Prevalence and risk factors for carbapenem-resistant Enterobacterales colonization in hospitalized children in a provincial hospital in Vietnam
Van Anh Thi Dinh, Nhung Nguyen Thi Trang, Ngoc Duc Vo, Ngoc Hoang Thi Bich, Dien M. Tran, Pham Duc Phuc, Son Luong Duc, Do Manh Dung, Flavie Goutard, Thirumalaisamy P. Velavan, Dennis Nurjadi, Yaovi M. G. Hounmanou, Bent Jörgensen, Le Huu Song, Truong Nhat My, Etienne Loire

TL;DR
This study found that CRE colonization is common in hospitalized children in Vietnam, especially in intensive care units and among those hospitalized for longer periods.
Contribution
The study provides new insights into CRE colonization risk factors in a high antimicrobial resistance setting in Vietnamese pediatric hospitals.
Findings
CRE colonization was detected in 28.2% of hospitalized children.
Hospitalization for more than 48 hours increased the risk of CRE colonization by 2.27-fold.
The highest CRE colonization rates were observed in the Intensive Care Unit (77.8%).
Abstract
Carbapenem-resistant Enterobacterales (CRE) colonization is an important prerequisite to hospital-acquired infections (HAIs) caused by CRE and increased mortality. This study assessed the prevalence of, and risk factors for, CRE colonization among children admitted to a provincial pediatric hospital in a high–antimicrobial-resistance setting in Vietnam. A point prevalence survey was conducted on 15 August 2022 at a provincial pediatric hospital in the Red River Delta. Rectal swabs were collected from 376 hospitalized children after informed consent. Samples were inoculated on chromogenic selective agar for CRE detection, and bacterial identification and antimicrobial susceptibility testing were performed using the VITEK® 2 system. Clinical and demographic data were obtained from structured questionnaires and medical records. Logistic regression analyses were used to identify risk…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
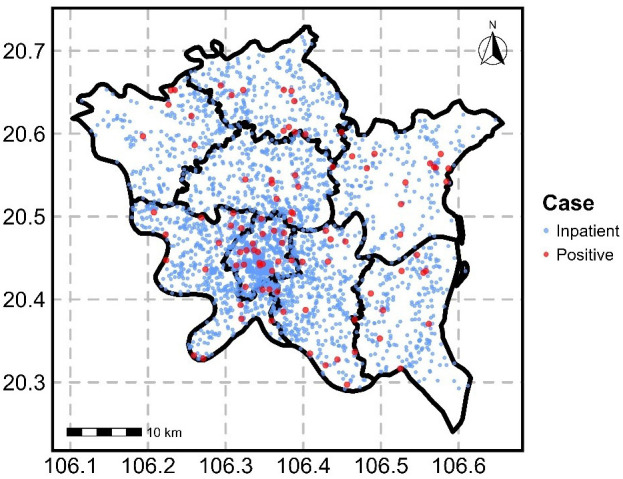 Figure 1
Figure 1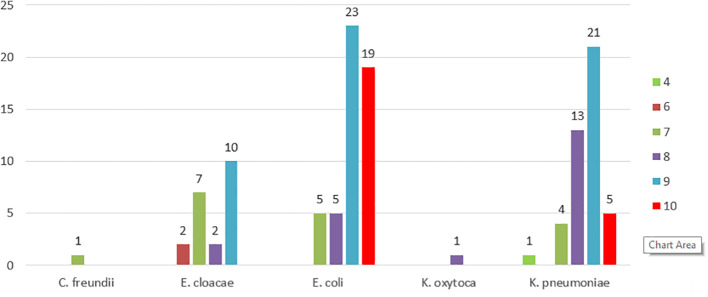 Figure 2
Figure 2| Characteristic | Number of patients with negative CRE | Number of patients with positive CRE | Total |
|---|---|---|---|
| Age group | |||
| ≤ 6 years | 242 (70.3%) | 102 (29.7%) | 344 |
| > 6 years | 28 (87.5%) | 4 (12.5%) | 32 |
| ≤ 3 years | 205 (69.7%) | 89 (30.3%) | 294 |
| Gender | |||
| Male | 170 (71.1%) | 69 (28.9%) | 239 |
| Female | 99 (73.3%) | 36 (26.7%) | 135 |
| Missing data | 1 (50%) | 1 (50%) | 2 |
| Referral source | |||
| Other hospital | 0 (0%) | 3 (100%) | 3 |
| Other department | 11 (100%) | 0 (0%) | 11 |
| Lower-level medical facility | 20 (80%) | 5 (20%) | 25 |
| Direct from home | 220 (70.1%) | 94 (29.9%) | 314 |
| No data | 19 (82.6%) | 4 (17.4%) | 23 |
|
| 22 (61.1%) | 14 (38.9%) | 36 |
| Normal delivery | 14 (63.6%) | 8 (36.4%) | 22 |
| Caesarean section | 6 (50%) | 6 (50%) | 12 |
| Missing data | 2 (100%) | 0 (0%) | 2 |
| Timing of carbapenem screening | |||
| ≤ 48 hours after admission | 58 (82.9%) | 12 (17.1%) | 70 |
| > 48 hours after admission | 211 (69.2%) | 94 (30.8%) | 305 |
| Missing data | 1 (100%) | 0 (0%) | 1 |
| Length of stay ≥ 7 days | 74 (59.2%) | 51 (40.8%) | 125 |
|
|
|
|
|
| Department | Neg | Pos | Total |
|---|---|---|---|
| ICU | 4 (22.2%) | 14 (77.8%) | 18 |
| 3 specialities (Ophthalmology; Odonto-Stomatology and Maxillofacial Surgery; Otorhinolaryngology) | 9 (56.3%) | 7 (43.7%) | 16 |
| Neonatal | 22 (61.1%) | 14 (38.9%) | 36 |
| Respiratory | 42 (65.6%) | 22 (34.4%) | 64 |
| Infectious Diseases | 21 (65.6%) | 11 (34.4%) | 32 |
| Traditional medicine | 9 (69.2%) | 4 (30.8%) | 13 |
| Gastroenterology | 22 (75.9%) | 7 (24.1%) | 29 |
| Cardiology | 13 (76.5%) | 4 (23.5%) | 17 |
| Nephrology - Urology | 36 (83.7%) | 7 (16.3%) | 43 |
| Pediatrics | 51 (82.3%) | 11 (17.7%) | 62 |
| Emergency | 13 (86.7%) | 2 (13.3%) | 15 |
| Trauma | 19 (90.5%) | 2 (9.5%) | 21 |
| Nutrition | 9 (90%) | 1 (10%) | 10 |
|
|
|
|
|
| Department | CRE-positive patients (n) | Total isolate (n) |
|
|
|
|
| Other # (%) |
|---|---|---|---|---|---|---|---|---|
| Respiratory | 22 | 28 | 12 (42.9%) | 12 (42.9%) | 2 (7.1%) | 2 (7.1%) | ||
| Neonatal | 14 | 17 | 4 (23.5%) | 6 (35.3%) | 6 (35.3%) | 1 (5.9%) | ||
| ICU | 14 | 20 | 7 | 8 | 2 | 3 (15%) | ||
| Infectious Diseases | 11 | 12 | 4 (33.3%) | 4 (33.3%) | 4 (33.3%) | 0 (0%) | ||
| General Internal Medicine | 11 | 13 | 5 (38.5%) | 5 (38.5%) | 2 (15.4%) | 1 (7.6%) | 0 (0%) | |
| Nephrology – Urology | 7 | 9 | 4 (44.4%) | 2 (22.2%) | 1 (11.1%) | 2 (22.2%) | ||
| 3 Specialities | 7 | 7 | 3 (42.9%) | 2 (28.5%) | 1 (14.3%) | 1 (14.3%) | ||
| Gastroenterology | 7 | 8 | 4 | 0 | 3 (37.5%) | 1 (12.5%) | ||
| Cardiology | 4 | 4 | 4 (100%) | 0 | 0 | 0 (0%) | ||
| Traditional medicine - Rehabilitation | 4 | 4 | 2 | 2 | 0 | 0 (0%) | ||
| Trauma | 2 | 2 | 1 | 1 | 0 | 0 (0%) | ||
| Emergency | 2 | 3 | 2 (66.7%) | 1 (33.3%) | 0 | 0 (0%) | ||
| Nutrition | 1 | 1 | 0 | 1 (100%) | 0 | 0 (0%) | ||
|
|
|
|
|
|
|
|
|
|
| Antimicrobial group/agent |
|
|
|
|---|---|---|---|
| Aminoglycoside (gentamicin/amikacin) | 26 (50%) | 37 (84.1%) | 16 (76.2%) |
| Antipseudomonal penicillins + β-lactamase inhibitors (piperacillin-tazobactam) | 50 (96.2%) | 44 (100%) | 21 (100%) |
| Carbapenems (ertapenem/meropenem) | 52 (100%) | 44 (100%) | 21 (100%) |
| Non-extended spectrum cephalosporins; 1st and 2nd generation (cefuroxime) | 52 (100%) | 43 (97.7%) | 21 (100%) |
| 3rd-4th generation cephalosporin (cefotaxime/cefepime/ceftazidime) | 50 (96.2%) | 43 (97.7%) | 21 (100%) |
| Cephamycins (Cefoxitin) | 50 (96.2%) | 43 (97.7%) | 21 (100%) |
| Fluoroquinolones (ciprofloxacin) | 47(90.1%) | 43 (97.7%) | 20 (95.2%) |
| Folate pathway inhibitors (trimethoprim-sulphamethoxazole) | 41 (78.8%) | 24 (54.5%) | 13 (61.9%) |
| Penicillins (ampicillin)* | 52 (100%) | Not tested | Not tested |
| Penicillins + β-lactamase inhibitors (amoxicillin-clavulanic acid)* | 52 (100%) | 44 (100%) | Not tested |
| Phosphonic acids (fosfomycin) | 2 (3.8%) | 12 (27.3%) | 15 (71.4%) |
| MDR phenotype (combined resistance to 3rd generation cephalosporins, fluoroquinolones, and aminoglycosides) | 23 (44.2%) | 35 (79.5%) | 16 (76.2%) |
| Characteristic | n | cOR (95%CI) | p -value | aOR (95%CI)+ | p-value |
|---|---|---|---|---|---|
| Age group | |||||
| > 6 years (reference) | 32 | 1.00 | 1 | ||
| ≤ 6 years | 342 | 2.93 (1.00 - 8.58) | 0.049 | 2.7 (0.86 - 8.47) | 0.090 |
| Time from admission to CRE screening | |||||
| ≤ 48 hours (reference) | 69 | 1.00 | 1 | ||
| > 48 hours | 305 | 2.35 (1.18 - 4.68) | 0.015 | 2.27 (1.1 - 4.67) | 0.026 |
| Diagnosis at time of study | |||||
| Other diagnoses (reference) | 90 | 1,00 | 1 | ||
| Lower respiratory tract infection | 216 | 1.68 (0.94 - 3.01) | 0.081 | 1.4 (0.74 - 2.64) | 0.303 |
| Upper respiratory tract infection | 31 | 1.78 (0.72 - 4.41) | 0.213 | 1.52 (0.58 - 3.97) | 0.392 |
| Sepsis | 10 | 5.61 (1.44 - 21.9) | 0.013 | 6.54 (1.55 - 27.64) | 0.011 |
| Diarrhea | 27 | 0.47 (0.13 - 1.72) | 0.252 | 0.48 (0.13 - 1.85) | 0.289 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Antibiotic Use and Resistance · Nosocomial Infections in ICU
Highlights
Carbapenem-resistant Enterobacterales (CRE) pose a major public health threat due to limited treatment options and their association with prolonged hospitalization and poor clinical outcomes.A point prevalence survey in a provincial pediatric hospital in Vietnam found a 28.2% prevalence of CRE colonization among hospitalized children.Colonization was highest among neonates and children admitted to intensive care units.Key risk factors for CRE colonization included hospitalization for >48 hours and age ≤6 years, and admission to ICU or neonatal units.The findings underscore the urgent need to strengthen infection prevention and control measures in low- and middle-income settings to reduce in-hospital CRE transmission and potential household dissemination after discharge.
Introduction
Carbapenem-resistant Enterobacterales (CRE) are recognized as among the most critical priority antimicrobial resistant pathogens and represent a major global threat to human health and antimicrobial resistance. Their emergence is particularly concerning in inpatient settings, where vulnerable patients and high antimicrobial use facilitate selection and transmission, underscoring the need for robust infection prevention and control (IPC) strategies (World Health, O, 2017). CRE prevalence varies considerably across healthcare environments, ranging from 1% to 30.4% in long-term care facilities in the United States and from 13% to 22.7% across Asian hospitals (Chen et al., 2021). In a neonatal intensive care unit (NICU) in Shanghai, China, the CRE colonization rate reached 11.7% during 2017–2018 (Yin et al., 2021).
In Vietnam, carbapenems have been used clinically since 2008 (Nguyen et al., 2013), and increasing reports of carbapenem-resistant organisms—including strains producing NDM-1—reflect the growing burden of resistance nationwide (Hoang et al., 2013; Tran et al., 2015). A multicenter survey involving 12 hospitals showed that 52% of screened patients were colonized with CRE, with prevalence rising from 13% at admission to 89% by hospital day 15; in one provincial pediatric hospital, carriage increased from 29% to 53% over a 16-month period (Tran et al., 2019). These data highlight both high background colonization pressure and rapid in-hospital acquisition.
A national survey of Vietnamese intensive care units reported HAIs in 30% of approximately 5,000 admitted patients (Le et al., 2016), and mortality among neonates with culture-confirmed HAIs caused by carbapenem-resistant Gram-negative bacteria exceeded 50% (Peters et al., 2019). CRE colonization is a prerequisite to subsequent invasive infection. Clearance of colonization is protracted, with median persistence of roughly one year, and prolonged carriage was associated with therapeutic antimicrobial exposure (Kramer et al., 2013).
High CRE colonization rates at discharge raise concerns about onward dissemination to household members, the community, and the environment. Such transmission may further complicate the management of community-onset infections, including urinary tract infections that may fail standard empirical therapy, even when treated with intravenous agents such as amikacin. Evidence from a longitudinal study of extended-spectrum β-lactamase (ESBL)-producing Enterobacterales demonstrated high within-household transmission probabilities - 67% from index patient to household contact and 37% in the reverse direction - and prolonged carriage associated with antibiotic exposure (Haverkate et al., 2017). Although focused on ESBL organisms with resistance to third generation cephalosporins, these findings underscore the potential for similar dynamics for CRE.
Early and accurate detection of CRE colonization is critical for IPC, outbreak containment, and guiding clinical management, particularly in high-risk units such as NICUs and ICUs (Zaidah et al., 2017). This study aimed to determine the prevalence and risk factors for CRE colonization among children hospitalized in a provincial pediatric hospital in Vietnam. The findings are intended to inform the development and implementation of targeted strategies to mitigate CRE transmission within healthcare facilities and reduce dissemination to the community.
Methods
Setting
The study was conducted at a provincial pediatric hospital in the Red River Delta, a densely populated region of northern Vietnam (1,185 inhabitants/km² in 2022) (United Nations and General Statistics Office Vietnam, 2024). The hospital provides comprehensive pediatric care, with 600 inpatient beds and 25,620 admissions in 2022, and hosts an on-site microbiology laboratory capable of performing culture, identification, and antimicrobial susceptibility testing. The mean inpatient stay was 7.4 days, with substantially longer durations in the Neonatal, Intensive Care, and Respiratory Departments (22.9, 10.6, and 7.9 days, respectively). In 2022, 71 hospital-acquired infections (HAIs) were recorded, highlighting the importance of strengthening infection prevention and control (IPC) measures (Appendix 3). Given previously documented high CRE colonization rates and the hospital’s commitment to IPC improvement, the facility was selected as a study site within the randomized controlled trial entitled Interventions to Reduce CRE Colonization and Transmission Across Hospitals, Households, Communities, and Domesticated Animals.
Study population
All inpatients <18 years of age admitted to any of the 13 clinical departments were eligible for inclusion. A total of 376 caregivers provided written informed consent for participation and specimen collection.
Study design
A cross-sectional point prevalence survey study was conducted on August 15, 2022.
Data collection
Data were collected using a structured questionnaire with coded identifiers to ensure confidentiality. Informed consent was obtained from caregivers prior to enrolment. Trained clinicians conducted interviews and extracted clinical information from medical records.
Collected data included: 1) Household characteristics: address, number of household members, animal husbandry practices, household conditions, water source, and reported antimicrobial use; 2) Clinical information: age, sex, diagnosis at admission, symptoms, admission and discharge dates, hospital department, source of referral, prior antimicrobial exposure, and previous hospitalizations; 3) Microbiological samples: faucal specimens obtained using rectal swabs.
Microbiological methods
Rectal swabs were collected using sterile cotton swabs and delivered to the hospital microbiology laboratory within two hours. Samples were inoculated onto MELAB Chromogenic Carba agar (Lavitec, Vietnam), a locally manufactured equivalent of CHROMagar™ mSuperCARBA™, for CRE screening (Lavitec, [[NoYear]]) Plates were subsequently transported within two hours to the Vietnam National Children’s Hospital for incubation at 35 ± 2°C for 18–24 hours.
Bacterial isolates were identified to species level and tested for antimicrobial susceptibility using the VITEK^®^ 2 XL system (bioMérieux, France). Susceptibility testing included agents across 11 antimicrobial classes: aminoglycosides; fluoroquinolones; antipseudomonal penicillins with β-lactamase inhibitors; carbapenems; non-extended-spectrum cephalosporins; first- and second-generation cephalosporins; cephamycins; third- and fourth-generation cephalosporins; penicillins; penicillins with β-lactamase inhibitors; phosphonic acids; and folate-pathway inhibitors. AST interpretation followed current Clinical and Laboratory Standards Institute (CLSI) breakpoints (Clinical and Laboratory Standards Institute, C, 2021). All isolates were stored at –80°C for future analyses.
Multidrug resistance (MDR) was defined according to Magiorakos (Magiorakos et al., 2012): non-susceptibility to ≥1 agent in ≥3 antimicrobial classes.
Statistical analysis
Data analysis was conducted using R Statistical Software (v4.5.1; R Core Team 2025). Descriptive statistics summarized demographic and clinical characteristics. Visualizations were produced with the ggplot2 package (v4.0.0).
Multivariable logistic regression was used to identify risk factors for CRE colonization. Covariates included age, sex, diagnosis at the time of the survey, prior antimicrobial exposure, residential address, time to detection after hospital administration, and previous hospitalization. Associations were expressed as crude odds ratios (ORs) from univariate analyses and adjusted ORs from multivariable models. Statistical significance was defined as p < 0.05.
Quality control
Standardized training was provided to all data collectors and laboratory personnel to ensure methodological consistency and accuracy. Laboratory procedures at the Vietnam National Children’s Hospital microbiology department adhere to ISO 15189 standards.
Ethical considerations
Ethical approval for this study and the overarching I-CRECT project (“Intervention to Decrease CRE Colonization and Transmission Between Hospitals, Households, Communities and Domesticated Animals”) was obtained from Ministry of Health, Vietnam, and performed after ethical approval from Ethical Review Board of Vietnam Children’s Hospital (approval code VNCH-TRICH-2022–87 dated 30th September, 2022 issued by Vietnam Ministry of Health and Ethical Review Board of Hanoi University of Public Health (approval code 022-350/DD-YTCC, 25 July, 2022).
Results
Among the 376 hospitalized children included in the survey, the overall prevalence of CRE colonization was 28.2% (Table 1). Children ≤6 years accounted for most of the study population (344/376, 91.5%) and had a higher prevalence of colonization (29.7%) compared with those >6 years (12.5%). Similarly, children ≤3 years exhibited a CRE prevalence of 30.3%. CRE colonization did not differ markedly by sex, with colonization observed in 28.9% of males and 26.7% of females.
Most patients had been admitted directly from home (314/376), and this group showed a colonization prevalence of 29.9%. In contrast, children transferred from other hospitals or lower-level medical facilities had smaller sample sizes but also demonstrated notable colonization rates. (please see Table 1).
CRE colonization was 17.1% of among children screened within 48 hours of admission, and 30.8% after 48 hours. The highest prevalence was observed in patients with stays ≥7 days, 40.8% of whom were colonized. In the neonatal subgroup, CRE prevalence reached 38.9%. Overall, these findings indicate substantial colonization pressure across age groups and admission pathways, with markedly increased prevalence associated with prolonged hospitalization.
The prevalence of CRE colonization varied markedly across hospital departments (Table 2). The highest prevalence was observed in the Intensive Care Unit, where 77.8% of patients were colonized. High rates of colonization rates were also seen in the 3 Specialities Department (43.7%), the Neonatal Department (38.9%), and the Respiratory and Infectious Diseases Departments (both 34.4%). In contrast, substantially lower rates were found in the Trauma (9.5%), Nutrition (10.0%), and Emergency (13.3%) Departments. Intermediate prevalence levels were reported in Gastroenterology (24.1%), Cardiology (23.5%), and Nephrology–Urology (16.3%). These findings indicate substantial differences in CRE burden across clinical areas, with intensive care and neonatal services representing the highest-risk settings.
A total of 128 CRE isolates were recovered from 106 colonized patients, corresponding to an average of 1.2 isolates per patient (Table 3). Escherichia coli was the most frequently identified species (40.6%), followed by K. pneumoniae (34.4%) and E. cloacae (16.4%). Species distribution varied across departments. In the ICU, E. coli and K. pneumoniae predominated, together accounting for 75% of isolates, while Pseudomonas spp. constituted an additional 15%. In the Neonatal Department, K. pneumoniae and E. cloacae were equally common (both 35.3%). Respiratory wards showed a similar dominance of E. coli and K. pneumoniae (each 42.9%). Less commonly isolated species included K. oxytoca, Citrobacter freundii, Aeromonas sobria, Acinetobacter spp., and Brevundimonas diminuta. These findings indicate that the CRE reservoir in the hospital is primarily composed of E. coli and K. pneumoniae, with notable departmental variation suggesting multiple ecological niches for CRE persistence and transmission.
Antimicrobial susceptibility patterns showed uniformly high resistance across CRE species (Table 4). All E. coli, K. pneumoniae, and E. cloacae isolates demonstrated 100% resistance to carbapenems and near-panresistance to 1st- and 2nd-generation cephalosporins, 3rd- and 4th-generation cephalosporins, cephamycins, and piperacillin–tazobactam. Fluoroquinolone resistance was also high, ranging from 90.1% in E. coli to 97.7% in K. pneumoniae. Aminoglycoside resistance was common, particularly among K. pneumoniae (84.1%). Fosfomycin resistance varied by species, from low levels in E. coli (3.8%) to high levels in E. cloacae (71.4%). Multidrug resistance (MDR), defined as combined resistance to 3rd-generation cephalosporins, fluoroquinolones, and aminoglycosides, was most prevalent in K. pneumoniae (79.5%) and E. cloacae (76.2%). Overall, the isolates exhibited extensive resistance across nearly all tested antimicrobial classes, leaving very limited therapeutic options.
Multivariable analysis identified several significant risk factors for CRE colonization (Table 5). Children screened more than 48 hours after admission had more than twice the odds of being colonized compared with those screened within 48 hours (aOR 2.27, 95% CI 1.10–4.67, p = 0.026), indicating high in-hospital acquisition. Age ≤6 years was associated with higher colonization in crude analysis (cOR 2.93, p = 0.049), although this association did not remain statistically significant after adjustment. Sepsis at the time of the survey was strongly associated with CRE colonization, with affected children having more than sixfold increased odds to be CRE colonized compared with those with other diagnoses (aOR 6.54, 95% CI 1.55–27.64, p = 0.011). Unfortunately, data obtained did not allow us to determine whether patients had sepsis due to CRE or were septic due to other causes and colonized with CRE. Other diagnostic categories, including respiratory infections and diarrhea, did not show significant associations to CRE colonization. Overall, prolonged hospitalization and severe systemic illness emerged as the strongest predictors of CRE colonization in this cohort.
Discussion
In this point prevalence survey (PPS), we found a CRE colonization rate of 28.2% among hospitalized children in a provincial pediatric hospital. Colonization was particularly common in high-risk units, with prevalence of 77.8% in the ICU, 43.7% in the 3 Specialities Department, 38.9% in the Neonatal Department, and 34.4% in the Respiratory Department, whereas the lowest rates were observed in the Nutrition (10%) and Trauma (9.5%) Departments. These findings are comparable to, and in some instances higher than, earlier reports from Viet Nam and other settings. At the Vietnam National Children’s Hospital, a cross-sectional survey conducted from March to June 2018 reported a CRE carriage rate of 35% among ICU inpatients (Garpvall et al., 2021). Most of those patients had previously been treated at lower-level healthcare facilities, including provincial pediatric or obstetric-paediatric hospitals (Garpvall et al., 2021). In an adult cohort from the Intensive Care–Toxicology Unit of Thai Binh Provincial General Hospital, the CRE carriage rate at admission was 41% (McConville et al., 2017). In contrast, rectal screening on admission to adult medical or surgical ICUs in the United States found a CRE colonization rate of 11% (Armin et al., 2023). At a university hospital in Thailand, the prevalence of CRE colonization at admission was 15.5% in 2022, and a cross-sectional study from Iran reported a CRE colonization prevalence of 37% among hospitalized children (van Loon et al., 2018). Taken together, our data add to the evidence that CRE carriage in healthcare facilities in low- and middle-income countries remains high and underline the urgent need for strengthened and targeted interventions.
Most confirmed CRE cases in our study (94/106; 88.7%) were detected more than 48 hours after admission, and hospitalization beyond 48 hours was associated with a 2.27-fold higher risk of CRE colonization compared with screening within 48 hours (p = 0.026). Thus, in-hospital acquisition was a major driver of CRE colonization in this setting. Length of hospital stay is a well-recognized risk factor for CRE colonization and infection, as patients are increasingly exposed to transmission via colonized or infected patients, contaminated environmental surfaces, and medical equipment (van Loon et al., 2018; Tran et al., 2019; Yen et al., 2023). The risk is amplified when hospitalization is prolonged because of severe disease or the need for invasive procedures—such as mechanical ventilation, central venous catheters, urinary catheters, or surgery—particularly in ICUs and neonatal units (van Loon et al., 2018; Tran et al., 2019; Yen et al., 2023). The high colonization pressure observed in our ICU and Neonatal Department is consistent with this pattern and reflects a combination of patient vulnerability and a challenging transmission environment.
In our study, most CRE-positive patients were admitted directly from home (travel by oneself) and were distributed across all districts and the provincial city (Table 1; Appendix 1). Our data from admission screening showed significant CRE colonization which increased during the hospital stay and which may further contribute to spread within the community after discharge. It also raises concern for increasing rates of community-onset infections—such as urinary tract caused by CRE, with consequent difficulties in selecting appropriate empirical antibiotics.
In our study, most CRE-positive patients were admitted directly from home and resided across all districts and the provincial city (Table 1; Appendix 1). High CRE prevalence was also observed among children diagnosed with sepsis at the time of the survey, and sepsis was associated with substantially higher odds of CRE colonization in multivariable analysis (adjusted OR = 6.54, 95% CI 1.55–27.64, p = 0.011). This distribution suggests that CRE colonization is not confined to a few geographic “hot spots” and raises concern both for household transmission after discharge and for spread to other healthcare facilities upon referral or readmission. It also points to a potential increase in community-onset infections, such as urinary tract caused by CRE, which may be difficult to treat empirically with standard regimens.
In this PPS, all identified CRE species showed high levels of resistance to multiple antibiotic classes (Appendix 2). Escherichia coli was the most common species (40.6%), followed by Klebsiella pneumoniae (34.4%) and Enterobacter cloacae (16.4%) (Table 3). The resistance profiles showed very high rates of non-susceptibility to carbapenems, extended-spectrum cephalosporins, fluoroquinolones, and β-lactam/β-lactamase inhibitor combinations (Table 4). CRE colonization is a recognized prerequisite to healthcare-associated infections (HAIs) caused by CRE and therefore represents a latent clinical risk: if infection occurs, therapeutic options are limited and the probability of treatment failure increases (Kramer et al., 2013; Tischendorf et al., 2016) These findings emphasize the importance of identifying colonized patients early and preventing progression to infection whenever possible.
To date, Viet Nam still lacks comprehensive national data on CRE carriage, particularly due with respect to low screening capacity and systematic sharing of data on CRE colonization status between facilities. Notification of CRE carriage at inter-facility transfer is not uniformly implemented across the country, which hampers coordinated infection prevention and control (IPC) measures. Early and accurate detection of CRE colonization is essential for identifying outbreaks and guiding IPC and treatment strategies (Zaidah et al., 2017). The cost of CRE screening depends on consumables, reagents, staff time, and local resource constraints and therefore differs between high-income and low- and middle-income countries (World Health Organization, 2019). For example, the average cost of a single CRE screening test was estimated at 8.65 in the United States ([Lin et al., 2022](#B10)). In contrast, in our study the material cost for one CRE screening plate was approximately 2, which could be used for two patients, thus a laboratory cost of about $1 per patient. Nonetheless, CRE screening is currently not reimbursed by health insurance and is not routinely performed in Vietnamese healthcare facilities, limiting its uptake despite its relatively low direct cost in this setting.
CRE screening and cohort care are widely recognized as key components of effective CRE control programs. At Vietnam National Children’s Hospital, admission screening of more than 900 children to three ICUs, followed by cohorting according to CRE status, reduced CRE acquisition from 90% to 48% (Garpvall et al., 2021). In Israel, a nationwide intervention combining CRE screening with cohort and isolation care significantly reduced CRE transmission (Schwaber and Carmeli, 2014). Our findings, together with these previous results, support the implementation of targeted screening strategies and cohort care in high-risk pediatric departments, particularly ICUs and neonatal units, as part of a broader IPC package.
This study has several limitations. First, it is based on a single PPS conducted in one provincial pediatric hospital, and thus not representative for Viet Nam. Nevertheless, the PPS provides a detailed snapshot of the wards studied and it may be relevant for similar provincial pediatric hospitals. Second, genotyping data are not presented here; however, a companion publication using the same isolate collection reported carbapenemase genes in 63.8% of isolates, with NDM being the predominant carbapenemase in 86.7% of CRE isolates (Pham et al., 2024). For the other 36.2% of isolates please see pham et al (Pham et al., 2024). Third, due to low reported HAI incidence and limited routine culture before starting antibiotics, we were unable to systematically link colonizing and clinical isolates and therefore could not quantify the progression from colonization to infection. Previous studies, however, have shown a strong association between CRE colonization and subsequent CRE HAI (Tischendorf et al., 2016). Finally, as a PPS, this study captures a single time point and does not account for temporal fluctuations in colonization pressure or the incidence of new acquisitions over time.
Conclusion
In summary, we report a high prevalence of CRE colonization among pediatric inpatients in a Vietnamese provincial hospital, with evidence of substantial in-hospital transmission and a predominance of multidrug-resistant E. coli, K. pneumoniae, and E. cloacae. The particularly high colonization rates in ICU and neonatal wards, and among children with prolonged hospital stay or sepsis, highlight priority targets for IPC interventions, CRE screening, and cohort care. These findings form an important baseline for the ongoing randomized controlled trial on interventions to reduce CRE colonization and transmission in hospitals, households, communities, and domesticated animals, and underscore the urgent need to strengthen CRE control strategies in pediatric healthcare settings in Vietnam.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Armin S. Azimi L. Shariatpanahi G. Shirvani A. Tehrani N. A . (2023). The prevalence of colonization with carbapenem-resistant enterobacteriaceae, escherichia coli, klebsiella and enterobacter, and related risk factors in children. Arch. Pediatr. Infect. Dis. 11, e 134518. doi: 10.5812/pedinfect-134518 · doi ↗
- 2Chen H. Y. Jean S. S. Lee Y. L. Lu M. C. Ko W. C. Liu P. Y. . (2021). Carbapenem-resistant enterobacterales in long-term care facilities: A global and narrative review. Front. Cell Infect. Microbiol. 11, 601968. doi: 10.3389/fcimb.2021.601968, PMID: 33968793 PMC 8102866 · doi ↗ · pubmed ↗
- 3Clinical and Laboratory Standards Institute, C (2021). Performance Standards for Antimicrobial Susceptibility Testing, M 100. 31st edition (Wayne, USA: Clinical and Laboratory Standard Institute). 10.1128/JCM.00213-21PMC 860122534550809 · doi ↗ · pubmed ↗
- 4Garpvall K. Duong V. Linnros S. Quốc T. N. Mucchiano D. Modeen S. . (2021). Admission screening and cohort care decrease carbapenem resistant enterobacteriaceae in Vietnamese pediatric ICU’s. Antimicrob. Resist. Infect. Control 10, 128. doi: 10.1186/s 13756-021-00994-9, PMID: 34462014 PMC 8404250 · doi ↗ · pubmed ↗
- 5Haverkate M. R. Platteel T. N. Fluit A. C. Cohen Stuart J. W. Leverstein-van Hall M. A. Thijs S. F. T. . (2017). Quantifying within-household transmission of extended-spectrum beta-lactamase-producing bacteria. Clin. Microbiol. Infect. 23, 46 e 1–46 e 7. doi: 10.1016/j.cmi.2016.08.021, PMID: 27596534 · doi ↗ · pubmed ↗
- 6Hoang T. H. Wertheim H. Minh N. B. Duong T. N. Anh D. D. Phuong T. T. L. . (2013). Carbapenem-resistant Escherichia coli and Klebsiella pneumoniae strains containing New Delhi metallo-beta-lactamase isolated from two patients in Vietnam. J. Clin. Microbiol. 51, 373–374. doi: 10.1128/JCM.02322-12, PMID: 23100353 PMC 3536186 · doi ↗ · pubmed ↗
- 7Kramer A. A. Higgins T. L. Zimmerman J. E. (2013). The association between ICU readmission rate and patient outcomes. Crit. Care Med. 41, 24–33. doi: 10.1097/CCM.0b 013e 3182657 b 8a, PMID: 23128381 · doi ↗ · pubmed ↗
- 8Lavitec Chromagar plate Melab diagnostics. 2023 [cited 2023 17/1]; Compoany profile with list of Chromagar plates]. Available online at: https://www.melab.vn/moi-truong-tao-mau (Accessed December 5, 2025).