Transnasal–Transoral Endoscopic Surgery Followed by Radiotherapy for Nasopharyngeal Spindle Cell Carcinoma
Yuji Kanazawa, Yoshiharu Kitani, Aya Matsubara, Riki Goda, Makoto Suzuki

TL;DR
A rare case of nasopharyngeal spindle cell carcinoma was treated with a minimally invasive endoscopic surgery followed by radiotherapy, achieving long-term disease-free survival.
Contribution
Presents a novel transnasal-transoral endoscopic approach for treating nasopharyngeal SpCC in high-risk patients.
Findings
The transnasal-transoral approach enabled precise tumor resection with minimal surgical invasiveness.
Postoperative radiotherapy effectively managed positive surgical margins and achieved disease-free survival for over 3 years.
The approach preserved renal function and reduced surgical morbidity in a patient with significant comorbidities.
Abstract
Spindle cell carcinoma (SpCC) is a rare and aggressive variant of squamous cell carcinoma characterized by the coexistence of epithelial and mesenchymal components, accounting for <1% of all head and neck malignancies. Nasopharyngeal SpCC is extremely rare, and its optimal management remains unclear, particularly in patients who cannot tolerate extensive surgery. An 80-year-old man presenting with right-sided ear fullness was diagnosed with nasopharyngeal SpCC (T1N0M0). Imaging revealed a submucosal tumor on the posterior wall of the nasopharynx that was in contact with the right Eustachian tube. The patient also had severe chronic kidney disease; therefore, conventional open approaches requiring prolonged operative time and significant surgical stress were considered unsuitable. Therefore, a combined transnasal-transoral endoscopic approach was selected to achieve maximal tumor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
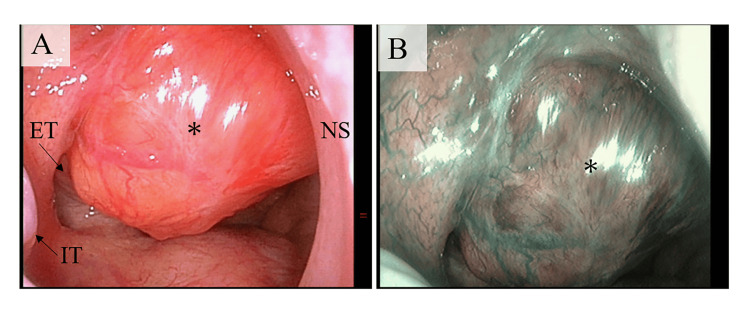 Figure 1
Figure 1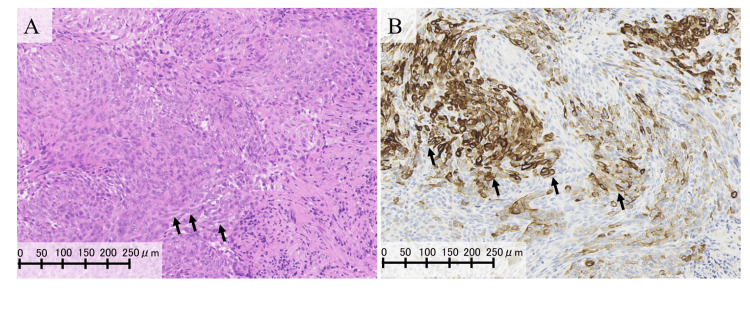 Figure 2
Figure 2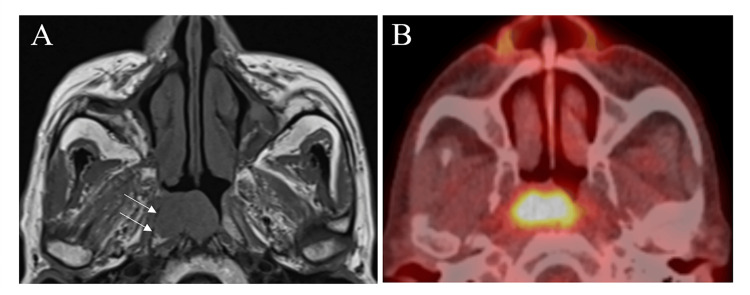 Figure 3
Figure 3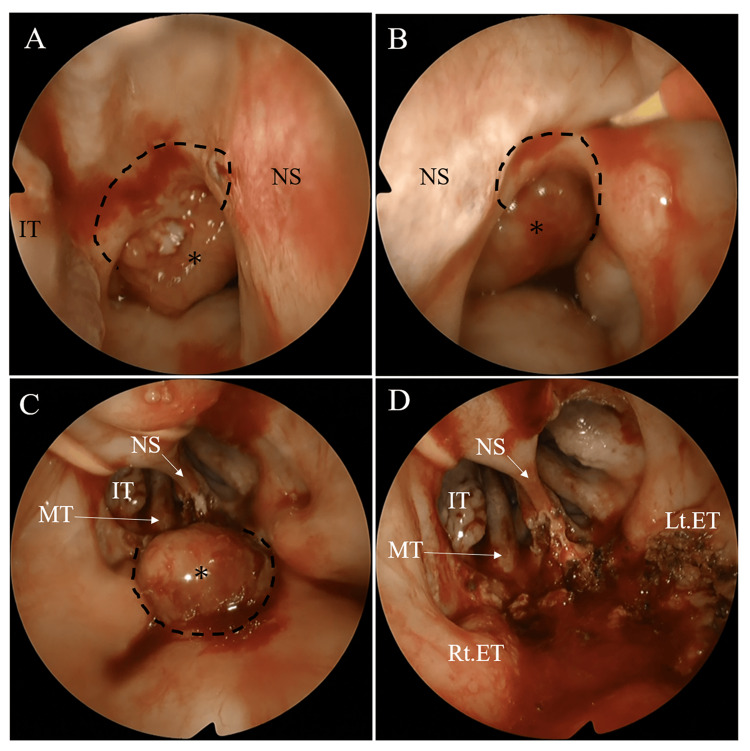 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Head and Neck Cancer Studies · Salivary Gland Tumors Diagnosis and Treatment
Introduction
Spindle cell carcinoma (SpCC) is a rare neoplasm characterized by the concurrent presence of mesenchymally differentiated spindle-shaped cells and squamous cell carcinoma (SCC) components. This carcinoma accounts for <1% of all head and neck cancers, with the larynx being the most frequently affected site [1,2]. Compared with SCC, SpCC is considered a more aggressive malignancy and poses unique therapeutic challenges, including lower radiosensitivity and a higher rate of local recurrence [2]. Consequently, a higher proportion of patients with SpCC are treated surgically rather than with radiotherapy, in contrast to patients with head and neck SCC. However, due to the rarity of nasopharyngeal SpCC and the limited number of reported cases, standardized treatment protocols have not been established, and optimal management remains unclear, particularly in patients who cannot tolerate extensive surgery because of comorbidities.
Herein, we report the case of an 80-year-old man with nasopharyngeal SpCC. Surgical access to the nasopharynx is technically challenging and highly invasive when using conventional open approaches such as the maxillary swing, midfacial degloving, and transmaxillary or infratemporal fossa approaches. Owing to the patient’s poor tolerance for prolonged surgery due to severe renal impairment, palliative tumor resection was performed using a transnasal-transoral endoscopic approach. Postoperative radiotherapy was subsequently administered because of a positive surgical margin. As a result of this combined treatment, the patient has remained disease-free for three years following surgery. Although the final margin status was positive, the transnasal-transoral endoscopic approach provided an adequate surgical field, and adjuvant radiotherapy proved effective in achieving local disease control.
Case presentation
An 80-year-old man presented to our clinic with a one-week history of right-sided ear fullness. He was undergoing treatment for membranous nephropathy with an estimated glomerular filtration rate (eGFR) of 16 mL/min, corresponding to stage 4 chronic kidney disease (eGFR 15-29 mL/min/1.73 m²) [3]. Otoscopic and nasopharyngeal examinations revealed right-sided serous otitis media and a submucosal mass on the posterior wall of the nasopharynx (Figure 1).
Endoscopic findings at the initial examination.(A) Endoscopic view via the right nasal cavity showed a submucosal tumor overlying the right Eustachian tube on the posterior wall of the nasopharynx (). (B) Narrow-band imaging demonstrated no abnormal mucosal findings on the tumor surface, such as the absence of irregular microvascular patterns. ET: Eustachian tube; IT: inferior turbinate; NS: nasal septum.*
Histopathological analysis of the biopsy specimen revealed squamous cell carcinoma with cytokeratin-positive spindle-shaped cells (Figure 2).
Histopathological and immunohistochemical findings of the tumor.(A) Microscopically, short spindle-shaped to spindle-shaped tumor cells were observed. Arrows indicate representative examples of spindle-shaped tumor cells. (B) Immunohistochemically, the tumor cells were partially positive for cytokeratin. Arrows indicate representative examples of cytokeratin-positive tumor cells.
Magnetic resonance imaging (MRI) showed a 25-mm tumor on the posterior wall of the nasopharynx that was in contact with the right Eustachian tube cartilage (Figure 3A). A gadolinium contrast agent was not administered because of the patient’s renal dysfunction. Positron emission tomography-computed tomography (PET-CT) demonstrated fluorodeoxyglucose (FDG) uptake in the nasopharynx without evidence of regional or distant metastasis (Figure 3B).
Imaging studies at the initial examination.(A) T1-weighted MRI showed the tumor was in contact with the right Eustachian tube (arrow). (B) PET-CT showed FDG uptake with a maximum standardized uptake value (SUVmax) of 9.8 in the tumor.
Based on these findings, the tumor was diagnosed as nasopharyngeal SpCC (T1N0M0). Given the limited efficacy of radiotherapy alone against the mesenchymal component of SpCC, surgical resection was planned using a transnasal endoscopic approach combined with a transoral approach as the tumor extended toward the oropharyngeal side. A transpterygoid approach is also considered if infiltration into the right Eustachian tube is identified during surgery [4,5]. However, because the patient’s severe chronic kidney disease limited his tolerance to prolonged surgery and large fluid shifts, maximal cytoreductive endoscopic resection was planned to reduce the tumor burden while minimizing surgical invasiveness, followed by postoperative radiotherapy. During surgery, a submucosal resection of the inferior turbinate was performed to make the surgical instruments easier to handle. The tumor was initially dissected anteriorly, cranially, and laterally from the distally located superior pharyngeal constrictor muscles (Figures 4A, 4B). Subsequently, posterior, caudal, and lateral dissections were performed using a 70-degree endoscope via the oropharynx (Figure 4C). This approach confirmed that the right Eustachian tube remained intact (Figure 4D), and intraoperative frozen section analysis demonstrated no malignant involvement of the Eustachian tube mucosa. The operative time was 121 min, the intraoperative infusion volume was 900 mL, the urine output was 300 mL, and the estimated blood loss was 150 mL.
Intraoperative findings of transnasal–transoral approach.(A) Transnasal view via the right nasal cavity. The curved incision (dotted lines) was made around the tumor (), from the posterior end of the nasal septum (NS) to the medial aspect of the inferior turbinate. (B) Transnasal view via the left nasal cavity. An incision (dotted lines) was made around the tumor () in the same manner on the right side. (C) Transoral view using a 70-degree endoscope. The curved incision (dotted lines) was made around the tumor () at the posterior wall of the nasopharynx. (D) Transoral view after resecting the tumor. On visual inspection, the Eustachian tube appeared intact. ET: Eustachian tube; IT: inferior turbinate; MT: middle turbinate; NS: nasal septum, Lt: left; Rt: right.*
Postoperatively, no intravenous fluids were administered, oral intake of water was resumed 3 hours after surgery, and the patient was discharged on postoperative day three. The final histopathological examination confirmed SpCC with a positive surgical margin on the posterior wall of the nasopharynx and a negative margin on the right side of the Eustachian tube. Thirty days after the surgery, localized intensity-modulated radiotherapy was administered to the nasopharynx, delivering a total dose of 65 Gy in 26 fractions. The clinical target volume included the postoperative tumor bed and area of the positive margin, with appropriate sparing of adjacent critical structures. The patient remained recurrence-free for >3 years after surgery (Figure 5).
Endoscopic and radiologic findings three years after postoperative radiotherapy.(A) Endoscopic examination revealed no evidence of local recurrence. (B) PET–CT showed no evidence of recurrence.
Perioperative renal function remained stable (eGFR 15-18 mL/min). Although renal function gradually declined postoperatively, reaching an eGFR of 10 mL/min at 30 months and necessitating dialysis initiation, no acute deterioration in renal function was observed during radiotherapy.
Discussion
In this case, postoperative radiotherapy administered for a positive surgical margin contributed to long-term disease-free survival, suggesting that adjuvant radiotherapy may play an important role in the management of SpCC with positive margins. The combined transnasal-transoral endoscopic approach provided an adequate surgical view, allowing maximal tumor resection with minimal invasiveness. Although the clinical benefit of surgery resulting in positive margins remains unclear, a strategy combining maximal cytoreductive resection and postoperative radiotherapy may be a viable treatment option for nasopharyngeal SpCCs in patients who cannot tolerate more invasive procedures. Further studies are required to establish optimal treatment strategies for patients with nasopharyngeal SpCC.
Advances in endoscopic techniques have improved surgical visualization and expanded the operative field, thereby facilitating minimally invasive tumor resection for nasopharyngeal malignancies. Two primary endoscopic approaches have been described for the treatment of localized early-stage nasopharyngeal carcinoma: transnasal and transoral approaches. The transnasal approach provides limited access to lesions extending inferiorly beyond the soft palate into the oropharynx, whereas the transoral approach provides access to the nasopharyngeal region below the soft palate, thereby overcoming this limitation [6]. In this case, the combined transnasal-transoral approach enabled sufficient visualization for tumor resection. Retrospective pathological evaluation revealed a negative surgical margin in the right Eustachian tube, indicating that complete resection may have been achieved. From this perspective, postoperative radiotherapy may not have been strictly necessary; however, it was administered to ensure local disease control.
This case highlights the potential therapeutic role of radiotherapy for SpCC. A previous cohort study suggested that combined surgery and radiotherapy provided better survival outcomes than surgery alone for patients with head and neck SpCC [1]. A previous case series reported long-term disease-free survival exceeding 3 years in patients with positive surgical margins who underwent postoperative radiotherapy or chemoradiotherapy for head and neck SpCC [7,8]. In these reports, none of the patients had regional or distant metastases, including cases of early-stage palatine tonsil and maxillary cancers as well as advanced ethmoid sinus cancer, suggesting that radiotherapy may be effective even in locally advanced SpCC. Conversely, the effectiveness of radiotherapy for SpCC has been inconsistent across observational studies. For early-stage laryngeal SpCC, favorable outcomes with low recurrence rates have been reported in patients treated with radiotherapy alone [9], whereas another study demonstrated better survival outcomes in patients treated with surgery alone than in those who underwent surgery followed by adjuvant radiotherapy [10]. However, the latter study acknowledged that radiotherapy was preferentially administered in more advanced cases, limiting definitive conclusions regarding its efficacy. Although SpCC has traditionally been considered relatively radioresistant, there is currently no conclusive evidence demonstrating the lack of benefit of radiotherapy for this disease.
In this case, maximal cytoreductive surgery was performed, followed by postoperative radiotherapy. The therapeutic rationale for cytoreductive surgery is supported by evidence from other solid tumors, in which tumor debulking enhances the effectiveness of adjuvant therapies. In advanced ovarian carcinoma, many patients present with extensive tumor dissemination throughout the abdomen and pelvis, making complete surgical resection challenging. In particular, when the disease involves the upper abdomen, achieving complete resection is generally difficult. Consequently, cytoreductive surgery followed by chemotherapy has become the standard treatment strategy and has been shown to confer significant survival benefits [11]. This benefit is attributed to a reduction in tumor burden, which decreases the number of treatment-resistant cells and limits the emergence of resistant phenotypes [12]. However, evidence supporting the effectiveness of cytoreductive surgery for SpCC remains limited, and it is possible that radiotherapy alone may have been sufficient in this case. Ideally, complete resection should be performed whenever feasible rather than cytoreductive surgery.
CKD is a major public health concern characterized by the progressive deterioration of renal function, with severity classified from stages 1 to 5 [3]. Patients with stage 4 CKD are at an increased risk of further renal impairment and cardiovascular complications due to surgical stress, anesthesia, and perioperative fluid and electrolyte fluctuations [3]. Although no definitive criteria exist regarding the acceptable operative duration or blood loss in such patients, minimizing surgical invasiveness and anesthesia exposure is essential. In the present case, perioperative management was successful, and the patient’s renal function remained stable during the perioperative period.
Conclusions
This study demonstrates that a treatment strategy combining maximal cytoreductive endoscopic surgery with subsequent radiotherapy may be a feasible option for nasopharyngeal SpCC. This approach may be particularly beneficial for patients with significant comorbidities, such as advanced CKD, who are unable to tolerate extensive surgery. Larger studies and multicenter case series are needed to better define optimal management strategies, evaluate long-term outcomes, and clarify the respective roles of surgery and radiotherapy in nasopharyngeal SpCC. Future research should also focus on elucidating the biological behavior of nasopharyngeal SpCC and identifying prognostic factors to guide personalized treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prognostic significance of head and neck spindle cell carcinoma Head Neck Patel AM Choudhry HS Desai AD 6856964520233658417110.1002/hed.27285 · doi ↗ · pubmed ↗
- 2Laryngeal spindle cell carcinoma: a population-based analysis of incidence and survival Laryngoscope Dubal PM Marchiano E Kam D 2709271412520152599452010.1002/lary.25383 · doi ↗ · pubmed ↗
- 3Patient with chronic renal failure undergoing surgery Curr Opin Anaesthesiol Meersch M Schmidt C Zarbock A 4134202920162694530810.1097/ACO.0000000000000329 · doi ↗ · pubmed ↗
- 4Endoscopic endonasal transpterygoid nasopharyngectomy: Anatomical considerations and technical note Head Neck Liu J Zhao J Wang Y 3063204620243798723810.1002/hed.27581 · doi ↗ · pubmed ↗
- 5Endoscopic endonasal transpterygoid nasopharyngectomy Laryngoscope Al-Sheibani S Zanation AM Carrau RL 2081208912120112189844710.1002/lary.22165 · doi ↗ · pubmed ↗
- 6The combined endonasal and transoral approach for the management of skull base and nasopharyngeal pathology: a case series Neurosurg Focus Sreenath SB Rawal RB Zanation AM 037201410.3171/2014.7.FOCUS 1435325270139 · doi ↗ · pubmed ↗
- 7Spindle cell carcinoma of the oral cavity and oropharynx: factors affecting outcome J Chin Med Assoc Su H-H Chu S-T Hou Y-Y 4784836920061709867210.1016/S 1726-4901(09)70312-0 · doi ↗ · pubmed ↗
- 8Spindle cell carcinoma of the head and neck region: treatment and outcomes of 15 patients Ecancermedicalscience Iqbal MS Paleri V Brown J 594920152663589810.3332/ecancer.2015.594PMC 4659701 · doi ↗ · pubmed ↗