Individualized rs-fMRI reveals brain-circuit heterogeneity and predicts early recurrence in trigeminal neuralgia
Zhongshuai Ma, Zhengming Wang, Xu Su, Min Cheng, Zhijia Wang, Chao Du, Yu Tian

TL;DR
This study uses brain scans to identify abnormal brain regions in trigeminal neuralgia patients and finds specific areas that predict early recurrence after treatment.
Contribution
The study introduces an individualized rs-fMRI approach to identify high-risk brain regions for early recurrence after radiofrequency ablation in trigeminal neuralgia.
Findings
Four new abnormal brain regions were identified in trigeminal neuralgia patients.
Six brain regions were found to be high-risk for early recurrence after treatment.
Abnormalities in these regions were reduced or eliminated after surgery.
Abstract
To identify abnormal brain regions in patients with trigeminal neuralgia (TN) and screen for specific regions that can predict short-term recurrence after percutaneous radiofrequency ablation (RFT). Resting-state functional magnetic resonance imaging (rs-fMRI) was used to identify differential brain regions in TN patients. An individualized rs-fMRI approach was applied to screen for recurrence-related brain regions in patients undergoing RFT. Among these, regions with a 100% recurrence rate were classified as high-risk recurrence regions. Treatment outcomes and changes in these differential brain regions were observed postoperatively. Thirty TN patients exhibited 19 differential brain regions. Four of these—Rolandic_Oper_L, Cerebellum_9_L, Lingual_R, and Calcarine_L—were newly identified as abnormal regions in TN. Among the 15 patients who underwent RFT, 15 potential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
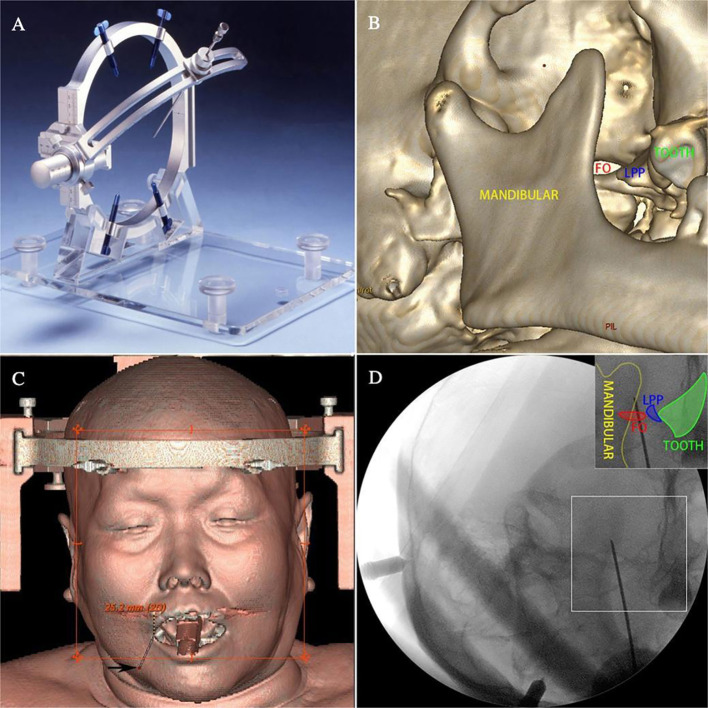 Figure 1
Figure 1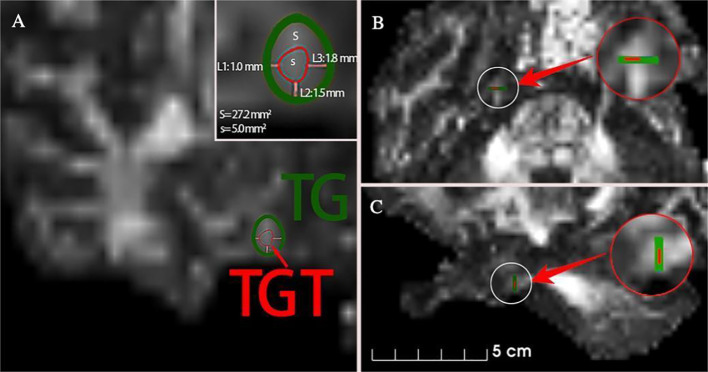 Figure 2
Figure 2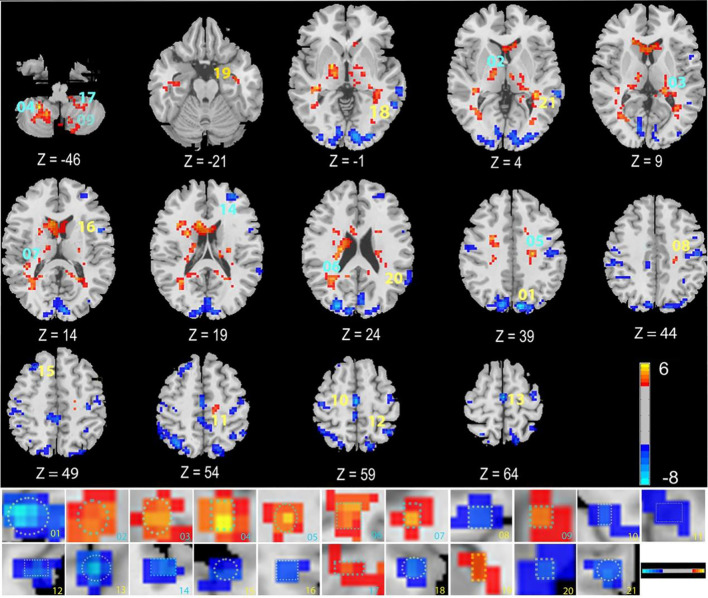 Figure 3
Figure 3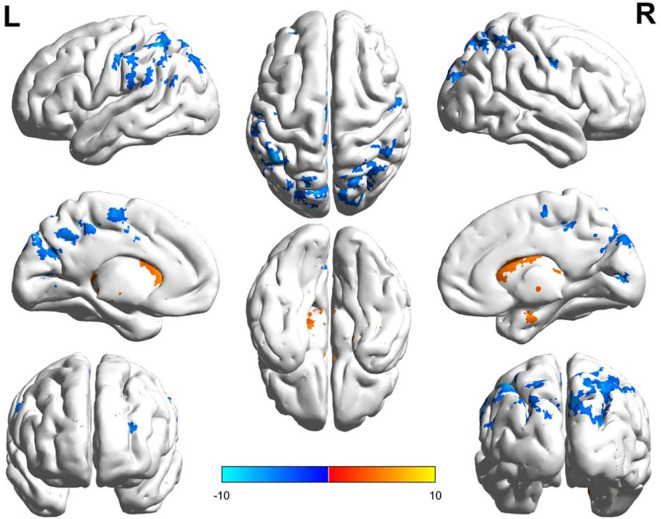 Figure 4
Figure 4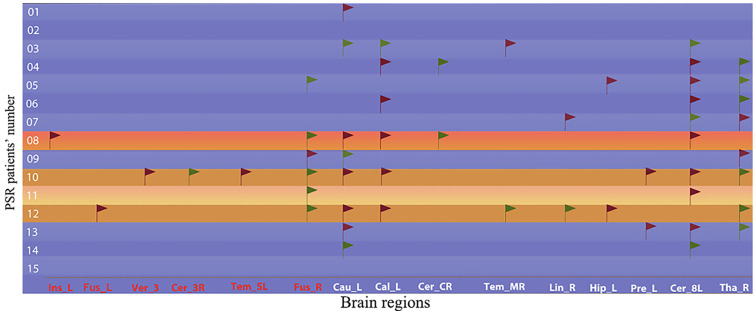 Figure 5
Figure 5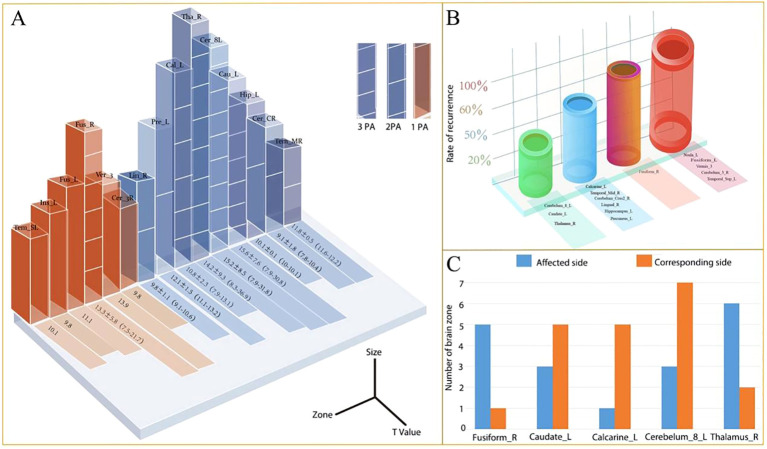 Figure 6
Figure 6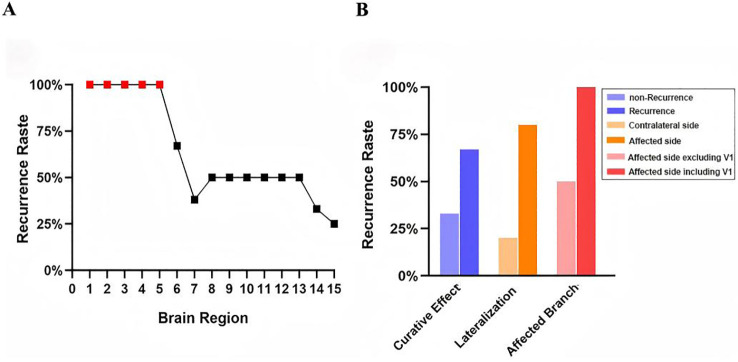 Figure 7
Figure 7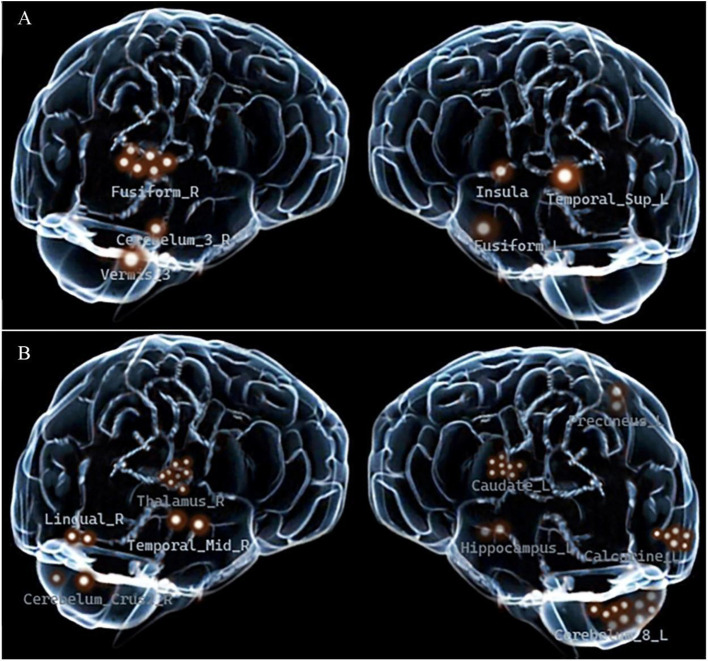 Figure 8
Figure 8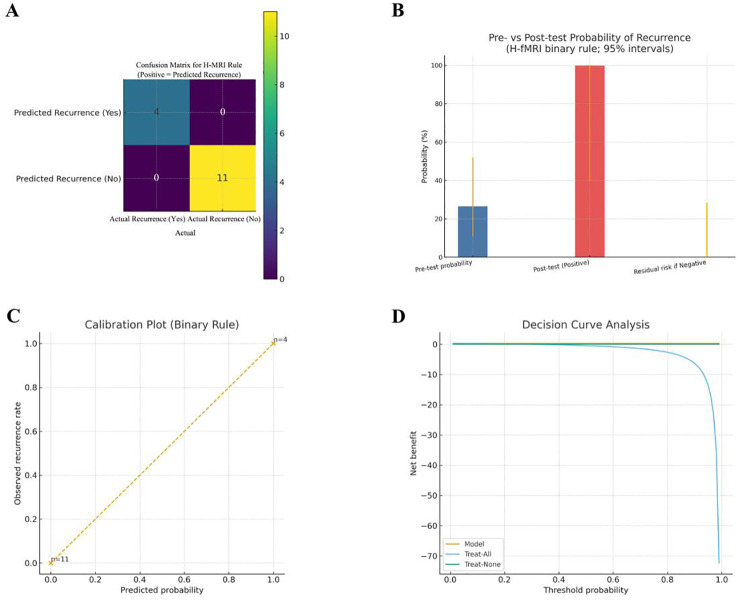 Figure 9
Figure 9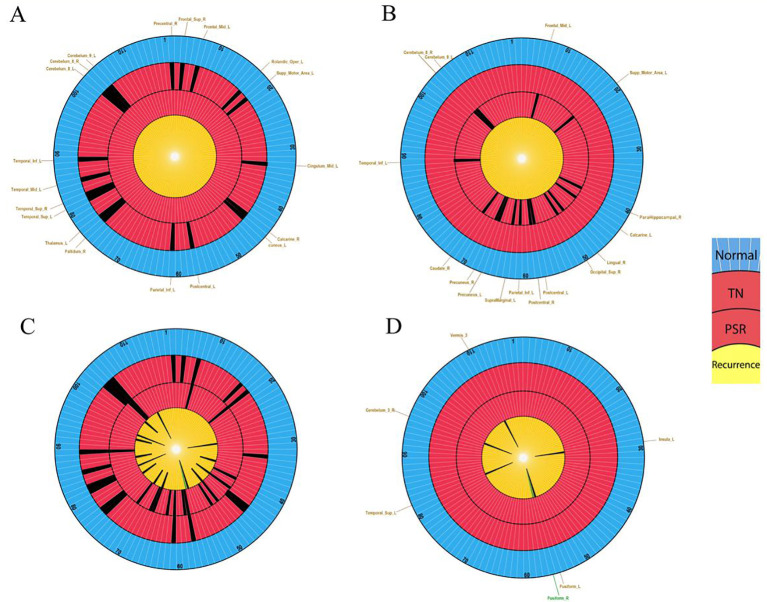 Figure 10
Figure 10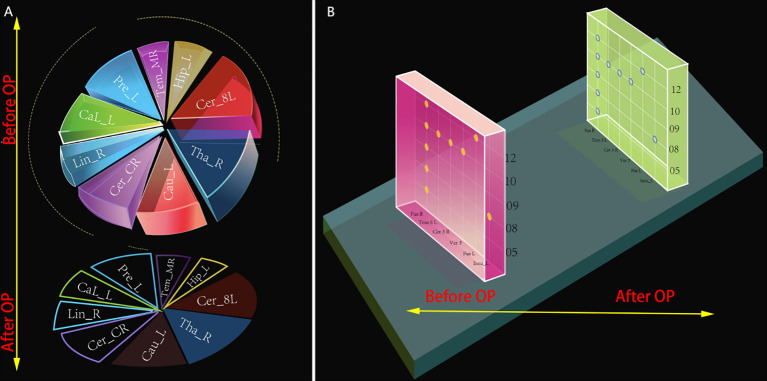 Figure 11
Figure 11| Characteristic | Number of patients | Number of PSR-DTI patients |
|---|---|---|
| Total | 30 | 15 |
| Age and sex | ||
| Age range | 38-85 | 38-85 |
| Age (Mean ± SD) | 62.9 ± 11.5 | 65.5 ± 11.7 |
| Male | 13 | 6 |
| Female | 17 | 9 |
| Affected side | ||
| Right | 18 | 11 |
| Left | 12 | 4 |
| V1 | 1 | 1 |
| V2 | 15 | 4 |
| V3 | 3 | 1 |
| V1 + V2 | 5 | 4 |
| V2 + V3 | 3 | 2 |
| V1 + V2 + V3 | 3 | 3 |
| ALL no. | No. | Brain region | Cluster size (Voxels) | MNI (X Y Z) | T value |
|---|---|---|---|---|---|
| 45 | 1 | Cuneus_L | 1367 | -9 -81 39 | -8.98862 |
| 76 | 2 | Pallidum_R | 575 | 18 -3 -3 | 6.12437 |
| 77 | 3 | Thalamus_L | 302 | -21 -30 6 | 6.19444 |
| 104 | 4 | Cerebellum_8_R | 218 | 24 -48 -45 | 5.78382 |
| 33 | 5 | Cingulum_Mid_L | 192 | -24 -18 39 | 5.58191 |
| 44 | 6 | Calcarine_R | 181 | 33 -51 24 | 5.14981 |
| 82 | 7 | Temporal_Sup_R | 157 | 39 -33 12 | 6.00197 |
| 57 | 8 | Postcentral_L | 120 | -51 -18 42 | -5.84031 |
| 103 | 9 | Cerebellum_8_L | 98 | -12 -63 -48 | 4.88525 |
| 2 | 10 | Precentral_R | 94 | 42 -21 60 | -4.92064 |
| 33 | 11 | Cingulum_Mid_L | 88 | 0 -36 51 | -7.14651 |
| 61 | 12 | Parietal_Inf_L | 60 | -48 -51 57 | -6.04622 |
| 19 | 13 | Supp_Motor_Area_L | 56 | 0 -18 60 | -7.35853 |
| 7 | 14 | Frontal_Mid_L | 53 | -30 48 21 | -5.85342 |
| 4 | 15 | Frontal_Sup_R | 51 | 24 27 51 | -5.41887 |
| 17 | 16 | Rolandic_Oper_L | 46 | -51 6 12 | -5.73314 |
| 105 | 17 | Cerebellum_9_L | 40 | -21 -45 -51 | 5.28106 |
| 85 | 18 | Temporal_Mid_L | 33 | -57 -51 0 | -6.1812 |
| 89 | 19 | Temporal_Inf_L | 32 | -36 -6 -24 | 4.79442 |
| 81 | 20 | Temporal_Sup_L | 32 | -63 -42 21 | -4.87135 |
| 85 | 21 | Temporal_Mid_L | 31 | -63 -36 3 | -5.65972 |
| ALL no. | No. | Brain region | Cluster size (Voxels) | MNI (X Y Z) | T value |
|---|---|---|---|---|---|
| 72 | 1 | Caudate_R | 1999 | 24 -24 42 | 8.25937 |
| 50 | 2 | Occipital_Sup_R | 663 | 27 -84 24 | -7.77502 |
| 105 | 3 | Cerebellum_9_L | 316 | -12 -51 -39 | 7.39727 |
| 104 | 4 | Cerebellum_8_R | 175 | 30 -63 -51 | 6.19134 |
| 43 | 5 | Calcarine_L | 174 | -30 -66 6 | 5.99316 |
| 61 | 6 | Parietal_Inf_L | 135 | -48 -51 57 | -8.37313 |
| 67 | 7 | Precuneus_L | 118 | -3 -54 42 | -6.21712 |
| 57 | 8 | Postcentral_L | 105 | -51 -15 45 | -7.70574 |
| 43 | 9 | Calcarine_L | 65 | -9 -90 0 | -5.60083 |
| 68 | 10 | Precuneus_R | 60 | 18 -45 18 | 5.36338 |
| 19 | 11 | Supp_Motor_Area_L | 60 | 0 -15 63 | -6.65415 |
| 89 | 12 | Temporal_Inf_L | 56 | -39 -12 -18 | 5.69072 |
| 40 | 13 | ParaHippocampal_R | 53 | 24 -3 -27 | 5.58155 |
| 58 | 14 | Postcentral_R | 53 | 54 -6 39 | -6.7594 |
| 7 | 15 | Frontal_Mid_L | 52 | -33 48 18 | -8.17244 |
| 48 | 16 | Lingual_R | 50 | 12 -75 -6 | -7.52571 |
| 63 | 17 | SupraMarginal_L | 33 | -63 -45 30 | -4.91563 |
| 7 | 18 | Frontal_Mid_L | 30 | -27 -3 51 | -5.55443 |
| Brain zone | Quantity of appearance | Complete remission and percentage (%) | Recurrence and percentage (%) |
|---|---|---|---|
| Insula-L |
|
|
|
| Fusiform_L |
|
|
|
| Vermis_3 |
|
|
|
| Cerebellum_3_R |
|
|
|
| Temporal_Sup_L |
|
|
|
| Fusiform_R |
|
|
|
| Caudate_L | 8 | 5 (63%, 5/8) | 3(37%, 3/8) |
| Calcarine_L | 6 | 3(50%, 3/6) | 3(50%, 3/6) |
| Cerebellum_Crus2_R | 2 | 1(50%, 1/2) | 1(50%, 1/2) |
| Temporal_Mid_R | 2 | 1(50%, 1/2) | 1(50%, 1/2) |
| Lingual_R | 2 | 1(50%, 1/2) | 1(50%, 1/2) |
| Hippocampus_L | 2 | 1(50%, 1/2) | 1(50%, 1/2) |
| Precuneus_L | 2 | 1(50%, 1/2) | 1(50%, 1/2) |
| Cerebellum_8_L | 10 | 7(70%, 7/10) | 3(30%, 3/10) |
| Thalamus_R | 8 | 6(75%, 6/8) | 2(25%, 2/8) |
| Brain zone | Affected side | Contralateral side | ||||
|---|---|---|---|---|---|---|
| Number of brain regions | Number of good effects | Number and percentage of poor effects (%) | Number of brain regions | Number of good effects | Number and percentage of poor effects (%) | |
| Insula-L | 0 | 0 | 0 | 1 | 0 | 1(100%, 1/1) |
| Fusiform_L | 0 | 0 | 0 | 1 | 0 | 1(100%, 1/1) |
| Vermis_3 | 0 | 0 | 0 | 1 | 0 | 1(100%, 1/1) |
| Cerebellum_3_R | 1 | 0 | 1(100%, 1/1) | 0 | 0 | 0 |
| Temporal_Sup_L | 0 | 1 | 0 | 1 | 0 | 1(100%, 1/1) |
| Fusiform_R | 5 | 1 | 4(80%, 4/5) | 1 | 1 | 0 |
| Caudate_L | 3 | 3 | 0 | 5 | 2 | 3(60%, 3/5) |
| Calcarine_L | 1 | 1 | 0 | 5 | 2 | 3(60%, 3/5) |
| Cerebellum_Crus2_R | 2 | 1 | 1(50%, 1/2) | 0 | 0 | 0 |
| Temporal_Mid_R | 1 | 0 | 1(50%, 1/2) | 1 | 1 | 0 |
| Lingual_R | 1 | 0 | 1(50%, 1/2) | 1 | 1 | 0 |
| Hippocampus_L | 0 | 0 | 0 | 2 | 1 | 1(50%, 1/2) |
| Precuneus_L | 0 | 0 | 0 | 2 | 1 | 1(50%, 1/2) |
| Cerebellum_8_L | 3 | 3 | 0 | 7 | 4 | 3(43%, 3/7) |
| Thalamus_R | 6 | 4 | 2(33%, 2/6) | 2 | 2 | 0 |
- —Natural Science Foundation of Jilin Province10.13039/100007847
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrigeminal Neuralgia and Treatments · Migraine and Headache Studies · Meningioma and schwannoma management
Introduction
Trigeminal neuralgia (TN) is a severe neurological disorder characterized by paroxysmal pain (1, 2). The primary surgical treatment modalities for TN include: microvascular decompression(MVD), percutaneous radiofrequency thermocoagulation (RFT), and gamma knife radiosurgery (GKS) (1, 3, 4). The coexistence of multiple surgical approaches for TN stems from the distinct advantages and disadvantages associated with each method. RFT offers a higher safety profile, with no reported mortality or severe disability, making it suitable for patients without confirmed vascular compression on CNV, elderly patients, or those with comorbidities precluding craniotomy. Nevertheless, the relatively high postoperative recurrence rate significantly impacts the efficacy of RFT (5–9).
There are some reports about magnetic resonance imaging (MRI) and postoperative recurrence rate of RFT. 5%-10% of patients with severe vascular compression (Grade III) fund by MRI experience recurrence within 6 months postoperatively (1, 10–12). Forevermore, our previous work revealed that when classifying TN patients using MR Diffusion Tensor Imaging (MR-DTI) findings, the probability of recurrence within 6 months after RFT was 10% for the L-FA type but as high as 60% for the N-FA type (13, 14). While these studies have identified some factors contributing to short-term recurrence after RFT, the complete set of risk factors predicting short-term recurrence for individual TN patients remains incompletely defined. Predicting and preventing short-term recurrence is therefore a critical concern.
Functional magnetic resonance imaging (fMRI) is another MR technique and can analyze changes in brain activity induced by pain stimuli (15).Abnormal functional brain regions in TN are critical findings on fMRI. Key questions warranting attention are whether the abnormal activation in specific brain regions can serve as novel predictive indicators for short-term recurrence following RFT (16–18).
In this study, while applying traditional fMRI methodology, we also first established a novel rs-fMRI approach: individualized comparison of each TN patient against a normal control group. This new individualized method – individualized rs-fMRI (irs-fMRI) – holds promise for providing clinically meaningful predictive indicators of surgical treatment outcomes for individual TN patients.
Using conventional rs-fMRI methods, this study identified four novel abnormal brain regions. Furthermore, applying the irs-fMRI method to 15 consecutive patients undergoing percutaneous stereotactic radiofrequency ablation(PSR)with DTI guiding surgery, we discovered that abnormal activation in six brain regions, including Insula_L, Fusiform_L, Vermis_3, Cerebellum_3_R, Temporal_Sup_L, and Fusiform_R, can serve as predictive indicators for short-term recurrence after RFT in TN patients.
Beyond group-level effects, TN likely reflects meaningful inter-individual heterogeneity in pain-related brain circuits. Precision neuropsychiatry emphasizes linking biological heterogeneity to individualized biomarkers that can support patient stratification and targeted clinical decision-making. In chronic pain conditions such as TN, brain networks involved in sensory processing, salience, affect, and memory may jointly shape symptom severity and treatment response. Therefore, an individualized rs-fMRI strategy that evaluates each patient against a normative reference could provide a practical imaging biomarker for identifying patients at higher risk of early relapse and for informing precision-oriented follow-up and targeted intervention planning.
Methods
Study subjects
Subjects: A total of 30 patients with TN (12 males, 18 females; age 62.93 ± 11.52 years) were enrolled from China-Japan Union Hospital of Jilin University. The inclusion criteria were as follows: (1) Diagnosis of TN meeting the criteria of the International Classification of Headache Disorders, 3rd edition (ICHD-3) (19); (2) Seeking treatment at the Department of Neurosurgery, China-Japan Union Hospital of Jilin University (Changchun City, Jilin Province) between March 2021 and December 2024.The inclusion criteria for the healthy control group were: (1) No history of neurological or psychiatric disorders; (2) No history of trigeminal nerve-related pain. Exclusion criteria for both groups: (1) Contraindications for MRI/fMRI scanning; (2) History of other facial pain syndromes or prior invasive surgical interventions for trigeminal neuralgia.
All participants provided written informed consent. Written consent for publication of a potentially identifiable facial photograph (Figure 1) was obtained from the patient.
PSR surgical equipment and procedure. (A) Komai’s frame-based CT-Stereotactic system. (B) 3D CT reconstruction image for FOT localization. (C) Application of the air-to-air meeting technique to complete the puncture. (D) X-ray C-arm verification of the puncture needle reaching the FOT.
Grouping: All 30 TN patients (VAS score 4-10) constituted the TN observation group (TN group). Fifteen patients who underwent PSR-DTI surgery constituted the PSR observation group (PSR group). Within the PSR group, patients experiencing postoperative recurrence formed the recurrence subgroup, while patients achieving complete pain relief formed the non-recurrence subgroup. Thirty healthy individuals served as the control group.
PSR Surgical Method: PSR surgery was performed using the Komai’s frame-based CT-Stereotactic system (Mizuho Medical Innovation, Tokyo, Japan) (Figure 1) and guided by MR-DTI images for aim at the trigeminal Gasserian target (TGT) (13, 14) (Figure 2). RFT parameters: patients with V1 division involvement received continuous pulsed radiofrequency at 65 °C for one cycle of 60 seconds; V2 division involvement received 70 °C for two cycles of 120 seconds each; V3 division involvement received 75 °C for 2-4 cycles of 120 seconds each.
MR-DTI Imaging for Trigeminal Ganglion Treatment Target (TGT) (A, B) Axial and coronal images showing the TGT located medially within the center of the Trigeminal Ganglion (TG). (C) Coronal image showing the TGT located inferiorly within the TG.
Data analysis
Data were acquired on a 3.0 T Siemens Skyra (32-channel head coil). T1 MP-RAGE: TR/TE/TI 2000/2.29/900 ms, flip 8°, 0.9-mm isotropic. rs-fMRI: T2*-EPI, TR/TE 2000/30 ms, flip 90°, FOV 200×200 mm, 60 slices, 2.0/0.4 mm thickness/gap, 80×80, multiband 3, 10 min (300 volumes). Preprocessing (DPABI/MATLAB): discard first 10 volumes, slice-timing, realignment; exclude translation >2 mm, rotation >2°, or mean FD >0.3 mm (20). Coregister to T1; nuisance regression (6 motion, WM/CSF), detrend, band-pass 0.01–0.08 Hz. ReHo was computed in native space (3×3×3 voxels, Kendall’s W), global-mean normalized, then normalized to MNI with DARTEL, resampled to 2 mm, and smoothed (4-mm FWHM). Frames with FD >0.5 mm were scrubbed (proportion recorded). Cases with poor brain extraction/segmentation were excluded (21).
Statistical analysis
Group-level analyses used a mass-univariate GLM with age, sex, and mean FD as covariates. Multiple-comparison control used permutation testing (5,000) with TFCE (two-tailed, FWE-corrected p<0.05; minimum cluster extent reported). Individual normative deviation maps were obtained by z-scoring each patient’s ReHo against age/sex-matched HCs, applying |Z|≥2.3 and cluster-wise FWE via permutation. For predicting ≤6-month recurrence, we fit penalized logistic regression with H-fMRI indicators (presence/side, V1 involvement) and clinical covariates (age, sex, disease duration, side, mean FD). Performance was optimism-corrected (0.632+ bootstrap, 1,000 resamples) with 95% CIs for AUC, sensitivity, specificity, and PPV/NPV.
Clinical outcome assessment
Efficacy was evaluated at postoperative days 2–3 and at 6 months, 1 year, 2 years, and 3 years. Recurrence was graded by medication required to control pain (pre-specified standardized dose units): mild, < 50% of the preoperative dose with no additional intervention; moderate, 50–100%; severe, > 100% or uncontrolled pain requiring re-intervention. The primary endpoint for short-term recurrence was ≤ 6 months. “Effective” was defined as pain-free without medication or only mild recurrence; “Ineffective” as moderate or severe recurrence.
Results
Demographic and clinical data
Thirty TN patients were included: 15 managed with medication and 15 treated with PSR-DTI surgery. Full clinical characteristics are presented in Table 1.
Treatment outcomes
All 15 patients achieved successful TGT puncture. Sensory electrophysiological validation at the TGT (50 Hz, 1ms pulse) yielded voltage values ranging from 0.15-0.30 V.
Postoperative Days 2-3: 13 patients had VAS scores of 1-3, and two patients achieved VAS = 1 on postoperative days 4 and 14, respectively. Immediate overall efficacy was 86.6% (13/15).
6 Months Postoperative: 11 patients experienced complete pain relief, and four patients developed moderate or severe recurrence. Ultra-short-term efficacy was 73.3% (11/15); recurrence rate was 26.7% (4/15).
1 Year Postoperative: Effective treatment in 12 patients (including 11 with complete relief and 1 transitioning from moderate to mild recurrence). Ineffective treatment occurred in 3 patients. Short-term efficacy was 80% (12/15).
2 Years Postoperative: No new recurrences occurred. Long-term efficacy remained 80% (12/15).
3 Years Postoperative: One new moderate recurrence occurred (No.1). Long-term efficacy at 3 years was 73.3% (11/15).
Most recurrences (80%, 4/5) occurred within 6 months postoperatively. One recurrence (20%, 1/5) occurred at 3 years. No new recurrences arose between 6 months and 2 years. These findings indicate that precise PSR-DTI targeting of the TGT substantially inhibited (91%, 10/11) neural regeneration-mediated recurrences occurring between 1 year to 3 years.
Differential brain region findings in TN subgroups
TN Group: rs-fMRI identified 19 differential brain regions across all 30 TN patients (VAS 4-10) (Figure 3, Table 2). The presence of these regions may contribute to TN pathophysiology.
Regional homogeneity differences in TN patients. Differential analysis between TN patients and HC was performed using two-sample t-tests. The color bar represents the t-statistic values; warm colors (e.g., red/yellow) indicate brain regions with significantly increased ReHo values (positive t-values) in TN patients compared to controls, whereas cool colors (e.g., blue) indicate regions with significantly decreased ReHo values (negative t-values). The statistical significance threshold was set at GRF-corrected p < 0.05. Abbreviations: ReHo: Regional Homogeneity; TN: Trigeminal Neuralgia; HC: Healthy Controls; GRF: Gaussian Random Field.
PSR-DTI Group: Preoperative rs-fMRI identified 16 differential brain regions in the 15 PSR-DTI patients (VAS = 10) (Figure 4, Table 3). Compared to the TN group, 9 regions were novel: Caudate_R, Occipital_Sup_R, Calcarine_L, Precuneus_L, Precuneus_R, ParaHippocampal_R, Postcentral_R, Lingual_R, SupraMarginal_L. This suggests novel regional abnormalities may indicate progression requiring surgery.
ReHo differences in PSR-DTI surgical patients. Differential analysis between the PSR-DTI group and HC was performed using two-sample t-tests, with results projected onto the brain surface. The color bar indicates the range of t-values: red/yellow regions denote significantly increased ReHo (positive t-values) relative to HC, while blue regions denote significantly decreased ReHo (negative t-values). The statistical threshold was set at GRF-corrected p < 0.05. Numbered regions correspond to: 1-Caudate_R, 2-Occipital_Sup_R, 3-Cerebellum_9_L, 4-Cerebellum_8_R, 5-Calcarine_L (X=-30, Y=-66, Z = 6), 6-Parietal_Inf_L, 7-Precuneus_L, 8-Postcentral_L, 9-Calcarine_L (X=-33, Y=-48, Z = 18), 10-Precuneus_R, 11-Supp_Motor_Area_L, 12-Temporal_Inf_L, 13-ParaHippocampal_R, 14-Postcentral_R, 15-Frontal_Mid_L, 16-Lingual_R, 17-SupraMarginal_L, 18-Frontal_Mid_L (X=-27, Y=-3, Z = 51).
Rs-fMRI in the 4 recurrence patients identified 15 differential regions, including: Insula, Fusiform_L, Vermis_3, Cerebellum_3_R, Temporal_Sup_L, Fusiform_R, Caudate_L, Calcarine_L, Cerebellum_Crus2_R, Temporal_Mid_R, Lingual_R, Hippocampus_L, Precuneus_L, Cerebellum_8_L and Thalamus_R. These regions (we named them as 1-15, respectively) constitute a library of potential predictive brain regions (PPBR) for recurrence.
Screening predictive brain regions for short-term recurrence
Entire PSR-DTI Group (n=15): Total PPBR occurrences were 53 instances across all patients which including 13 patients exhibited 1-9 PPBRs and 2 patients had no PPBR, 45% in ipsilateral and other 55% in contralateral (Figure 5).
Positive sites of potential predictive brain regions for recurrence in TN patients. Treatment Outcome: =Excellent (Pain-free, no meds); =Good (Mild recurrence; pain reduction ≥50%, reduced meds); =Fair (Slight relief; pain reduction <50%); =Poor (No relief). Laterality: =Ipsilateral; =Contralateral.
PSR-DTI Recurrence Subgroup (n=4): Total PPBRs were 25 instances, mean times was 6.3 in per patient, 40% in ipsilateral and 60% in contralateral.
PSR-DTI Non-Recurrence Subgroup (n=11): Total PPBRs were 28 instances, mean times was 2.5 in per patient, 61% in ipsilateral and 39% in contralateral.
Patients with recurrence exhibited a significantly higher mean PPBR burden (6.3 vs. 2.5; mean difference 2.5-fold, 95% CI: 2.1-5.5; t (13) = 3.92, p = 0.002, Cohen**’**s d = 1.74) and a greater proportion of contralateral PPBRs (61% vs. 39%) compared to non-recurrence patients. These findings indicate that both novel and contralateral abnormalities are associated with an increased risk of recurrence.
Preliminary screening of predictive regions
Frequency & Recurrence Rate: Regions 1-5, Occurred only once, and exclusively in recurrence patients (100% recurrence rate); Regions 6-15, Occurred in both recurrence and non-recurrence patients; Regions 6, 7, 8, 14, 15 (common, 6-10 occurrences) and 9-13 (rare, all were 2 occurrences) showed varying recurrence rates (Figure 6, Table 4). Thus, regions 1-5 were selected as primary predictive candidates, and Region 6 (Fusiform_R) was identified as a secondary candidate due to its relatively higher recurrence rate.
Characteristics of potential predictive brain regions for pain recurrence in PSR-DTI patients. (A) Number and value of positive brain regions. (B) Recurrence rate per PPBR. (C) Distribution of common abnormal brain regions (3 PA = 3 patients; 2 PA = 2 patients; 1 PA = 1 patient).
Refining the predictive role of Fusiform_R
Overall Recurrence Rate: 67% (4/6) (Figure 7A). Laterality: recurrence rate was 80% (4/5) for ipsilateral Region 6 abnormality vs. 0% (0/1) for contralateral. Trigeminal branch involvement: recurrence rate was 100% (2/2) for patients with region 6 abnormality and V1 division pain (Case 10: V1+V2+V3; Case 12: V1+V2), recurrence rate was 50% (2/4) for region 6 abnormality without V1 pain (Figure 7B). Thus, ipsilateral region 6 abnormality combined with V1 pain predicted recurrence with 100% accuracy, equivalent to regions 1-5.
Recurrence risk stratification based on fMRI-Defined brain regions. (A)Recurrence rates across 15 potential predictive brain regions. (B) Differential recurrence rates associated with Fusiform_R under specific clinical conditions.
Recurrence risk stratification via final predictive brain regions
Recurrence rates for unilateral Regions 7-15 ranged from 33%-60% (Table 5). Six regions with 100% recurrence rate within contralateral Insula, Fusiform_L, Vermis_3 and Temporal_Sup_L, ipsilateral Cerebellum_3_R, Fusiform_R with V1 division pain, constitute the final set of High-Risk fMRI (H-fMRI) regions of recurrence (Figure 8).
Spatial distribution of fMRI-based risk regions in surgical trigeminal neuralgia patients. (A) Six kinds of high-risk fMRI regions. (B) Nine middle- and low-risk fMRI regions. Each highlighted marker represents a positive finding in a single patient scan.
The pre-specified six-region H-fMRI binary rule achieved apparent perfect discrimination in the PSR-DTI derivation cohort and showed marked post-test probability shifts with favorable net benefit on decision-curve analysis (Figure 9).
Apparent performance of the pre-specified H-fMRI rule in the PSR-DTI derivation cohort (n=15; 4 recurrences ≤6 months). (A) Confusion matrix (positive = predicted recurrence): TP = 4, TN = 11, FP = 0, FN = 0, showing apparent perfect classification. (B) Pre-/post-test probability of recurrence (4/15, 4/4, 0/11; 95% CIs). (C) Calibration: two-point calibration for the binary rule (observed recurrence rates at predicted = 1 and predicted = 0); the 45° line denotes ideal calibration. (D) Decision curve: net benefit across threshold probabilities 0.01–0.99; the model overall outperforms Treat-All and Treat-None.
Analysis of H-fMRI regional location characteristics
Automated Anatomical Labeling (AAL) Atlas includes 116 normal regions. TN Group (19 regions) vs. PSR-DTI Group (16 regions), 7 overlapping regions (36.8% overlap); recurrence PPBRs (15 regions) vs. PSR-DTI Group, 3 overlapping regions (18.7% overlap); H-fMRI Regions (6 regions) vs. PSR-DTI Group, 0% overlap; H-fMRI Regions vs. TN Group, 1 overlapping region (5.2% overlap) (Figure 10). These results suggesting that patient-specific H-fMRI regions may drive short-term recurrence.
Schematic representation of brain region locations in healthy individuals and TN patients. (A) Healthy individuals (116 regions, blue circle) vs. TN patients VAS 4-10 (19 positive regions, outer red circle). (B) PSR-DTI patients VAS 8-10 (16 positive regions, inner red circle). (C) Recurrence patients (15 Potential Predictive Brain Regions, yellow circle). (D) Recurrence patients (6 high-risk fMRI Regions, yellow circle). Insets show regional distributions.
Changes in brain regions 2-3 days post-PSR-DTI
13 patients whom VAS were 1-3: All 15 recurrence-related differential regions disappeared (100% elimination). Two patients with VAS scores of 4: 12 recurrence-related regions (6 H-fMRI, 6 L-fMRI) disappeared (80%, 12/15), and 3 regions weakened (Caudate_L & Cerebellum_8_L in Case No.8; Thalamus_R in Case No.10) (Figure 11).
Schematic of potential predictive brain regions pre- and post PSR-DTI in TN patients. (A) Nine regions positive preoperatively in both outcome groups (Top). Six boxed regions disappeared postoperatively (Bottom); three unboxed regions showed weakened activity. (B) Five regions positive preoperatively only in the poor outcome group, plus Fusiform_R (Left). All six regions disappeared postoperatively (Right).
Discussion
Recurrence in TN patients after RFT can be categorized into two types based on the timing of onset: short-term recurrence (STR) which occurring within 1 year postoperatively, and long-term recurrence (LTR) which occurring more than 1 year postoperatively. Reported rates of STR and LTR vary considerably in the literature. STR rates fall into three ranges: low range (<9.8%) (22–26), medium range (12%—17%) (27–30), and high range (21%—56%) (31–34). Two-year LTR rates are distributed into two ranges: low range (7%—17%) (25, 26, 35) and high range (20%—50%) (5, 28, 29, 33, 36, 37).
The currently prevailing theoretical explanation for LTR is the regeneration of nerve fibers within the TGT occurring 1-3 years postoperatively, leading to the reappearance of pain (5), termed neuroregeneration-mediated recurrence. Regarding STR, we propose that it represents non-neuroregeneration-mediated recurrence under the premise of effective RFT, i.e., recurrence due to patient-specific factors.
Indeed, not only STR research had been received considerable attention (31–34), but STR occurring even earlier (within 1-6 months) has also been noted (23, 24, 31, 38). J. Piquer et al. (39) reported a 1-year recurrence rate of 13% (13/98), but patients recurring within one year accounted for 46% (13/30) of all recurrences observed over more than three years. In our cohort, STR patients constituted 80% (4/5) of all recurrences within 3 years postoperatively. We speculate that the unusually high STR rate in our group may be related to a relatively higher proportion of patients with specific constitutional factors.
To date, 23 brain regions have been identified by various researchers as abnormally functional in TN patients (2, 40–42). We identified 19 abnormal functional brain regions in TN patients. The majority of these abnormal regions (68.4%, 13/19) were fully consistent with literature reports, a smaller portion (21.0%, 4/19) partially consistent, while abnormalities in the Rolandic_Oper_L and Cerebellum_9_L regions have not been previously reported in the literature.
Furthermore, in 15 PSR group patients with VAS scores of 10, we identified 16 abnormal brain regions. Among these, abnormalities in 9 regions related to pain perception, pain processing, emotional processing, vision, and memory differed from those observed in the broader TN group. This finding suggests that TN patients with severe pain possess unique characteristics in their abnormal brain region distribution. Among these 16 abnormal regions, abnormalities in Cerebellum_9_L, Lingual_R, and Calcarine_L have not been previously reported.
Overall, our study identified four novel abnormal brain regions in TN patients: Rolandic_Oper_L, Cerebellum_9_L, Lingual_R, and Calcarine_L. We attribute these findings to differences in the clinical characteristics of enrolled TN patients and variations in fMRI methodologies across studies. In fact, Liang Y et al. (43) also noted a lack of consistency in the locations of abnormal brain regions reported by different centers conducting fMRI research on TN patients.
Traditionally associated with motor control, the cerebellum is increasingly recognized for its critical role in non-motor functions, including pain modulation and emotional processing. The “cognitive-affective cerebellum” theory suggests that the posterior lobe and vermis serve as integral nodes within the pain matrix and salience network, specifically influencing the affective-motivational dimension of pain. Persistent abnormalities in these regions (e.g., Vermis_3 and Cerebellum_3_R) observed in our high-risk cohort may reflect entrenched central sensitization or maladaptive emotional learning associated with chronic neuropathic pain. Consequently, these central circuit disturbances could drive early symptom recurrence, independent of the technical success of the peripheral nerve intervention.
Departing from previous group-level comparison methods, this study also performed individual case-control comparisons for each of the 15 PSR group patients against a normal control group. Based on this cohort, all patients exhibiting abnormalities in one or more of the following regions (contralateral Insula_L, Fusiform_L, Vermis_3, Temporal_Sup_L, and ipsilateral Cerebellum_3_R, Fusiform_R with V1 involvement) experienced short-term recurrence after PSR-DTI. We therefore refer to these regions as candidate high-risk fMRI regions for recurrence risk stratification, pending external validation. Consequently, we define these 6 brain regions as high-risk recurrence regions on fMRI (H-fMRI) for individual TN patients undergoing PSR. Abnormalities in the Vermis_3 and Cerebellum_3_R regions in TN patients have not been previously reported.
The distinct predictive value of V1 division involvement combined with Fusiform_R abnormalities may be attributed to both anatomical and functional factors. Clinically, radiofrequency ablation of the ophthalmic (V1) division often requires more conservative temperature parameters to preserve the corneal reflex, which can potentially lead to less complete denervation compared to procedures targeting the V2 or V3 divisions. Functionally, the fusiform gyrus is integral to higher-order visual and object processing. The specific coupling of V1 pain—which involves the ophthalmic nerve—with fusiform abnormalities suggests a specific maladaptive neuroplasticity within visual-pain associative pathways. This unique central network alteration may be more resistant to standard thermal coagulation, thereby predisposing patients to higher rates of early recurrence.
In this study, PSR surgery resulted in the elimination or reduction of recurrence-related differential brain regions in each TN patient. This outcome aligns with Dou Z et al. (44) reporting decreased ReHo values in the Middle Temporal Gyrus, Postcentral Gyrus, and left Insula after RFT; matches Moisset X et al. (2)reporting the disappearance of Insula activation 1-2 months post-RFT; and is largely consistent with Wen-Ching Liu et al. (45) reporting significant regression of Insula and Cerebellar activation 1-2 weeks post-RRT. These findings demonstrate that PSR-DTI surgery effectively modulates abnormal brain region activity in TN patients.
Research on individualized rs-fMRI (irs-fMRI) is clinically essential for using abnormal brain regions as an indicator to predict postoperative recurrence risk. Theoretically, irs-fMRI results could be influenced by differences in patient state during pre- and postoperative scans. In this study, irs-fMRI examinations focusing on abnormal regions within the potential recurrence library confirmed that all 15 abnormal regions were either eliminated or attenuated following effective immediate treatment. This result suggests that targeting specific brain regions is an effective approach for individualized fMRI assessment.
There are reports that TN patients whom with increased ReHo values in Insula and/or Vermis experienced moderate short-term recurrence post-RFT (2, 44). Those reports had some extent corroborate our finding that Insula and Vermis might contribute to short-term recurrence after RFT. However, the other four of our fund 6 H-fMRI regions as causes of short-term recurrence not previously reported. For the highest recurrence rates (100%) of fMRI compare with MRI (5%-15%) and DTI (60%). Taken together, these observations suggest that abnormal functional brain regions may represent an important correlate of short-term recurrence risk after RFT/PSR-DTI in TN. However, the predictive utility and generalizability of these candidate regions require prospective evaluation in larger, independent cohorts.
This study has certain limitations. We applied lateralization and branch-specific restrictions to the H-fMRI regions in this timeframe. As research sample sizes increase in the future, these lateralization and branch restrictions for H-fMRI regions may require further refinement.
Conclusion
Rolandic_Oper_L, Cerebellum_9_L, Lingual_R, and Calcarine_L were newly discovered abnormal brain regions in trigeminal neuralgia patients. For the first time, six high-risk recurrence regions on fMRI highly associated with short-term postoperative recurrence were identified: contralateral Insula_L, Fusiform_L, Vermis_3 and Temporal_Sup_L, ipsilateral Cerebellum_3_R, Fusiform_R (specifically associated with V1 division involvement). This study provides an objective imaging basis for individualized prediction of early recurrence risk after PSR-DTI in trigeminal neuralgia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bendtsen L Zakrzewska JM Heinskou TB Hodaie M Leal PRL Nurmikko T . Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia. Lancet Neurol. (2020) 19:784–96. doi: 10.1016/S 1474-4422(20)30233-7, PMID: 32822636 · doi ↗ · pubmed ↗
- 2Moisset X Villain N Ducreux D Serrie A Cunin G Valade D . Functional brain imaging of trigeminal neuralgia. Eur J Pain. (2011) 15:124–31. doi: 10.1016/j.ejpain.2010.06.006, PMID: 20609605 · doi ↗ · pubmed ↗
- 3Cruccu G Finnerup NB Jensen TS Scholz J Sindou M Svensson P . Trigeminal neuralgia: New classification and diagnostic grading for practice and research. Neurology. (2016) 87:220–8. doi: 10.1212/WNL.0000000000002840, PMID: 27306631 PMC 4940067 · doi ↗ · pubmed ↗
- 4Cruccu G Di Stefano G Truini A . Trigeminal neuralgia. N Engl J Med. (2020) 383:754–62. doi: 10.1056/NEJ Mra 1914484, PMID: 32813951 · doi ↗ · pubmed ↗
- 5Son BC Kim HS Kim IS Yang SH Lee SW . Percutaneous radiofrequency thermocoagulation under fluoroscopic image-guidance for idiopathic trigeminal neuralgia. J Korean Neurosurg Soc. (2011) 50:446–52. doi: 10.3340/jkns.2011.50.5.446, PMID: 22259692 PMC 3259465 · doi ↗ · pubmed ↗
- 6Mousavi SH Gehling P Burchiel KJ . The long-term outcome of radiofrequency ablation in multiple sclerosis-related symptomatic trigeminal neuralgia. Neurosurgery. (2022) 90:293–9. doi: 10.1227/NEU.0000000000001817, PMID: 35113822 · doi ↗ · pubmed ↗
- 7Gunduz HB Cevik OM Asilturk M Gunes M Uysal ML Sofuoglu OE . Percutaneous radiofrequency thermocoagulation in trigeminal neuralgia: analysis of early and late outcomes of 156 cases and 209 interventions. J Korean Neurosurg Soc. (2021) 64:827–36. doi: 10.3340/jkns.2020.0333, PMID: 34320779 PMC 8435657 · doi ↗ · pubmed ↗
- 8Jain A . Comparative analysis of balloon compression and radiofrequency ablation in idiopathic trigeminal neuralgia: A retrospective study with a 24-month follow-up. Turk J Anaesthesiol Reanim. (2019) 47:146–50. doi: 10.5152/TJAR.2019.53533, PMID: 31080957 PMC 6499048 · doi ↗ · pubmed ↗