Clinical Frailty Scale as a Predictor of Early Treatment Discontinuation in Elderly Patients With Chronic Lymphocytic Leukemia Treated With Zanubrutinib: A Multicenter Real‐World Study
Ernesto Vigna, Enrica Antonia Martino, Annalisa Pitino, Raffaella Pasquale, Isacco Ferrarini, Riccardo Moia, Andrea Visentin, Alessandro Sanna, Marina Motta, Massimo Moratti, Paolo Sportoletti, Annalisa Chiarenza, Alessandro Maggi, Valentina Zammit, Michele Merli

TL;DR
This study shows that the Clinical Frailty Scale can predict which elderly CLL patients are more likely to stop treatment with zanubrutinib.
Contribution
The study demonstrates the Clinical Frailty Scale's predictive value for treatment discontinuation in elderly CLL patients on zanubrutinib.
Findings
A CFS score of 3 was the optimal threshold for predicting treatment discontinuation.
Patients with a CFS > 3 had a significantly higher discontinuation rate at 12 months.
Frailty assessment adds prognostic value beyond standard disease-related factors.
Abstract
The management of chronic lymphocytic leukemia (CLL) in older patients requires careful balancing of therapeutic efficacy with the risks of treatment intolerance. Frailty assessment is increasingly recognized as a critical determinant of clinical outcomes, but its specific role in guiding therapy with second‐generation Bruton tyrosine kinase inhibitors remains poorly defined. We conducted a prospective, multicenter investigation of 326 consecutive CLL patients aged 65 years or older who received zanubrutinib across 52 Italian centers, aiming to evaluate whether the Clinical Frailty Scale (CFS) could predict treatment discontinuation in real‐world practice. The cohort was characterized by advanced age (median 78.1 years, range 65.1–94.5), with over half of the patients presenting with Binet stage C disease. Two‐thirds were treated in the frontline setting, while the remainder received…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
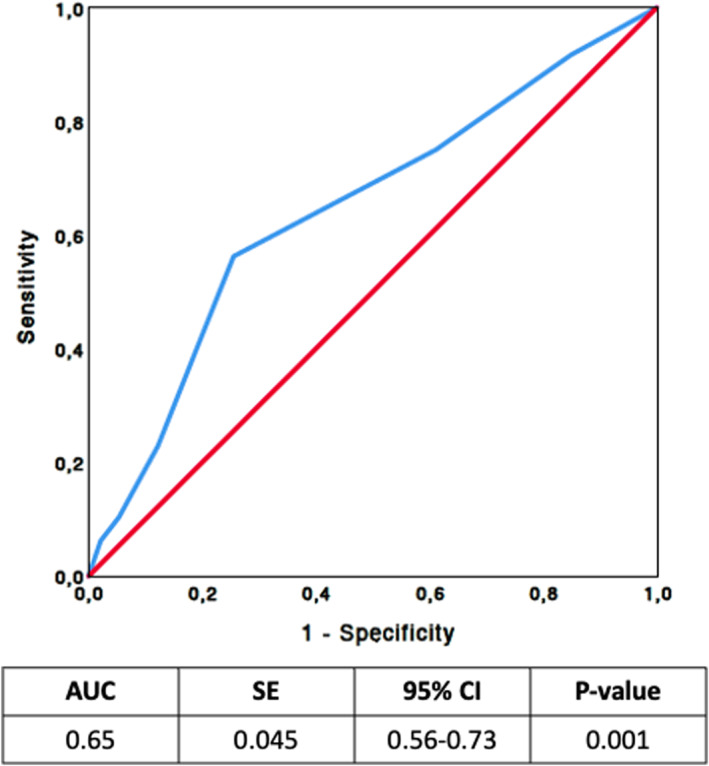 FIGURE 1
FIGURE 1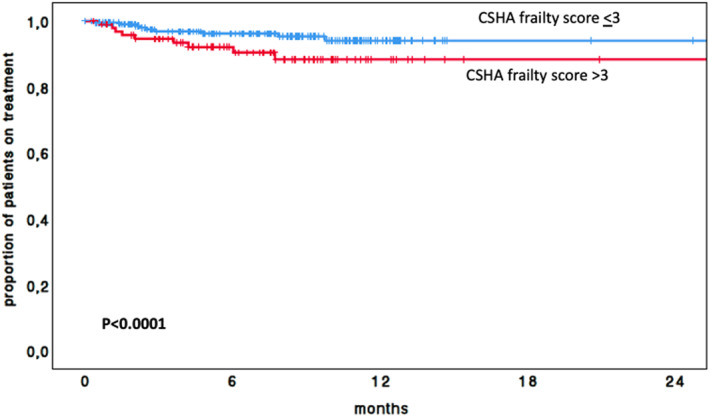 FIGURE 2
FIGURE 2| Level 1 | Very fit: People who are robust, active, energetic, and motivated. These people commonly exercise regularly. They are among the fittest for their age. |
| Level 2 | Fit: Previously known as well: People who have no intense disease symptoms but are less fit than level 1. Often, they exercise or are very active occasionally, for example, seasonally. |
| Level 3 | Managing well: People whose medical problems are well controlled, but are not regularly active beyond routine walking. |
| Level 4 | Living with very mild frailty‐while not dependent on others for daily help, often symptoms limit activities. A common complaint is being “slowed‐up” and being tired during the day. |
| Level 5 | Living with mild frailty: These people usually have more evident slowing and need help in higher‐order instrumental activities of daily living (IADLs) such as finance, transportation, heavy housework, medications. Typically, mild frailty progressively impairs shopping and walking outside alone, meal preparation, and housekeeping. |
| Level 6 | Living with moderate frailty: They need help with all outside activities and with keeping house. Inside, they often have problems with stairs and need help with bathing, and might need minimal assistance (standby) with dressing. |
| Level 7 | Living with severe frailty: is characterized by progressive dependence in personal ADLs. Completely dependent on personal care from whatever cause (physical or cognitive). Even though they seem stable and not at high risk of dying (within 6 months). |
| Level 8 | Living with very severe frailty: These patients are completely dependent, approaching the end of life. Typically, they could not recover even from minor illnesses. |
| Level 9 | Terminally Ill: Approaching the end of life. This category applies to people with a life expectancy of under 6 months, which are not otherwise evidently frail. |
|
Zanubrutinib ( | |
|---|---|
| Median age, years (range) | 78,1 (65,1–94,5) |
| Sex, | |
| Male | 195 (59.8) |
| Female | 131 (40.2) |
| Line of therapy, | |
| TN | 208 (63.8) |
| R/R | 118 (36.2) |
| Binet stage, | |
| A | 2 (9.8) |
| B | 124 (38) |
| C | 170 (52.1) |
| IGHV mutational status, | |
| Mutated | 97 (29.8) |
| Germline | 190 (58.3) |
| Unknown | 39 (12) |
| TP53 disruption, | |
| Absent | 218 (66.9) |
| Present | 68 (20.8) |
| Unknown | 40 (12.3) |
| CLL‐IPI risk (%) | |
| Low | 13 (4) |
| Intermediate | 67 (20.5) |
| High | 122 (37.4) |
| Very‐high | 59 (18.1) |
| Unknown | 65 (20) |
| CIRS | |
| 0–6 | 198 (60.7) |
| > 6 | 128 (39.3) |
| Clinical frailty scale | |
| 1 | 46 (14.1) |
| 2 | 74 (22.7) |
| 3 | 108 (33.1) |
| 4 | 53 (16.3) |
| 5 | 25 (7.7) |
| 6 | 11 (3.4) |
| 7 | 9 (2.8) |
| Cardiovascular risk factor, | |
| Hypertension | 139 (42.6) |
| Atrial fibrillation | 49 (15) |
| Hypercholesterolemia | 54 (16.6) |
| Congestive heart failure | 24 (7.4) |
| Peripheral arterial disease | 12 (3.7) |
| Cerebrovascular disease | 13 (4) |
| Diabetes | 62 (19) |
| Myocardial infarction | 47 (14.4) |
| Zanubrutinib | |
|---|---|
| Total patients | 326 |
| Patients who discontinued treatment, | 48 (18.7) |
| Median follow‐up (months) | 13 |
| Reasons for discontinuation | |
| Toxic effect of therapy | 14 (4.3) |
| Infection | 6 (1.8) |
| Bleeding episodes | 5 (1.5) |
| Atrial fibrillation | 1 (0.3) |
| Rash | 1 (0.3) |
| Hepatitis B virus reactivation | 1 (0.3) |
| Disease progression | |
| CLL | 16 (4.9) |
| Richter syndrome | 1 (0.3) |
| Second neoplasia | 3 (0.9) |
| Patient request | 1 (0.3) |
| not‐CLL related death | 6 (1.8) |
| Death from unknown causes | 7 (2.1) |
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| |
| Age | 1.052 (1.007–1.098) |
| 1.02 (0.98–1.07) | 0.33 |
| Sex | ||||
| Male versus female | 0.88 (0.49–1.59) | 0.68 | — | — |
| Line of therapy | ||||
| R/R versus TN | 2.03 (1.15–3.59) |
| 1.92 (1.08–3.41) |
|
| Binet stage | ||||
| B versus A | 1.83 (0.53–6.36) | 0.34 | — | — |
| C versus A | 1.69 (0.5–5.67) | 0.4 | — | — |
| IGHV mutational status | ||||
| Germline versus mutated | 1.66 (0.81–3.39) | 0.17 | — | — |
| TP53 disruption | ||||
| Present versus absent | 1.47 (0.74–2.93) | 0.27 | — | — |
| Clinical frailty scale | ||||
| ≤ 3 versus > 3 | 3.3 (1.87–5.84) |
| 2.74 (1.47–5.09) |
|
| CIRS | ||||
| < 6 versus ≥ 6 | 1.33 (0.75–2.36) | 0.32 | ||
| Cardiovascular risk factor | ||||
| Hypertension | 1.08 (0.61–1.91) | 0.9 | — | — |
| Atrial fibrillation | 1.1 (0.49–2.45) | 0.65 | — | — |
| Hypercholesterolemia | 2.2 (0.79–6.16) | 0.13 | — | — |
| Congestive heart failure | 3.07 (1.43–6.58) |
| 2.14 (0.98–4.68) | 0.06 |
| Peripheral arterial disease | 1.07 (0.25–4.48) | 0.93 | — | — |
| Cerebrovascular disease | 1.13 (0.27–4.67) | 0.86 | — | — |
| Diabetes | 1.57 (0.67–3.71) | 0.29 | — | — |
| Myocardial infarction | 1.38 (0.67–2.85) | 0.39 | — | — |
| ≥ 1 cardiovascular risk factor | 1.02 (0.77–1.35) | 0.89 | — | — |
- —PNRR‐MAD‐2022‐12375673
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · Frailty in Older Adults · Economic and Financial Impacts of Cancer
Introduction
1
Chronic lymphocytic leukemia (CLL) is the most common hematologic malignancy in Western countries, primarily affecting older adults who are more susceptible to age‐related health declines [1].
At treatment initiation, many elderly patients with CLL already present with multiple chronic conditions, which can impair physical function and compromise adherence to therapy [1, 2].
Over the last decades, the introduction of targeted oral agents has markedly improved treatment outcomes in CLL, leading to durable remissions and prolonged survival [2]. However, these therapies also pose new challenges, particularly regarding long‐term adherence and the risk of drug–drug interactions in a comorbid population [3].
Frailty, defined as a state of increased vulnerability to stressors due to age‐related decline in physiological reserves and functions, has emerged as a key prognostic factor in oncology. In older cancer patients, frailty assessment helps identify individuals at higher risk for treatment‐related toxicity and early mortality [4]. The European Society for Medical Oncology (ESMO) recommends incorporating frailty assessment into treatment decision‐making, as it is strongly associated with impaired physical and cognitive performance as well as reduced survival in CLL [5]. Additional instruments such as the Cumulative Illness Rating Scale (CIRS) and the Charlson Comorbidity Index (CCI) are frequently applied in CLL to quantify comorbidity burden, which has been correlated with inferior overall survival. Nevertheless, comprehensive geriatric assessments remain underutilized in routine practice, largely due to their complexity, time requirements, and specialized expertise [6, 7, 8].
The prognostic role of frailty in elderly CLL patients has been prospectively evaluated in the CLL‐Frail trial, which assessed the FRAIL scale in patients aged ≥ 80 years or otherwise classified as frail and treated with acalabrutinib [9]. This study established the feasibility of integrating frailty assessment into BTKi therapy and provided benchmark data for treatment outcomes in this population. However, the trial was limited by a small sample size and relied on a patient‐reported measure rather than a clinician‐assessed scale, leaving open questions regarding the applicability of objective frailty tools in larger, real‐world cohorts.
Recently, our group investigated the use of the Clinical Frailty Scale (CFS) for frailty assessment in elderly CLL patients treated with novel targeted agents, including Bruton's tyrosine kinase inhibitors (BTKis) and BCL2 inhibitors (BCL2is) [10]. The CFS, originally developed within the Canadian Study of Health and Aging (CSHA), is a simple 9‐point scale that provides a rapid global assessment of an older adult's overall fitness or frailty, making it a practical tool in busy clinical settings [11].
The present study aims to evaluate the predictive value of the CFS for therapy discontinuation in a cohort of 326 consecutive elderly CLL patients, both treatment‐naive and relapsed‐refractory, treated with second‐generation BTKi, zanubrutinib.
Materials and Methods
2
Study Design and Population
2.1
This study encompasses a cohort of 326 consecutive patients aged over 65 years, affected by CLL and treated with zanubrutinib as first‐line or subsequent therapy between May 2024 and the time of data cutoff, across 52 Italian centers. All patients signed a written informed consent. Frailty was assessed by physicians using CFS. Comprehensive demographic and clinical data were collected, including age, sex, CIRS score, and concomitant cardiovascular risk factors. Disease‐related characteristics included Binet staging, TP53 aberrations (17p deletion and/or TP53 mutations), and IGHV gene mutational status. Adverse events leading to therapy discontinuation were registered according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Discontinuations due to surgery were not considered treatment‐related toxicity. The study was approved by the Institutional Ethics Committees of all participating centers prior to data collection, in compliance with Italian regulations. The study was also conducted in accordance with the Declaration of Helsinki and Good Clinical Practice.
CSHA Clinical Frailty Scale
2.2
The CFS, developed within the CSHA [11], is a validated 9‐point tool that classifies older individuals according to functional capacity, vulnerability, and risk of mortality. The scale ranges from 1 (indicating robust health) to 9 (terminally ill) (Table 1). Frailty assessment was performed by trained physicians at treatment initiation, with each score assigned based on a physical examination and overall clinical impression. The scale ranges from 1 (very fit) to 9 (terminally ill) (Table 1). CFS assessments were conducted by trained hematologists at each participating center following CSHA guidelines. Although formal inter‐rater reliability was not evaluated, minor variability in scoring across centers cannot be excluded.
TABLE 1: The Canadian study of health and aging clinical frailty scale version 2.0 a .
Analytic Approach
2.3
The primary objective of the study was to evaluate the prognostic role of CFS in predicting time to discontinuation (TTD).
TTD was defined as the interval from treatment initiation to permanent discontinuation for any cause, including adverse events, disease progression, transformation to Richter's syndrome, or death, with a treatment interruption of > 30 days considered a discontinuation event. Competing risks, such as death, were not formally modeled in this analysis. All adverse events resulting in definitive treatment discontinuation were graded > 3 and considered irreversible. Only grade ≥ 3 adverse events leading to treatment discontinuation were considered; lower‐grade events potentially affecting adherence were not captured. Patients who were still receiving zanubrutinib at data cutoff were censored at their last follow‐up.
All included patients received zanubrutinib at the standard dose of 320 mg daily. Categorical variables were analyzed using Fisher's exact test (for two‐way tables) and Pearson's χ^2^ test (for multi‐way tables). Associations between individual variables and overall survival (OS) were assessed with the log‐rank test, and results were presented as hazard ratios (HRs) with 95% confidence intervals (CIs). The predictive performance of the CFS was evaluated using receiver operating characteristic (ROC) curve analysis, calculating the area under the curve (AUC), along with sensitivity, specificity, and both positive and negative predictive values, all reported with 95% CIs. The optimal cut‐off point for CFS was identified using Youden's index (J = sensitivity + specificity − 1), with the maximum value of J (0.243) indicating the threshold that best balanced sensitivity and specificity. The prognostic relevance of each variable was first assessed through univariable Cox regression analysis, with HRs and 95% CIs reported. Variables found to be statistically significant (P < 0.05) in univariable analysis were then included in a multivariable Cox regression model. All statistical analyses were conducted using STATA for Windows version 9 and SPSS Statistics version 21.
Results
3
Patients
3.1
Baseline characteristics of the study cohort are summarized in Table 2. The median age at zanubrutinib initiation was 78.1 years (range 65.1–94.5 years). More than half of the cohort (52.1%) presented with Binet stage C disease, while the remaining patients (stage A/B) initiated treatment due to disease progression or disease‐related symptoms, according to the International Workshop on CLL guidelines [8].
With regard to IGHV gene status, 29.8% of patients were mutated, 58.3% unmutated, and in 11.9% the information was unavailable. Cytogenetic analysis revealed del(17p) and/or TP53 mutations in 20.8% of patients (68 cases). A CIRS score > 6 at therapy initiation was observed in over one‐third of the cohort. Hypertension was the most frequent comorbidity (42.6%). Atrial fibrillation and previous myocardial infarction were reported in 15% and 14.4% of patients, respectively. Additional cardiovascular risk factors included diabetes (19%) and hypercholesterolemia (16.6%). According to the CSHA CFS, 46 patients (14.1%) scored 1, 74 (22.7%) scored 2, 108 (33.1%) scored 3, 53 (16.3%) scored 4, 25 (7.7%) scored 5, 11 (3.4%) scored 6, and 9 (2.8%) scored 7; no cases scored 8–9. Overall, 63.8% (208 cases) were treatment‐naïve, while 36.2% (118 patients) received zanubrutinib as salvage therapy. In the subgroup of the treatment‐naïve, 28 patients (13.5%) showed a CSHA CFS of 1, 45 (21.6%) of 2, 73 (35.1%) of 3, 31 (14.9%) of 4, 18 (8.7%) of 5, 8 (3.8%) of 6, and 5 (2.4%) of 7; in the subgroup of relapsed/refractory 18 patients (15.3%) showed a CSHA CFS of 1, 29 (24.6%) of 2, 35 (29.7%) of 3, 22 (18.6%) of 4, 7 (5.9%) of 5, 3 (2.5%) of 6, and 4 (3.4%) of 7.
Safety
3.2
After a median follow‐up of 13 months, treatment was permanently discontinued in 48 patients (18.7%). The major causes for discontinuation were treatment‐related toxicity and disease progression (Table 3). Specifically, 14 patients (5.8%) discontinued due to adverse events: 6 cases for infections, 5 for bleeding, 1 for atrial fibrillation, 1 for rash, and 1 for HBV reactivation. Disease progression accounted for 17 discontinuations, including 1 Richter's transformation. An additional 13 patients (1.5%) discontinued treatment due to deaths (6 cases unrelated to CLL and 7 for unknown causes) (Table 3). Three patients discontinued treatment due to the occurrence of a second malignancy, and 1 patient withdrew consent.
CSHA CFS and Prediction of Treatment to Discontinuation
3.3
The predictive value of the CSHA CFS for TTD was evaluated using ROC curve analysis (Figure 1). The AUC was 0.65 (95% CI: 0.56–0.73; p < 0.001). The optimal cutoff point was identified at a CFS of 3, corresponding to a sensitivity of 56% and specificity of 75%. Overall, 228 (69.9%) had a CFS ≤ 3, while 98 (30.1%) had a CFS > 3. At 12 months, the discontinuation rate was significantly higher among patients with a CFS > 3 (29.2%) compared with those with a CFS ≤ 3 (8.8%) (p < 0.001; Figure 2 and Table 4).
Receiver operating characteristic (ROC) analysis of canadian study of health and aging (CSHA) clinical frailty scale (CFS) for predicting time to discontinuation (TTD) of CLL patients treated with zanubrutinib.
Kaplan‐meier curve of TTD of the entire cohort according to the canadian study of health and aging (CSHA) clinical frailty scale (CFS).
At univariate analysis, in addition to a CFS > 3, age, treatment setting (treatment‐naïve vs. relapsed/refractory) and congestive heart failure showed a significant association with treatment discontinuation. At multivariate analysis only CFS > 3 (HR = 1.92, 95% CI: 1.08–3.41; p = 0.001) and relapsed/refractory disease (HR = 2.74, 95% CI: 1.47–5.09; p = 0.027) remained statistically associated with a shorter TTD (Table 4).
Discussion
4
Geriatric assessment provides a comprehensive evaluation of elderly patients' health status, enabling identification of those at increased risk of treatment‐related toxicity and early therapy discontinuation. Integrating geriatric dimensions into routine clinical practice remains highly relevant, even in the era of targeted therapies.
Several clinical trials [12, 13] have highlighted the prognostic impact of geriatric domains—including functional, psychological, and cognitive status, as well as social support—on survival, underscoring the importance of incorporating the frailty evaluation into therapeutic decision‐making for CLL patients. Such assessment may help identify individuals more likely to experience toxicities and guide the implementation of supportive measures.
In our previous study [10] of 82 CLL patients aged ≥ 65 years treated with BTKis or BCL‐2is, the CSHA CFS proved to be a simple and effective tool for distinguishing patients able to tolerate small‐molecule therapy from those who were not. ROC curve analysis identified a value of 3, above which patients were more likely to discontinue therapy prematurely.
The CLL‐Frail trial represents the first prospective study evaluating frailty in elderly CLL patients treated with a BTK inhibitor, using the patient‐reported FRAIL scale to identify individuals at higher risk of treatment‐related toxicity and adverse outcomes [9]. This study demonstrated the feasibility of integrating frailty assessment into treatment planning and provided important benchmark data for therapy response and early discontinuation. Our study complements these findings by assessing frailty using a clinician‐judged global measure (CFS) in a larger, multicenter, real‐world cohort treated with zanubrutinib. Unlike the FRAIL scale, which relies on patient‐reported functional items, the CFS provides a rapid, objective bedside evaluation of overall physiological reserve and vulnerability, allowing a practical assessment that can inform therapy decisions and predict early discontinuation in routine practice. However, direct head‐to‐head comparisons are lacking and warranted in future studies.
The present analysis, conducted in a larger cohort of elderly CLL patients treated exclusively with zanubrutinib, confirmed the prognostic validity of this cut‐off. Patients who scored ≥ 3 had nearly a 2.7‐fold likelihood of early treatment interruption compared with those scoring ≤ 3. These findings support the hypothesis that dose adjustment strategies could be beneficial for frail patients deemed unlikely to tolerate full‐dose therapy. While pharmacokinetic and pharmacodynamic data specifically for zanubrutinib in frail patients are not available, studies with other BTK inhibitors, such as ibrutinib have demonstrated that full‐dose administration produces drug concentrations exceeding those required for a complete occupancy of the BTK receptor [14]. These observations suggest that, in frail patients at higher risk of early discontinuation, careful dose adjustment strategies could potentially improve adherence and prolong treatment exposure, though this hypothesis requires formal evaluation in prospective studies.
Although no clinical trial has demonstrated that educed doses of BTK inhibitors achieve clinical outcomes comparable to standard dosing in terms of response rates, PFS, or OS compared and zanubrutinib dose reductions have generally been associated with inferior outcomes in general [15], it is conceivable that in highly frail patients at increased risk of early discontinuation, carefully selected dose modifications reduced dosing could improve tolerability, enhance adherence, and ultimately prolong treatment exposure. This hypothesis remains speculative and warrants prospective evaluation. Relapsed/refractory disease, together with a CSHA CFS > 3, was independently associated with treatment discontinuation. This is expected, as relapsed/refractory patients have a higher incidence of disease progression compared with first‐line patients (7% vs. 3%).
Interestingly, other clinical and biological parameters—including age, gender, CIRS > 6, Binet stage, IGHV mutational status, and TP53 abnormalities—did not significantly influence the risk of treatment discontinuation in our study.
With a median follow‐up of 13 months, 14 out of 326 patients (4.3%) discontinued zanubrutinib due to toxicity. To note, limited cardiac events were recorded (1 case of atrial fibrillation), and among the off‐target effects, 5 bleeding events led to drug withdrawal. Although the short follow‐up limits definitive conclusions, these findings reinforce the favorable tolerability profile of zanubrutinib and support its feasibility in real‐world use among older CLL patients. A recent real‐world study from Kaiser Permanente Northern California [16], including 281 CLL patients treated with ibrutinib followed by zanubrutinib or zanubrutinib alone, found that in the zanubrutinib‐only cohort—where at least half of the patients were ≥ 71 and had multiple comorbidities—after a median follow up of 8.2 months, zanubrutinib was associated with low cardiotoxicity and a reduced rate of discontinuations due to adverse events.
Nonetheless, several important challenges remain regarding frailty assessment in CLL. First, most evidence on the prognostic value of geriatric tools derives from the chemoimmunotherapy era, with relatively few studies exploring their relevance in the context of targeted therapies. Second, the predictive value of frailty may be influenced by disease biology, particularly in cases with Richter's transformation or B symptoms. In our cohort, only one transformation to aggressive lymphoma occurred, limiting further interpretation. Third, the practical implementation of frailty assessments in daily practice is hampered by their complexity and the time required, particularly in high‐volume hematology clinics.
In conclusion, this real‐world multicenter study highlights the value of the CFS in assessing elderly patients with CLL treated with zanubrutinib.
Strengths include the pragmatic design, the inclusion of a frail population rarely represented in clinical trials, and the use of a simple bedside tool easily applicable in routine practice. CFS provides meaningful information beyond conventional prognostic markers and may help personalize therapy in the era of second‐generation BTK inhibitors. Compared with the FRAIL score, CFS is a clinician‐judged global frailty scale rather than a patient‐reported screening tool, offering a more nuanced and objective assessment, though direct comparisons are warranted.
The study also presents limitations. The relatively short follow‐up and the low number of discontinuation events limit the power of multivariable analyses and may increase the risk of overfitting. The definition of treatment discontinuation as a > 30‐day interruption, while consistent with real‐world practice, may overestimate events relative to standard iwCLL criteria. CFS assessments were physician‐judged across multiple centers without formal inter‐rater reliability testing, introducing potential variability. Competing risks, such as death, were not formally modeled. Only grade ≥ 3 adverse events resulting in permanent discontinuation were captured, potentially underestimating the impact of lower‐grade toxicities on adherence. Moreover, discussion of dose reductions remains speculative due to limited pharmacokinetic data for zanubrutinib in frail populations, underscoring the need for prospective validation. Finally, long‐term outcome evaluation, and the absence of direct comparison with other geriatric tools precludes definitive conclusions on its superiority.
Overall, CFS emerges as a feasible and informative approach to frailty assessment, warranting confirmation in larger, prospective studies with extended follow‐up.
Author Contributions
All Authors contributed equally to this study.
Funding
This study was supported by the PNRR‐MAD‐2022‐12375673.
Ethics Statement
All participating centers obtained ethics approval for this study, which was conducted in accordance with the Declaration of Helsinki.
Consent
Written informed consent has been obtained from the involved patients
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. C. Barrientos , “Management of Chronic Lymphocytic Leukemia in the Elderly,” supplement, Cancer Control 22, no. 4S 1 (2015): 17–23, 10.1177/107327481502204 s 04.26618342 PMC 4763599 · doi ↗ · pubmed ↗
- 2B. Eichhorst , P. Ghia , C. Niemann , et al., “ESMO Clinical Practice Guideline Interim Update on New Targeted Therapies in the First Line and at Relapse of Chronic Lymphocytic Leukaemia,” Annals of Oncology 35, no. 9 (2024): 762–768, 10.1016/j.annonc.2024.06.016.38969011 · doi ↗ · pubmed ↗
- 3J. M. Rhodes , J. C. Barrientos , and K. R. Rai , “How Have Targeted Agents Changed the Treatment Landscape for Elderly Patients With CLL?,” Current Oncology Reports 24, no. 12 (2022): 1705–1713, 10.1007/s 11912-022-01322-z.36334220 · doi ↗ · pubmed ↗
- 4A. Clegg , J. Young , S. Iliffe , M. O. Rikkert , and K. Rockwood , “Frailty in Elderly People,” Lancet 381, no. 9868 (2013): 752–762, 10.1016/S 0140-6736(12)62167-9.23395245 PMC 4098658 · doi ↗ · pubmed ↗
- 5R. Stauder , B. Eichhorst , M. E. Hamaker , et al., “Management of Chronic Lymphocytic Leukemia (CLL) in the Elderly: A Position Paper From an International Society of Geriatric Oncology (SIOG) Task Force,” Annals of Oncology 28, no. 2 (2017): 218–227, 10.1093/annonc/mdw 547.27803007 · doi ↗ · pubmed ↗
- 6P. Thurmes , T. Call , S. Slager , et al., “Comorbid Conditions and Survival in Unselected, Newly Diagnosed Patients With Chronic Lymphocytic Leukemia,” Leukemia and Lymphoma 49, no. 1 (2008): 49–56, 10.1080/10428190701724785.18203011 · doi ↗ · pubmed ↗
- 7T. Baumann , J. Delgado , R. Santacruz , et al., “Chronic Lymphocytic Leukemia in the Elderly: Clinico‐Biological Features, Outcomes, and Proposal of a Prognostic Model,” Haematologica 99, no. 10 (2014): 1599–1604, 10.3324/haematol.2014.107326.24972773 PMC 4181256 · doi ↗ · pubmed ↗
- 8M. Hallek , B. D. Cheson , D. Catovsky , et al., “iw CLL Guidelines for Diagnosis, Indications for Treatment, Response Assessment, and Supportive Management of CLL,” Blood 131, no. 25 (2018): 2745–2760, 10.1182/blood-2017-09-806398.29540348 · doi ↗ · pubmed ↗