The Characteristic “Tunnel Sign” on MRI as a Diagnostic Marker of Tunneling Abscesses in Listeria Rhombencephalitis in a Patient With Multiple Myeloma: A Case Report
Madhushan Ranabahu, Nipuna Weerasinghe, Janya Jayawardena, Kishan Dissanayake, Janaka Peiris

TL;DR
A rare brain infection caused by Listeria was diagnosed using an MRI 'tunnel sign' in a cancer patient, leading to successful treatment.
Contribution
The case highlights the 'tunnel sign' as a novel MRI marker for diagnosing Listeria rhombencephalitis without microbiological confirmation.
Findings
MRI showed a 'tunnel sign' indicative of tunneling abscesses in Listeria rhombencephalitis.
Prompt antibiotic treatment led to significant neurological recovery in the patient.
Diagnosis was made solely based on radiological features in the absence of microbiological evidence.
Abstract
Neurolisteriosis is a rare but potentially serious CNS infection. Diagnosis can be established through bacteriological studies or by identifying characteristic tunneling abscesses in the CNS. Delayed initiation of appropriate antibiotic therapy may result in permanent structural brain damage, disability, or death. We report the case of a 65-year-old woman with multiple myeloma undergoing chemotherapy who presented with an acute febrile illness accompanied by drowsiness, slurred speech, difficulty swallowing, neck stiffness, and complex ophthalmoplegia. MRI of the brain demonstrated characteristic findings of the “tunnel sign,” suggestive of a tunneling abscess in Listeria rhombencephalitis. The diagnosis was made based on radiological features alone, in the absence of microbiological confirmation. With prompt initiation of IV ampicillin, she demonstrated marked neurological recovery,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
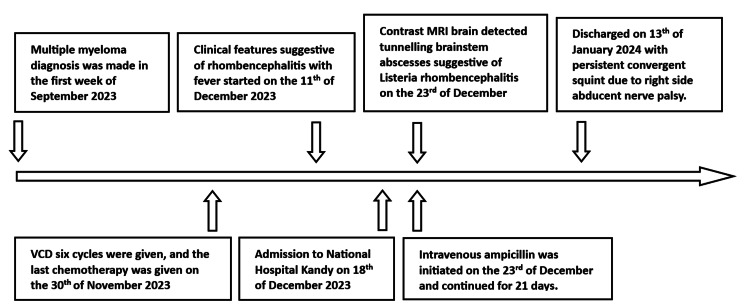 Figure 1
Figure 1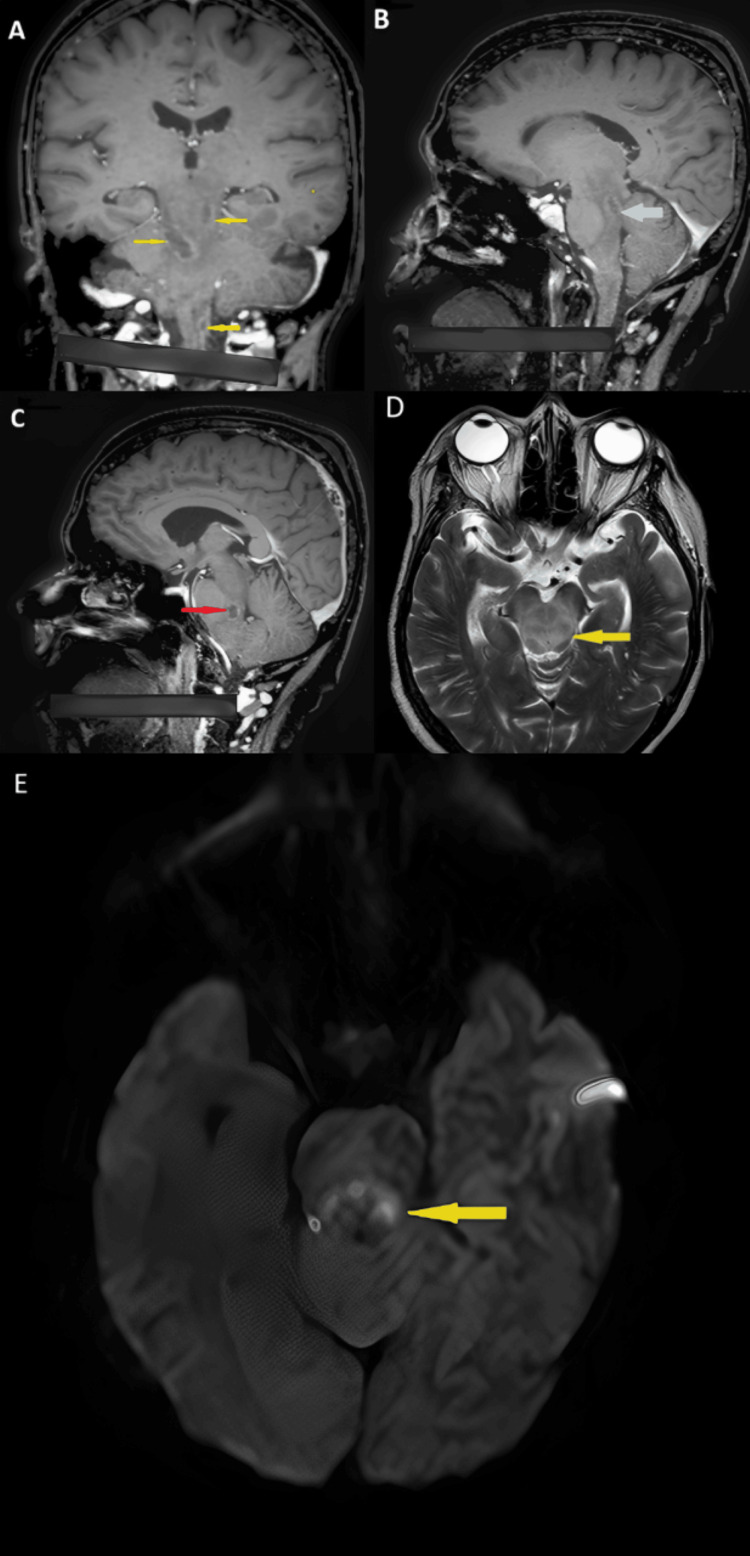 Figure 2
Figure 2| Parameter | Result | Reference range |
| White blood count | 10.09 (neutrophils 76%) | 4-10 × 10³/µL |
| Hemoglobin | 11.7 | 12-15 g/dL |
| Platelets | 245 | 150-450 × 10³/µL |
| Corrected calcium | 2.02 | 2.15-2.65 mmol/L |
| Serum creatinine | 63 | 60-120 µmol/L |
| Sodium | 134 | 135-148 mmol/L |
| Aspartate transaminase | 17 | 10-35 U/L |
| Alanine transaminase | 13 | 10-40 U/L |
| Serum albumin | 37 | 35-52 g/L |
| Serum globulin | 26 | 25-35 g/L |
| C-reactive protein | 32 | 0.5-5.0 mg/dL |
| Erythrocyte sedimentation rate | 50 | <30 mm/h |
| Blood culture | Negative | - |
| Mantoux test | Negative | - |
| HIV screening | Negative | - |
| IHA for melioidosis | Negative | - |
| CSF cryptococcal antigen | Negative | - |
| CSF TB culture | Negative | - |
| CSF TB PCR | Negative | - |
| CSF pyogenic culture | Negative (up to 48 hours incubation) | - |
| CSF VDRL | Nonreactive | - |
| CSF color | Clear | - |
| CSF protein | 112 | 15-45 mg/dL |
| CSF sugar | 43 mg/dL | >2/3 of blood glucose |
| Serum blood sugar | 120 | 72-200 mg/dL |
| CSF cells | WBC 250/mm³ (lymphocytes 83%) | <5 lymphocytes/mm³ |
| CSF microscopy | Negative | - |
| Author | Patient characteristics | Abscess location |
|
|
Sakarunchai et al. (2016) [ | 36-year-old female on prednisolone for systemic lupus erythematosus | Left frontal lobe | Blood |
|
Slezák et al. (2020) [ | 41-year-old immunocompetent | Cervical spine, brainstem | CSF |
| 50-year-old man on prednisolone for autoimmune hemolytic anemia | Right parietal lobe | Blood | |
| 67-year-old man with multiple myeloma on chemotherapy | Right frontal lobe | Abscess biopsy tissue | |
|
Zhang et al. (2021) [ | 64-year-old female with type 2 diabetes mellitus | Left frontal and parietal lobes | Blood |
|
Simonsen et al. (2021) [ | 39-year-old female with metastatic lung cancer on chemotherapy | Right frontal lobe and basal ganglia | Blood |
|
Bristowe et al. (2024) [ | 82-year-old man with type 2 diabetes mellitus and monoclonal gammopathy of undetermined significance | Right frontal lobe | Blood |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Antifungal resistance and susceptibility · Ocular Infections and Treatments
Introduction
Listeria monocytogenes is a gram-positive intracellular bacillus transmitted to humans through food contamination. Listeriosis is a foodborne infection caused by the consumption of unheated, processed, refrigerated, or canned meat and fish products, as well as unpasteurized dairy products [1,2]. *Listeria *is a neurotropic bacterium that primarily affects the CNS, causing neurolisteriosis. Neurolisteriosis is common in neonates, pregnant women, the elderly, and immunocompromised patients [3]. CNS involvement in neurolisteriosis can manifest as meningitis, encephalitis, and, rarely, abscess formation [4]. In immunocompromised patients, neurolisteriosis has a high case-fatality rate of approximately 30% [5]. Diagnosis can be established by isolating the bacteria from CSF using Gram staining, culture, or PCR. CNS imaging is also essential, as contrast-enhanced MRI can reveal characteristic tunneling abscesses in 1-10% of patients [3,6].
Case presentation
A 65-year-old female tailor was diagnosed with multiple myeloma during the first week of September 2023. She received six cycles of VCD (bortezomib, cyclophosphamide, and dexamethasone) for treatment. Her last chemotherapy session was on November 30, 2023. Following this, she experienced generalized ill health for 10 days. Subsequently, over seven days, she developed fever, headache, nausea, vomiting, loss of appetite, diplopia, reduced vision, slurred speech, and difficulty swallowing (Figure 1).
Timeline illustrating the chronological progression of the patient’s illness
She was admitted to National Hospital Kandy on December 18, 2023. Physical examination revealed an ill-appearing patient with a temperature of 38.8°C, a blood pressure of 130/80 mmHg, a regular pulse of 86 beats per minute, and a respiratory rate of 18 breaths per minute. Precordial, lung, and abdominal examinations were normal. Detailed neurological examination showed a Glasgow Coma Scale score of 13/15 (eye 3, verbal 4, motor 6), neck stiffness, right eye deviation medially with complex ophthalmoplegia, and pupillary size of 3 mm bilaterally with sluggish direct and consensual light reflexes. Motor power was 3/5 in all limbs with normal reflexes, and plantar responses were downgoing bilaterally.
An initial clinical diagnosis of meningoencephalitis was made in this elderly patient with multiple myeloma undergoing chemotherapy. Empirical IV ceftriaxone 2 g every 12 hours was initiated after obtaining a peripheral blood culture on December 18. A diagnostic lumbar puncture was performed on December 20, 2023. CSF analysis revealed lymphocytic pleocytosis with low glucose (Table 1).
MRI of the brain with contrast was performed on December 23, 2023, and demonstrated characteristic findings of brainstem abscesses with the “tunnel sign,” consistent with *Listeria *rhombencephalitis (Figure 2A-2E).
(A) Coronal T1 MR image with contrast of the patient’s brain. Yellow arrows indicate multiple lesions in the midbrain, pons, and upper cervical spinal cord. These lesions demonstrate peripheral ring enhancement with central non-enhancement, typical of tunneling abscesses. Right side is indicated. (B) Sagittal T1 MR image with contrast. Light blue arrow shows a lesion in the upper pontine tegmentum with peripheral ring enhancement and central non-enhancement. (C) Sagittal T1 MR image with contrast. Red arrow shows a lesion in the lower pontine tegmentum with central low intensity and peripheral ring enhancement. (D) Axial T2 MR image. Green arrow indicates midbrain hyperintensity consistent with edema. (E) Axial diffusion-weighted MR image. Yellow arrow demonstrates diffusion restriction within small ring-enhancing lesions, consistent with microabscesses.
IV ampicillin 2 g was administered every four hours starting on December 23, 2023, and continued for 21 days. Ceftriaxone was discontinued after 10 days. All neurological deficits improved following the ampicillin course, except for a persistent convergent squint due to right lateral rectus weakness from right-sided abducent nerve palsy. The patient was discharged from the hospital on January 13, 2024, with the convergent squint remaining.
Discussion
The patient was a late middle-aged female with recently diagnosed multiple myeloma undergoing chemotherapy. Multiple myeloma causes immunoparesis due to an excess of uninvolved immunoglobulins and suppression of normal immunoglobulin production. In addition, the patient received six cycles of VCD chemotherapy for multiple myeloma, which further aggravated her immunocompromised status [7].
*L. monocytogenes *spreads into the CNS via either hematogenous dissemination from the gastrointestinal tract or retrograde axonal transport. Interestingly, retrograde axonal spread typically occurs along the trigeminal nerve to the brainstem [4,6]. When L. monocytogenes enters the brain white matter, it spreads along axons, causing tunneling abscesses along the pathways of spread. CNS tunneling abscess formation is characteristic of neurolisteriosis [2,6]. However, tunneling abscesses in the CNS can also occur in neuromelioidosis and Spirometra mansoni infestation. Neurolisteriosis-associated brain tunneling abscess formation is rare [2,6].
Our patient developed an acute febrile illness with progressive neurological deficits over seven days. Typical clinical features of infective rhombencephalitis include fever, headache, neck stiffness, confusion, and cranial nerve palsies, all of which were observed in this case [1].
CSF analysis showed lymphocytic pleocytosis with elevated protein and a low CSF glucose level of 35.8% relative to blood glucose (Table 1). In the literature, CSF analysis in neurolisteriosis typically shows a predominant polymorphonuclear pleocytosis, with CSF glucose below 40 mg/dL in 39% of patients. CSF protein can be elevated to 100-200 mg/dL [8]. However, CSF pleocytosis and glucose levels in neurolisteriosis vary depending on the timing of lumbar puncture, prior antibiotic use, and the patient’s immune status. CSF Gram stain and culture are considered the gold standard for diagnosing listeriosis. In this patient, blood and CSF Gram stains and cultures were negative, possibly due to prior antibiotic treatment and delayed culture sampling. CSF culture positivity for L. monocytogenes is reported in approximately 40% of clinically suspected cases [9].
MRI of the brain demonstrated characteristic tunneling abscesses in the brainstem (Figure 2A-2E). The presence of brainstem tunneling abscesses, along with a dramatic response to IV ampicillin in an elderly, immunocompromised patient, supported the diagnosis of *Listeria *rhombencephalitis. Neuromelioidosis was excluded by performing a blood melioidosis antibody assessment.
There are seven case reports in the literature describing CNS tunneling abscess formation associated with neurolisteriosis. Only one case report has described brainstem tunneling abscess formation due to *Listeria *rhombencephalitis (Table 2).
Conclusions
We report a case of a 65-year-old woman with multiple myeloma undergoing chemotherapy who presented with acute CNS infection and cranial nerve palsies. MRI demonstrated the characteristic “tunnel sign” in the brain, suggestive of tunneling abscesses in the brainstem due to Listeria rhombencephalitis. The patient showed marked improvement following IV ampicillin therapy. This case highlights that MRI is a valuable tool for diagnosing suspected neurolisteriosis, particularly when microbiological confirmation is not available.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Listeria monocytogenes meningitis in the elderly: epidemiological, clinical and therapeutic findings Infez Med Pagliano P Ascione T Boccia G De Caro F Esposito S 105111242016 https://pubmed.ncbi.nlm.nih.gov/27367319/27367319 · pubmed ↗
- 2Listeria monocytogenes brain abscess on MR imaging mimicking the track of a migrating worm like a sparganum: a case report Interdiscip Neurosurg Sakarunchai I Saeheng S Oearsakul T Sanghan N 91152016
- 3Listeriosis Clin Infect Dis Lorber B 111241997899474710.1093/clinids/24.1.1 · doi ↗ · pubmed ↗
- 4Early trigeminal nerve involvement in Listeria monocytogenes rhombencephalitis: case series and systematic review J Neurol Karlsson WK Harboe ZB Roed C Monrad JB Lindelof M Larsen VA Kondziella D 1875188426420172873057110.1007/s 00415-017-8572-2 · doi ↗ · pubmed ↗
- 5Increasing incidence of Listeriosis and infection-associated clinical outcomes Ann Lab Med Choi MH Park YJ Kim M 1021093820182921475310.3343/alm.2018.38.2.102PMC 5736668 · doi ↗ · pubmed ↗
- 6Worm-like appearance of Listeria monocytogenes brain abscess: presentation of three cases Neuroradiology Slezák O Žižka J Kvasnička T 118911936220203240572910.1007/s 00234-020-02441-9 · doi ↗ · pubmed ↗
- 7Characterisation of immunoparesis in newly diagnosed myeloma and its impact on progression-free and overall survival in both old and recent myeloma trials Leukemia Heaney JL Campbell JP Iqbal G 172717383220182992590210.1038/s 41375-018-0163-4PMC 6087716 · doi ↗ · pubmed ↗
- 8Central nervous system infection with Listeria monocytogenes: 33 years' experience at a general hospital and review of 776 episodes from the literature Medicine (Baltimore) Mylonakis E Hohmann EL Calderwood SB 313336771998977292110.1097/00005792-199809000-00002 · doi ↗ · pubmed ↗