Long‐Term Survival After Desperation Surgery for Primary Mediastinal Non‐Seminomatous Germ Cell Tumor With Rising Alpha‐Fetoprotein
Tomohiko Aigase, Takeshi Kishida, Hayato Kubo, Takahiro Matsumoto, Atsuto Suzuki, Kota Washimi, Yoichiro Okubo, Satoshi Hara, Hitoshi Sugiura, Noboru Nakaigawa

TL;DR
A rare aggressive tumor in the chest was successfully treated with surgery after chemotherapy failed, leading to long-term survival.
Contribution
This case demonstrates that desperation surgery can lead to long-term survival in PMNSGCT patients with elevated tumor markers.
Findings
Desperation surgery led to complete tumor resection and normalization of alpha-fetoprotein levels.
The patient remained recurrence-free after surgery despite elevated tumor markers before the operation.
Abstract
Primary mediastinal non‐seminomatous germ cell tumors (PMNSGCTs) are rare and aggressive neoplasms that carry a poor prognosis, especially following salvage chemotherapy. In cases of residual tumors with elevated tumor marker levels, desperation surgery may be considered. A 32‐year‐old man with PMNSGCT presented with a 100‐mm anterior mediastinal mass and elevated alpha‐fetoprotein (AFP; 17 000 ng/mL). After induction and salvage chemotherapy, AFP levels decreased to 20 ng/mL but did not normalize, and a 55‐mm cystic tumor persisted. Desperation surgery was performed despite an increase in AFP (40 ng/mL) before the operation. The tumor was completely resected, and histopathological examination revealed no viable tumor cells or teratomas. Postoperatively, AFP normalized, and the patient has remained recurrence‐free. This case highlights the potential role of desperation surgery in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
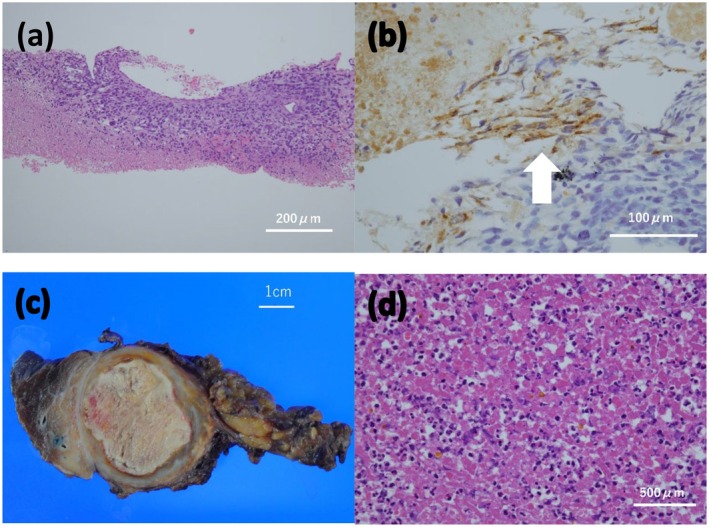 FIGURE 1
FIGURE 1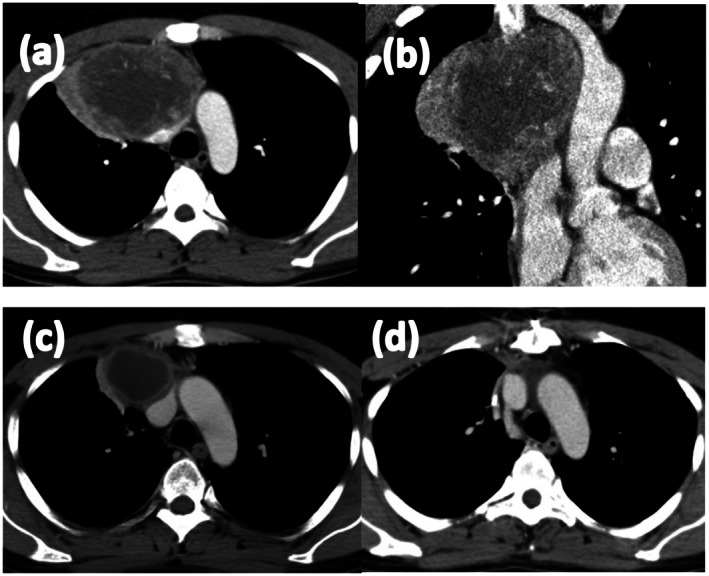 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Teratomas and Epidermoid Cysts · Myasthenia Gravis and Thymoma
Introduction
1
Primary mediastinal germ cell tumors (PMGCTs) are rare neoplasms [1]. According to the International Germ Cell Consensus Classification, mediastinal primary tumors are categorized as having a poor prognosis [2]. Even with standard treatment, the 5‐year overall survival rate is only 40%–50%, likely due to their intrinsic chemoresistance and aggressive histological features [3, 4].
The standard treatment for PMGCTs comprises platinum‐based combination chemotherapy, followed by surgical resection of residual masses once tumor markers normalize [2, 5].
Despite the suggestive presence of active residual cancer, surgical resection may be considered in cases where tumor markers remain elevated despite aggressive chemotherapy. Such a surgery is termed “desperation surgery.” [6] Its indications remain controversial, and are generally limited to select patients with resectable disease when no other effective options are available [7]. Although high‐level evidence is lacking, recent guidelines have proposed potential benefits in carefully selected cases [8, 9].
Herein, we report a rare case of a patient with a primary mediastinal non‐seminomatous germ cell tumor (PMNSGCT) who exhibited persistently abnormal and rising tumor marker levels after multiple courses of chemotherapy and achieved long‐term recurrence‐free survival following desperation surgery without further treatment.
Case Presentation
2
A 32‐year‐old man presented with a fever. Chest computed tomography (CT) at the referral hospital revealed an anterior mediastinal mass. CT‐guided biopsy indicated tumor cells with enlarged nuclei (Figure 1a). Immunohistochemically, the tumor was focally positive for alpha‐fetoprotein (AFP) (Figure 1b), glypican‐3, and c‐KIT. Considering these findings, a yolk sac tumor was strongly suspected. The patient was referred to our institution for further treatment. Laboratory evaluation revealed the following results: AFP, 17 000 ng/mL; AFP‐lectin 3 fraction > 99.6%; and human chorionic gonadotropin (HCG) < 1.0 IU/mL. No abnormalities were observed. Contrast‐enhanced CT revealed a 100‐mm solid mass in the anterior mediastinum with enhancement (Figure 2a,b), and no distant metastases were identified. Scrotal ultrasonography revealed no abnormality. Based on these findings, the patient was diagnosed with PMNSGCT, and systemic chemotherapy was initiated.
Histopathological findings. (a) Hematoxylin and eosin (H&E) staining of the CT‐guided biopsy specimen (original magnification ×100) showing proliferation of tumor cells with nuclear enlargement, suggestive of malignancy. (b) Immunohistochemical staining for alpha‐fetoprotein (AFP) using an anti‐AFP antibody (×400), demonstrating focal AFP positivity indicated by arrows. (c) Gross specimen of the resected mediastinal tumor, revealing a yellow‐white solid mass with internal necrosis. (d) H&E staining of the resected specimen (×400) showing no viable tumor cells.
Contrast‐enhanced computed tomography (CT) images of the anterior mediastinal tumor. (a) Axial view at initial diagnosis reveals a 100‐mm solid mass in the anterior mediastinum. (b) Coronal view of the same lesion confirms its extent with no evidence of distant metastasis. (c) Axial view just before surgery shows a residual 55‐mm cystic mass. (d) Axial view after surgery demonstrates complete resection with no evidence of residual tumor.
The treatment course is summarized in Figure 3. The patient received four cycles of bleomycin, etoposide, and cisplatin as first‐line chemotherapy. AFP subsequently decreased to 30 ng/mL but did not normalize. Imaging revealed a decreased residual mass with cystic changes. One cycle of etoposide and cisplatin was administered as additional therapy, but the AFP response was poor (23 ng/mL). Two cycles of salvage chemotherapy with paclitaxel, ifosfamide, and cisplatin (TIP) resulted in a modest decrease in the AFP levels to 20 ng/mL. CT revealed a 55‐mm residual tumor with cystic changes in the anterior mediastinum (Figure 2c). Brain magnetic resonance imaging was not performed at that time because the patient had no neurological symptoms, and no clinical findings suggested central nervous system involvement.
Timeline of chemotherapy administration and tumor marker kinetics. Changes in serum alpha‐fetoprotein (AFP) and AFP‐L3 fraction levels are plotted in relation to the timing of BEP, TIP, and EP chemotherapy regimens. BEP: Bleomycin, etoposide, and cisplatin; TIP: Paclitaxel, ifosfamide, and cisplatin; EP: Etoposide and cisplatin.
Given the persistently elevated tumor marker levels and residual tumor on imaging, surgery was planned. Although AFP increased up to 40 ng/mL just before the operation, the patient underwent surgical resection 1 month after the final TIP course. The tumor was completely resected, and histopathological examination revealed no residual tumor or teratoma elements (Figure 1c,d). The AFP level normalized to 4 ng/mL postoperatively, and CT confirmed complete resection (Figure 2d). The patient is being followed up with serial AFP measurements and imaging and remains recurrence‐free without additional treatment for 7 years postoperatively.
Discussion
3
Previous studies have reported poor survival rates in patients with mediastinal tumors undergoing salvage chemotherapy [1]. Compared to retroperitoneal germ cell tumors, PMNSGCT respond poorly to salvage regimens, and no specific regimen has demonstrated superior outcomes [10, 11, 12].
In patients with PMNSGCT, elevated serum marker levels after chemotherapy do not always correlate with residual viable disease. Approximately 30%–40% of patients undergoing desperation surgery have no residual cancer, with pathology demonstrating only teratoma or necrotic tissue [13]. This discordance may be explained by the leakage of AFP or HCG from the accumulated fluid of the cystic components rather than actual tumor activity [14, 15]. Although leakage of AFP into the cystic fluid likely contributed to the persistent serum AFP elevation in this case, AFP levels in the cystic fluid were not measured, which is a limitation of this report.
In the present case, AFP levels reached a plateau following TIP salvage chemotherapy, indicating a limited likelihood of further response to additional systemic therapy. According to the National Comprehensive Cancer Network (NCCN) and European Association of Urology guidelines, surgical resection should be considered when serum tumor markers plateau and the residual mass is surgically resectable [8, 9]. Imaging findings in our case also demonstrated a cystic component, raising the possibility of AFP accumulation rather than a viable tumor. Furthermore, third‐line chemotherapy, including irinotecan‐based regimens, provides limited benefit in PMNSGCT and is generally regarded as palliative rather than curative. These considerations supported the decision to proceed with desperation surgery.
Based on these factors some reports recommend surgical resection of resectable mediastinal masses regardless of post‐chemotherapy tumor marker levels [13, 16, 17]. Although desperation surgery in PMNSGCT generally shows poor outcomes, with reported 5‐year survival rates of 25%–35% and median overall survival of 9.7–11.5 months [13, 18], long‐term survival is achieved in some cases. Furthermore, patients with elevated AFP at the time of residual tumor resection reportedly have more favorable outcomes than those with elevated HCG. Ong et al. reported significantly better survival among patients with AFP elevation compared with HCG elevation in the setting of post‐chemotherapy mediastinal germ cell tumors [19]. This prognostic distinction may help contextualize the favorable long‐term course observed in the present case despite persistent AFP elevation. Reported favorable prognostic factors include localization of the disease to the mediastinum, achievement of complete resection, normalization of tumor markers postoperatively, and the absence of viable tumor on pathological examination [16, 18, 20]; the present case fulfilled these criteria. In contrast to these favorable prognostic factors, the NCCN guidelines recommend proceeding with desperation surgery only when tumor markers are mildly elevated and trending downward. For patients with persistently elevated markers, as in our case, further chemotherapy is generally advised.
This case is unique in that the decision to proceed with surgery was made despite rising AFP levels after salvage chemotherapy—an indication in which further systemic therapy is typically recommended. The combination of plateauing AFP levels and a predominantly cystic residual mass suggested limited viable tumor, allowing multidisciplinary judgment to favor resection. This case therefore demonstrates that carefully selected patients may still achieve excellent long‐term outcomes and help avoid unnecessary administration of salvage chemotherapy with timely desperation surgery, even in the presence of increasing tumor markers.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. Rosti , S. Secondino , A. Necchi , G. Fornarini , and P. Pedrazzoli , “Primary Mediastinal Germ Cell Tumors,” Seminars in Oncology 46 (2019): 107–111.31076171 10.1053/j.seminoncol.2019.04.001 · doi ↗ · pubmed ↗
- 2International Germ Cell Cancer Collaborative Group , “International Germ Cell Consensus Classification: A Prognostic Factor‐Based Staging System for Metastatic Germ Cell Cancers,” Journal of Clinical Oncology 15 (1997): 594–603.9053482 10.1200/JCO.1997.15.2.594 · doi ↗ · pubmed ↗
- 3C. Albany and L. H. Einhorn , “Extragonadal Germ Cell Tumors: Clinical Presentation and Management,” Current Opinion in Oncology 25 (2013): 261–265.23422328 10.1097/CCO.0b 013e 32835 f 085d · doi ↗ · pubmed ↗
- 4C. Rivera , A. Arame , J. Jougon , et al., “Prognostic Factors in Patients With Primary Mediastinal Germ Cell Tumors, a Surgical Multicenter Retrospective Study,” Interactive Cardiovascular and Thoracic Surgery 11 (2010): 585–589.20709694 10.1510/icvts.2010.238717 · doi ↗ · pubmed ↗
- 5D. F. Bajorin , H. Herr , R. J. Motzer , and G. J. Bosl , “Current Perspectives on the Role of Adjunctive Surgery in Combined Modality Treatment for Patients With Germ Cell Tumors,” Seminars in Oncology 19 (1992): 148–158.1372757 · pubmed ↗
- 6D. P. Wood, Jr. , H. W. Herr , R. J. Motzer , et al., “Surgical Resection of Solitary Metastases After Chemotherapy in Patients With Nonseminomatous Germ Cell Tumors and Elevated Serum Tumor Markers,” Cancer 70 (1992): 2354–2357.1382832 10.1002/1097-0142(19921101)70:9<2354::aid-cncr 2820700924>3.0.co;2-u · doi ↗ · pubmed ↗
- 7T. Habuchi , T. Kamoto , I. Hara , et al., “Factors That Influence the Results of Salvage Surgery in Patients With Chemorefractory Germ Cell Carcinomas With Elevated Tumor Markers,” Cancer 98 (2003): 1635–1642.14534879 10.1002/cncr.11711 · doi ↗ · pubmed ↗
- 8National Comprehensive Cancer Network , “NCCN Clinical Practice Guidelines in Oncology: Testicular Cancer,” (2025), Version 2.2025.10.6004/jnccn.2009.004719555582 · doi ↗ · pubmed ↗