Preferences for Shared Language for Health Equity Across the Political Spectrum
Samantha X. Y. Wang, Sujin Song, Margaret C. Nikolov, Zakary Tormala, Robert M. Kaplan, Kevin Schulman

TL;DR
This study finds that using inclusive and collective language can help bridge political divides in understanding health equity concepts.
Contribution
The study identifies specific language and framing preferences that can increase cross-ideological receptiveness to health equity initiatives.
Findings
Terms like 'accessible health care' and 'community health' were broadly well received across political groups.
Collectivist and affirming language (e.g., 'we', 'support') was consistently preferred over individualistic or divisive language.
Health equity was more strongly aligned with personal values than health equality, especially among conservative respondents.
Abstract
Are differences in language and framing associated with public receptiveness to health equity concepts across political ideology groups? In this survey study including 1000 US adults, a higher proportion of respondents endorsed personal values alignment with health equity than health equality definitions. The terms marginalized communities and inclusive health care elicited divergent reactions, whereas accessible health care, health care investment, population health, and community health were broadly well received; across all groups, collectivist, affirming, action-oriented statement framings (eg, we, start, support, increase) were preferred. These findings suggest that strategic use of language emphasizing shared values and collective action may increase public understanding and receptiveness to health equity initiatives. This survey study of US adults explores the alignment of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
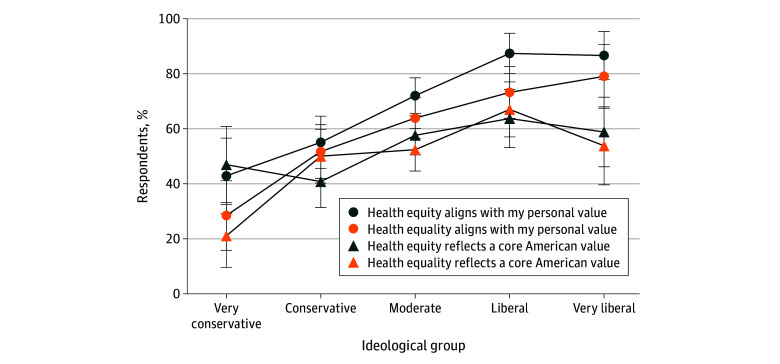 Figure 1
Figure 1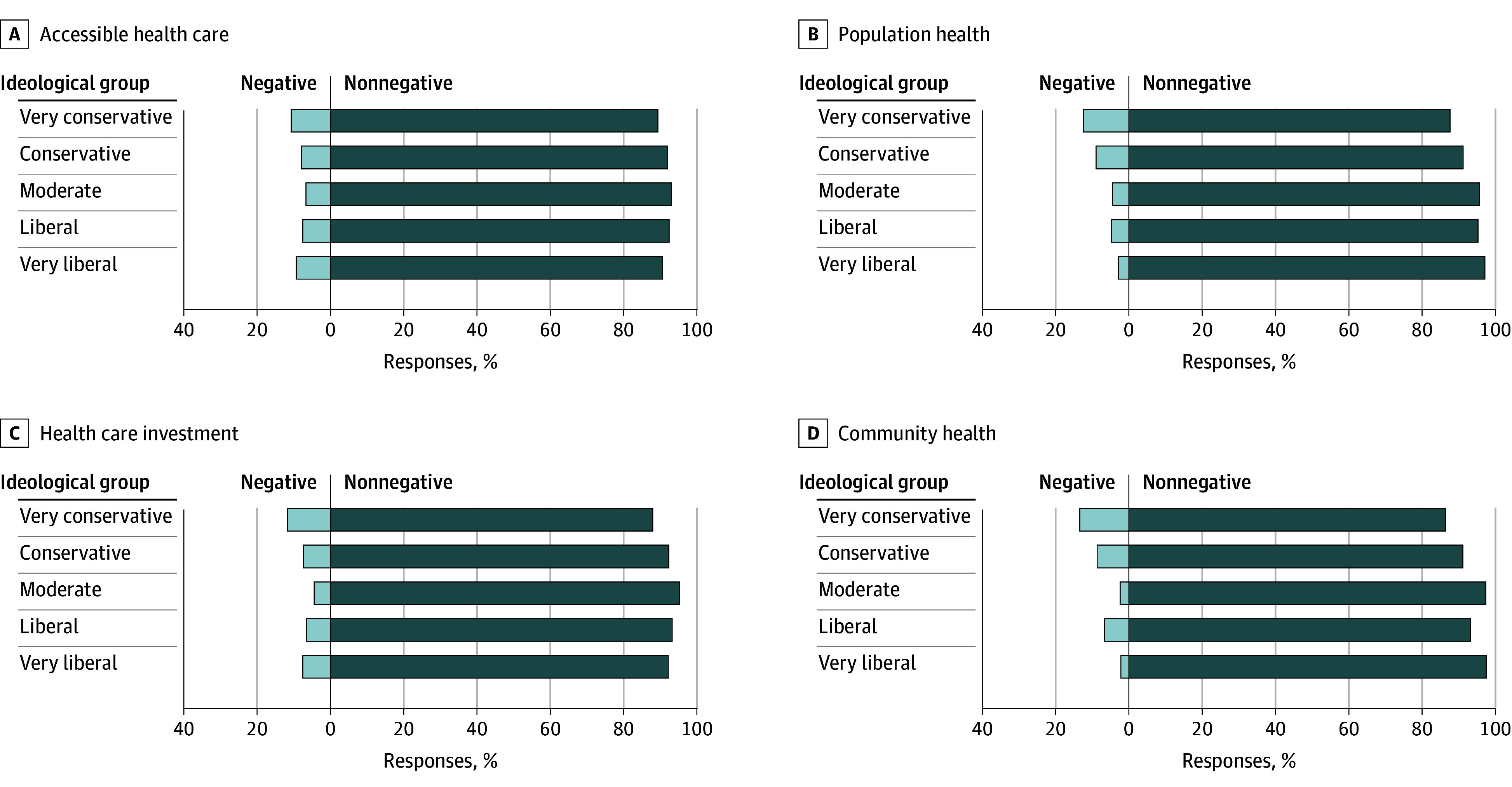 Figure 2
Figure 2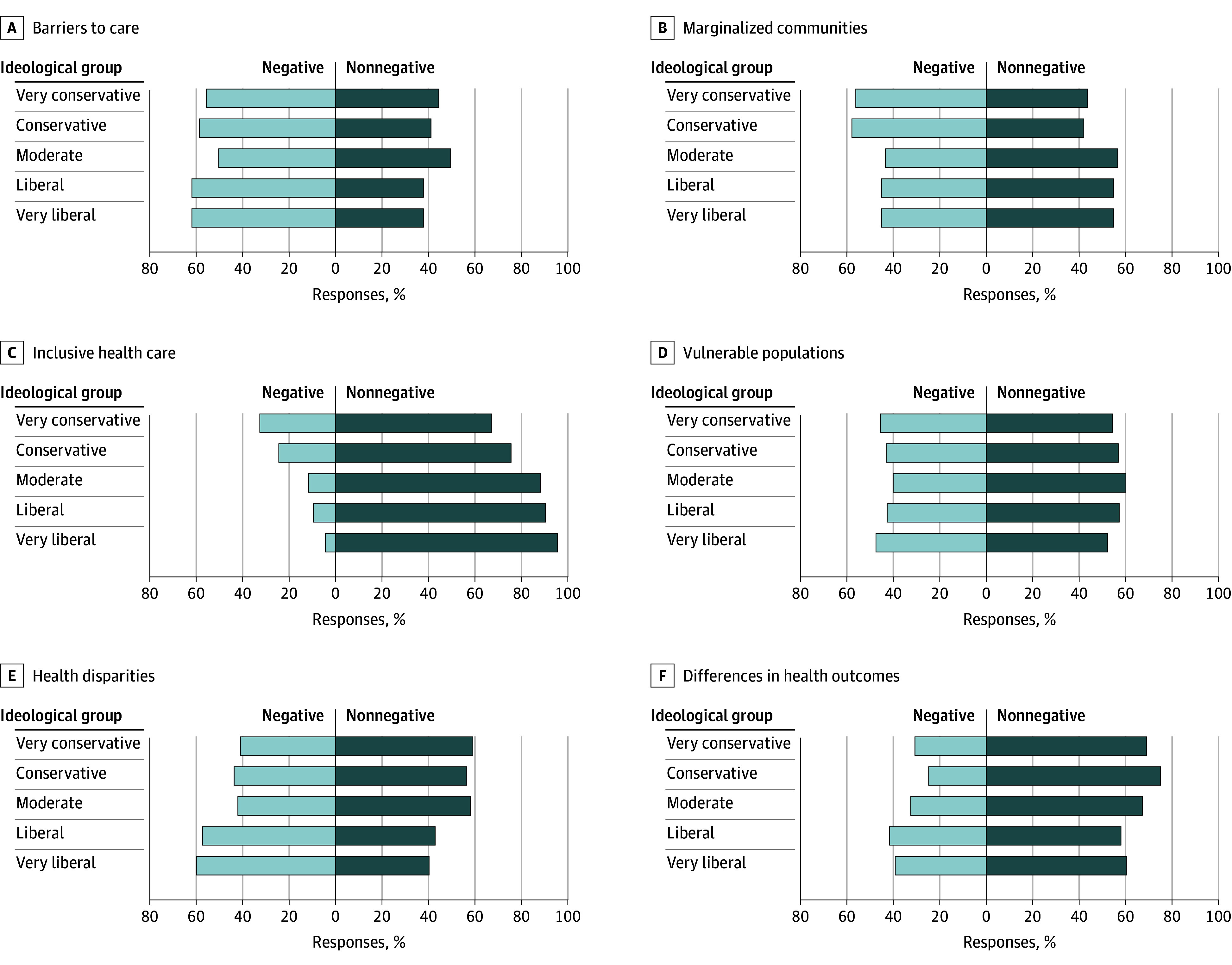 Figure 3
Figure 3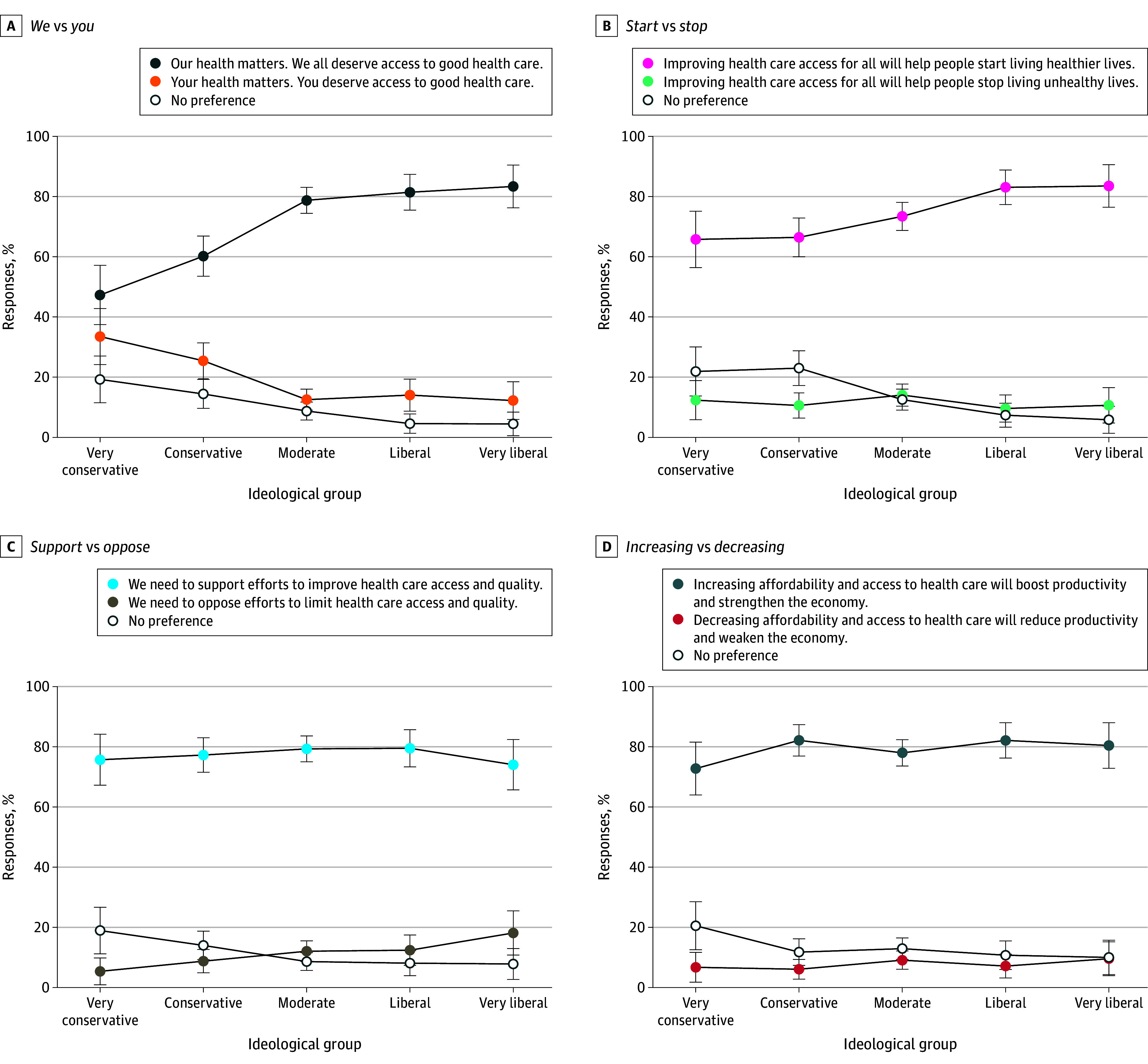 Figure 4
Figure 4| Characteristic | Weighted No. (%) |
|---|---|
| Ideology: In general, how would you describe your own political viewpoint? | |
| Very liberal | 105.8 (10.6) |
| Liberal | 164.0 (16.4) |
| Moderate | 344.0 (34.4) |
| Conservative | 205.9 (20.6) |
| Very conservative | 98.7 (9.9) |
| Not sure | 81.5 (8.2) |
| Insurance (may be >1): Are you currently covered by any of the following types of health insurance or health coverage plans? | |
| Public (includes public plus private) | 416.6 (41.7) |
| Private only | 430.2 (43.0) |
| Other | 36.1 (3.6) |
| Uninsured | 114.4 (11.4) |
| General health condition: Would you say your health in general is excellent, very good, good, fair, or poor? | |
| Excellent | 253.3 (25.3) |
| Very good | 274.6 (27.4) |
| Good | 309.0 (30.9) |
| Fair | 129.0 (12.9) |
| Poor | 34.0 (3.4) |
| Serious health events: In the past 12 mo, have you experienced any of the following serious health events? | |
| Hospitalization | 97.7 (9.7) |
| Major surgery | 59.2 (5.9) |
| Emergency care | 55.0 (5.5) |
| Diagnosis serious condition | 61.4 (6.1) |
| None of the above | 811.4 (81.1) |
| Age range, y | |
| 18-24 | 106.6 (10.7) |
| 25-34 | 172.7 (17.2) |
| 35-44 | 181.5 (18.2) |
| 45-54 | 144.0 (14.4) |
| 55-64 | 183.4 (18.3) |
| 65-74 | 146.1 (14.6) |
| ≥75 | 65.7 (6.6) |
| Sex: Are you…? | |
| Male | 486.8 (48.7) |
| Female | 513.2 (51.3) |
| Race and ethnicity: What racial or ethnic group best describes you? | |
| Asian or Asian American | 29.3 (2.9) |
| Black or African American | 124.6 (12.5) |
| Hispanic or Latino | 105.1 (10.5) |
| Middle Eastern | 3.9 (0.4) |
| Native American | 18.2 (1.8) |
| White | 664.7 (66.5) |
| Multiracial | 29.0 (2.9) |
| Other (unspecified) | 25.1 (2.5) |
| Hispanic ethnicity: Are you of Spanish, Latino, or Hispanic origin or descent? | |
| Yes | 160.6 (16.1) |
| No | 839.4 (83.9) |
| Marital status: What is your marital status? | |
| Married or partnered | 525.9 (52.6) |
| Previously married | 175.6 (17.6) |
| Never married | 298.5 (29.9) |
| Educational attainment: What is the highest level of education you have completed? | |
| Did not graduate from high school | 69.6 (7.0) |
| High school graduate | 314.3 (31.4) |
| Some college or Associate’s degree | 278.6 (27.9) |
| Bachelor’s degree | 214.7 (21.5) |
| Postgraduate degree (MA, MBA, MD, JD, PhD, etc) | 122.8 (12.3) |
| Employement: Which of the following best describes your current employment status? | |
| Employed | 513.1 (51.3) |
| Unemployed | 79.3 (7.9) |
| Student | 51.8 (5.2) |
| Permanently disabled | 61.9 (6.2) |
| Not in labor force | 293.8 (29.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNursing Education, Practice, and Leadership · Health Policy Implementation Science · Community Health and Development
Introduction
Recent changes in federal policy have altered the landscape of public health programs, including reductions in funding for disease surveillance, prevention initiatives, community health infrastructure, and equity-focused efforts.^1,2,3,4^ These changes have occurred in the context of long-standing underinvestment in public health.^5^ These shifts have raised questions about how the public perceives current health equity efforts and whether communication strategies can bridge differences in understanding across ideological groups. Recent federal actions have challenged public health infrastructure and curtailed programs designed to reduce health disparities and advance population health.^6,7,8,9^ While these steps are a clear political response to public health initiatives, it is not clear if these actions represent the interests and values of the broader public.
Research has shown that both topic and context shape the effectiveness of health and science messaging and that audience values, including political ideology, influence how messages are received.^10^ This concept has been described as information framing.^11,12^ While no single framing approach resonates uniformly across the political spectrum, emerging evidence suggests that certain message attributes, such as emphasizing personal responsibility, economic stability, or national strength, may hold greater appeal for some, whereas others may respond more positively to frames invoking fairness, community care, or systemic change.^13,14,15^ Even small linguistic differences have been shown to affect public perception and policy support in areas ranging from the opioid crisis^16,17^ to childhood obesity,^18^ beverage regulation,^19,20^ and climate change.^14,15,16,19,20,21^
Strategic message framing has been proposed as a tool to strengthen public and legislative support for population health initiatives.^22^ However, as the discourse around equity-oriented programs has become increasingly contested, it remains unclear how specific health equity terms and concepts are received by the public. To examine how language influences receptiveness to health equity concepts, we conducted a national cross-sectional online survey of US adults in which participants assessed the alignment of health equity or health equality definitions with personal values and perceived national identity values (termed American values in the survey), reported reactions to commonly used health equity terms, and indicated their framing preferences by choosing between paired public health statements. We hypothesized that receptiveness to health equity language and framing would vary across political ideological groups, with some terms and messages eliciting broader acceptance than others.
Methods
Population Sample
We conducted this survey study in partnership with YouGov, an international public opinion research firm that recruits participants from a large, opt-in online panel and constructs samples to approximate national representativeness through matching and weighting procedures. Because the YouGov panel is nonprobability based and no pilot data were available to guide expected effect sizes, we did not perform an a priori power calculation. Instead, a target sample of 1000 respondents was selected because this size yields stable weighted estimates and is consistent with standard practice in national public opinion research for enabling subgroup comparisons.^23,24^ Political ideology was self-reported using standard YouGov response categories without additional prompts or definitions provided. Race and ethnicity were self-reported by participants using fixed categories provided in the survey instrument (Asian or Asian American, Black or African American, Hispanic or Latino, Middle Eastern, Native American [American Indian or Alaska Native], White, multiracial, or other [unspecified]), which were based on US Census classifications. Race and ethnicity were assessed because perceptions of health equity–related language may vary across social groups and differential experiences of health care in the US. Sampling frames were derived from US Census and election data, and respondents were matched to these frames on sex, age, race and ethnicity, and educational attainment using propensity score methods. Poststratification weights were applied to align with demographic and voting benchmarks. Data collection occurred between April 9 and April 25, 2025. The study was approved by the Stanford Institutional Review Board, and all participants provided electronic informed consent before beginning the survey. This study adheres to the American Association for Public Opinion Research (AAPOR) reporting guidelines for survey studies.
Survey Instrument
Consistent with the AAPOR standards, we report the sampling frame, recruitment and matching procedures, weighting approach, survey administration details, and analytical methods. The survey instrument (eAppendix in Supplement 1) was developed by the coauthor team of social scientists with expertise in survey methodology and health communication (S.X.Y.W., Z.T., R.M.K., and K.S.), and through iterative review to optimize clarity and minimize ambiguity. The survey consisted of 3 modules. In the first module, Personal and Perceived American Values, respondents were randomly assigned (1:1) to view a definition of either health equity or health equality. To minimize confusion and potential carryover effects, respondents were randomized to respond to a single definition. After reading the assigned definition, participants rated the extent to which it aligned with their personal values and their perception of core American values on a 5-point Likert scale. Core American values were intentionally left undefined to capture the participant’s own interpretations. In the second module, Evaluative Reactions to Terms, participants rated their reactions to common terms used in health equity initiatives on a 7-point scale (−3, very negative; 0, neutral; +3, very positive). In the third module, Framing Preferences, participants reviewed 4 pairs of semantically equivalent public health statements that differed only in framing and selected their preferred framing or indicated no preference. The 4 pairs of statements included variations in we vs you, support vs oppose, increase vs decrease, and start vs stop framing.
Modules 2 and 3 were designed to be independent of module 1. They contained separate content and did not reference the assigned definition in module 1. Terms and framings were presented without reminders of earlier material. Thus, no carryover effects were expected.
Statistical Analysis
To assess national representativeness, we compared the weighted demographic characteristics of the analytic sample with US population estimates from the American Community Survey, a nationally representative survey conducted by the US Census Bureau.^25^ Consistent with YouGov’s weighting approach, the correspondence across key demographic variables aligned closely with population benchmarks. These comparisons are provided in the eTable in Supplement 1. For module 1, we calculated the proportion of respondents agreeing or strongly agreeing that the assigned definition aligned with personal or American values. Because respondents viewed only 1 definition, differences reflect between-group comparisons rather than within-person preferences. For module 2, we evaluated the relative frequency of negative (−3, −2, or −1) vs nonnegative (0, +1, +2, or +3) reactions to 10 terms. For module 3, we examined preferences for each framing pair, including no preference. Both unweighted and weighted results were examined; results with and without weights were comparable, and weighted results are reported herein. The χ^2^ test of association was used to assess differences in agreement, reaction, and preference by ideology. One-sided P < .05 was considered statistically significant. Standard methods for proportions were used to construct (pointwise) 95% CIs for agreement (module 1), terms (module 2), and framing preference (module 3) by political ideology. Given the potential reduction in power when dichotomizing an ordinal measure (module 2), Kruskal-Wallis rank sum tests were conducted as well to assess ideological differences in reaction to terms. All analyses were conducted in R software, version 4.2.1 (R Project for Statistical Computing).
Results
Respondents included 1000 US adults (weighted sample, 513.2 [51.3%] female and 486.8 [48.7%] male), ranging in age from 18 to 75 years or older, with racial and ethnic distributions representative of national composition (29.3 [2.9%] Asian or Asian American, 124.6 [12.5%] Black or African American, 105.1 [10.5%] Hispanic or Latino, 3.9 [0.4%] Middle Eastern, 18.2 [1.8%] Native American, 664.7 [66.5%] White, 29.0 [2.9%] multiracial, and 25.1 [2.5%] other), and political ideology distributed across very liberal (105.8 [10.6%]), liberal (164.0 [16.4%]), moderate (344.0 [34.4%]), conservative (205.9 [20.6%]), very conservative (98.7 [9.9%]), and not sure (81.5 [8.2%]). Additional demographic characteristics are provided in the Table. Missingness in survey responses was negligible, with just 2 respondents (self-described moderates) skipping a single survey item (term accessible health care in module 2).
Personal and Perceived American Values
Module 1 assessed whether population health concepts aligned with personal values and perceived core American values. Agreement for definitions of health equity or health equality increased progressively across the political spectrum (Figure 1), from very conservative (42.9% [95% CI, 29.2%-56.6%] for health equity, 28.5% [95% CI, 15.8%-41.1%] for health equality) to very liberal respondents (86.6% [95% CI, 77.9%-95.4%] for health equity, 79.0% [95% CI, 67.5%-90.6%] for health equality), indicating an association between political ideology and alignment with personal values (P < .001 for both definitions). Across all groups, a higher proportion of respondents endorsed alignment with health equity than with health equality. When respondents were asked whether these concepts reflected a core American value, however, the results were more mixed. Among liberal and very liberal respondents, endorsement of health equity and health equality as core American values was similar (liberal respondents: 63.7% [95% CI, 53.1%-74.3%] vs 67.0% [95% CI, 57.0%-77.0%]; very liberal respondents: 58.8% [95% CI, 46.2%-71.4%] vs 53.8% [95% CI, 39.6%-68.0%]). In contrast, among very conservative respondents, a higher proportion assigned to the health equity definition endorsed alignment compared with those assigned to the health equality definition (47.0% [95% CI, 33.1%-60.8%] vs 21.1% [95% CI, 9.6%-32.5%]). Agreement that health equity and health equality are core American values differed across political ideology (health equity, 63.7% [95% CI, 53.1%-74.3%] liberal vs 47.0% [95% CI, 33.1%-60.8%] very conservative; P = .01; health equality, 67.0% [95% CI, 57.0%-77.0%] liberal vs 21.1% [95% CI, 9.6%-32.5%] very conservative; P < .001). The largest divergence between personal values and perceived American values was observed among liberal and very liberal respondents. In these groups, endorsement of both terms was substantially higher for personal values than for perceived American values.
Line Graph Displaying Agreement With Health Equity or Health Equality Definition Across Ideological GroupsError bars indicate 95% CIs.
Evaluative Reactions to Common Terms
Reactions to health equity–related terms were first assessed on the original 7-point scale (range, −3 to +3). Kruskal-Wallis tests demonstrated significant differences in median reactions across political ideology for all terms except vulnerable populations. For interpretability, reactions were subsequently dichotomized as negative (<0) vs nonnegative (≥0).
Across ideology groups, negative reactions were uncommon for accessible health care, health care investment, population health, and community health, with fewer than 10% of respondents expressing negative reactions in most groups (Figure 2). Although overall responses were largely neutral or positive, very conservative respondents expressed higher negative reactions to population health (12.3% [95% CI, 5.8%-18.8%] vs 8.9% [95% CI, 5.0%-12.8%] for conservative respondents to 2.8% [95% CI, 0-5.9%] for very liberal respondents; P = .008) and community health (13.5% [95% CI, 6.7%-20.2%] vs 8.6% [95% CI, 4.8%-12.5%] for conservative respondents to 2.2% [95% CI, 0-5.0%] for very liberal respondents; P < .001).
Bar Graphs Showing Common Health Equity Terms With Broadly Nonnegative Reactions Across Ideological GroupsFour terms describing health equity were received favorably or neutrally: accessible health care, population health, health care investment, and community health. Most responses were nonnegative across ideological groups.
Six other terms elicited more mixed reactions across ideology (Figure 3), with clear ideological divisions observed for marginalized communities, inclusive health care, health disparities, and differences in health outcomes. For marginalized communities, negative reactions were highest among very conservative (56.2% [95% CI, 46.4%-65.9%]) and conservative respondents (57.9% [95% CI, 51.1%-64.6%]), compared with moderate (43.3% [95% CI, 38.0%-48.5%]), liberal (45.1% [95% CI, 37.5%-52.7%]), and very liberal respondents (45.1% [95% CI, 35.6%-54.6%]) (P = .006). For inclusive health care, negative reactions declined progressively across the political spectrum, from 32.7% (95% CI, 23.4%-42.0%) among very conservative respondents to 24.4% (95% CI, 18.6%-30.3%) among conservative, 11.7% (95% CI, 8.3%-15.0%) among moderate, 9.5% (95% CI, 5.0%-14.0%) among liberal, and 4.3% (95% CI, 0.4%-8.2%) among very liberal respondents (P < .001). In contrast, negative reactions to health disparities were more common among very liberal (59.8% [95% CI, 50.5%-69.2%]) and liberal respondents (57.2% [95% CI, 49.6%-64.7%]) than among moderate (42.0% [95% CI, 36.8%-47.2%]), conservative (43.5% [95% CI, 36.8%-50.3%]), and very conservative respondents (41.0% [95% CI, 31.3%-50.7%]) (P = .001). A similar pattern was observed for differences in health outcomes, with higher negative reactions among very liberal (39.2% [95% CI, 29.9%-48.5%]) and liberal respondents (41.6% [95% CI, 34.1%-49.2%]) compared with moderate (32.6% [95% CI, 27.6%-37.6%]), conservative (24.8% [95% CI, 18.9%-30.7%]), and very conservative respondents (30.7% [95% CI, 21.6%-39.8%]) (P = .008).
Bar Graph Showing Common Health Equity Terms With Mixed Reactions Across Ideological GroupsSix terms elicited a mix of negative and nonnegative reactions. Reactions differed significantly by ideology in 4 terms, with more conservative and very conservative respondents expressing negativity toward the terms marginalized communities and inclusive health care, and more liberal and very liberal respondents expressing negativity toward the terms health disparities and differences in health outcomes.
Framing Preferences for Public Health Statements
Across ideologies, respondents preferred collectivist (we) over individual (you) framing, action-oriented (start) over avoidance-oriented (stop) framing, affirmative (support) over oppositional (oppose) framing, and increase over decrease framing of semantically equivalent statements (Figure 4). The strongest consistent preferences across ideology groups were for support and increase framings: preference for support framing ranged from 74.0% (95% CI, 65.7%-82.4%) for very liberal respondents to 79.5% (95% CI, 73.3%-85.7%) for liberal respondents (P = .008), and preference for increase framing ranged from 72.7% (95% CI, 64.0%-81.5%) for very conservative respondents) to 82.1% (95% CI, 76.2%-88.0%) for liberal respondents (P = .33). These framings showed high endorsement across ideology groups with narrow ranges of preference compared with the other 2 framing contrasts.
Line Graph of Preferred Framings of Public Health Statements Across Ideological GroupsError bars indicate 95% CIs.
Political ideology differentiated strength of preference for collectivist and action-oriented framing. Preference for the we framing was highest among very liberal (83.3% [95% CI, 76.2%-90.4%]) and liberal respondents (81.4% [95% CI, 75.5%-87.4%]) compared with conservative (60.2% [95% CI, 53.5%-66.9%]) and very conservative respondents (47.3% [95% CI, 37.4%-57.1%]) ( P < .001). Similarly, preference for start framing differed by ideology, with stronger endorsement among liberal (83.1% [95% CI, 77.3%-88.8%]) and very liberal respondents (83.5% [95% CI, 76.4%-90.6%]) than among conservative (66.4% [95% CI, 60.0%-72.9%]) and very conservative respondents (65.8% [95% CI, 56.4%-75.1%]) (P < .001).
Discussion
Our study supports previous reports that have shown there are strong differences in language and framing preferences across political ideological groups when it comes to health communication.^10,26,27^ Using embedded randomized experiments, we specifically sought to test acceptability of definitions and their alignment with personal and perceived American values, evaluative reactions to common terms used in health equity work, and framing preference for public health messages in a three-module survey.
In module 1, respondents across ideological groups judged both health equity and health equality as consistent with their personal values. Values alignment was higher for the health equity definition than for the health equality definition. Perceived alignment between definitions and core American values varied across political ideology. Taken together, these findings suggest that despite differing political perspectives, there is a shared recognition of fairness and opportunity in health as guiding principles and that equity language resonates personally, even when audiences are uncertain that it represents a shared civic norm. An important finding was the divergence between personal beliefs and the respondent’s beliefs about core American values. Liberal and very liberal respondents demonstrated a sharp distinction between personal and core American values, while very conservative respondents reported closer alignment between personal and core American values. Even among conservative and very conservative groups, there was lower endorsement of either definition as a core American value, suggesting that across ideological groups, individuals perceive a gap between personal beliefs and perceptions of national norms. Prior work in political psychology has shown that misperceptions about where the broader public stands can amplify perceived polarization and increase the sense that policy issues are more ideologically divisive than they truly are.^28^ Recognizing and addressing this perceived misalignment may be a critical component of effective public health communication. Taken together, these results may help identify opportunities for bridging conversations through values-based language, presented clearly and with context, to facilitate resonance across ideological lines. For health communication across ideological identities, a pragmatic approach may be to lead with widely shared values, then subsequently link those values to concrete actions (ie, health care coverage, timely care, prevention) without partisan cues. These findings are supported by previous work showing that values-based policy framing increases support across political ideologies without backlash from other groups.^29,30^
In module 2, we looked at reactions toward commonly used terms in health equity discourse. We found that several terms elicited overwhelmingly positive responses (accessible health care and health care investment). Even when statistically significant ideological differences emerged—specifically, more negative reactions from very conservative respondents to population health and *community health—*more than 85% still viewed these terms positively or neutrally, suggesting that these terms remain largely unifying rather than polarizing. A second cluster of terms elicited more varied evaluative reactions across political ideologies, reflecting language that may be perceived as less neutral or more ideologically charged. For example, inclusive health care showed a clear ideological gradient, with only 4.3% of very liberal respondents reacting negatively compared with 32.7% of very conservative respondents. While most respondents across all groups still rated the term as neutral or positive, this divergence suggests that phrases invoking inclusion may carry political connotations for some audiences. Similarly, very conservative and conservative respondents had more negative reactions to the term marginalized communities. In contrast, liberal respondents provided unexpectedly greater negative ratings for terms such as health disparities and differences in health outcomes. This may reflect fatigue or skepticism in driving structural change or a reaction to the underlying issues themselves rather than the terminology. Although no terms were wholly rejected, some terms may not have the same resonance across people with differing political ideologies. In ideologically diverse settings, terms that elicit more variable reactions may benefit from contextual framing or coupling with shared values to reduce ambiguity and potential resistance. The terms that elicited consistently nonnegative reactions across ideology groups map onto policy domains that have historically attracted bipartisan support. Although our study did not evaluate policy preferences directly, prior evidence shows that population health initiatives such as Medicaid expansion have gained broad public legitimacy across states and party lines, and investments in core public health infrastructure receive support across political contexts.^31^ US global health programs—including US Agency for International Development and the President’s Emergency Plan for AIDS Relief—are further examples of health-directed investments that have maintained bipartisan backing over time.^32,33^ These domains may represent areas of shared interest where health system strengthening and community well-being align with public values across the public spectrum.
In module 3 of our study, we examined how subtle shifts in framing of public health messages affect respondent preferences across political ideologies. Although ideological gradients were observed, respondents across all groups largely favored collectivist language over individual-focused phrasing. Although community-oriented appeals are often perceived as less resonant with conservative audiences, our findings indicate that reactions were not uniform and showed meaningful variation within ideology groups.^34^
For the remaining paired statements, most respondents across all ideological groups preferred approach-oriented, positive framing. At least 65% of respondents in each ideological group favored statements using support, increase, and start framing over statements using oppose, decrease, and stop framing. These results reinforce evidence that affirmatively framed, approach-oriented messages elicit broader appeal than negative- or avoidance-based alternatives and highlight a pathway for building consensus around health equity communication across diverse audiences.^35,36,37^
Limitations
Our results must be interpreted considering several limitations. Although the YouGov methodology has been extensively validated and shown to produce samples that closely match US population benchmarks, recruitment from a nonprobability-based online panel may be subject to selection and coverage biases (eg, differential internet access), and the findings are to be interpreted as descriptive, particular for subgroup estimates. Despite matching and weighting to national benchmarks, respondents may differ from the broader US population in unmeasured ways. Self-reported ideology and evaluative reactions may also be imprecise, as respondents interpret ideological labels differently and may vary in how they react to terminology without additional context. Second, the surprising negative responses among liberal and very liberal respondents to certain health equity terms are difficult to interpret, as we did not distinguish whether these reflected disapproval of the terminology, frustration with the issues, or another source of negative reactions, nor did we test comprehension to ensure participants fully understood the contrasts. Finally, as with all survey research, expressed preferences may not translate to actual behaviors, where context, messenger identity, and repeated exposure shape communication effects.
Although this study focused on how language and framing shape receptiveness to health equity concepts in the wake of policy changes, it is important to acknowledge that health equity has long been embedded in political discourse. Advocates for equity have historically engaged in social and political movements aimed at addressing structural determinants of health, and public health institutions themselves are not ideologically neutral actors. Communication strategies alone cannot resolve deeper disagreements about the substantive goals of health equity, nor should they be substitutes for genuine engagement with communities whose values and policy preferences may differ from those held by many in the public health community. Recognizing these long-standing political dimensions provides necessary context for interpreting our findings and underscores that effective communication must be paired with responsiveness to diverse perspectives in a pluralistic society.
Conclusions
In this cross-sectional online survey study of 1000 US adults, ideological differences were observed in reactions to specific health equity terms, yet several commonly used terms and affirmative, collective framings were viewed favorably across groups. These findings may help public health professionals and advocates shape language that connects more deeply and inclusively with broad audiences, regardless of political orientation.^38^ As debates over health and equity increasingly intersect with political identity, these data provide actionable insights for clinicians, researchers, policymakers, and advocates. Strategic language and framing anchored in shared values and constructive framing offer a pathway to advance public health communication that is both principled and broadly resonant. Future efforts should embed more intentional language in public health messaging and policy debates, with testing and refinement in real-world contexts to build trust, engage diverse constituencies, and advance equity in health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Public health infrastructure in crisis: HHS workforce cuts, reorganizations, and funding reductions: impacts and solutions. Trust for America’s Health. Accessed December 18, 2025. https://www.tfah.org/report-details/funding-report-2025/
- 2Greer SL, Jarman H, Kulikoff R, Yaver M. Trump’s second presidency begins: evaluating effects on the US health system. Lancet Reg Health Am. 2025;48:101173. doi:10.1016/j.lana.2025.10117340678372 PMC 12270643 · doi ↗ · pubmed ↗
- 3Wang SX, Eniasivam A, Sterken D, ; the HOMERUN HEARS Work Group and the HOMERUN Collaborative. Navigating uncertainty: sustaining health equity in a shifting landscape. J Gen Intern Med. Published online November 17, 2025. doi:10.1007/s 11606-025-09874-z 41247421 PMC 13009315 · doi ↗ · pubmed ↗
- 4Eick SM, Eatman JA, Chandler M, Brooks NR. Reproductive and social policies, sociopolitical stress, and implications for maternal and child health equity. Curr Environ Health Rep. 2024;11(2):279-287. doi:10.1007/s 40572-024-00443-w 38639910 PMC 11531301 · doi ↗ · pubmed ↗
- 5Leider JP, Resnick B, Bishai D, Scutchfield FD. How much do we spend? creating historical estimates of public health expenditures in the United States at the federal, state, and local levels. Annu Rev Public Health. 2018;39:471-487. doi:10.1146/annurev-publhealth-040617-01345529346058 · doi ↗ · pubmed ↗
- 6Frieden TR. Dismantling public health infrastructure, endangering American lives. N Engl J Med. 2025;393(7):625-627. doi:10.1056/NEJ Mp 250908740737612 · doi ↗ · pubmed ↗
- 7Oberlander J. Progress lost—the unraveling of Medicaid and the Affordable Care Act. N Engl J Med. 2025;393(7):628-629. doi:10.1056/NEJ Mp 250976840737607 · doi ↗ · pubmed ↗
- 8Duggan CP, Bhutta ZA. “Putting America First”—undermining health for populations at home and abroad. N Engl J Med. 2025;392(18):1769-1771. doi:10.1056/NEJ Mp 250324340239090 · doi ↗ · pubmed ↗