Interactive behavior in mothers with and without borderline personality disorder: non-hostile behavior is associated with stronger neural activation of the theory of mind network in response to sad faces of the own child
Kristina Meyer, Catherine Hindi Attar, Christian Banzhaf, Katja Boedeker, Ines Boegen, Katja Dittrich, Christine Heim, Sabine C. Herpertz, Charlotte Jaite, Dorothea Kluczniok, Corinne Neukel, Sina K. Poppinga, Salomé Porten, Stefan Roepke, Nikola Schoofs, Felix Bermpohl

TL;DR
Mothers with borderline personality disorder show reduced ability to recognize their child's emotions, and non-hostile behavior is linked to stronger brain activity in regions related to understanding others' emotions.
Contribution
This study links non-hostile maternal behavior to stronger theory of mind network activation in response to a child's sad face in mothers with and without BPD.
Findings
Mothers with BPD showed lower performance in recognizing child facial expressions across emotions.
Maternal non-hostility was associated with higher activation in the temporoparietal junction and dorsomedial prefrontal cortex when viewing their own child's sad face.
Stronger theory of mind network activation in response to a child's sad face is linked to less hostile maternal behavior.
Abstract
Borderline personality disorder (BPD) affects many facets of interpersonal functioning, including maternal caregiving. Deficits in theory of mind (ToM) may put mothers with BPD at risk of showing dysfunctional parenting behavior. The present study investigated the association between the ToM brain network activation and parental behavior using functional magnetic resonance imaging (fMRI). In the present study conducted within the UBICA project (Understanding and Breaking the Intergenerational Cycle of Abuse), mothers with BPD (n=19) and healthy controls (HCs, n=30) completed an affect recognition task where they viewed sad, happy, and neutral faces of their own vs. unknown children during fMRI. Additionally, maternal non-hostility, the degree of maternal angry or irritable negative affect during mother-child-interactions, was assessed with the emotional availability scales. Mothers…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
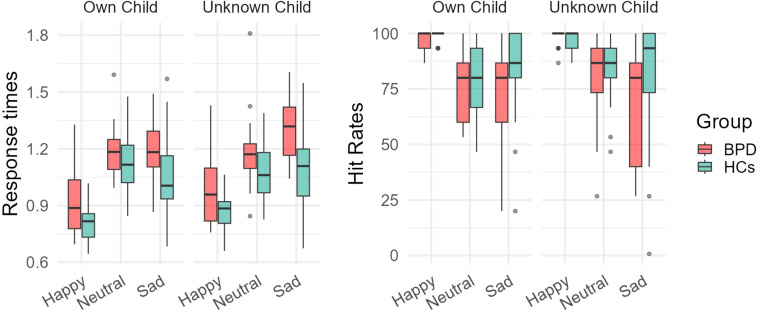 Figure 1
Figure 1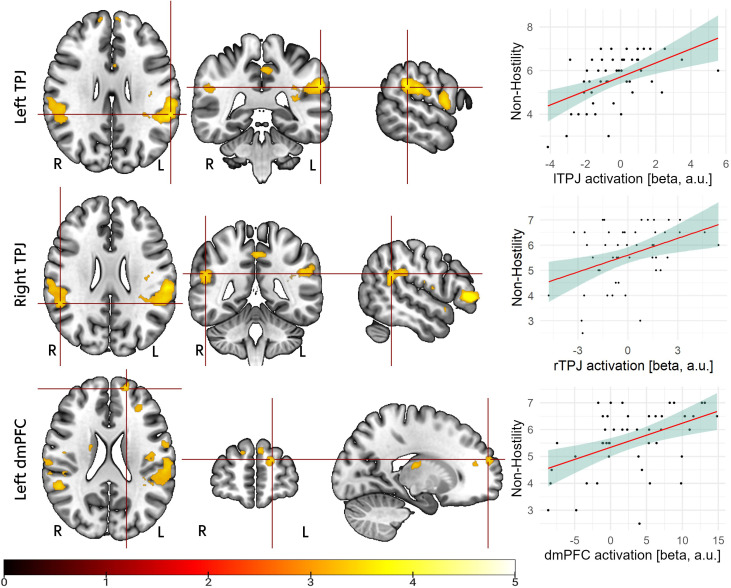 Figure 2
Figure 2| Variable name | BPD (n = 19) | HCs (n = 30) |
|
| ||
|---|---|---|---|---|---|---|
|
|
|
|
| |||
| Age (mother) | 34.8 | 4.8 | 39.8 | 5.4 | 3.3 | 0.002 |
| BDI-II | 24.6 | 15.2 | 4.3 | 5.1 | -6.6 | <.001 |
| PSI | 141 | 34 | 171.8 | 36.4 | 2.8 | 0.004 |
| Child sex: female | 47.40% | 56.70% | ||||
| History of abuse assessed using CECA: | ||||||
| Neglect: none | 4 (21.1%) | 25 (83.3%) | ||||
| Neglect: low | 4 (21.1%) | 5 (16.7%) | ||||
| Neglect: moderate | 6 (31.6%) | 0 | ||||
| Neglect: severe | 4 (21.1%) | 0 | ||||
| Emotional abuse: none | 10 (52.6%) | 30 (100%) | ||||
| Emotional abuse: low | 2 (10.5%) | 0 | ||||
| Emotional abuse: moderate | 3 (15.8%) | 0 | ||||
| Emotional abuse: severe | 4 (21.1%) | 0 | ||||
| Physical abuse: none | 2 (10.5%) | 23 (76.7%) | ||||
| Physical abuse: low | 7 (36.8%) | 7 (23.3%) | ||||
| Physical abuse: moderate | 7 (36.8%) | 0 | ||||
| Physical abuse: severe | 3 (15.8%) | 0 | ||||
| Sexual abuse: none | 6 (31.6%) | 27 (90.0%) | ||||
| Sexual abuse: low | 3 (15.8%) | 2 (6.7%) | ||||
| Sexual abuse: moderate | 2 (10.5%) | 0 | ||||
| Sexual abuse: severe | 8 (42.1%) | 1 (3.3%) | ||||
| Reported medication | ||||||
| Antidepressant | 3 (15.8%) | 0 | ||||
| Antiepileptics | 1 (5.2%) | 0 | ||||
| Thyroid | 1 (5.2%) | 4 (13.3%) | ||||
| Other | 1 (5.2%) | 3 (10%) | ||||
| Group | Emotion | Identity | Hit rates (%) | Response time (s) | ||
|---|---|---|---|---|---|---|
| M | SD | M | SD | |||
| BPD | Happy | Own Child | 97.89 | 3.88 | 0.92 | 0.18 |
| BPD | Happy | Unknown Child | 97.89 | 3.88 | 0.98 | 0.18 |
| BPD | Neutral | Own Child | 73.68 | 23.46 | 1.19 | 0.15 |
| BPD | Neutral | Unknown Child | 77.19 | 26.13 | 1.17 | 0.22 |
| BPD | Sad | Own Child | 64.91 | 32.80 | 1.21 | 0.16 |
| BPD | Sad | Unknown Child | 61.75 | 32.95 | 1.28 | 0.18 |
| HCs | Happy | Own Child | 99.31 | 2.07 | 0.82 | 0.10 |
| HCs | Happy | Unknown Child | 97.93 | 3.61 | 0.88 | 0.09 |
| HCs | Neutral | Own Child | 78.39 | 17.06 | 1.13 | 0.16 |
| HCs | Neutral | Unknown Child | 84.37 | 13.72 | 1.07 | 0.14 |
| HCs | Sad | Own Child | 85.29 | 19.30 | 1.05 | 0.21 |
| HCs | Sad | Unknown Child | 81.40 | 24.82 | 1.09 | 0.20 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPersonality Disorders and Psychopathology · Bipolar Disorder and Treatment · Attachment and Relationship Dynamics
Introduction
1
Borderline personality disorder (BPD) is characterized by difficulties in forming relationships, an unstable self-image, impulsivity, and identity problems (1). Close social relationships of individuals with BPD often show conflicts, alternating idealization and devaluation, and a lack of trust (2, 3). These difficulties manifest also in the family context. In families of mothers with BPD, mother-child relationships are often burdened (4, 5). For instance, mothers with BPD and their children have an increased risk of insecure or disorganized attachment styles (6). Family interactions are reported to be characterized by less family cohesion and lower structuring (7).
Dysfunctional parenting behavior may include overt and covert aggression towards the child, facially or vocally expressed anger, annoyance, or boredom, and frightening or threatening behaviors (8, 9). Such dysfunctional parenting behavior is a risk factor for adverse child outcomes. For example, mother-child interactions with mutual anger expression in toddlerhood predicted child conduct problems at school entry (10). In a meta-analysis, Khaleque (11) linked parental hostility/aggression, a subscale of the child version of the parental acceptance-rejection questionnaire, to child maladjustment, e.g., child aggression and emotional instability. Many BPD patients were exposed to childhood maltreatment (12), which parents with BPD describe as a strong source of motivation to do their best to create a better developmental environment for their own children (13). However, despite the parents’ best efforts, parental personality disorders, including BPD, remain a risk factor for dysfunctional parenting behavior (14). This underlines the urgent need for research to understand the intergenerational transmission pathways of dysfunctional parenting and, ultimately, improve targeted care for parents with BPD and their children (5).
Different BPD symptoms may affect parent-child interactions in parents with BPD (13, 15). Part of the social interaction difficulties in BPD may be attributed to social cognition deficits (16–18). Social cognition refers to cognitive abilities relevant to social interactions (19). It includes theory of mind (ToM), the ability to internally represent the feelings, intentions, and actions of others (20). Affective ToM refers to the representation of the feelings of others while cognitive ToM refers to the interpretation of others’ thoughts and intentions. In the context of parenthood, social cognitive abilities have been capitalized as important, allowing parents to understand their children’s needs and feelings (21, 22).
Experimental studies linked BPD symptoms to social cognition deficits. For example, Ortega-Díaz et al. (23) asked individuals with BPD, their first-degree relatives, and a sample of healthy controls (HCs) to complete tasks of different aspects of ToM. They found altered ToM processing in BPD patients relative to HCs. In a meta-analysis, Nemeth and colleagues (16) reported consistent deficits in cognitive ToM and task-dependent deficits in affective ToM in individuals with BPD.
Using functional magnetic resonance imaging (fMRI), ToM abilities have been mapped to activation in regions of the brain such as the temporoparietal junction (TPJ), the dorsomedial prefrontal cortex (dmPFC), the posterior cingulate cortex (PCC), and the precuneus (24, 25). Previous fMRI studies have demonstrated increased neural responses of brain regions associated with ToM as well as empathy upon seeing children in social situations in mothers compared to age-matched non-mothers, hinting towards the relevance of social cognition in motherhood (26, 27).
FMRI studies have shown that the brain regions activated upon seeing one’s own as opposed to an unknown child diverge (28), indicating specific neural processes that allow mothers to engage in social interactions with their children. Because the risk of parent-child interaction problems is higher in demanding emotional situations, and because sadness is thought to be particularly difficult for many BPD patients (29, 30), we focus on neural responses to children’s sad faces.
Given the role of ToM in successful parenting, we will focus on the ToM brain network (24, 31) in mothers with BPD. We use data from the multicentric UBICA project (Understanding and Breaking the Intergenerational Cycle of Abuse) on maternal parenting behavior observed in mother-child interactions, performance in an affect recognition task with own and unknown sad child faces, and the ToM network activation in response to these faces. In a previous study from the UBICA project, Kluczniok et al. (32) found that mothers with BPD showed less non-hostile parenting behavior as assessed using the emotional availability (EA) scales (8, 9) than mothers with remitted major depression and HCs. While the present study uses partly the same behavioral data, we focus here on a sub-sample who participated in the fMRI study.
In the present study, we examined whether dysfunctional parenting behavior, specifically the display of maternal irritability, anger, or aggression, is associated with altered affective ToM at the behavioral and neural level. At the behavioral level, we hypothesize that 1) mothers with BPD show impaired affect recognition, which we deem a precursor ability related to affective ToM, and that 2) the affect recognition performance for sad child faces is associated with maternal dysfunctional parenting behavior. At the neural level, we hypothesize that 3) mothers with BPD activate their ToM network less strongly than HCs when seeing faces of their own versus unknown sad children, and that 4) the ToM network activation in own vs. unknown sad children is related to the extent of maternal dysfunctional parenting behavior.
Methods
2
Sample description
2.1
19 mothers with BPD and 30 HC mothers (Table 1) participated in the study that was approved by the ethics committee of the Charité – Universitätsmedizin Berlin (approved 27.08.2013, EA2/097/13). All 49 participated in the fMRI study and had sufficient data quality after fMRI quality control (Supplementary Material 1 contains quality control criteria). One mother in the BPD group and one in the HC group did not participate in the mother-child interaction task due to time constraints unrelated to the study design, reducing sample sizes in these sub-analyses by one per group.
Mothers from both groups and their biological children aged 5–12 years (M = 8.31, SD = 1.97) were required to live together and be proficient in German. In the BPD group, inclusion criteria were a current BPD diagnosis (per the International Personality Disorder Examination interview, IPDE) (36) and remission from mood episodes as per a score of < 8 in the Hamilton Depression Scale (37, 38).
In the HC group, mothers were included if they reported no current or lifetime axis I or II disorders in the IPDE or the Mini International Neuropsychiatric Interview (MINI) (39).
Mothers were excluded in case of: acute suicidality, being in an emotional crisis or hospitalized, neurological diseases, current alcohol or drug dependence, a history of schizophrenia or manic episodes per the MINI, anxious-avoidant or antisocial personality disorder per the IPDE, use of benzodiazepines within the past six months (40), change of psychotropic medication two weeks before study entry.
Children were excluded if they had a diagnosis of autistic disorder (based on DSM-IV criteria) or an IQ score below 70 in the Culture Fair Intelligence Tests (41).
In the BPD group, current and lifetime comorbid disorders were assessed using the MINI (39). Of the mothers with BPD, n = 17 reported a history of previous depressive disorders, n = 4 reported current comorbid anxiety disorders, n = 1 a current obsessive compulsive disorder, n = 3 reported current substance abuse, and n = 2 reported a current eating disorder. N = 5 mothers with BPD reported no history of psychiatric hospitalizations, n = 4 reported one hospitalization, n = 10 reported two or more hospitalizations.
Data collection
2.2
Maternal non-hostility assessed using the emotional availability scales
2.2.1
The EA scales are an observation tool for parent-child interactions that yields the parental scales non-hostility, non-intrusiveness, sensitivity, and structuring (9). The validity of the EA scales is suggested, for instance, by convergent validity with other parent-child interaction observation tools (42) and criterion validity through associations with parent and child attachment and parental mental illness (43, 44) as reviewed in (8).
Because Kluczniok, Boedeker (32) reported less non-hostile parenting behavior, but unaffected sensitivity in mothers with BPD, we focus on maternal non-hostility for the present analysis.
In the first 15 minutes of the video-recorded parent-child interaction, dyads played with a standardized set of age-appropriate toys as they normally would. After the free play, the children were given a puzzle (Shape by Shape) at a difficulty level slightly too high for their age for 6 minutes. Mothers were instructed to assist the child without solving the puzzle for them.
Three trained raters evaluated maternal non-hostility on a scale of 1 to 7 with higher scores signifying lack of hostility, higher scores signifying covert hostility (e.g., subtle signs of annoyance or boredom, slightly raising one’s voice, responding irritably), and lowest scores signifying overtly aggressive or threatening behaviors. All videos were coded by at least two raters blind to participant diagnosis. Discrepancies were resolved through discussion. Inter rater reliability ranged between r = .84 and r = .90 for the non-hostility scale, indicating good to excellent agreement (45).
MRI task
2.2.2
The task was developed for the purpose of the UBICA project (46, 47) and heeded common recommendations for timing and stimulus presentation in fMRI (48). In the scanner, mothers completed an affect recognition task in a 3x2 design (facial emotion: happy, sad, neutral; child identity: own child vs. unknown child) with child face stimuli generated for the present study. Individual child images of the participants’ children were created beforehand in a separate mood induction session [Supplementary Material 2 and (46)]. During fMRI, a total of 180 images were presented in a pseudo-randomized order. 50% of the images showed the own child, the other 50% the unfamiliar child. A trial started with the presentation of a child face (2s) followed by a fixation cross for a randomly chosen period of 2-6s. Mothers were instructed to classify the affective facial expression as quickly and accurately as possible by button press using the index (randomized for sad/happy), middle (for neutral) and ring finger (randomized for sad/happy) of their right hand. The task was distributed across two runs of 8 minutes each.
MRI scanning parameters
2.2.3
MRI scanning parameters are described in Supplementary Material 3.
Data analysis
2.3
Behavioral data
2.3.1
Behavioral data were analyzed using R (49) and different packages (50–57). We conducted a 2x3x2 analysis of variance (ANOVA) to investigate the effect of group (BPD vs. HC), child facial expression (sad, neutral, happy), and child identity (own child vs. unknown child) on response times (RTs) and hit rates of the within-scanner affect recognition task. Greenhouse-Geisser corrections were applied whenever deemed necessary by sphericity tests (58). Further, bivariate Pearson correlations between performance in recognizing sad faces and maternal non-hostility were computed.
We performed one-sided significance tests and applied Bonferroni corrections to the ANOVAs’ post-hoc pairwise comparisons and Pearson correlations.
MRI data
2.3.2
Data analysis of the imaging data was conducted using the statistical parametric mapping (SPM12) in MATLAB. Preprocessing is described in Supplementary Material 4.
At the first level, neural responses were modelled using a general linear model including six regressors representing all combinations of child identity (own, unknown) and facial emotion (sad, happy, neutral).
To test group differences in neural activation to sad expressions of one’s own versus an unfamiliar child, the first-level contrast (sad own > sad unknown) was computed for each participant. These individual contrast images were then entered into a two-sample t-test to compare BPD and HC groups (HC > BPD and BPD > HC), with age included as a covariate.
We tested for an association between maternal behavior and brain activation by regressing non-hostility on ToM network activation while viewing sad faces of the own vs. unknown children in SPM12. For this, groups were pooled. Maternal age was entered as a nuisance regressor to the model.
All hypothesis-driven second-level analyses of brain activation using fMRI – group comparisons and regressions – were restricted to an a priori ToM network mask. This region of interest (ROI) included the bilateral TPJ, dmPFC, PCC, and precuneus, based on the predefined ToM template from (24). The use of an a priori–defined template of the ToM network was chosen to facilitate comparability with previous research on ToM network modulations in clinical samples (59). Small-volume correction within this mask was applied (FWE p <.05). Using a single combined ToM mask ensured a conservative and theory-guided testing.
To validate the findings derived from this template-based ROI, we additionally employed a functional ROI of the regions significantly (whole-brain analysis, p < 0.01 uncorrected) activated in the own sad child > unknown sad child contrast generated by a one-sample t-test in the current sample (Supplementary Material 5).
To explore potential effects outside the ToM network, we additionally conducted whole-brain analyses at a threshold of FWE-corrected p <.001 (Supplementary Material 6).
Results
3
Behavioral results: maternal non-hostility
3.1
Mothers with and without BPD showed overall mostly non-hostile parenting behavior with average ratings between five and six, indicating mostly covert signs of anger, impatience, or boredom (e.g., slightly raising one’s voice, rolling eyes, snapping at the child or responding irritably), but the HCs were rated significantly more non-hostile than mothers with BPD (MHCs = 5.93 ± 0.96; t = 2.6, p = .01; MBPD = 5.08 ± 1.31). This was in line with the results from the total UBICA sample reported in Kluczniok et al. (32).
Behavioral results, hypothesis 1: group differences in affect recognition
3.2
In the following, ANOVA results for RTs and hit rates of the affect recognition task are reported (Figure 1, Table 2). In two individuals of the BPD and one of the HC groups, hit rates were 0% in at least one condition. In a sensitivity analysis, we excluded these individuals and repeated the ANOVA analyses, but the results remained identical in interpretation. Therefore, we report the results with the full sample.
Boxplots of response times in seconds and hit rates in % correct responses in the inside-scanner affect recognition task. The task followed a 3x2 design with emotion (happy, neutral, sad) and identity (own child vs. unknown child) as within-subject factors. BPD, mothers with borderline personality disorder. HCs, healthy control mothers. The black crossbars represent mean values, the boxes represent the 25th to 75th quartile, the whiskers represent values up to 1.5 times the interquartile range outside the 25th and 75th quartiles.
Response times
3.2.1
There were significant main effects of group (F (1, 44) = 14.7, p <.001), emotion (F_(2, 88)_ = 64.8, p <.001), identity (F_(1, 44)_ = 5.2, p = .03), and a significant emotion*identity interaction (F_(2, 88)_ = 4.9, p = .02). Pairwise comparisons revealed that mothers with BPD compared to HCs showed longer response times (p <.001), confirming Hypothesis 1. Faces of own children were generally processed faster than faces of unknown children (p = .03). Happy faces were processed faster than neutral and sad faces (p <.001), but there was no difference between sad and neutral faces (p = 1.0).
The emotion*identity interaction indicated that the processing of own child faces was faster than unknown child faces for sad (p = .03) and happy (p <.001) facial expressions, but there was no difference between the speed of processing neutral own vs. unknown child faces (p = .24).
Hit rates
3.2.2
There were significant main effects of group (F_(1, 46)_ = 10.6, p = .002), emotion (F_(2,80)_ = 35.7, p <.001), and a significant group*emotion interaction (F_(2, 80)_ = 5.1, p = .01). Pairwise comparisons indicated that HCs compared to BPD showed higher hit rates (p = .002), confirming Hypothesis 1. Further, happy faces were identified with higher accuracy compared to neutral (p <.001) and sad (p <.001) facial expressions, but there was no significant difference between neutral and sad faces (p = .5).
The group*emotion interaction revealed that the main effect of group was driven by the lower hit rate in sad faces in the BPD vs. HC group (p = .002), whereas there were no differences between mothers with BPD and HCs in happy (p = .36) and neutral (p = .23) faces.
Behavioral results, hypothesis 2: association between affect recognition and non-hostility
3.3
None of the correlations between hit rates or RTs in the affect recognition task of sad faces with maternal non-hostility were significant after correcting for multiple comparisons (p values >.16), disconfirming Hypothesis 2.
FMRI results, hypothesis 3: group differences in ToM network activation when seeing own vs. unknown sad children
3.4
For the HC > BPD contrast of own > unknown sad child faces, we observed a non-significant (ROI p_FWE_ = .28) activation within the left dmPFC (x = -12, y = 50, z = 30; t = 3.6), disconfirming Hypothesis 3. In the reversed BPD > HC contrast of own > unknown sad children, no group differences in ToM network activation emerged.
fMRI results, Hypothesis 4: association between ToM network activation and maternal non-hostility
3.5
In mothers with and without BPD, associations between higher non-hostility scores and brain activation while viewing sad faces of their own vs. unknown children were significant for the left TPJ (x = -50, y = -44, z = 28; T = 4.52; ROI p_FWE_ = .03), right TPJ (x = 52, y = -44, z = 22; T = 4.44; ROI p_FWE_ = .04), and left dmPFC (x = -16, y = 58, z = 20; T = 4.39, ROI p_FWE_ = .05), confirming Hypothesis 4 (Figure 2).
Upper part: activation in the left temporoparietal junction (lTPJ; x = -50, y = -44, z = 28) associated with maternal non-hostility, measured with the emotional availability scales (60); middle part: activation in the right temporoparietal junction (rTPJ; x = -50, y = -44, z = 28) associated with maternal non-hostility; lower part: activation in the left dorsomedial prefrontal cortex (dmPFC; x = -16, y = 58, z = 20) associated with maternal non-hostility. For illustration purposes, masks of the activated clusters were used and activations are overlaid on the Montreal Neurological Institute (MNI152) template embedded in MRIcroGL software (61). For illustration purposes only, beta values were exported from the mean activations of the respective activated cluster and correlated off-line with non-hostility ratings.
To explore if the association between ToM network activation and maternal behavior was driven by differences in positive parenting behavior, we regressed maternal sensitivity during the mother-child interaction on ToM network activation but found no significant relationship (T < 3.69, ROI p_FWE_ >.23).
There were no activations significantly associated with maternal non-hostility in the precuneus or PCC.
Discussion
4
Mothers with borderline personality disorder (BPD) and healthy control (HC) mothers in our sample showed overall high scores of non-hostility falling in the range of covert, subtle signs of irritability, anger, or boredom (8, 9), but HCs were rated more non-hostile than mothers with BPD.
Our hypothesis that mothers with BPD vs. HCs would show longer response times and lower accuracies in the inside-scanner affect recognition task with sad, neutral, and happy faces of their own vs. unknown children, was confirmed by our data, indicating impaired child affect recognition in BPD. For hit rates, an interaction between group and emotion indicated that the effect was mainly driven by lower performance for sad faces in mothers with BPD compared to HCs, whereas happy and neutral faces were recognized with equal accuracy across groups. In the pooled group of mothers with BPD and HCs, consistent with our hypotheses, maternal non-hostility was positively associated with activation in the bilateral temporoparietal junction (TPJ) and dorsomedial prefrontal cortex (dmPFC), key regions of the ToM network, when viewing sad faces of their own versus unknown children.
Contrary to our hypotheses, we found no significant association between maternal ToM ability in the affect recognition task with sad faces and maternal non-hostility, and no significant group differences between mothers with BPD and HCs in ToM brain network activation while seeing sad faces of own vs. unknown children.
Behavioral findings
4.1
Mothers with BPD showed a reduced ability to understand children’s facially expressed emotions. Stepp et al. (62) suggest that mothers with BPD have difficulties understanding and regulating their own and their children’s emotions, possibly leading to higher ambiguity in emotional social interactions. Problems in dealing with other individuals’ emotional expressions is further implied by studies showing that individuals with BPD have difficulties in understanding the feelings of others (63) and find emotionally loaded social situations more overwhelming than HCs (64). The findings of the present study support this view. Possibly, in social interactions with their children, mothers with BPD find it harder than HCs to understand their child’s feelings, causing higher ambiguity and possibly, higher parenting stress (65). As indicated by an interaction between group and emotion showing difficulties of mothers with BPD in identifying sad faces, this might be most prevalent in situations where their children are sad.
However, we found no association between affect recognition performance and maternal non-hostility. This absence of a direct correlation suggests that the basic ability to recognize a sad face may be too distant from the complex demands required for displaying non-hostile parenting behavior during real-life interaction. In a study by Kiel et al. (66), mothers with BPD showed the same negative affect towards their child’s distress as HCs in the strange situations test but were less likely to engage in positive soothing behavior. Therefore, the difference may lie not in emotion recognition itself but in the downstream expression, regulation, or utilization of emotions to maintain positive behavior.
Future studies should employ more faceted, naturalistic affective ToM tasks. Further, studying mother-child social interactions might benefit from employing more emotionally salient stimuli such as infant and child crying, as these are expected to elicit stronger maternal emotional responses (67, 68).
Neural correlates of maternal non-hostility
4.2
Our results suggest that a neural correlate of non-hostile parenting behavior is increased activation of the mothers’ ToM network when viewing their own sad children. This association was found specifically for maternal non-hostility, not maternal sensitivity, highlighting the role of ToM processes, specifically affective ToM, in reducing dysfunctional parenting behavior. The regions found to be associated with non-hostility, the TPJ and dmPFC, have previously been shown to be associated with social cognition in close relationships (69). TPJ activation was, for example, shown to be positively related to self-reported parental empathy, meaning empathy with the participants’ children versus empathy in general (70). A dismissive attachment style was associated with lower TPJ activation during the reading the mind in the eyes test, an affect recognition task often implicated in affective ToM (71). Wever et al. (72) found the TPJ and dmPFC to be associated with empathy with the participants’ own versus unfamiliar children. The dmPFC is thought to play an important role in mentalizing processes (73), possibly enabling individuals to represent the intentions of others (74).
Together with the previous literature, our results suggest that mothers who respond in a non-hostile manner when interacting with their children show stronger activation of the TPJ and dmPFC when seeing their child displaying sadness. The role of these brain regions in maternal care is suggested (75). Further, this is compatible with the notion that interpersonal problems in mother-child relationships of mothers with BPD are partly explainable by maternal affective ToM.
We found no significant group differences between mothers with BPD and HCs in ToM network activation while seeing the sad faces of own vs. unknown children. Activation of the ToM network might be related to BPD symptoms in ways not covered by a group contrast. For example, when comparing brain activation upon seeing their own children in mothers with early life maltreatment versus non-maltreated mothers, Neukel et al. (47) reported heightened activation in ToM-related regions of the brain. Boehme et al. (76) found increased social anxiety to be related with increased TPJ and dmPFC activation in self-referential thinking. Beeney et al. (77) also reported greater activation in BPD compared to HCs in the TPJ, dmPFC, precuneus, and cingulate cortex when participants were asked to evaluate themselves. Possibly, in the present study, different symptom constellations in our BPD patients might have led to different, counteracting alterations in the ToM network activation. Alternatively, the absence of a group difference might be attributable to the small sample size, as group analyses are especially prone to power issues (78).
Clinical implications
4.3
The association between ToM network activation upon seeing own sad children and maternal non-hostility implies affective ToM as a potential intervention target in parents at risk for dysfunctional parenting behavior. Interventions targeting social abilities are being developed for parents and their families (79). For example, Volkert et al. (80) present a parent training directed at severely mentally ill parents that constitutes an adaptation of the lighthouse parent training against childhood maltreatment (81) interlaced with mentalization-based psychotherapy (82). Mentalization is conceptualized as the ability to represent the mental states of oneself and others and understanding current feelings and behaviors as an expression of these mental states (82).
Previous studies demonstrate that by psychotherapeutic interventions, specific neural processes can be strengthened (31, 83). For instance, in patients with bipolar disorder, Meyer et al. (31) demonstrated that a psychotherapeutic intervention with a practical focus on social functioning and perspective-taking increased the neural activation in the ToM network post-therapy. Pre- and post-intervention fMRI studies are needed to better understand the role of the ToM brain network in improving parent-child interactions.
Strengths and limitations
4.4
The major limitation of the present study is its small sample size, especially in the BPD group, which renders the results preliminary and limits the generalizability of the findings. Further, it is possible that fluctuating mood states in the mothers with BPD influenced the association between ToM network activation and maternal non-hostility. Repeated measurements are warranted in future research, as they would allow for stronger conclusions regarding causality, which the current cross-sectional data do not permit.
The strengths of the study lie in its integration of different data sources (observational, experimental, neuroimaging) and the use of stimuli based on images of the participants’ own children. Pooling BPD and HC groups for the regression had the advantages of increasing the variance in maternal non-hostility observed in interactions and improving the power over studying the groups separately but prevented us from detecting group-specific effects.
As described in Table 1, the BPD sample of the current study reported low intake of medication relative to many other patients with BPD (84), a possible consequence of the psychotherapeutic as opposed to pharmacological treatment approach of our clinic, where many of the patients were recruited, and of the exclusion of patients with current depression scores above a clinical cut-off from participation. This low intake of medication has the advantage of reducing the effect of the pharmacotherapy on brain activation.
Conclusion
4.5
Mothers with BPD showed difficulties recognizing facial emotion expressions compared to HCs. Maternal non-hostile behavior was related to higher bilateral TPJ and left dmPFC activation, indicating that mothers who showed more non-hostility while playing with their children employed their ToM network more strongly when seeing their own sad children. This finding underscores the relevance of affective ToM in parenting behavior and may suggest that targeting affective ToM therapeutically could benefit parent-child interaction quality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Psychiatric Association . Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.). Arlington, VA: American Psychiatric Publishing, Inc. (2013). doi: 10.1176/appi.books.9780890425596 · doi ↗
- 2Lis S Bohus M . Social interaction in borderline personality disorder. Curr Psychiatry Rep. (2013) 15:1–7. doi: 10.1007/s 11920-012-0338-z, PMID: 23307561 · doi ↗ · pubmed ↗
- 3Weinbrecht A Niedeggen M Roepke S Renneberg B . Feeling excluded no matter what? Bias in the processing of social participation in borderline personality disorder. Neuro Image: Clinical. (2018) 19:343–50. doi: 10.1016/j.nicl.2018.04.031, PMID: 30013917 PMC 6044182 · doi ↗ · pubmed ↗
- 4Petfield L Startup H Droscher H Cartwright-Hatton S . Parenting in mothers with borderline personality disorder and impact on child outcomes. BMJ Ment Health. (2015) 18:67–75. doi: 10.1136/eb-2015-102163, PMID: 26205740 PMC 11234925 · doi ↗ · pubmed ↗
- 5Florange JG Herpertz SC . Parenting in patients with borderline personality disorder, sequelae for the offspring and approaches to treatment and prevention. Curr Psychiatry Rep. (2019) 21:1–8. doi: 10.1007/s 11920-019-0996-1, PMID: 30729325 · doi ↗ · pubmed ↗
- 6Macfie J Swan SA . Representations of the caregiver–child relationship and of the self, and emotion regulation in the narratives of young children whose mothers have borderline personality disorder. Dev psychopathology. (2009) 21:993–1011. doi: 10.1017/S 0954579409000534, PMID: 19583894 PMC 2825084 · doi ↗ · pubmed ↗
- 7Feldman RB Zelkowitz P Weiss M Vogel J Heyman M Paris J . A comparison of the families of mothers with borderline and nonborderline personality disorders. Compr Psychiatry. (1995) 36:157–63. doi: 10.1016/S 0010-440X(95)90110-8, PMID: 7758301 · doi ↗ · pubmed ↗
- 8Biringen Z Derscheid D Vliegen N Closson L Easterbrooks MA . Emotional availability (EA): Theoretical background, empirical research using the EA Scales, and clinical applications. Dev review. (2014) 34:114–67. doi: 10.1016/j.dr.2014.01.002 · doi ↗