmonary host defense and surfactant homeostasis [16]. In the present study, we found significantly higher SP-D levels in both bronchoalveolar lavage fluid (BALF) and plasma in patients who succumbed to ARDS, compared to survivors. This suggests that elevated SP-D reflects heightened alveolar epithelial injury and systemic inflammation, both of which are linked to poorer prognosis. During mechanical ventilation, lung tissue may be subjected to cyclic overdistension and oxidative stress, resulting in increased release of SP-D into the alveolar space and systemic circulation [17]. High SP-D levels may therefore indicate a maladaptive inflammatory response and impaired alveolar-capillary integrity. Previous studies have also proposed that SP-D contributes to epithelial cell apoptosis by modulating cas- pase-related pathways, further exacerbating lung injury and worsening clinical outcomes [18].
Conversely, our data showed no statistically significant difference in exosome concentrations between the survival and death groups. While exosomes are recognized carriers of various bioactive molecules—including proteins, RNAs, and lipids— that mirror the functional state of their parent cells, their prognostic value in ARDS remains uncertain. It is possible that the molecular composition of exosomes, rather than their concentration alone, may be more predictive of patient outcomes. Additionally, differences in exosome origin, isolation techniques, and quantification methods may contribute to inconsistencies in their assessment. Therefore, future research should focus on characterizing the molecular cargo of exosomes and elucidating their functional roles in the pathophysiology of ARDS.
Biochemical analysis of blood gas parameters revealed that patients in the death group had significantly lower pH and elevated lactate levels. These findings are consistent with metabolic acidosis secondary to systemic hypoperfusion and cellular hypoxia, reflecting inadequate tissue oxygenation in the context of severe lung injury [19]. Lactate accumulation and acidemia have long been associated with poor prognosis in critically ill patients, including those with ARDS.
Additionally, we evaluated a panel of ventilatory indices including the oxygenation index (PaO_2_/FiO_2_), oxygen index, plateau pressure-oxygenation index, and driving pressure-oxygenation index. Lower oxygenation index and higher values of the other indices in non-survivors indicate more severe impairment in pulmonary function and increased dependence on mechanical ventilatory support. These metrics serve not only as clinical severity indicators but also as indirect reflections of alveolar-capillary damage and altered lung mechanics [20].
ROC analysis demonstrated that SP-D levels in both BALF and plasma, as well as lactate, pH, and oxygenation-related indices, each possess independent prognostic value. Notably, combining multiple high-performing biomarkers—specifically those with AUC values greater than 0.75—resulted in the highest predictive accuracy for 28-day mortality (AUC = 0.883, sensitivity = 0.909, specificity = 0.849). These findings highlight the importance of a multiparameter biochemical approach to ARDS risk stratification. Early assessment of SP-D, lactate, and ventilatory indices may facilitate the identification of patients at increased risk of mortality, thereby enabling more timely and targeted interventions.
In summary, this study demonstrates that elevated SP-D levels in BALF and plasma, together with key biochemical and ventilatory parameters, are significantly associated with poor prognosis in mechanically ventilated ARDS patients. These biomarkers may serve as valuable tools for early risk assessment and personalized management in critical care settings.
Dodatak
Funding
This work was supported by the A Comparative Study on the Effects of High-Concentration Oxygen Inhalation and Good PEEP Levels on Lung Injury (20170034).
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1459372402022 Gragossian A Siuba M T Emerg Med Clin N Am Acute Respiratory Distress Syndrome 10.1016/j.emc.2022.05.002PMC 908550835953211 · doi ↗ · pubmed ↗
- 21145103581156400202210.1016/s 0140-6736(22)01485-4 Bos L Ware L B Lancet Acute respiratory distress syndrome: causes, pathophysiology, and phenotypes 36070787 · doi ↗ · pubmed ↗
- 3209221843202410.5937/jomb 0-45340 Jing P Wu C Du C Zhou L Gu L J Med Biochem Predictive value of plasma s ICAM-1 and s P-Selectins in the risk of death in patients with acute respiratory distress syndrome 38699690 PMC 11062343 · doi ↗ · pubmed ↗
- 4S 8712 Supplement 29824202310.1097/pcc.0000000000003161 Yehya N Smith L Thomas N J Steffen K M Zimmerman J Lee J H et al Pediatr Crit Care Me Definition, Incidence, and Epidemiology of Pediatric Acute Respiratory Distress Syndrome: From the Second Pediatric Acute Lung Injury Consensus Conference 36661438 · doi ↗ · pubmed ↗
- 5524753423202210.1097/pcc.0000000000002961 De Luca D Tingay D G van Kaam A H Courtney S E Kneyber M Tissieres P et al Pediatr Crit Care Me Epidemiology of Neonatal Acute Respiratory Distress Syndrome: Prospective, Multicenter, International Cohort Study 35543390 · doi ↗ · pubmed ↗
- 6606461846202010.1007/s 00134-020-05942-6 Spinelli E Mauri T Beitler J R Pesenti A Brodie D Intens Care Med Respiratory drive in the acute respiratory distress syndrome: pathophysiology, monitoring, and therapeutic interventions PMC 722413632016537 · doi ↗ · pubmed ↗
- 75145525201202010.1164/rccm.201907-1283 ci Abrams D Schmidt M Pham T Beitler J R Fan E Goligher E C et al Am J Respir Crit Care Mechanical Ventilation for Acute Respiratory Distress Syndrome during Extracorporeal Life Support. Research and Practice 31726013 · doi ↗ · pubmed ↗
- 8e 1429010202210.7717/peerj.14290 Hueda-Zavaleta M Copaja-Corzo C Miranda-Chávez B Flores-Palacios R Huanacuni-Ramos J Mendoza-Laredo J et al Peerj Determination of Pa O 2/Fi O 2 after 24 h of invasive mechanical ventilation and Delta Pa O 2/Fi O 2 at 24 h as predictors of survival in patients diagnosed with ARDS due to COVID-1936530414 PMC 9756861 · doi ↗ · pubmed ↗