A European survey on allogeneic haematopoietic cell transplantation for myelofibrosis on behalf of the Chronic Malignancies Working Party of the EBMT: focus on ‘real world’ experience of JAK inhibitors, splenomegaly management and novel agents in the transplant algorithm
Alexandros Rampotas, Jose Maria Aspa-Cilleruelo, Linda Koster, Daniele Avenoso, Jakob Passweg, Elisa Sala, Marie Robin, Anders Eivind Myhre, Moniek de Witte, Erfan Nur, Patrice Chevallier, Thomas Schroeder, Micha Srour, Patrizia Chiusolo, Urpu Salmenniemi, Mareike Verbeek

TL;DR
A survey of European centers shows varied practices in using JAK inhibitors and managing splenomegaly in myelofibrosis patients undergoing allogeneic transplants.
Contribution
The study provides insights into real-world practices and challenges in integrating JAK inhibitors and novel agents into myelofibrosis transplant protocols.
Findings
Most centers use ruxolitinib before conditioning to reduce splenomegaly and control symptoms.
Post-transplant reintroduction of JAK inhibitors is not routine, but some centers use them for relapse or GVHD.
Transplant delays due to prolonged medical therapy are common, leading to disease progression.
Abstract
Allogeneic haematopoietic cell transplantation (allo-HCT) remains the only potentially curative option for patients with myelofibrosis (MF), yet the integration of JAK inhibitors (JAKi) and novel agents into transplant pathways has created increasing complexity. To capture current real-world practice, the EBMT Chronic Malignancies Working Party conducted a survey of 19 high-volume European centres performing MF allo-HCT. Most centres (68%) routinely initiated JAKi, primarily ruxolitinib, in transplant-eligible patients prior to conditioning, with goals of splenomegaly reduction and symptom control. Management of ruxolitinib intolerance or resistance was heterogeneous, with strategies including switching to alternative JAKi, proceeding directly to allo-HCT, or enroling in clinical trials. Peri-transplant approaches also varied: over half of centres continued ruxolitinib throughout…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
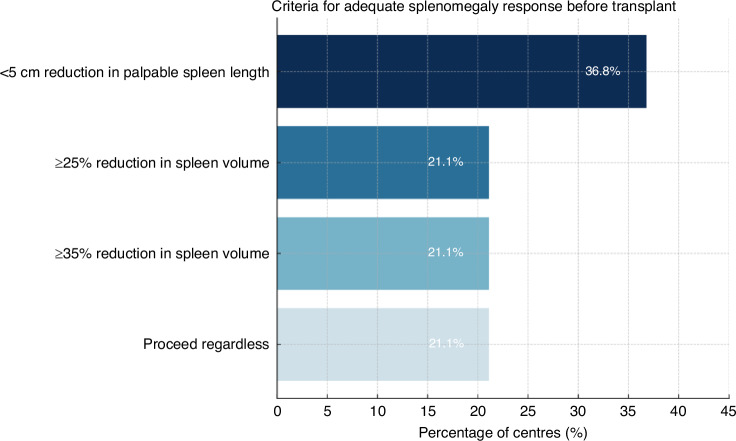 Figure 1
Figure 1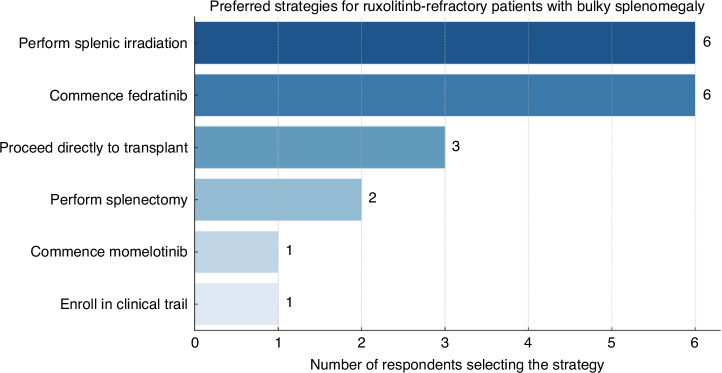 Figure 2
Figure 2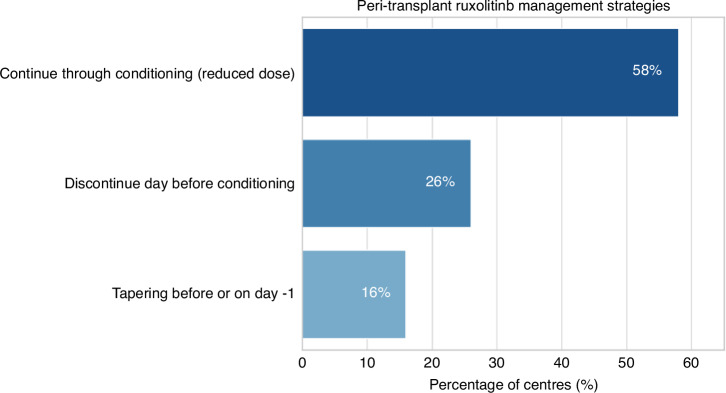 Figure 3
Figure 3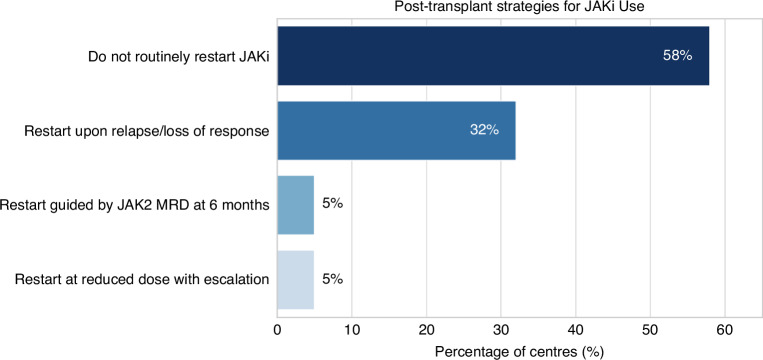 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyeloproliferative Neoplasms: Diagnosis and Treatment · Multiple Myeloma Research and Treatments · Chronic Myeloid Leukemia Treatments