Mental health disorders among people living with human immunodeficiency virus on antiretroviral therapy in Benin: the overlooked role of sleep quality
Boni Maxime Ale, Calixte Oswald Assogba, Eugénie Dansou, Olushina Ayo Junior Ale, Oswald Lionel Koutangni, Adébiyi Raphaël K Alogou, Simon Giscard Akpi, Kenneth Geovania Dèlonou Damassoh, Eric Youm, Nelly Njeri Wakaba, Houénoudé Mickaël Arnaud Assogba, Kouessi Anthelme Agbodande

TL;DR
This study in Benin finds that poor sleep quality is strongly linked to depression and anxiety in people living with HIV on antiretroviral therapy.
Contribution
The study highlights the previously overlooked role of sleep quality in mental health outcomes among HIV patients in Benin.
Findings
Depression and anxiety were present in 20.8% and 12.8% of participants, respectively.
Poor sleep quality was independently associated with higher odds of depression and anxiety.
Good sleep quality was protective against both mental health disorders.
Abstract
Depression and anxiety are common comorbidities among people living with HIV (PLHIV) and may be influenced by sleep quality; evidence from Benin remains limited. We assessed the prevalence of depression and anxiety among PLHIV on antiretroviral therapy (ART) and evaluated their association with sleep quality. We conducted a hospital-based cross-sectional study at Benin’s National Teaching Hospital from December 2023 to February 2024. Adults on ART ≥ 6 months were randomly sampled from the clinic registry. Validated tools were used: Patient Health Questionnaire-9 and Generalized Anxiety Disorder-7, moderate-or-worse threshold ≥ 10; Pittsburgh Sleep Quality Index, poor sleep > 5. Multivariable logistic regression identified factors independently associated with depression and anxiety. Among 312 participants (68.3% female; mean age 44.3 ± 12.3 years), the prevalence of depression and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
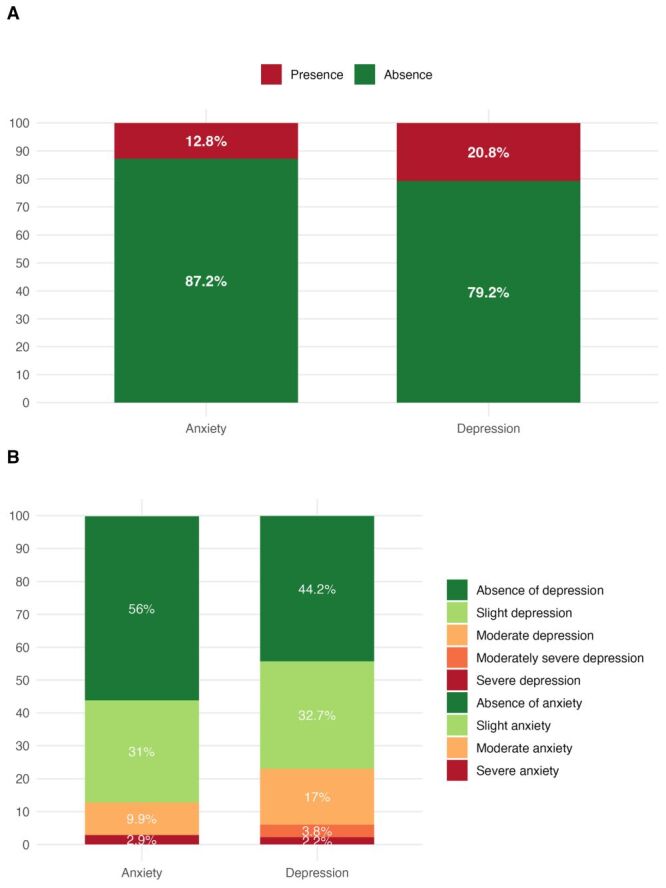 Figure 1
Figure 1| Characteristics | n | % |
|---|---|---|
| Mean age | 44.3 | 12.3 |
| Age group |
|
|
|
| 152 | 48.7 |
|
| 160 | 51.3 |
| Sex |
|
|
|
| 99 | 31.7 |
|
| 213 | 68.3 |
| Level of education |
|
|
|
| 84 | 26.9 |
|
| 80 | 25.6 |
|
| 93 | 29.8 |
|
| 55 | 17.6 |
| Marital status |
|
|
|
| 124 | 39.7 |
|
| 188 | 60.3 |
| Employment status |
|
|
|
| 59 | 18.9 |
|
| 253 | 81.1 |
| Tobacco consumption |
|
|
|
| 287 | 92.0 |
|
| 25 | 8.0 |
| Alcohol consumption |
|
|
|
| 180 | 57.7 |
|
| 132 | 42.3 |
| Time since diagnosis |
|
|
|
| 95 | 30.4 |
|
| 217 | 69.6 |
| Time since initiation of ART |
|
|
|
| 95 | 30.4 |
|
| 217 | 69.6 |
| ART regimen |
|
|
|
| 4 | 1.3 |
|
| 1 | 0.3 |
|
| 2 | 0.6 |
|
| 1 | 0.3 |
|
| 271 | 86.9 |
|
| 31 | 9.9 |
|
| 2 | 0.6 |
| HIV type |
|
|
|
| 308 | 98.7 |
|
| 3 | 1.0 |
|
| 1 | 0.3 |
| Viral load (copies) |
|
|
|
| 242 | 77.6 |
|
| 46 | 14.7 |
|
| 3 | 1.0 |
|
| 21 | 6.7 |
| WHO Stage |
|
|
|
| 57 | 18.3 |
|
| 61 | 19.6 |
|
| 152 | 48.7 |
|
| 42 | 13.5 |
| Hypertension |
|
|
|
| 247 | 79.2 |
|
| 65 | 20.8 |
| Body mass index |
|
|
|
| 28 | 9.0 |
|
| 140 | 44.9 |
|
| 77 | 24.7 |
|
| 67 | 21.5 |
| Regular physical activity |
|
|
|
| 41 | 13.1 |
|
| 271 | 86.9 |
| Sleep quality |
|
|
|
| 178 | 57.1 |
|
| 134 | 42.9 |
| Characteristics | Unadjusted model | Adjusted model | |||||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
| Sleep quality | 312 |
|
|
| <0.001 |
| <0.001 |
|
|
| 128 (51.8) | 50 (76.9) | Ref |
| Ref |
|
|
|
| 119 (48.2) | 15 (23.1) | 0.3 (0.2–0.6) |
| 0.3 (0.2–0.6) |
|
| Age group | 312 |
|
|
| 0.710 |
|
|
|
|
| 119 (48.2) | 33 (50.8) | Ref |
|
|
|
|
|
| 128 (51.8) | 32 (49.2) | 0.9 (0.5–1.6) |
|
|
|
| Sex | 312 |
|
|
| 0.278 |
|
|
|
|
| 82 (33.2) | 17 (26.2) | Ref |
|
|
|
|
|
| 165 (66.8) | 48 (73.8) | 1.4 (0.8–2.7) |
|
|
|
| Level of education | 312 |
|
|
| 0.947 |
|
|
|
|
| 68 (27.5) | 16 (24.6) | Ref |
|
|
|
|
|
| 63 (25.5) | 17 (26.2) | 1.1 (0.5–2.5) | 0.725 |
|
|
|
|
| 72 (29.1) | 21 (32.3) | 1.2 (0.6–2.6) | 0.564 |
|
|
|
|
| 44 (17.8) | 11 (16.9) | 1.1 (0.4–2.5) | 0.890 |
|
|
| Marital status | 312 |
|
|
| 0.141 |
| 0.087 |
|
|
| 93 (37.7) | 31 (47.7) | Ref |
| Ref |
|
|
|
| 154 (62.3) | 34 (52.3) | 0.7 (0.4–1.2) |
| 0.6 (0.3–0.8) |
|
| Employment status | 312 |
|
|
| 0.543 |
|
|
|
|
| 45 (18.2) | 14 (21.5) | Ref |
|
|
|
|
|
| 202 (81.8) | 51 (78.5) | 0.8 (0.4–1.6) |
|
|
|
| Tobacco consumption | 312 |
|
|
| 0.915 |
|
|
|
|
| 227 (91.9) | 60 (92.3) | Ref |
|
|
|
|
|
| 20 (8.1) | 5 (7.7) | 0.9 (0.3–2.4) |
|
|
|
| Alcohol consumption | 312 |
|
|
| 0.672 |
|
|
|
|
| 141 (57.1) | 39 (60.0) | Ref |
|
|
|
|
|
| 106 (42.9) | 26 (40.0) | 0.9 (0.5–1.5) |
|
|
|
| Use of recreational substances | 312 |
|
|
| 0.111 |
| 0.169 |
|
|
| 246 (99.6) | 63 (96.9) | Ref |
| Ref |
|
|
|
| 1 (0.4) | 2 (3.1) | 7.8 (0.7–169.6) |
| 5.5 (0.5–121.7) |
|
| Regular physical activity | 312 |
|
|
| 0.547 |
|
|
|
|
| 31 (12.6) | 10 (15.4) | Ref |
|
|
|
|
|
| 216 (87.4) | 55 (84.6) | 0.8 (0.4–1.8) |
|
|
|
| Hypertension | 312 |
|
|
| 0.597 |
|
|
|
|
| 194 (78.5) | 53 (81.5) | Ref |
|
|
|
|
|
| 53 (21.5) | 12 (18.5) | 0.8 (0.4–1.6) |
|
|
|
| History of cardiovascular events | 312 |
|
|
| 0.070 |
|
|
|
|
| 236 (95.5) | 58 (89.2) | Ref |
|
|
|
|
|
| 11 (4.5) | 7 (10.8) | 2.6 (0.9–6.9) |
|
|
|
| Body mass index | 312 |
|
|
| 0.664 |
|
|
|
|
| 23 (9.3) | 5 (7.7) | Ref |
|
|
|
|
|
| 107 (43.3) | 33 (50.8) | 1.4 (0.5–4.5) | 0.511 |
|
|
|
|
| 61 (24.7) | 16 (24.6) | 1.2 (0.4–4.0) | 0.741 |
|
|
|
|
| 56 (22.7) | 11 (16.9) | 0.9 (0.3–3.1) | 0.864 |
|
|
| Duration on ART | 312 |
|
|
| 0.714 |
|
|
|
|
| 74 (30.0) | 21 (32.3) | Ref |
|
|
|
|
|
| 173 (70.0) | 44 (67.7) | 0.9 (0.5–1.6) |
|
|
|
| Type of HIV | 312 |
|
|
| 0.193 |
|
|
|
|
| 245 (99.2) | 63 (96.9) | Ref |
|
|
|
|
|
| 1 (0.4) | 2 (3.1) | 7.8 (0.7–168.9) | 0.096 |
|
|
|
|
| 1 (0.4) | 0 (0.0) | 0.0 | 0.988 |
|
|
| WHO stage of HIV | 312 |
|
|
| 0.038 |
|
|
|
|
| 47 (19.0) | 10 (15.4) | Ref |
|
|
|
|
|
| 55 (22.3) | 6 (9.2) | 0.5 (0.2–1.5) | 0.227 |
|
|
|
|
| 111 (44.9) | 41 (63.1) | 1.7 (0.8–3.9) | 0.161 |
|
|
|
| 34 (13.8) | 8 (12.3) | 1.1 (0.4–3.1) | 0.848 | |||
| Characteristics | Unadjusted model | Adjusted model | |||||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
| Sleep Quality | 312 |
|
|
| 0.014 |
| 0.032 |
|
|
| 148 (54.4) | 30 (75.0) | Ref |
| Ref |
|
|
|
| 124 (45.6) | 10 (25.0) | 0.4 (0.2–0.8) |
| 0.4 (0.2–0.9) |
|
| Age group | 312 |
|
|
| 0.028 |
| 0.045 |
|
|
| 139 (51.1) | 13 (32.5) | Ref |
| Ref |
|
|
|
| 133 (48.9) | 27 (67.5) | 2.2 (1.1–4.5) |
| 2.1 (1.0–4.5) |
|
| Sex | 312 |
|
|
| 0.538 |
| 0.666 |
|
|
| 88 (32.4) | 11 (27.5) | Ref |
| Ref |
|
|
|
| 184 (67.6) | 29 (72.5) | 1.3 (0.6–2.7) |
| 1.2 (0.6–2.7) |
|
| Level of education | 312 |
|
|
| 0.066 |
|
|
|
|
| 68 (25.0) | 16 (40.0) | Ref |
|
|
|
|
|
| 73 (26.8) | 7 (17.5) | 0.4 (0.1–1.0) | 0.063 |
|
|
|
|
| 79 (29.0) | 14 (35.0) | 0.8 (0.3–1.7) | 0.480 |
|
|
|
|
| 52 (19.1) | 3 (7.5) | 0.2 (0.1–0.8) | 0.032 |
|
|
| Marital status | 312 |
|
|
| 0.511 |
|
|
|
|
| 110 (40.4) | 14 (35.0) | Ref |
|
|
|
|
|
| 162 (59.6) | 26 (65.0) | 1.3 (0.6–2.6) |
|
|
|
| Employment status | 312 |
|
|
| 0.499 |
|
|
|
|
| 53 (19.5) | 6 (15.0) | Ref |
|
|
|
|
|
| 219 (80.5) | 34 (85.0) | 1.4 (0.6–3.8) |
|
|
|
| Tobacco consumption | 312 |
|
|
| 0.754 |
|
|
|
|
| 249 (91.5) | 38 (95.0) | Ref |
|
|
|
|
|
| 23 (8.5) | 2 (5.0) | 0.6 (0.1–2.0) |
|
|
|
| Alcohol consumption | 312 |
|
|
| 0.979 |
|
|
|
|
| 157 (57.7) | 23 (57.5) | Ref |
|
|
|
|
|
| 115 (42.3) | 17 (42.5) | 1.0 (0.5–2.0) |
|
|
|
| Use of recreational substances | 312 |
|
|
| 0.044 |
| 0.113 |
|
|
| 271 (99.6) | 38 (95.0) | Ref |
| Ref |
|
|
|
| 1 (0.4) | 2 (5.0) | 14.3 (1.3–311.3) |
| 7.3 (0.7–162.9) |
|
| Regular physical activity | 312 |
|
|
| 0.258 |
|
|
|
|
| 38 (14.0) | 3 (7.5) | Ref |
|
|
|
|
|
| 234 (86.0) | 37 (92.5) | 2.0 (0.7–8.6) |
|
|
|
| Hypertension | 312 |
|
|
| 0.889 |
|
|
|
|
| 215 (79.0) | 32 (80.0) | Ref |
|
|
|
|
|
| 57 (21.0) | 8 (20.0) | 0.9 (0.4–2.1) |
|
|
|
| History of cardiovascular events | 312 |
|
|
| 0.487 |
|
|
|
|
| 255 (93.8) | 39 (97.5) | Ref |
|
|
|
|
|
| 17 (6.3) | 1 (2.5) | 0.4 (0.0–2.0) |
|
|
|
| Body mass index | 312 |
|
|
| 0.002 |
|
|
|
|
| 26 (9.6) | 2 (5.0) | Ref |
|
|
|
|
|
| 115 (42.3) | 25 (62.5) | 2.8 (0.8–18.2) | 0.175 |
|
|
|
|
| 65 (23.9) | 12 (30.0) | 2.4 (0.6–16.1) | 0.273 |
|
|
|
|
| 66 (24.3) | 1 (2.5) | 0.2 (0.0–2.1) | 0.192 |
|
|
| Duration on ART | 312 |
|
|
| 0.242 |
|
|
|
|
| 86 (31.6) | 9 (22.5) | Ref |
|
|
|
|
|
| 186 (68.4) | 31 (77.5) | 1.6 (0.8–3.7) |
|
|
|
| Type of HIV | 312 |
|
|
| >0.999 |
|
|
|
|
| 268 (98.5) | 40 (100.0) | Ref |
|
|
|
|
|
| 3 (1.1) | 0 (0.0) | 0.0 | 0.992 |
|
|
|
|
| 1 (0.4) | 0 (0.0) | 0.0 | 0.995 |
|
|
| WHO stage of HIV | 312 |
|
|
| 0.095 |
|
|
|
|
| 53 (19.5) | 4 (10.0) | Ref |
|
|
|
|
|
| 50 (18.4) | 11 (27.5) | 2.9 (0.9–11.1) | 0.083 |
|
|
|
|
| 129 (47.4) | 23 (57.5) | 2.4 (0.9–8.3) | 0.129 |
|
|
|
| 40 (14.7) | 2 (5.0) | 0.7 (0.1–3.6) | 0.644 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · HIV/AIDS Research and Interventions · Family Caregiving in Mental Illness
HIV/AIDS affects 38.4 million people living with HIV (PLHIV) worldwide as of 2021. Notably, two-thirds of this population reside in sub-Saharan Africa, where the disease burden is disproportionately high [1]. Over the past few decades, significant advancements in the management of HIV/AIDS, particularly through the development of potent antiretroviral therapy (ART), have transformed HIV infection from an acute, life-threatening disease into a chronic condition [2–5]. While this transformation has improved life expectancy and reduced morbidity, it has also redefined the clinical and public health challenges associated with HIV, particularly in the domain of mental health comorbidities. Among these, anxiety and depression are notably prevalent, exerting profound effects on treatment adherence, disease progression, and overall quality of life among PLHIV [6].
A growing body of evidence highlights the high prevalence of anxiety and depression among individuals living with HIV, with estimates varying across different settings. For instance, studies indicate a prevalence ranging from 13.8% in Guinea to 79.0% in China, underscoring both geographic and systemic variations in mental health burden and care accessibility [2,6–8]. These psychiatric conditions are often underdiagnosed and undertreated, particularly in resource-limited settings such as sub-Saharan Africa, where mental health services are scarce [9,10]. The lack of adequate screening and treatment for psychiatric comorbidities among PLHIV not only exacerbates individual suffering but also contributes to poorer health outcomes, increasing the risk of treatment non-adherence, disease progression, and even mortality [9,11].
Several sociodemographic and clinical factors have been identified as significant determinants of anxiety and depression among PLHIV. Socioeconomic disparities, particularly low levels of education and financial instability, have been strongly linked to increased psychological distress in this population [11]. Additionally, the female sex has been associated with a higher likelihood of developing anxiety and depression. Furthermore, poor sleep quality has been recognised as a crucial factor contributing to the onset and exacerbation of psychiatric symptoms, with studies demonstrating a strong correlation between sleep disturbances and the severity of depression and anxiety in PLHIV [11]. Biologically, sleep disturbances trigger dysregulation of the hypothalamic-pituitary-adrenal axis and increase pro-inflammatory cytokine levels (e.g. interleukin-6, tumour necrosis factor alpha), which are strongly linked to the onset and persistence of depression and anxiety [12,13]. Sleep impairment also disrupts circadian regulation of mood and cognitive processes, thereby exacerbating vulnerability to psychiatric symptoms [14]. In the context of HIV, poor sleep can further undermine adherence to ART, as fatigue and low motivation reduce consistent medication intake, which in turn worsens virological outcomes and heightens psychological distress [15]. These interrelated biological and behavioural pathways underscore the plausibility of poor sleep acting both as a contributor to and a consequence of mental health disorders among PLHIV.
The implications of untreated mental health disorders in PLHIV extend beyond the individual level, affecting treatment adherence and overall public health outcomes. Depression and anxiety have been shown to significantly reduce adherence to ART, which is crucial for achieving and maintaining viral suppression [2,16–18]. Individuals experiencing mental health distress may struggle with motivation, forgetfulness, and feelings of hopelessness, leading to suboptimal medication adherence and higher risks of virological failure [17,19]. Additionally, the presence of psychiatric disorders is associated with an increased risk of suicidality, further compounding the health risks for affected individuals [2]. Despite the high burden of anxiety and depression among PLHIV, access to mental health screening and treatment remains alarmingly low. This underscores an urgent need for policies and interventions aimed at enhancing mental health integration within HIV care programmes [20]. In Benin, for instance, there is no report assessing the association of mental health and sleep disorders. Considering these challenges, we hypothesised that poor sleep quality is independently associated with depression and anxiety in PLHIV after adjusting for sociodemographic and clinical factors. Thus, our study seeks to assess the prevalence of anxiety and depression and associated factors, including the impact of poor sleep, among PLHIV receiving ART, to inform the integration of sleep and mental health screening into HIV care in Benin.
METHODS
Study setting and design
This was a hospital-based cross-sectional study assessing the prevalence of anxiety and depression and factors associated, carried out at Benin’s National Teaching Hospital Hubert Koutoukou Maga (CNHU/HKM) conducted between December 2023–February 2024.
Study population
The study population was composed of people living with HIV on antiretroviral treatment followed up in the outpatient clinic of Benin’s National Teaching Hospital.
Inclusion and exclusion criteria
We included patients aged over 18 and on ART for more than six months. Patients with severe cognitive disorders preventing them from responding to questionnaires, those undergoing psychiatric treatment for other chronic psychiatric conditions, pregnant women, or women in the postpartum period were excluded.
Sample size and sampling techniques
The sample size was estimated using Schwarz’s formula, based on 13.8% prevalence of anxiety, 16.9% prevalence of depression [11], a 5% standard error margin and with a 95% confidence interval (CI). To account for potential non-respondents, an additional 10% was added, which led to the total minimal sample size of 203 for anxiety and 238 for depression. Participants were selected through a simple random sampling method using a random generator in Excel applied to the hospital’s database of actively followed-up patients.
Study variables
The primary outcomes were anxiety and depression, and the key independent variable was sleep quality (poor or good quality). The other independent variables were sociodemographic (age, sex, level of education, marital status, professional status), medical (comorbidities, hypertension, cardiovascular diseases), and HIV-associated factors (ART treatment duration, viral load, treatment protocol).
Operational definition
Anxiety was defined using the Generalized Anxiety Disorder-7 (GAD-7) scale. We categorised anxiety symptoms as none/minimal (0–4), mild (5–9), moderate (10–14), and severe (15–21), with primary analyses using a ‘moderate-or-worse’ threshold of ≥ 10. This classification follows established guidelines for assessing anxiety disorders in clinical and research settings [10].
Depression was defined according to the Patient Health Questionnaire-9 (PHQ-9) scale. We categorised depressive symptoms as none/minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27), with primary analyses using a ‘moderate-or-worse’ threshold of ≥10 [21]. This threshold is widely used for detecting depressive symptoms in PLHIV.
Quality of sleep was evaluated using the Pittsburgh Sleep Quality Index (PSQI), with a global score > 5 indicating poor sleep quality [22].
Antiretroviral therapy duration was defined as the time since the first prescription of ART, based on the patient's medical records.
Alcohol consumption was defined based on patient declarations, with current alcohol use referring to any alcohol consumption in the past month.
Smoking status was classified as current smoker (any cigarette use in the past month), former smoker (stopped smoking for more than a month), or never smoker based on self-reported history.
Education level was classified as no formal education, primary, secondary, or higher.
Employment status was classified as employed or unemployed.
Hypertension was defined according to the European Society of Hypertension guidelines as a systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg [23], or/and the current use of antihypertensive medication as documented in medical records.
Body mass index (BMI) was used to classify physical status as follows: underweight: BMI ≤ 18.5 kg/m^2^, normal weight: BMI between 18.5–24.9 kg/m^2^, overweight: BMI between 25.0–29.9 kg/m^2^, obesity: BMI > 30 kg/m^2^.
Comorbidities such as diabetes and cardiovascular diseases were documented based on patients' medical records and self-reported diagnoses confirmed by health care providers.
Data collection
Data quality control and collection procedure
Eligible participants were contacted via phone by hospital staff, who provided a detailed explanation of the study’s objectives and procedures. Patients who agreed to participate were scheduled for an appointment at the clinic, where they provided informed consent before data collection commenced. incorporating validated evaluation tools such as the PSQI, STOP-BANG Questionnaire, PHQ-9, and GAD-7. The data were sourced from multiple channels, including patient self-reports, medical records, and physical measurements. Trained staff conducted face-to-face interviews with written informed consent.
Data processing and analyses
To ensure high data quality, the research team underwent comprehensive training before data collection. The data collection process was digitised using the Open Data Kit software on smartphones, enabling real-time monitoring for completeness and accuracy. Following the collection, data were consolidated, reviewed, and validated for internal consistency. The collected data were analysed using R software version 4.4.3 (Vienna, Austria). The analysis comprised descriptive statistics, with results presented as means, standard deviations, and percentages; bivariate analysis, employing the χ^2^ test for categorical variables and the Wilcoxon test for continuous variables, to examine associations between independent and dependent variables, and multivariate analysis, conducted through logistic regression, to identify factors independently associated with anxiety and depression among PLHIV on ART.
Ethics approval and consent to participate
The study sought the approval of the Health Research Ethics Committee of the Cotonou Faculty of Health Sciences and the Local Biomedical Research Ethics Committee of the University of Parakou. In addition, the study sought the authorisation of the administration of the CNHU-HKM of Cotonou on the one hand and of the National Reference Center for Research and Care for HIV (CNRRPEC) on the other hand to allow data collection in the institution.
Written informed consent was obtained from all the subjects before the study. The study was also conducted following the Helsinki Declaration of research involving human subjects.
RESULTS
A total of 312 PLHIV on ART were included; 213 (68.3%) were female, and 160 (51.3%) were aged ≥44 years. Educational attainment was low for many participants (no formal education: n = 84, 26.9%). Most were employed (n = 253, 81.1%), 25 (8.0%) reported current tobacco use, 132 (42.3%) reported alcohol use, and 271 (86.9%) engaged in regular physical activity. Hypertension affected 91 participants (29.2%) and cardiovascular disease 18 (5.8%). By BMI, 28 (9.0%) were underweight, 140 (44.9%) normal weight, 77 (24.7%) overweight, and 67 (21.5%) obese. Antiretroviral therapy duration exceeded five years for 190 participants (60.9%); 271 (86.9%) were on Dolutegravir/lamivudine/tenofovir (TDF-3TC-DTG) and 31 (9.9%) on Efavirenz/lamivudine/tenofovir (EFV/3TC/TDF). Nearly all had HIV-1 (n = 308, 98.7%).
World Health Organization clinical stage distribution was (out of 312 participants):
• Stage 1: 57 (18.3%)
• Stage 2: 61 (19.6%)
• Stage 3: 152 (48.7%)
• Stage 4: 42 (13.5%).
Virologic failure was uncommon (n = 8, 2.6%), as were clinical (n = 5, 1.6%) and immunologic (n = 1, 0.3%) failures. Poor sleep quality (PSQI>5) affected 178 participants (57.1%) (Table 1).
Mental health burden was substantial: 65 participants (20.8%) met criteria for depression. Symptom severity was distributed as follows: slight (n = 102, 32.7%), moderate (n = 53, 17.0%), moderately severe (n = 12, 3.8%), and severe (n = 7, 2.2%). Anxiety criteria were met by 40 participants (n = 12.8%); severity levels included slight symptoms in 98 (31.0%), moderate in 31 (9.9%), and severe in 9 (2.9%) (Figure 1, Panels A–B). Poor sleep quality (PSQI>5) was common overall (n/N = 178/312, 57.1%) and more frequent among those with depression (n/N = 50/65, 76.9%) vs. those without (n/N = 128/247, 51.8%), and among those with anxiety (n/N = 30/40, 75.0%) vs. those without (n/N = 148/272, 54.4%). In multivariable models, good sleep quality remained independently protective for both depression (aOR = 0.3; 95% CI = 0.2–0.6, P < 0.001) and anxiety (aOR = 0.4; 95% CI = 0.2–0.9, P = 0.032), implying roughly 3-fold higher odds of depression (Table 2) and 2.5-fold higher odds of anxiety with poor sleep (Table 3). For anxiety, age ≥44 years was also associated with higher odds (aOR = 2.1; 95% CI = 1.0–4.5, P = 0.045). The association between being married and lower odds of depression (aOR = 0.6; 95% CI = 0.3–0.8) was observed, though the P-value approached but did not reach conventional significance (P = 0.087). Other sociodemographic and clinical variables were not independently associated after adjustment. We did not analyse sleep or mental-health outcomes by ART regimen because too few participants received regimens other than TDF-3TC-DTG to permit meaningful inference.
Prevalence of anxiety and depression in people living with HIV in Benin’s National Teaching Hospital, 2024. Panel A. Overall prevalence of anxiety and depression. Panel B. Distribution of anxiety and depression severity levels among participants.
DISCUSSION
This study aimed to assess the prevalence of depression and anxiety and their association with sleep quality among PLHIV on ART in Benin. Out of 312 PLHIV at CNHU-HKM, 65 (20.8%) had depression (mild: n = 53, 17.0%; severe: n = 7, 2.2%) and 40 (12.8%) had anxiety (mild: n = 31, 9.9%; severe: n = 9, 2.9%), underscoring a meaningful mental-health burden. In multivariable analyses, good sleep quality was protective for both outcomes (depression aOR = 0.3; 95% CI = 0.2–0.6; anxiety aOR = 0.4; 95% CI = 0.2–0.9), implying that poor sleep was associated with roughly 3-fold (depression) and 2.5-fold (anxiety) higher odds. Age ≥44 years increased the odds of anxiety (aOR = 2.1; 95% CI = 1.0–4.5), marriage showed a protective trend for depression (aOR = 0.6; P = 0.087), and sex was not independently associated after adjustment.
The prevalence of depression observed in our study (20.8%) surpassed previously reported rates in Nigeria (14.3%) [24]. This highlights the urgent need for targeted interventions to address mental health issues in PLHIV, particularly in sub-Saharan Africa, where access to psychological care remains limited. While certain studies have reported even higher depression rates in France (28.1%) and China (79%), the small sample size in these investigations limits generalisability [2,8]. These findings reinforce the notion that depression prevalence varies significantly across different populations, depending on cultural, socioeconomic, and health care accessibility factors. Nonetheless, the consistently high prevalence of depression among PLHIV across studies is a major cause for concern [20].
Similarly, the prevalence of anxiety (12.8%) in our study is notably high as previously reported in West Africa. For instance, Camara et al. (2020) reported anxiety prevalence (13.8%) in Guinea, while Tesfaw et al. documented an even higher rate (32.4%) [7,25]. Despite these variations, our study confirms that PLHIV are disproportionately affected by mental health disorders, with higher anxiety rates than those observed in the general population [26]. These rates may be higher because the mental-health system is thin; the country reports 0.43 mental-health workers per 100 000 and sub-optimal integration of mental health into primary care; limiting detection and treatment in ART clinics [27]. Socioeconomic stressors are substantial and food insecurity is linked to worse mental health among PLHIV [28]. HIV-related stigma documented in the region deters help-seeking, while routine mental-health screening is not yet standard in many HIV programmes.
Our study population had a strong female predominance, which aligns with findings from similar studies conducted in Benin, Nigeria, Rwanda, and Guinea [6,7,24]. However, this trend contrasts with observations in France, where male predominance was reported [2]. This sex disparity in African countries may be attributed to increased HIV screening among women during maternity care programmes, leading to a higher diagnosis rate in females compared to males. Despite the absence of an independent association between sex and mental health disorders in our study, it is well documented that women are biologically and socially more vulnerable to developing anxiety and depression. For instance, Turk et al. highlighted hormonal differences as key contributors to this disparity [29].
Hypertension was observed in 29.2% of our study population, a prevalence comparable to findings from prior studies in Benin and Guinea [7,30,31]. However, this rate is slightly lower than that reported by Feuillet et al. in France, likely reflecting differences in lifestyle, diet, and health care access [2]. Furthermore, obesity prevalence in our cohort was lower than reported in PLHIV in France, which may be attributable to nutritional and environmental variations. These findings suggest that noncommunicable diseases such as hypertension and obesity are increasingly becoming a concern among PLHIV, emphasising the importance of comprehensive HIV care that includes metabolic and cardiovascular health monitoring.
In adjusted analyses, age over 44 years was associated with higher odds of anxiety (aOR = 2.1; 95% CI = 1.0–4.5). This age effect is biologically and contextually plausible: chronic immune activation and inflammation persist despite ART and have been linked to neuroinflammation and affective symptoms in PLHIV, providing a substrate for anxiety in later life [32,33]. Ageing is also accompanied by lighter, more fragmented sleep and a greater burden of sleep disorders, which show robust associations with anxiety; moreover, insomnia itself predicts subsequent anxiety disorders [34]. Among women, the menopausal transition adds sleep disruption and mood symptoms, with similar patterns reported in cohorts of women living with HIV [35].
Beyond the high burden observed, our data show a robust, independent association between sleep quality and mental health: good sleep quality was protective for both depression (aOR = 0.3; 95% CI = 0.2–0.6) and anxiety (aOR = 0.4; 95% CI = 0.2–0.9), implying roughly 3-fold higher odds of depression and about 2.5-fold higher odds of anxiety among participants with poor sleep; this pattern was reflected in prevalence contrasts and persisted after adjustment for sociodemographic and clinical covariates. These findings are biologically and behaviourally plausible: sleep disturbance activates inflammatory pathways and hypothalamic-pituitary-adrenal (HPA) axis dysregulation linked to depressive and anxious symptomatology [12–14], and poorer sleep is associated with antiretroviral non-adherence that can worsen virologic control and psychological distress [15]. HIV-specific evidence also connects sleep impairment with heightened anxiety and depressive symptoms, particularly among women living with HIV [11]. Nonetheless, the cross-sectional design precludes causal inference, and unmeasured factors such as pain/neuropathy, stigma, and food insecurity may contribute. Antiretroviral therapy regimen effects could not be assessed given the predominance of TDF-3TC-DTG. Taken together, our results support routine PSQI-based screening and brief sleep interventions such as sleep-hygiene counselling, cognitive behavioural therapy for insomnia referral pathways within ART clinics as pragmatic strategies to mitigate mental-health morbidity in this population [36].
CONCLUSIONS
We identified a substantial burden of depression and anxiety among PLHIV on ART and a robust, independent association with sleep quality, with good sleep protective for both outcomes. After adjustment, age ≥44 years increased the odds of anxiety, marriage showed a protective trend for depression, and sex and other clinical covariates were not independently associated. These findings support integrating routine PHQ-9/GAD-7 and PSQI screening into ART services with clear referral pathways (e.g. Cognitive Behavioral Therapy for Insomnia) and brief psychosocial care. Key limitations include the cross-sectional, single-centre design and regimen homogeneity; prospective and interventional studies should assess whether improving sleep reduces symptoms and enhances ART adherence and virologic outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Consolidated guidelines on HIV, viral hepatitis and STI prevention, diagnosis, treatment and care for key populations. Geneva, Switzerland: World Health Organization; 2022.36417550 · pubmed ↗
- 2Feuillet P Lert F Tron L Aubriere C Spire B Dray-Spira R Prevalence of and factors associated with depression among people living with HIV in France. HIV Med. 2017;18:383–94. 10.1111/hiv.1243827625202 · doi ↗ · pubmed ↗
- 3Narayan KM Miotti PG Anand NP Kline LM Harmston C Gulakowski R 3rd HIV and Noncommunicable Disease Comorbidities in the Era of Antiretroviral Therapy: A Vital Agenda for Research in Low- and Middle-Income Country Settings. J Acquir Immune Defic Syndr. 2014;67:S 2. 10.1097/QAI.000000000000026725117958 · doi ↗ · pubmed ↗
- 4Wandeler G Johnson LF Egger M Trends in life expectancy of HIV-positive adults on antiretroviral therapy across the globe: comparisons with general population. Curr Opin HIV AIDS. 2016;11:492. 10.1097/COH.000000000000029827254748 PMC 5055447 · doi ↗ · pubmed ↗
- 5Lofgren SM Bond DJ Nakasujja N Boulware DR Burden of Depression in Outpatient HIV-Infected adults in Sub-Saharan Africa; Systematic Review and Meta-analysis. AIDS Behav. 2020;24:1752–64. 10.1007/s 10461-019-02706-231720956 PMC 7478178 · doi ↗ · pubmed ↗
- 6Omann LR Dushimiyimana V Musoni-Rwililiza E Arnbjerg CJ Niyonkuru VU Iyamuremye JD Prevalence of Mental Health Disorders and Their Associated Risk Factors Among People Living with HIV in Rwanda: A Cross-Sectional Study. AIDS Behav. 2024;28:2666–82. 10.1007/s 10461-024-04358-338736005 PMC 11286631 · doi ↗ · pubmed ↗
- 7Camara A Sow MS TouréA Sako FB Camara I Soumaoro K Anxiety and depression among HIV patients of the infectious disease department of Conakry University Hospital in 2018. Epidemiol Infect. 2020;148:e 8. 10.1017/S 095026881900222 X 31931897 PMC 7019126 · doi ↗ · pubmed ↗
- 8Jin H Hampton Atkinson J Yu X Heaton RK Shi C Marcotte TP Depression and suicidality in HIV/AIDS in China. J Affect Disord. 2006;94:269–75. 10.1016/j.jad.2006.04.01316764941 · doi ↗ · pubmed ↗