Pitfall of false localization in basal temporal epilepsy: A clinical vignette
Mathieu Dhoisne, Romain Carron, Fabrice Bartolomei, Stanislas Lagarde

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
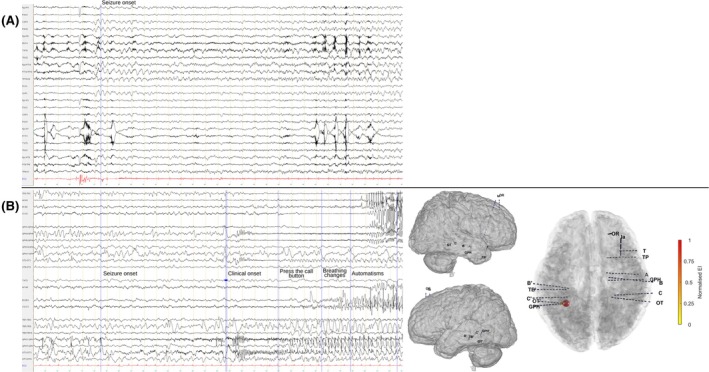 Figure 1
Figure 1- —French Ministry of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEpilepsy research and treatment · Neuroscience and Neuropharmacology Research · EEG and Brain-Computer Interfaces
False lateralization of ictal EEG onset is uncommon in temporal lobe epilepsy, but has been reported in mesial TLE with hippocampal sclerosis or vascular malformation.1, 2, 3, 4, 5, 6, 7 This phenomenon may relate to low‐amplitude ictal discharges from cortical atrophy or cerebral damage, severe hippocampal sclerosis (“burned‐out” hippocampus), rapid contralateral spread via hippocampal commissures, anterior commissure, or frontal limbic pathways, or the coexistence of multiple epileptogenic foci.1, 2, 8, 9, 10 This clinical vignette highlights the particular value of stereoelectroencephalography (SEEG) for anatomo‐electro‐clinical correlations when ictal EEG onset conflicts with imaging or semiology.
We report a 21‐year‐old right‐handed woman, with no prior medical history, who developed seizures at age nine. They initially consisted of isolated loss of awareness. At age 14, following a focal to bilateral tonic–clonic seizure, MRI revealed a left parahippocampal gyrus cavernoma, which was resected. Despite this, seizures persisted under multiple antiseizure medications.
Over time, her seizures evolved to include a rising chest sensation and déjà‐vu, followed by impaired awareness, oroalimentary automatisms, and right‐hand dystonia, with postictal headaches and aphasia. Scalp EEG showed right anterior and middle temporal spikes, with rare left anterior temporal spikes. Two habitual seizures were recorded: the first began with a right posterior temporal discharge spreading to the entire right temporal electrodes (Figure 1A), while the second was brief and without significant EEG change. Magnetoencephalography revealed predominantly right temporal spikes with rare independent left temporal discharges. Positron emission tomography (PET) demonstrated bilateral temporo‐parietal hypometabolism and focal hypometabolism at the prior resection site. Neuropsychological testing showed impaired verbal declarative memory with preserved visual memory.
Given the discordance between seizure semiology, MRI, and scalp EEG ictal onset, SEEG was performed. It revealed background slowing around the left temporo‐basal resection cavity, as well as in the right temporo‐basal region and temporal pole. Abundant pseudo‐periodic spikes arose from the left temporo‐basal region, sometimes also asymptomatic rhythmic discharges, and fewer spikes were observed in the left entorhinal and parahippocampal gyri. High‐amplitude spikes were also recorded in the right amygdala, hippocampus, and parahippocampal gyrus, activated during sleep and occurring at a lower rate than the left temporo‐basal ones. Habitual seizures were recorded during SEEG, showing a characteristic progression (Figure 1B). They began with flattening and disappearance of interictal spikes, followed by a progressive build‐up of low‐voltage fast activity in the left parahippocampal gyrus, then rhythmic theta activity in both temporo‐basal regions. Two distinct hemispheric patterns were observed: on the left, a sinusoidal alpha rhythm with superimposed fast activity evolved into spike–wave discharges in the temporo‐basal area, propagating to the hippocampus after 15 seconds; on the right, low‐voltage fast activity arose in the temporo‐basal area, spreading to the amygdala and hippocampus after 20 seconds, and to the insula after 25 seconds. Seizure activity terminated earlier on the right than on the left. The patient underwent SEEG‐guided radiofrequency thermocoagulation of the left temporo‐basal contacts surrounding the resection cavity and has remained seizure‐free for 9 months.
This case highlights the key role of anatomo‐electro‐clinical correlations in defining the epileptogenic zone. Any discrepancies should prompt suspicion and warrant further exploration with SEEG.6, 7 In such cases, bilateral SEEG implantation with extensive sampling of mesial and basal temporal structures is paramount to distinguish delays in regional involvement at seizure onset. In our patient, omission of electrodes around the resection cavity would have led to recording only the bitemporal activity emerging after the true onset, potentially leading to the erroneous diagnosis of bitemporal epilepsy. In our patient, seizure semiology (right‐hand dystonia and postictal aphasia) suggested a left temporal onset, consistent with the left‐sided resection cavity but conflicting with the right‐sided onset on EEG. SEEG exploration demonstrated a left temporo‐basal epileptogenic zone with rapid contralateral propagation. Several factors may explain the false lateralization. The deep location and limited spatial extent of the seizure onset zone, combined with the low amplitude of the initial ictal discharge, likely precluded the detection of early ictal activity on scalp EEG. Consequently, the recorded ictal EEG primarily reflected the propagation of the discharge, which exhibited greater amplitude and spatial spread in the right temporal lobe. Similar mechanisms have been previously proposed in the literature.1, 2 The resection cavity may also have restricted ipsilateral propagation toward the anterior left temporal lobe, enhancing the visibility of the right‐sided spread.
CONFLICT OF INTEREST STATEMENT
The authors have no conflict of interest to disclose.
Test yourself
- Which of the following mechanisms can explain false lateralization of ictal EEG onset in temporal lobe epilepsy?
- Rapid contralateral propagation via commissural pathways
- High‐amplitude ictal onset in the true seizure zone
- Low‐amplitude ictal discharges in atrophic or damaged cortex
- Multiple independent epileptogenic zones
- Increased scalp EEG sensitivity for mesial temporal structures
- Which clinical or investigative finding should raise suspicion for false lateralization in a patient with temporal lobe epilepsy?
- Concordant seizure semiology, imaging, and EEG
- Ictal EEG onset contralateral to the lesion
- Bitemporal interictal spikes with consistent unilateral seizure onset on EEG
- Neuropsychological deficit not concordant with ictal scalp EEG (e.g., verbal memory deficit with right‐sided EEG onset)
- Discordant semiological lateralizing signs (e.g., dystonic hand)
- Which of the following strategies helps reduce the risk of misinterpretation due to false lateralization during presurgical evaluation of temporal lobe epilepsy?
- Use of scalp EEG only
- Bilateral SEEG implantation with comprehensive sampling of mesial and basal temporal structures
- Recording of several habitual seizures
- Relying solely on interictal spike location
- Avoiding overinterpretation of the frequent increase in mesiotemporal spikes during sleep, which may occur in non‐epileptogenic regions
Answers may be found in the supporting information
Supporting information
Data S1:
Data S2:
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hatano K , Sato K , Nakamura T , Hotta R , Numoto S , Fujimoto A . Cavernous malformation located medially and deeply in the brain may be prone to false lateralization in cavernous malformation‐associated epilepsy. Heliyon. 2024;10(6):e 28273.38545148 10.1016/j.heliyon.2024.e 28273 PMC 10966682 · doi ↗ · pubmed ↗
- 2Gaviria Carrillo M , López J , Rodríguez QJH , Gaona I , Ortiz‐Guerrero G , Nava‐Mesa MO . Apparent false lateralization of seizure onset by scalp EEG in temporal lobe epilepsy associated with cerebral cavernous malformation: a case report and overview. Brain Sci. 2020;10(9):584.32846994 10.3390/brainsci 10090584 PMC 7565586 · doi ↗ · pubmed ↗
- 3Nakamura T , Hatano K , Sato K , Enoki H , Fujimoto A . False lateralization of scalp EEG and semiology in cavernous malformation‐associated temporal lobe epilepsy: a case report. Heliyon. 2023;9(7):e 18237.37501958 10.1016/j.heliyon.2023.e 18237 PMC 10368837 · doi ↗ · pubmed ↗
- 4Risinger MW , Engel J , Van Ness PC , Henry TR , Crandall PH . Ictal localization of temporal lobe seizures with scalp/sphenoidal recordings. Neurology. 1989;39(10):1288–1293.2797451 10.1212/wnl.39.10.1288 · doi ↗ · pubmed ↗
- 5Engel J . Consistent false lateralization of seizure onset with sphenoidal and scalp telemetered ictal EEG recording in two patients with partial epilepsy. Electroencephalogr Clin Neurophysiol. 1980;50:160.
- 6Sammaritano M , de Lotbinière A , Andermann F , Olivier A , Gloor P , Quesney LF . False lateralization by surface EEG of seizure onset in patients with temporal lobe epilepsy and gross focal cerebral lesions. Ann Neurol. 1987;21(4):361–369.3579221 10.1002/ana.410210408 · doi ↗ · pubmed ↗
- 7Spencer SS , Williamson PD , Bridgers SL , Mattson RH , Cicchetti DV , Spencer DD . Reliability and accuracy of localization by scalp ictal EEG. Neurology. 1985;35(11):1567–1575.4058746 10.1212/wnl.35.11.1567 · doi ↗ · pubmed ↗
- 8Amrie F , Sejahtera D , Khairani A , Vidyanti A . False lateralization of electroencephalogram in epilepsy patient with neuroglia cyst: a case report. J Neurol Sci. 2023;455:120662. 10.1016/j.jns.2023.120662 · doi ↗