Cost-effectiveness of personalized medical treatment in acromegaly: a post hoc analysis of the ACROFAST study
Montserrat Marques-Pamies, Laura Ricou, Joan Gil, Miguel Sampedro-Núñez, Betina Biagetti, Olga Giménez-Palop, Marta Hernández, Silvia Martínez, Cristina Carrato, Rocío Villar-Taibo, Marta Araujo-Castro, Concepción Blanco, Inmaculada Simón-Muela, Andreu Simó-Servat, Gemma Xifra

TL;DR
Personalized treatment for acromegaly using biomarkers is more effective and cost-effective than standard treatment.
Contribution
Demonstrates that personalized treatment based on biomarkers reduces costs and improves disease control in acromegaly.
Findings
Personalized treatment increased disease control probability by 2.53 times compared to standard treatment.
IGF1 normalization occurred in 78% of personalized treatment patients versus 53% with standard treatment.
Average cost per patient for disease control was 22% lower with personalized treatment.
Abstract
Medical treatment of acromegaly is currently performed through a trial-and-error approach using first-generation somatostatin receptor ligands (fgSRLs) as first-line drugs, with an efficacy of 50%. Some biomarkers can predict patient response, potentially benefiting nonresponders by using personalized treatment approaches. The ACROFAST study revealed that the probability of disease control was 2.53 times higher (CI 1.30-4.80) with personalized treatment, and insulin-like growth factor 1 (IGF1) normalization occurred in 78% vs 53% of patients, compared with standard treatment (P < .05). To evaluate the cost-effectiveness of personalized medicine based on predictive biomarkers, from the results of the ACROFAST study. Post hoc analysis from the ACROFAST study comparing cost-effectiveness of a protocol of medical treatment based on predictive biomarkers to fgSRLs (n = 32) vs standard…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
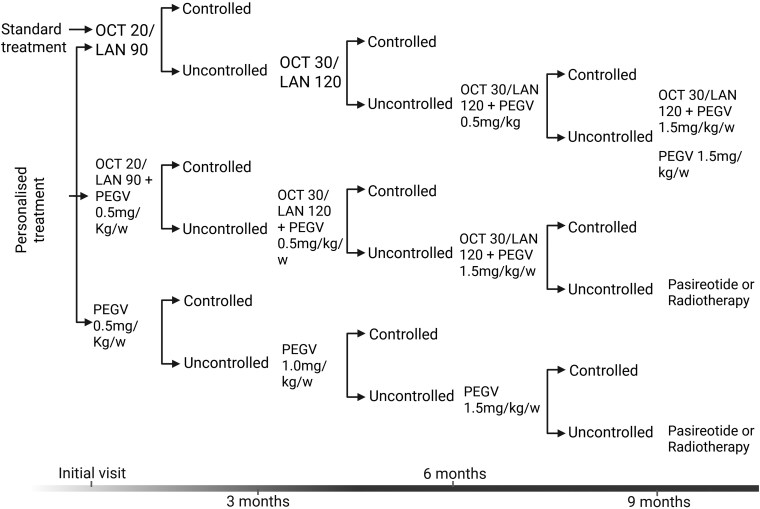 Figure 1
Figure 1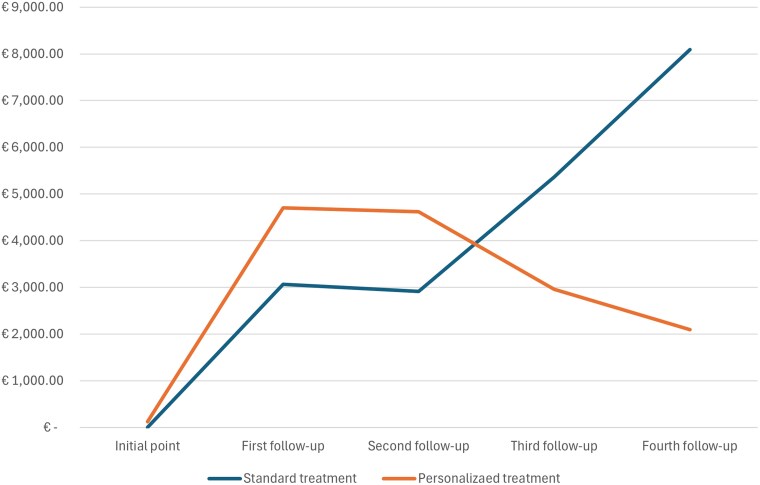 Figure 2
Figure 2| Standard treatment | Personalized treatment |
| |
|---|---|---|---|
| Cost per patient | |||
| Biomarkers study | |||
| Acute octreotide test | — | 8€ | |
| E-cadherin immunostaining | — | 15€ | |
| Medical visit | — | 98€ | |
| First follow-up | |||
| Medication | 2726€ | 4359€ | |
| Medical visit | 98€ | 98€ | |
| Blood analyses (hematology, biochemistry, and hormones) | 18€ | 18€ | |
| MRI | 226€ | 226€ | |
| Second follow-up | |||
| Medication | 3544€ | 7107€ | |
| Medical visit | 98€ | 98€ | |
| Blood analyses (hematology, biochemistry, and hormones) | 18€ | 18€ | |
| MRI | 226€ | 226€ | |
| Third follow-up | |||
| Medication | 9782€ | 9191€ | |
| Medical visit | 98€ | 98€ | |
| Blood analyses (hematology, biochemistry, and hormones) | 18€ | 18€ | |
| MRI | 226€ | 226€ | |
| Fourth follow-up | |||
| Medication | 15 846€ | 9191€ | |
| Medical visit | 98€ | 98€ | |
| Blood analyses (hematology, biochemistry, and hormones) | 18€ | 18€ | |
| MRI | 226€ | 226€ | |
| Percentage of patients achieving hormonal control | |||
| 3 months follow-up | 25% | 38% | .43 |
| 6 months follow-up | 47% | 69% | .14 |
| 9 months follow-up | 50% | 72% | .13 |
| 12 months follow-up | 50% | 78% | .04 |
| Standard treatment | Personalized treatment | Δ | |
|---|---|---|---|
| Average cost per patient | 19 420€ | 15 127€ | −4293€ |
| Percentage of patients achieving hormonal control | 50% | 78% | 28% |
| ICER | −15 263€ Per additional patient achieving hormonal control | ||
- —Instituto de Salud Carlos III10.13039/501100004587
- —European Union-ERDF
- —European Union -NextGenerationEU
- —M.P.-D
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPituitary Gland Disorders and Treatments · Cerebrovascular and genetic disorders · Autoimmune Neurological Disorders and Treatments
Acromegaly is a rare, chronic disorder characterized by excessive secretion of growth hormone (GH) and consequent elevation of insulin-like growth factor I (IGF1) levels, typically resulting from a pituitary adenoma [1-3]. Standard treatment modalities, including surgery, first-generation somatostatin receptor ligands (fgSRLs), GH receptor antagonists, and radiotherapy, aim to control hormone hypersecretion, alleviate symptoms, and prevent long-term complications [4, 5]. However, the heterogeneous nature of the disease and patients' variability in response to treatment highlight the limitations of a uniform therapeutic approach [6-9]. Personalized treatment protocols tailored to individual patient profiles have emerged as a promising alternative, aiming to optimize clinical outcomes while balancing economic considerations [6, 7, 10, 11].
The recently published ACROFAST study [12] introduced a novel personalized protocol for treating acromegaly, integrating patient-specific factors, such as tumor characteristics, biochemical response patterns, and comorbidities, to guide therapeutic decisions. Findings from ACROFAST indicated that this personalized approach may offer superior effectiveness by achieving IGF1 normalization in a shorter period of time. Moreover, the individualized approach could potentially reduce overtreatment, minimize adverse effects, and maximize patient satisfaction.
The present post hoc study of ACROFAST aims to evaluate the superiority of the personalized treatment protocol over standard treatment for acromegaly by examining cost-effectiveness. Medical standard treatment protocols based on the first-line use of fgSRLs have historically provided insufficient biochemical control rates [13-15], inconsistent symptom management, and varying impacts on patients' daily lives. Therefore, they may consequently be associated with higher healthcare costs. In contrast, personalized protocols try to address these shortcomings by adjusting treatment intensity based on individual needs. This may enhance therapeutic efficiency as well as decrease the general costs of acromegaly treatment.
In this context, the ACROFAST study serves as a critical benchmark to change the paradigm in acromegaly management, offering insights into the clinical and economic benefits of personalization. This research aims to elucidate the potential advantages of personalized protocols in terms of cost-effectiveness, paving the way for its broader implementation in clinical practice with the ultimate aim to improve medical management of patients living with acromegaly.
Methods
Study design
The design of the ACROFAST study and their main results have been described previously [12]. In brief, this was a prospective, randomized clinical trial comparing a protocol based on predictive biomarkers of fgSRLs vs standard treatment, in 2 parallel arms in which 21 Spanish university hospitals participated comparing the effectiveness and time to control of 2 treatment protocols for 12 months. A total of 85 patients participated and 68 patients completed the study and were evaluated: 32 in the personalized arm and 36 in the control group, either before or after unsuccessful surgery. In the personalized protocol, patients were treated with fgSRLs as monotherapy, fgSRLs in combination with pegvisomant, or pegvisomant as monotherapy, depending on the results obtained in the short Acute Octreotide Test (sAOT), tumor T2 magnetic resonance imaging (MRI) signal, or immunostaining for E-cadherin (mouse monoclonal anti-E-cadherin antibody [RRID AB_397580] [Ventana, Tucson, Ariz., USA] purchased as a prediluted antibody, with a concentration of 0.314 μg/dL). Serum GH was measured at each center by different automated immunoassays, all calibrated against World Health Organization (WHO) International Standard 98/574: Immulite i2000, Siemens Healthineers (RRID:AB_2811291); Liason XL, Diasorin (RRID:AB_3099571); UniCel DxI 800 Access, Beckman Coulter (RRID:AB_2756876) and Cobas 8000, Roche Diagnostics (RRID:AB_2883974). To ensure consistency and comparability of GH measurements obtained from different immunoassays and centers, the results were harmonized as previously described [12]. Serum IGF1 concentrations were also measured in each center by immunoassays calibrated against WHO NISBC 2stIS 02/254: Liason XL, Diasorin (RRID: AB_2928957), Immulite i2000, Siemens Healthineers (RRID: AB_2922766) and ELISA Mediagnost (RRID: AB_2813791). IGF1 concentrations were evaluated as absolute concentrations, and they were calculated as IGF1 SD score (SDS) for outcomes assessment and inter-center comparability as previously described [12]. In the control group the medical treatment always started with fgSRLs, and the other drugs were included after demonstrating inadequate control with those previously used, according to clinical judgment based on the standard of care. The main variables included were the time to control in each group, analyzed with a Survival Analysis, and the proportion of controlled patients at each visit and at the end of the study.
The primary measure of the present study was the monthly and the total cost of therapy for each treatment arm (12 months of study period). The required doses of fgSRLs and pegvisomant for all participants were assessed, and the monthly treatment costs were calculated based on the average wholesale price (AWP) in Spain for each dosing regimen (Table 1). Since the fgSRL dose followed a specific escalation per protocol within each treatment arm, the dose was multiplied by its respective AWP. For pegvisomant, the mean ± SD dose required by all patients in each of the treatment arms was determined.
The study utilized a cost-effectiveness analysis (CEA) to compare a personalized treatment protocol vs standard medical care in patients with acromegaly. The comparison was made using a decision tree model from the perspective of the healthcare provider, considering a 1-year time horizon. The model specified dose escalation for each therapeutic modality as shown in Fig. 1.
Algorithm for treatment escalation in standard and personalized arms. OCT (octreotide), LAN (lanreotide), PEGV (pegvisomant). Doses of octreotide: 20 and 30 mg administered every 4 weeks. Doses of lanreotide: 90 and 120 mg administered every 4 weeks. Doses of pegvisomant were calculated according to the weight of each patient at a weekly dose of 0.5 mg, 1.0 and 1.5 mg/Kg/w.
The costs associated with each treatment alternative were estimated according to the costs in Spain in 2024. In terms of effectiveness, the proportion of controlled and uncontrolled patients at the end of the study period was compared. The control of the disease was defined when gender and age adjusted IGF1 levels achieved < 2.5 SDS [16]. The results were expressed in terms of incremental cost-effectiveness ratio (ICER). The analysis followed the standards established in the CHEERS (Consolidated Health Economic Evaluation Reporting Standards) guide [17].
In addition, the medium-term results were estimated, considering a time horizon of 12 months as minimum and 24 months as maximum from the beginning of the treatment; as the uncontrolled patients, mostly from the standard algorithm, required an escalation of treatment which was performed following standard clinical practice. This analysis included the calculation of the additional costs associated with an uncontrolled patient case per year, as well as a projection of the evolution of the proportion of patients controlled in this period following the behavioral model obtained in the study period of the first year of the ACROFAST data. To make this estimate, 2 scenarios were defined for each type of treatment:
Positive scenario: Assuming a 25% increase in the proportion of patients controlled with respect to the average observed in the first year of the study in each follow-up visit performed at 3 months interval.Negative scenario: Assuming a 25% decrease in the proportion of patients controlled with respect to the average observed in the first year of the study.
These projections allowed the sensitivity of the economic and effectiveness results to be evaluated in the face of possible variations in the evolution of patient control.
Cost data
The direct costs of both treatments were estimated, including drugs, scheduled and nonscheduled visits, tests, imaging procedures, and biochemical analyses carried out during the study period. The cost data was obtained from the institution's administrative databases and was measured in monetary units (€2024). A discount rate was not applied due to the 1-year time limit of the study.
The effectiveness values, represented by the proportion of patients achieving hormonal control monitored in each phase of treatment, were obtained from the results of the patients in the study sample.
Statistical analysis
The ACROFAST trial was designed with 80% power to detect a difference of 1 SD in the effectiveness between any 2 study arms (effect size = 1.0), using an independent samples t test with a 2-sided alpha level of 5%. Forty participants per arm were required to meet these parameters. Numerical variables were summarized using mean, median, SD, and range. Categorical variables were summarized as frequencies and percentages and compared across treatment arms using Fisher's exact test.
Costs across treatment arms were analyzed using analysis of variance (ANOVA) with Tukey post hoc tests and simultaneous 95% CIs. Mean total monthly costs were calculated and compared accordingly. The Tukey test was used to perform pairwise comparisons between group means while controlling for the risk of type I error (false positives) in the context of multiple comparisons. In the cost-effectiveness analysis, this test was applied for analyzing the costs across multiple treatment groups to identify which specific pairs of groups had statistically significant differences in their mean costs. A 2-sided significance level of 0.05 was applied throughout the analysis. Statistical computations were performed using the statistical program R version 4.4.0 (2024-06-14) for Windows, while figures were generated using BioRender.com.
Results
The ACROFAST study included a total of 85 patients. From these, 68 patients ended the study and were finally analyzed: 32 patients in the personalized protocol and 36 patients in the standard protocol. Results of the ACROFAST study showed that the probability of achieving hormonal control adjusted by age and sex in the personalized group was defined by a hazard ratio of 2.53 (CI 1.30-4.80). Survival analysis with the cumulative number of controlled patients is available in the results of the ACROFAST study [12]. At the end of the study period, personalized treatment achieved 25% of more controlled patients compared to standard treatment (78% vs 53%), which implied a 22% reduction in the average cost per patient with a personalized treatment compared to standard treatment (15 127€ vs 19 420€) (Table 1). Cumulative line graph of costs in controlled and uncontrolled patients is represented in Fig. 2.
Cumulative line graph of costs in standard and personalized protocol treatment.
Personalized treatment generated an initial additional cost due to the sAOT, the E-cadherin immunostaining in postsurgical patients, and the medical visit associated with the result evaluation for assigning the specific medical treatment, totaling a cost of 121€ per patient. The cost of the sAOT was 8€. It included the cost of the medication, the GH evaluation at baseline and at 2 hours, and the cost of the professional who performed the 2 blood extractions. We did not include the cost of the administration process, as it is not established within the healthcare system and it was not necessary to hire additional resources beyond those already available. It also implied a higher pharmacological cost in the first 2 controls (12 150€ vs 6955€) since a proportion of patients were treated with pegvisomant in monotherapy or in combination with fgSRLs in the personalized arm. However, these costs decreased in the final stages of treatment (19 067€ vs 26 311€, in the last 2 follow-up visits). In contrast, the costs of medication in the conventional treatment arm increased progressively over time, as more therapeutic changes were required in the uncontrolled patients. Furthermore, the personalized treatment achieved a higher percentage of patients with hormonal control from the first follow-up evaluation (38% vs 25%) which increased steadily compared to the standard treatment arm at the last control visit (78% vs 53%). This higher level of effectiveness from the early stages reduced the number of patients who progress to more expensive stages, thus contributing to a lower total cost per patient at the end of the study (Table 2).
Thus, the personalized treatment reduced costs by 4293€ per patient/year and increased the effectiveness of the treatment, with 25% of more patients achieving hormonal control in less time in the personalized arm. These results represented a reduction of 15 263€ per additional patient monitored with the personalized treatment compared to the standard treatment.
When a 24-month projection was performed, the results showed that, in the medium term, personalized treatment also remained more cost-effective compared to standard treatment, both in the optimistic and pessimistic scenarios.
In the optimistic scenario (25% increase in the proportion of controlled patients), the average cost per patient was lower with personalized treatment compared to standard care (16 887€ vs 51 890€), representing a saving of 35 003€ per patient. The proportion of controlled patients was 13% higher with personalized treatment (91% vs 78%). The ICER indicated that for each additional patient controlled with personalized treatment, a saving of 261 718€ was achieved compared to standard treatment per patient in a scenario of 2 years of treatment. In the worst-case scenario (25% reduction in the proportion of controlled patients), the average cost per patient was lower with personalized treatment compared to standard therapy (16 324€ vs 55 803€), representing a saving of 36 479€ per patient. The proportion of controlled patients was 18% higher with personalized treatment (87% vs 69%). The ICER indicated that for each additional patient controlled with personalized treatment, a saving of 219 577€ was achieved compared to standard treatment in a 2-year estimation.
Discussion
These results from the ACROFAST study demonstrate that personalized medical treatment in acromegaly is not only clinically effective but also cost-efficient compared to conventional treatment approaches. Our findings highlighted that the personalized treatment strategy, which guides therapeutic decisions based on predictive biomarkers, achieves normal IGF1 control more frequently and in a significantly shorter timeframe than the conventional trial-and-error approach. This approach was emphasized some years ago by Melmed supporting an integrative medicine–based clinical practice in which this acceleration of the disease control translated into reduced healthcare costs and improved patient outcomes [18].
The cost-effectiveness of personalized treatment in acromegaly stems from its ability to optimize drug selection and dosing from the outset with relatively low costs (121€ per patient) in comparison with other diseases that require genetic studies [19]. In this context, for an affordable cost, an individualized approach has the ability to minimize the need for iterative adjustments that are common in the assay-error methodology [4]. By achieving higher and faster biochemical normalization, patients spend less time under suboptimal disease control, which reduces the risks associated with prolonged exposure to elevated GH and IGF1 levels, such as cardiovascular complications and metabolic dysregulation [20]. The costs related to the biomarkers analysis as well as the differences among both groups would have been different if the study would have been performed in other country, as the costs applied in the Spanish national health services are substantially different compared to other European countries. In this context, in other countries with higher unitary costs, the differences would have been much higher. Thus, in a certain way, the ACROFAST study was designed under less favorable conditions for comparing costs with the standard treatment, which gives even more value to the results obtained.
Importantly, the cost savings observed in this study are independent of the clinical superiority of personalized treatment in achieving biochemical control. Even if the clinical outcomes would have been equivalent between personalized and standard approaches, the reduced time to normalization inherently decreases costs associated with additional consultations, laboratory tests, and adjustments in therapy. Furthermore, personalized medicine fosters patient-centered care, potentially improving adherence and satisfaction, which are critical for chronic disease management and reduces the risk of treatment failure [21, 22]. To sum up, the personalized approach promotes patient empowerment and engagement in their care. This empowerment is also valid for physicians, as the understanding of the disease at the individual level that the study of biomarkers provides goes against therapeutic inertia and encourages medical practitioners to treat the patient with an appropriate medication. From a healthcare systems perspective, the efficient allocation of resources toward therapies with high predictive success enhances the sustainability of acromegaly management.
These findings underline the importance of integrating personalized approaches in the treatment of acromegaly and potentially other endocrine disorders. The combination of higher precision in drug selection and faster achievement of therapeutic goals, makes personalized medicine a way to more efficient and effective healthcare delivery [23]. Future studies should explore its applicability in broader populations and evaluate its long-term economic and clinical benefits. Moreover, implementation studies should investigate how personalized protocols perform outside clinical trials—particularly in real-world, resource-variable settings [24]. From the standpoint of healthcare systems, the more efficient allocation of resources toward treatments with higher predictive success rates improves the sustainability of managing a chronic and costly condition like acromegaly. As healthcare systems shift toward value-based care models, personalized strategies like those in ACROFAST become increasingly attractive for long-term integration [25].
The control of acromegaly and the use of pegvisomant have been related to an improvement in the metabolic risk factors related to acromegaly. A better control of the disease could have carried better control of risk factors and potentially, fewer costs related to control them. It is a limitation of the study that we cannot answer as it was not the primary objective of the ACROFAST study. However, this will not affect the results obtained in favor of personalized treatment, and in any case, the costs will be lower. As other studies have done [26, 27], we focused the cost-effectiveness analysis on the direct costs of acromegaly without including the indirect costs or the costs related to other treatments different than those used for acromegaly. Regarding the 6 patients treated with pegvisomant on monotherapy, 2 of them presented diabetes and the value of HbA1c improved at the end of the follow-up from 7.8% and 8% to 7% and 7.1%. This could be related to the control of the disease but also to an intensification of diabetes treatment or lifestyle changes.
Our study did not include the use of pasireotide in either arm, because at the time of the study's design, this compound was not yet sufficiently incorporated into the therapeutic medical strategies for acromegaly in Spain, nor had predictor biomarkers been described at the beginning of the study. This would have introduced bias into the standard treatment, so it was ultimately not included in the study protocol. However, it will be included in the ACROFAST II study, which will begin in late 2025 and it was considered apart from the study protocol in cases where hormonal control had not been achieved, as indicated in Fig. 1. Our study compared the cost-effectiveness of a personalized approach vs a standard therapy with fixed first-line drugs, thus it was not a drug cost-effectiveness study. However, some studies dealing with cost-effectiveness of specific drugs have been performed. In this regard, pasireotide has been shown as most cost-effective treatment compared with pegvisomant in case of persistent acromegaly after surgery, with a savings balance of 9423.26€/person/year (P = .12), that reach the amount of 30 415.98€/person/year at high doses (P < .001) [26]. This approach aims to use the same medication for all patients, and is surely less beneficial than individualized medical treatment. For example, using fgSRLs for responder patients, pasireotide for those with specific favorable predictive biomarkers to that compound, and pegvisomant possibly combined with radiotherapy for nonresponder patients. Also, Bonert et al [27] showed that after fgSRLs failure, low-dose fgSRLs plus weekly pegvisomant represents a good option for achieving cost-effective, optimal biochemical control in patients with uncontrolled acromegaly requiring combination therapy. Future research should build on these findings by exploring the broader application of personalized medicine in endocrine and other chronic disorders with all the drugs available for clinical practice with clearly different mechanisms of action. Comparative studies will also evaluate long-term benefits, including survival, cost-effectiveness across healthcare systems in different countries, and the broader societal impact.
In conclusion, this post hoc analysis from the ACROFAST study highlights the transformative potential of personalized medicine in the management of acromegaly, offering not only significant clinical benefits that restore more patients to a hormonally controlled state more rapidly and effectively than standard approaches but also cost savings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Melmed S . Acromegaly. N Engl J Med. 1990;322(14):966‐977.2179724 10.1056/NEJM 199004053221405 · doi ↗ · pubmed ↗
- 2Giustina A, Barkhoudarian G, Beckers A, et al Multidisciplinary management of acromegaly: a consensus. Rev Endocr Metab Disord. 2020;21(4):667‐678.32914330 10.1007/s 11154-020-09588-z PMC 7942783 · doi ↗ · pubmed ↗
- 3Fleseriu M, Biller BMK, Freda PU, et al A pituitary society update to acromegaly management guidelines. Pituitary. 2021;24(1):1‐13.33079318 10.1007/s 11102-020-01091-7PMC 7864830 · doi ↗ · pubmed ↗
- 4Melmed S, Bronstein MD, Chanson P, et al A consensus statement on acromegaly therapeutic outcomes. Nat Rev Endocrinol. 2018;14(9):552‐561.30050156 10.1038/s 41574-018-0058-5PMC 7136157 · doi ↗ · pubmed ↗
- 5Katznelson L, Laws ER, Melmed S, et al Acromegaly: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(11):3933‐3951.25356808 10.1210/jc.2014-2700 · doi ↗ · pubmed ↗
- 6Puig Domingo M . Treatment of acromegaly in the era of personalized and predictive medicine. Clin Endocrinol (Oxf). 2015;83(1):3‐14.25640882 10.1111/cen.12731 · doi ↗ · pubmed ↗
- 7Puig-Domingo M, Marazuela M. Precision medicine in the treatment of acromegaly. Minerva Endocrinol. 2019;44(2):169‐175.30531695 10.23736/S 0391-1977.18.02937-1 · doi ↗ · pubmed ↗
- 8Puig-Domingo M, Gil J, Sampedro-Nuñez M, et al Molecular profiling for acromegaly treatment: a validation study. Endocr Relat Cancer. 2020;27(6):375‐389.32302973 10.1530/ERC-18-0565 · doi ↗ · pubmed ↗