Esophageal Rupture in Recessive Dystrophic Epidermolysis Bullosa
Yutaro Hara, Takahiro Muroya, Kenichi Hakamada

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
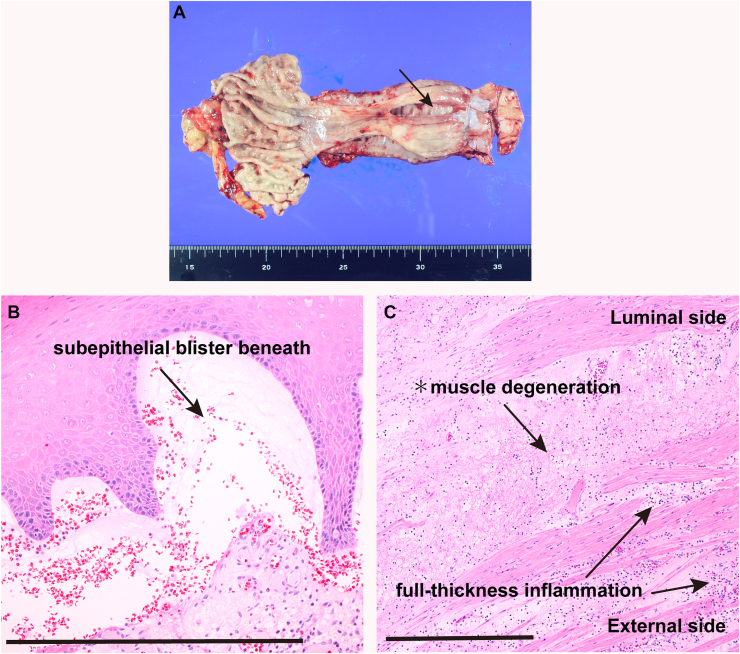 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSkin and Cellular Biology Research · Autoimmune Bullous Skin Diseases · Sympathectomy and Hyperhidrosis Treatments
A 44-year-old woman with severe generalized recessive dystrophic epidermolysis bullosa (RDEB) developed sudden anterior chest pain while eating. She reported no vomiting or other precipitating events that could increase intraesophageal pressure. Contrast esophagography demonstrated extravasation from the midthoracic esophagus into the right pleural cavity, and computed tomography revealed pneumomediastinum and a right pleural effusion. Emergency thoracoscopic subtotal esophagectomy with retrosternal gastric-conduit reconstruction was performed. Gross examination revealed a 5-cm longitudinal full-thickness perforation in the midthoracic esophagus (Figure A, arrow). Histological evaluation showed a subepithelial blister beneath the stratified squamous epithelium (Figure B, arrow), consistent with RDEB. Full-thickness chronic inflammation (Figure C, arrows) and degenerative changes with disruption of the inner circular muscle layer were also noted (Figure C, asterisk), indicating profound structural fragility of the esophageal wall. These findings support spontaneous esophageal rupture due to intrinsic mural fragility rather than an acute increase in luminal pressure. The postoperative course was uneventful, and the patient was discharged on postoperative day 22. Spontaneous esophageal rupture in RDEB is exceedingly rare and highlights the potential for mural fragility leading to catastrophic full-thickness failure of the esophageal wall in this condition.