Impact of Co-Mutations and Genetic Variations on Malignancy Risk in RAS-Positive Indeterminate Thyroid Nodules: an Institutional Experience
Lawrence Q. Wong, Zubair W. Baloch

TL;DR
This study shows that RAS mutations in thyroid nodules are more likely to be malignant when combined with other genetic changes, helping guide better diagnosis and treatment.
Contribution
The study identifies specific co-mutations that increase malignancy risk in RAS-positive thyroid nodules, improving risk stratification.
Findings
RAS mutations with additional genetic alterations are strongly linked to higher malignancy rates.
NRAS mutations are most common and often co-occur with EIF1AX and TERT mutations.
Isolated RAS mutations are more associated with benign or low-risk thyroid tumors.
Abstract
Mutations in RAS proto-oncogenes (NRAS, HRAS, KRAS) are common in thyroid nodules, though their prognostic significance remains unclear. This retrospective study analyzed 354 thyroid nodules from 346 patients (2018–2023) to investigate the clinical and pathological implications of isolated RAS mutations and RAS with co-occurring genetic alterations. Isolated RAS mutations were found in 41.0% (n = 145), while 54.8% (n = 194) had RAS with additional molecular alterations; NRAS was the most frequent subtype (62.1%). Among co-occurring mutations, EIF1AX (46.7%) and TERT (26.7%) were the most common, primarily in NRAS-positive cases. Surgical follow-up data from 302 cases revealed a malignancy rate of 52.3% (n = 158), with 60.1% (n = 95) being invasive encapsulated follicular variant of papillary thyroid carcinoma (IEFVPTC). NRAS mutations appeared in 64.6% of malignant cases. Isolated RAS…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
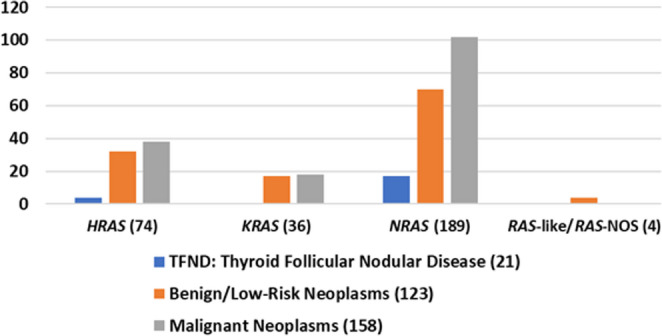 Figure 1
Figure 1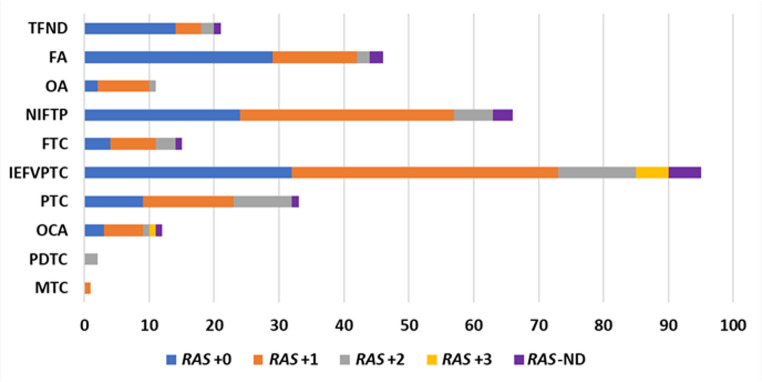 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid Disorders and Treatments · Thyroid and Parathyroid Surgery
Introduction
Thyroid cancer is the most common endocrine malignancy, with about 44,020 new cases annually in the U.S. alone [1]. Fine-needle aspiration (FNA) biopsy is essential for evaluating thyroid nodules, offering a minimally invasive method to assess malignancy risk. The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) was developed to standardize cytologic interpretation, ensuring consistent and clear communication across institutions [2]. While most nodules are clearly benign or malignant, some fall into indeterminate categories (e.g., atypia of undetermined significance (AUS), follicular neoplasm (FN), or suspicious for malignancy (SM)), where the cytologic results are inconclusive [3, 4]. These cases often lead to unnecessary surgeries, increased patient anxiety, and delayed treatment. To address this, next-generation sequencing (NGS) and molecular analysis are increasingly used to differentiate benign from malignant nodules [5]. ThyroSeq^®^ Genomic Classifier (GC) uses NGS to analyze 112 thyroid-related genes for mutations, fusions, copy number alterations, and gene expression changes linked to thyroid cancer [6]. ThyroSeq^®^ provides a personalized report that categorizes the nodule as either positive or negative for malignancy, detailing any genetic alterations and estimating malignancy risk. This advanced molecular profiling improves risk stratification in indeterminate cases and can help guide clinical decisions, potentially reducing unnecessary surgeries.
The RAS family mutations, including HRAS,* NRAS*, and KRAS, are among the most frequently observed genetic alterations in indeterminate thyroid nodules. Notably, these mutations can be found in both benign and malignant lesions upon surgical resection, underscoring their diagnostic ambiguity [7, 8]. The aim of this study is to retrospectively analyze thyroid FNA cases that tested positive for RAS mutations using the ThyroSeq^®^ Version 3 GC between 2018 and 2023. Data were collected on patient demographics, nodule characteristics, cytologic diagnoses based on TBSRTC, and corresponding surgical pathology outcomes. The primary objective is to evaluate the correlation between RAS mutation status and both cytologic interpretation and the final histopathologic diagnoses. By systematically reviewing these parameters, this study seeks to clarify the clinical significance of RAS mutations in indeterminate thyroid nodules, ultimately aiming to improve diagnostic accuracy, guide appropriate clinical management, and enhance prognostic assessment for affected patients.
Materials and methods
The study was approved by the University of Pennsylvania Health System Institutional Review Board. A retrospective search of our laboratory information system was performed to identify thyroid FNA cases with any RAS mutation identified on subsequent ThyroSeq^®^ V3 GC testing from 2018 to 2023 and relevant cytologic and/or surgical follow-up information. Follow-up in this study refers to the availability of cytology or surgical pathology at the time of review and does not represent longitudinal clinical surveillance. All thyroid FNAs are reviewed by a staff cytopathologist using criteria defined by TBSRTC. Data points collected for this study included: patient demographics, size of the thyroid nodule sampled, aspirator, pathologist rendering the final diagnosis, cytologic diagnosis, ThyroSeq^®^ GC classification, and applicable cytologic and/or surgical follow-up. Relevant surgical pathology follow-up was matched to the size and location of the index nodule. Histopathologic diagnoses were assigned following the nomenclature and criteria recently revised in the 2022 WHO Classification of Thyroid Neoplasms [9].
For the purposes of this study, surgically resected lesions were categorized as thyroid follicular nodular disease (TFND), benign/low-risk neoplasms, or malignant neoplasms in accordance with the WHO 5th edition classification. Lesions previously classified as hyperplastic, adenomatoid nodules, or as multinodular colloid goiter, were reclassified as TFND. Malignancy status was determined based on the final histopathologic diagnosis and served as the reference standard. The term “not otherwise specified (NOS)” was used when a gene mutation was reported but detailed molecular data were incomplete or unavailable. Copy number alterations (CNAs) classified as RAS-like were treated as primary RAS alterations. Cases with a RAS-like CNA and complete molecular profiling showing no additional alterations were classified as isolated RAS alterations. Data processing was performed on Microsoft Excel software (Microsoft, Redmond, WA, USA). Fisher’s exact test was used to compare outcomes between cases with isolated RAS mutations (no additional genetic alterations detected) and cases with RAS mutations plus one or more co-alterations. Second opinion cases with unavailable molecular profiling data (RAS-ND, not determined) were excluded from this analysis.
A total of 354 thyroid FNA cases from 346 patients met the inclusion criteria for this study, including 259 in-house cases and 95 second opinion cases. Surgical pathology follow-up was available for 302 cases and served as the reference standard for malignancy determination. All in-house FNAs were performed by a team of endocrinologists or radiologists using 25–27-gauge needles under ultrasound guidance, typically with 2–3 passes per nodule. Each pass yielded an air-dried slide, an alcohol-fixed slide, and residual material rinsed into PreservCyt^®^ solution (Hologic, Marlborough, MA, USA) for ThinPrep^®^ preparation. Rapid on-site evaluation (ROSE) was conducted in nearly all in-house cases by either a cytopathologist or a cytologist. Based on ROSE findings and clinical/radiologic impressions, an additional pass was collected for potential ThyroSeq^®^ GC testing. For second opinion cases, slides were re-reviewed by an in-house cytopathologist, and included confirmed RAS mutations by ThyroSeq^®^ GC.
Results
This study includes 354 thyroid nodules with RAS mutations from 346 patients (267 females, 79 males), with a mean age of 51 ± 16 years for females and 53 ± 15 years for males (Table 1). Nodule location was right lobe in 191 cases, left lobe in 148, and isthmus in 15. The mean size was 2.8 cm: 2% were < 1.0 cm, 33.3% between 1.1 and 2.0 cm, 27.4% between 2.1 and 3.0 cm, 17.2% between 3.1 and 4.0 cm, 14.7% >4.1 cm, and 5.4% unspecified.Table 1. Demographic characteristics of RAS-positive cytologic thyroid nodulesVariableValuePatients, n346 Female267 Male79Thyroid Nodules, n354 Right191 Left148 Isthmus15Age, mean ± SD, y51 ± 16Size, cmn (%)Mean ± SD, cm < 1.07 (2.0)0.9 ± 0.14 1.1–2.0118 (33.3)1.6 ± 0.26 2.1–3.097 (27.4)2.5 ± 0.28 3.1–4.061 (17.2)3.5 ± 0.28 > 4.152 (14.7)5.3 ± 1.0 NOS19 (5.4)Size, mean ± SD, cm (excluding NOS)2.8 ± 1.4NOS: Not otherwise specified
Cytologic diagnoses (TBSRTC) were Bethesda III (AUS) in 198 cases (55.9%), Bethesda IV (FN) in 125 (35.3%), Bethesda V (SM) in 29 (8.2%), and Bethesda II in 2 (0.6%). The two Bethesda II cases were second opinion cases reclassified as such upon review. ROSE was performed in 197 cases (55.6%); preliminary interpretations included AUS (61.9%), adequate (15.2%), FN (14.2%), neoplastic (5.0%), benign follicular nodule (3.0%), and suspicious for papillary thyroid carcinoma (0.5%).
Table 2 summarizes RAS-positive thyroid nodules and additional molecular alterations. NRAS mutations were most frequent (n = 220, 62.1%), followed by HRAS (n = 81, 22.9%) and KRAS (n = 48, 13.6%); 1 case had confirmed RAS mutation but the isoform was unknown and classified as RAS-NOS, four cases had molecular events that mimic RAS signaling and was classified as RAS-like. Overall, 41.0% (n = 145) had isolated RAS mutations, while 54.8% (n = 194) had RAS plus additional molecular alterations, including abnormal gene expression profiles (n = 146, 41.2%), copy number changes (n = 62, 17.5%), and/or other mutations (n = 45, 12.7%). Specifically, 40.4% (n = 143) had RAS plus one additional genomic alteration (RAS + 1), 12.7% (n = 45) had two (RAS + 2), and 1.7% (n = 6) had three (RAS + 3).Table 2. Degree of co-occurring molecular alterations in RAS-positive noduleRAS MutationRAS onlyRAS + 1RAS + 2RAS + 3RAS-NDRAS + Other MutationRAS + Copy Number AlterationsRAS + Abnormal Gene Expression ProfileHRAS2837130351641KRAS21223026120NRAS948129610324481RAS-NOS01000100RAS-like22000114RAS-NOS (not otherwise specified): RAS mutation, isoform unknown; RAS-like: molecular events that mimic RAS signaling; RAS + 0: RAS mutation with no other molecular alterations detected, RAS + 1: RAS mutation with 1 other molecular alteration detected, RAS + 2: RAS mutation with 2 other molecular alterations detected, RAS + 3: RAS mutation with 3 other molecular alterations detected, RAS-ND (not determined): RAS mutation but unavailable data on other molecular alterations
Four HRAS variants were identified, with p.Q61R (c.182 A > G) being the most frequent (n = 48, 59.3%), followed by p.Q61K (c.181 C > A) (n = 15), p.G13R (c.37G > C) (n = 10), and p.G13V (c.38G > T) (n = 1). Seven cases were HRAS NOS, and 61.7% (n = 50) had additional molecular alterations. Ten KRAS variants were identified, with p.Q61R (c.182 A > G) (n = 12) and p.G12D (c.35G > A) (n = 11) as the most common, followed by p.G12V (c.35G > T) (n = 8) and p.G13D (c.38G > A) (n = 4). Less frequent variants included p.G12R (c.34G > C) (n = 2), p.G13R (c.37G > C) (n = 1), p.G13E (c.38_39delinsAA) (n = 1), p.Q61K (c.180_181delinsAA) (n = 1), p.A146T (c.436G > A) (n = 1), and p.A146V (c.437 C > T) (n = 1). Six cases were classified as KRAS NOS. Over half (n = 25, 52.1%) had additional molecular alterations. Five NRAS variants were detected, with p.Q61R (c.182 A > G) being predominant (n = 147, 66.8%), followed by p.Q61K (c.181 C > A) (n = 34), p.G13R (c.37G > C) (n = 8), p.G12D (c.35G > A) (n = 1), and p.Q61L (c.182 A > T) (n = 1). Twenty-nine cases were NRAS-NOS, and 52.7% (n = 116) had additional genetic alterations. Of the second opinion cases, 28 (34.6%) were HRAS, 15 (31.3%) were KRAS, 50 (22.8%) were NRAS, and 2 (50.0%) had RAS-like genetic alterations.
A total of 45 RAS-positive nodules harbored concomitant mutations, all but two were surgically resected. EIF1AX was the most frequent co-mutation (n = 21, 46.7%), followed by TERT (n = 13, 28.9%). Most additional mutations (n = 32, 71.1%) occurred in NRAS-positive nodules. The most common combinations were NRAS + EIF1AX (n = 18, 40.0%), NRAS + TERT (n = 6, 13.3%), KRAS + TERT (n = 4, 8.9%), and NRAS + TP53 (n = 4, 8.9%).
Co-occurring variants included alterations in DICER1 (p.D1709E (c.5127T > A)), EIF1AX (p.G9R (c.25G > C), p.G9V (c.26G > T), splice-site variant, variant not otherwise specified), EZH1 (p.P573S (c.1717 C > T), p.Q571R (c.1712 A > G)), NRAS (p.Q61K (c.181 C > A)), PTEN (p.I101S (c.302T > G), p.R173Hfs7 (c.518_522delinsACTATG)), TERT (c.–124 C > T [C228T], c.–146 C > T [C250T]), TP53 (p.C275S (c.824G > C), p.E171G (c.512 A > G), p.G244V (c.731G > T), p.R280 (c.838 A > T), p.V272L (c.814G > T)), and TSHR (p.S281N (c.842G > A), p.D619V (c.1856 A > T)).
Histopathology follow-up data were available for 302 (85.3%) cases, 1 (0.3%) had a repeat FNA, and 51 (14.4%) had no documented follow-up (Table 3). The median time to surgical excision was 52 days from the initial FNA. Procedures included lobectomy in 204 cases (67.3%), total thyroidectomy in 96 (31.7%), isthmusectomy in 2 (0.7%), and repeat FNA in 1 (0.3%). Average nodule size was 2.45 cm for lobectomy, 3.10 cm for total thyroidectomy, 2.05 cm for isthmusectomy, and 1.6 cm for repeat FNA.Table 3. Follow-up characteristics of RAS-positive cytologic nodulesValueFollow-up Type, n No Follow-up51 Surgical Follow-up302 Cytology Follow-up1Elapsed, median, d52Procedure, n303 Lobectomy/Hemithyroidectomy204 Total Thyroidectomy96 Isthmusectomy2 Repeat FNA1
Overall, 52.3% (n = 158) of follow-up cases were malignant, 60.1% (n = 95) were invasive encapsulated follicular variant of papillary thyroid carcinoma (IEFVPTC). Follicular thyroid carcinoma (FTC) comprised 9.5% (n = 15), while classical and other subtypes of papillary thyroid carcinoma (PTC) accounted for 20.9% (n= 33). Benign/low-risk neoplasms accounted for 40.7% (n = 123) of cases, including 53.7% (n = 66) encapsulated non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), 37.4% (n = 46) follicular adenomas (FA), and 8.9% (n = 11) oncocytic adenomas (OA).
For surgically resected cases, cytology-histopathology correlation was as follows: among Bethesda III nodules, 9.0% (n = 15) were classified as TFND, 47.0% (n = 78) benign/low-risk neoplasms, and 44.0% (n = 73) malignant (Table 4), with a malignancy rate of 44.0%. For Bethesda IV nodules, 5.4% (n = 6) were TFND, 33.3% (n = 37) benign/low-risk neoplasms, and 61.3% (n = 68) malignant; the malignancy rate was 61.3%. Bethesda V nodules had no TFND on excision; 32.0% (n = 8) were benign/low-risk neoplasms and 68.0% (n = 17) malignant, the malignancy rate was 68.0%. Follicular adenoma (n = 46) and NIFTP (n = 66) comprised 91.1% of all benign/low-risk neoplasm diagnoses. When NIFTP cases were considered malignant, the malignancy rate increased to 68.1% for Bethesda III, 78.4% for Bethesda IV, and 96.0% for Bethesda V. Among malignant nodules, IEFVPTC represented 60.1% (n = 95) of cases.Table 4. Cytology, follow-up diagnosis, and RAS mutation type in RAS-positive nodulesCP: Indeterminate, nSP: TFND, nSP: Benign/Low-Risk Neoplasm, nSP: Malignant, nTBSRTC Bethesda II1000 Bethesda III0157873 Bethesda IV063768 Bethesda V00817 Total121123158RAS Mutation* HRAS043238 KRAS101718 NRAS01770102 RAS*-NOS0010* RAS*-like0030TBSRTC: The Bethesda System for Reporting Thyroid Cytopathology; CP: Cytopathology; SP: Surgical Pathology; SP: TFND (thyroid follicular nodular disease) – includes multinodular goiter, hyperplastic nodule, adenomatous nodule, or adenomatous hyperplasia; SP: Benign/low-risk neoplasms – includes: FA (follicular adenoma), OA (oncocytic adenoma), and NIFTP (non-invasive follicular thyroid neoplasm with papillary-like nuclear features); SP: Malignant neoplasms – includes: FTC (follicular thyroid carcinoma), IEFVPTC (invasive encapsulated follicular variant of papillary thyroid carcinoma), PTC (papillary thyroid carcinoma), OCA (oncocytic carcinoma), PDTC (poorly differentiated thyroid carcinoma), MTC: medullary thyroid carcinoma; RAS-NOS (not otherwise specified): RAS mutation, isoform unknown; RAS-like: molecular events that mimic RAS signaling
Histopathologic follow-up, along with the molecular profile, is illustrated in Fig. 1 and is summarized in Table 4. Among follow-up cases, HRAS mutations were found in 74 (24.5%), KRAS in 35 (11.6%), and NRAS in 189 (62.6%). In surgically resected cases, malignant neoplasms were found across all mutation types: HRAS (n = 38, 51.4%), KRAS (n = 18, 51.4%), and NRAS (n = 102, 54.0%).Fig. 1. Distribution of HRAS, KRAS, NRAS, or RAS-like/RAS-NOS mutation among TFND, benign/low-risk neoplasm, and malignant surgically resected nodules. TFND (Thyroid follicular nodular disease) – includes multinodular goiter, hyperplastic nodule, adenomatous nodule, or adenomatous hyperplasia; Benign/low-risk neoplasms – includes: FA (follicular adenoma), OA (oncocytic adenoma), and NIFTP (non-invasive follicular thyroid neoplasm with papillary-like nuclear features); Malignant neoplasms – includes: FTC (follicular thyroid carcinoma), IEFVPTC (invasive encapsulated follicular variant of papillary thyroid carcinoma), PTC (papillary thyroid carcinoma), OCA (oncocytic carcinoma), PDTC (poorly differentiated thyroid carcinoma), and MTC: medullary thyroid carcinoma; NOS: Not otherwise specified
DICER1 co-mutation was identified in one malignant case. EIF1AX co-mutations were identified in 10 benign/low-risk neoplasms and 11 malignant cases. Two RAS-positive cytologic nodules harbored co-occurring EZH1 mutation but did not undergo further follow-up. PTEN co-mutations were observed in one benign/low-risk neoplasm and one malignant case. TERT promoter co-mutations were found in one benign/low-risk neoplasm case and 12 malignant cases. TP53 co-mutations were found exclusively in 4 malignant cases; 1 case harbored 2 distinct TP53 co-mutations. TSHR co-mutations were present in one TFND and one benign/low-risk neoplasm case. The risk of malignancy for RAS co-mutation with DICER1 was 100%, 52.4% for EIF1AX, 50% for PTEN, 92.3% for TERT, 100% TP53, and 0% TSHR mutations (Table 5).Table 5. Co-occurring mutations and diagnostic categories in RAS-positive surgically resected thyroid nodulesDICER1EIF1AXNRASPTENTERTTP53TSHRThyroid follicular nodular disease (TFND) TFND0000001Benign/low-risk neoplasms FA0501000 OA0100001 NIFTP0410100Malignant neoplasms FTC0101000 IEFVPTC0800730 PTC1200200 OCA0000210 PDTC0000110ROM100%52.4%0%50%92.3%100%0%TFND (thyroid follicular nodular disease) – includes multinodular goiter, hyperplastic nodule, adenomatous nodule, or adenomatous hyperplasia; Benign/low-risk neoplasms – includes: FA (follicular adenoma), OA (oncocytic adenoma), and NIFTP (non-invasive follicular thyroid neoplasm with papillary-like nuclear features); Malignant neoplasms – includes: FTC (follicular thyroid carcinoma), IEFVPTC (invasive encapsulated follicular variant of papillary thyroid carcinoma), PTC (papillary thyroid carcinoma), OCA (oncocytic carcinoma), and PDTC (poorly differentiated thyroid carcinoma); ROM: Risk of Malignancy1 case of IEFVPTC harbored NRAS and 2 distinct TP53 mutations**1 case of IEFVPTC harbored NRAS, EIF1AX, and TERT mutations
Among the 43 nodules harboring RAS mutations with additional molecular alterations, 22 underwent lobectomy and 21 underwent total thyroidectomy (Table 6). Of the total thyroidectomies, 16 cases (76.2%) were malignant and 5 cases (23.8%) were benign/low-risk neoplasms (FA, NIFTP, OA). In comparison, 10 of 22 lobectomy cases (45.5%) were non-malignant and 12 (54.5%) were malignant. For this study, surgical pathology outcomes refer exclusively to the index nodule sampled by FNA; any additional malignant findings outside the index nodule were not considered.Table 6. Outcomes of lobectomy/isthmusectomy and total thyroidectomy in RAS + additional mutation nodulesSurgery typeNon-Malignant, nMalignant, nTotal, nLobectomy101222Total Thyroidectomy51621 Total152843
Cases with isolated RAS mutations were diagnosed on surgical follow-up as TFND (n = 14, 12.0%), benign/low-risk neoplasm (n = 55, 47.0%), or malignant (n = 48, 41.0%), with follicular adenoma (n = 29) more common than NIFTP (n = 24), as shown in Fig. 2. The malignancy rate was 41.0%, with the most frequent malignant diagnosis being IEFVPTC (n = 32). When a RAS mutation was accompanied by one additional molecular alteration (RAS + 1), the malignancy rate increased to 54.3% (n = 69). Among benign/low-risk neoplasms, NIFTP (n = 33) was most common, followed by follicular adenomas (n = 13) and oncocytic neoplasms (n = 8). IEFVPTC remained the main malignancy (n = 41). In cases with two additional genetic abnormalities (RAS + 2), 71.1% (n = 27) were malignant, with IEFVPTC (n = 12) as the most common malignancy, and NIFTP (n = 6) for benign/low-risk neoplasms. All RAS + 3 cases were malignant (n = 6), predominantly IEFVPTC (n = 5).Fig. 2. Degree of RAS molecular alterations among surgically resected nodules. RAS-NOS cases (confirmed RAS mutations with unknown isoform) and RAS-like alterations were included in the corresponding RAS category according to the number of additional alterations. TFND (Thyroid follicular nodular disease) – includes multinodular goiter, hyperplastic nodule, adenomatous nodule, or adenomatous hyperplasia; Benign/low-risk neoplasms - FA: follicular adenoma, OA: oncocytic adenoma, and NIFTP: non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP); Malignant neoplasms - FTC: follicular thyroid carcinoma, IEFVPTC: invasive encapsulated follicular variant of papillary thyroid carcinoma, PTC: papillary thyroid carcinoma – other subtypes, OCA: oncocytic carcinoma, PDTC: poorly differentiated thyroid carcinoma, MTC: medullary thyroid carcinoma; RAS + 0: Isolated RAS mutation, RAS + 1: RAS mutation with 1 other molecular alteration*, RAS + 2: RAS mutation with 2 other molecular alterations*, RAS + 3: RAS mutation with 3 other molecular alterations*, RAS-ND (not determined): RAS mutation but unavailable data on other molecular alterations *Other molecular alterations include an abnormal gene expression profile, copy number alterations, and/or distinct gene mutations in addition to RAS
Cases with additional molecular alterations (mutations beyond RAS, abnormal gene expression profile, and/or copy number alterations) were compared with cases harboring isolated RAS mutations. Statistically significantly higher risk of malignancy was observed in the RAS + any additional molecular alterations group (Fisher’s exact test, two-tailed p = 0.0026). Fifteen second opinion cases with RAS mutations lacked complete molecular profiling (RAS-ND) and were excluded from the analysis.
Discussion
RAS, a family of GTP-binding proteins upstream of BRAF, regulates cell growth through the MAPK and PI3K-AKT pathways and is mutated in about one-third of human tumors [7]. First identified in thyroid cancer in 1988, RAS mutations—particularly in NRAS, followed by HRAS and KRAS—are found in various thyroid tumors, including follicular and papillary types, but are more strongly associated with aggressive forms like poorly differentiated and anaplastic thyroid carcinomas. These mutations, commonly occur at codons 12, 13, and especially 61, alter GTP-binding or GTPase activity, leading to continuous activation of downstream signaling pathways. NRAS mutations tend to activate PI3K-AKT, while KRAS mutations favor the MAPK pathway. In PTC, RAS and BRAF mutations are mutually exclusive, indicating RAS can independently drive tumor development through aberrant signaling that promotes uncontrolled cell proliferation and differentiation.
RAS mutations are commonly found in indeterminate thyroid nodules, with clinical outcomes ranging from indolent to aggressive disease. Several studies have reported mostly benign or slow-growing courses [10–30], while others have described more aggressive clinical courses [31–38]. As molecular testing gains prominence, it has become routine to perform genomic profiling on indeterminate thyroid cytology cases to aid diagnosis and management. Within our healthcare system, all indeterminate cytology specimens undergo reflex testing with ThyroSeq^®^ GC automatically. Following testing, our cytopathologists provide a comprehensive final report with interpretative recommendations tailored to the patient’s molecular profile. This approach enables a more precise understanding of the tumor biology at an individual level, facilitating targeted and personalized clinical interventions [39, 40].
Overall, the presence of a RAS mutation is associated with a 1.7-fold increased risk of malignancy, often warranting surgical resection [41]. Across the six-year study period, follow-up data were available for our cohort in 85.6% (n = 303) cases, with all but one undergoing surgical resection. Among these, 52.3% (n = 158) were malignant, with IEFVPTC comprising 60.1% (n = 95) of malignant cases. The malignancy rate increased progressively with higher TBSRTC category, from 44.0% in Bethesda III to 68.0% in Bethesda V nodules. When NIFTP cases were included as malignant on follow-up, the malignancy rates rise substantially to 68.1% for Bethesda III to 96.0% for Bethesda V categories.
A recent meta-analysis by Riccio et al. [41] demonstrated that RAS mutations are frequently associated with thyroid tumors with a follicular growth pattern, including IEFVPTC and FTC. Consistent with this, lesions with a follicular growth pattern – including FA, OA, NIFTP, IEFVPTC, and oncocytic carcinoma (OCA) – predominated among RAS-positive nodules in our cohort, accounting for 81.1% (245/302). This spectrum highlights the diagnostic challenges posed by RAS-mutated lesions, which often overlap morphologically and molecularly between benign and malignant categories [42].
The study by Sfreddo et al. [43] compared outcomes in RAS-mutated indeterminate thyroid nodules managed either with active surveillance or immediate surgery. At our institution, most cases underwent prompt surgical resection, with a median interval of 52 days from cytologic diagnosis to surgical pathology. Only five cases had follow-up extending beyond 273 days, reflecting the surgical management approach in our practice.
Consistent with prior studies [41, 44], NRAS mutations were the most frequent in our cohort, present in 62.1% (n = 220) of cases, followed by HRAS in 22.9% (n = 81), and KRAS in 13.6% (n = 48). Overall, RAS p.Q61R was the most common hot-spot mutation in our cohort, occurring in 207 of 354 cases (58.5%). Although somewhat lower than the 76% prevalence reported by Alzumaili et al. [45], the predominance of p.Q61R in both cohorts underscores its central role among RAS-driven thyroid nodules. The prognostic significance of specific RAS subtypes remains an area of ongoing investigation. Radkay et al. [46] suggested that NRAS and KRAS mutations may be linked to less aggressive disease compared to HRAS mutations. However, in our study, malignancy rates were comparable across RAS subtypes: 51.4% for HRAS, 51.4% for KRAS, and 54.0% for NRAS indicating similar clinical behavior.
A comprehensive meta-analysis of thirty studies [41] revealed a heterogeneous distribution of RAS-positive malignant nodules following surgery: 34% classic subtype of papillary thyroid carcinoma (PTCcs), 39% IEFVPTC, and 23% FTC. In contrast, our cohort showed a predominance of IEFVPTC, which accounted for 60.1% of malignant cases with surgical follow-up. Other malignancies included subtypes of PTC (20.9%), FTC (9.5%), OCA (7.6%), poorly differentiated thyroid carcinoma (1.3%), and medullary carcinoma (0.6%). These findings align with Cameselle-Teijeiro et al. [47] where accurate classification requires integration of morphology with ancillary immunohistochemical and molecular findings.
The study by Bikas et al. [48] demonstrated that patients harboring RAS mutations alongside additional genetic alterations tend to exhibit more aggressive disease, with these cumulative genetic “hits” linked to higher mortality risk and greater neoplastic heterogeneity. Reflecting this, our cohort showed a near split between cases with an isolated RAS mutation (41.0%) and those with one additional molecular alteration (RAS + 1, 40.4%). Notably, the malignancy rate was significantly higher in the RAS + 1 group compared to isolated RAS cases (54.3% vs. 41.0%), underscoring the impact of coexisting mutations on tumor aggressiveness. When two (RAS + 2) or three (RAS + 3) additional molecular alterations were present alongside the RAS mutation, malignancy rates rose markedly to 71.1% and 100%, respectively. The additional abnormalities identified in our cohort included abnormal gene expression profiles (n = 146, 41.2%), copy number alterations (n = 62, 17.5%), and other distinct gene mutations beyond RAS (n = 45, 12.7%).
According to American Thyroid Association (ATA) recommendations, RAS-mutated indeterminate nodules may be managed with diagnostic lobectomy or, in select low-risk settings, active surveillance [3]. Our observation that many isolated RAS mutation benign/low-risk lesions were follicular adenomas (52.7%) reinforces the appropriateness of conservative or stepwise management strategies consistent with ATA guidance. However, with one or two additional molecular alterations (RAS + 1 and RAS + 2), the benign-to-low-risk neoplastic population shifted towards NIFTP, comprising 61.1% and 66.7%, respectively. The malignant cohort similarly became more diverse with the addition of genetic alterations; follicular-patterned lesions represented 75.0% of malignancies with isolated RAS mutations, 70.0% with RAS + 1, and 55.6% with RAS + 2. Interestingly, cases with three additional molecular alterations (RAS + 3) saw an increase again in follicular-patterned malignancies to 83.3%. These findings highlight how accumulating genetic alterations in RAS-mutated thyroid nodules contributes to increasing malignancy risk and complexity of tumor histology, emphasizing the importance of comprehensive molecular profiling for risk stratification and management decisions.
Aside from mutation and genomic variation burden, prior studies highlight that the type of co-occurring alteration with RAS strongly influences tumorigenesis and biologic behavior. Isolated EIF1AX mutations confer only a modest risk of malignancy (~ 25–40%) [49–51], yet the presence of EIF1AX alongside RAS, TERT promoter, or TP53 mutations increases the risk to approximately 86%, demonstrating potent cooperative oncogenic effects [51]. Notably, RAS + EIF1AX co-mutations, especially those involving the A113_splice variant, are consistently enriched in tumors showing progression toward poorly differentiated thyroid carcinoma (PDTC) [52, 53]. In our cohort, the RAS + EIF1AX combination accounted for 46.7% of all co-mutations with a risk of malignancy of 52.4%, predominantly IEFVPTC; 71.4% involved the A113_splice variant. Aligning with prior observations that RAS partnered with TERT promoter alterations strongly predicts aggressive clinical disease [54, 55], while RAS + TP53 combinations are similarly associated with dedifferentiation [56, 57]. RAS + TERT and RAS + TP53 co-mutations were observed in 26.7% and 8.9% of all combinations in our cohort. RAS + TERT co-mutations had a risk of malignancy of 92.3%, predominantly IEFVPTC with 1 case of PDTC; RAS + TP53 co-mutations were malignant in all cases with 1 case of PDTC. Collectively, these observations illustrate that whereas RAS alone often drives indolent or well-differentiated lesions, the acquisition of specific secondary mutations such as EIF1AX, TERT, or TP53 can drive tumors towards more aggressive, heterogeneous, and poorly differentiated phenotypes.
Although our data reinforces that additional mutations increase the risk of malignancy in RAS-mutated nodules, malignancy is not guaranteed. Notably, 5 patients with RAS + additional mutations underwent total thyroidectomy yet were found to have benign/low-risk neoplasms (FA, NIFTP, or OA) on final pathology. This emphasizes the potential for overtreatment and underscores the importance of careful surgical decision-making, particularly when other high-risk clinical or molecular features are absent, consistent with prior reports [58]. At this time, ATA guidelines state that the presence of additional molecular alterations, while informative for risk stratification, should be interpreted alongside cytologic, sonographic, and clinical features rather than used in isolation to determine malignancy or guide definitive surgery [3].
This study has several limitations. Its retrospective design, required for adequate surgical follow-up, limits variable control and may introduce bias. Long-term clinical outcomes were not assessed, so delayed or subsequent malignancies could not be evaluated. Inclusion of both in-house and consultation cases introduced variability in sampling techniques and testing methods. Selection bias is possible due to the exclusive focus on RAS-mutant nodules, though this was intentional. Findings may not generalize to nodules with non-diagnostic, benign, or overtly malignant cytology, as most cases had indeterminate cytology (Bethesda III–V). Some cases lacked follow-up, preventing determination of malignancy status—an inherent limitation of retrospective cytology-based studies. Additionally, incomplete ThyroSeq^®^ GC data from outside institutions resulted in classification of some cases as RAS-ND and precluded assessment of co-occurring molecular alterations.
Despite these limitations, this study offers several notable strengths. It represents one of the largest single-institution cohorts of RAS-mutated thyroid nodules, collected over six years with corresponding surgical follow-up. Approximately one-quarter were second opinion cases, included to enhance diversity and increase sample size, enabling more robust analysis of molecular alterations, histologic subtypes, and clinical outcomes. Importantly, findings were stratified by specific RAS point mutations, providing deeper molecular insights. Furthermore, the high rate of surgical resection allowed for strong histopathologic correlation and outcome assessment.
This study underscores that RAS mutations, particularly NRAS, are common in indeterminate thyroid nodules and frequently co-occur with additional molecular alterations. Our analysis demonstrated that nodules with RAS plus additional molecular alterations carry a statistically significantly higher malignancy risk than those with isolated RAS mutations. Malignancy risk increases with each added genetic alteration, reaching 100% when three are present. Isolated RAS mutations are more often associated with benign-to-low-risk neoplasms such as follicular adenoma or NIFTP, whereas co-mutations correlate with invasive malignancy, especially IEFVPTC. These findings highlight the critical role of comprehensive molecular profiling in refining risk stratification and guiding surgical decision-making for RAS-positive nodules.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Cancer Institute (2025) Cancer Stat Facts: Thyroid Cancer. https://seer.cancer.gov/statfacts/html/thyro.html. Accessed 06 June 2025
- 2Censi S, Cavedon E, Bertazza L et al. (2017) Frequency and Significance of Ras, Tert Promoter, and Braf Mutations in Cytologically Indeterminate Thyroid Nodules: A Monocentric Case Series at a Tertiary-Level Endocrinology Unit. Front Endocrinol (Lausanne) 8. 10.3389/fendo.2017.0027310.3389/fendo.2017.00273 PMC 565069829085338 · doi ↗ · pubmed ↗
- 3Gill SM, Nayan S, Kocovski L et al. (2015) Local molecular analysis of indeterminate thyroid nodules. J Otolaryngol Head Neck Surg 44. 10.1186/s 40463-015-0106-210.1186/s 40463-015-0106-2PMC 466616526621130 · doi ↗ · pubmed ↗
- 4Lu SY, Chen YC, Zhu CF et al. (2021) A five-gene panel refines differential diagnosis of thyroid nodules. J Clin Lab Anal 35. 10.1002/jcla.2392010.1002/jcla.23920 PMC 841850634318534 · doi ↗ · pubmed ↗
- 5Liu R, Xing M (2016) TERT promoter mutations in thyroid cancer. Endocr Relat Cancer 23: R 143-R 155. 10.1530/ERC-15-053310.1530/ERC-15-0533 PMC 475065126733501 · doi ↗ · pubmed ↗