Pharmacological advances in multi-targeted strategies for type 2 diabetes mellitus: a systematic perspective based on traditional Chinese medicine
Yan-Li Zhao, Jia-Bao Liao, Pan-Pan Pang, Jing-Yuan Li, Suo-Cai Su, Meng-Qiu Shao, Wei-Bo Wen, Fu-Rong Xu

TL;DR
This review explores how traditional Chinese medicine and plant-based compounds may help treat type 2 diabetes by targeting multiple biological pathways.
Contribution
The paper provides a systematic synthesis of TCM botanical drugs and metabolites with their mechanisms in T2DM, emphasizing multi-targeted strategies.
Findings
TCM botanicals like berberine and baicalin modulate key pathways such as PI3K/Akt and NF-κB/NLRP3 in T2DM.
Formula-based preparations require detailed reporting of composition and standardization for reproducibility.
Compound–target links from in silico studies need orthogonal validation to avoid false positives.
Abstract
Type 2 diabetes mellitus (T2DM) is a complex systemic metabolic disease driven by insulin resistance, β-cell dysfunction, chronic low-grade inflammation, oxidative stress, and neuro-immune dysregulation. It frequently progresses to multi-organ complications affecting the kidneys, retina, heart, and central nervous system. This review synthesizes mechanistic and translational evidence on Traditional Chinese Medicine (TCM)-related botanical drugs and botanical preparations (formula-based interventions), along with representative plant metabolites that are frequently investigated in the TCM research context (e.g., berberine, baicalin, and tanshinone IIA, which are not unique to TCM). For formula-based preparations, we extracted and reported intervention identity elements (dosage form, complete composition, and processing/standardization as described in primary studies); missing identity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
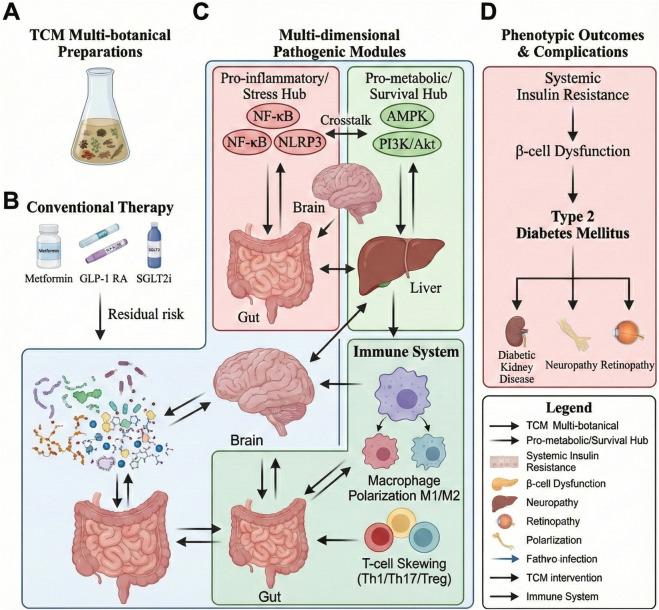 FIGURE 1
FIGURE 1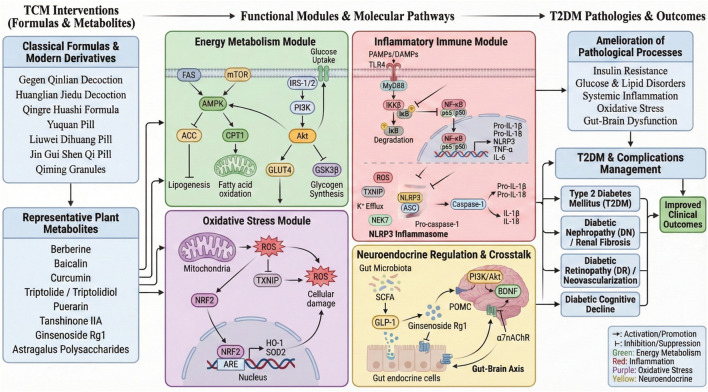 FIGURE 2
FIGURE 2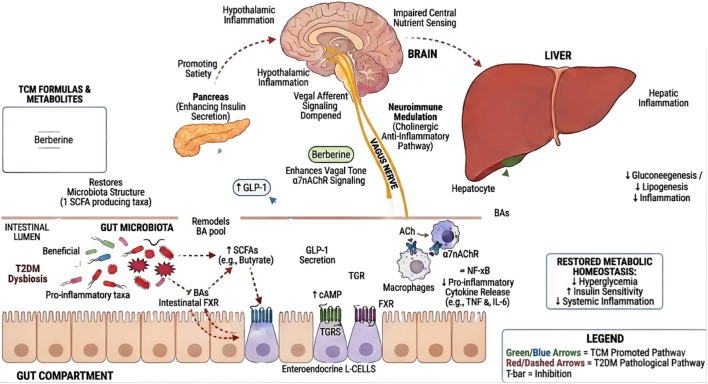 FIGURE 3
FIGURE 3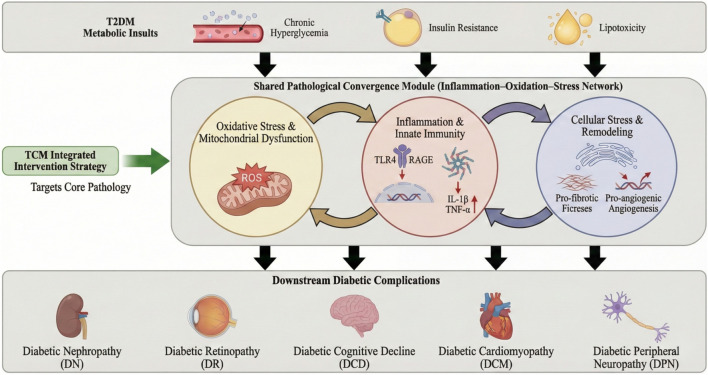 FIGURE 4
FIGURE 4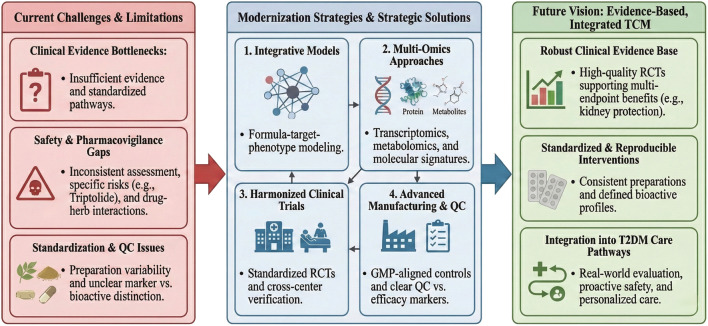 FIGURE 5
FIGURE 5| Functional module | Key pathways or targets | Representative TCM plant metabolites | Representative formulas | Clinical evidence tier | T2DM processes |
|---|---|---|---|---|---|
| Energy metabolism module ( | AMPK, PPARγ, SIRT1 | Berberine (from Coptis chinensis Franch. [Ranunculaceae]), Astragalus polysaccharides (from Astragalus membranaceus (Fisch.) Bunge [Fabaceae]/Astragalus mongholicus Bunge [Fabaceae], as reported) | Huanglian Jiedu Decoction (multi-botanical decoction; composition/processing/QC markers in | Supported by clinical trials and animal studies | Insulin resistance, energy imbalance |
| Inflammatory immune module ( | NF-κB, NLRP3, TNF-α, IL-6 | Baicalin (from Scutellaria baicalensis Georgi [Lamiaceae]), Triptolide (from Tripterygium wilfordii Hook.f. [Celastraceae]), Curcumin (from Curcuma longa L. [Zingiberaceae]) | Qingre Huashi Formula (multi-botanical preparation; composition/processing/QC markers in | Supported by animal and | Chronic inflammation, immune dysregulation |
| Oxidative stress module ( | NRF2/HO-1, ROS, SOD | Tanshinone IIA (from Salvia miltiorrhiza Bunge [Lamiaceae]), Puerarin (primarily associated with Pueraria lobata (Willd.) Ohwi [Fabaceae], as reported) | Qiming Granules (Chinese patent medicine; full botanical composition/manufacturing and QC information in | Supported mainly by animal/ | Oxidative stress injury, diabetic complications |
| Neuroendocrine regulation module ( | GLP-1, insulin receptor, BDNF | Ginsenoside Rg1 (from Panax ginseng C.A.Mey. [Araliaceae]), Poria polysaccharides (from Wolfiporia extensa (Peck) Ginns [Polyporaceae]; syn. Poria cocos, as reported) | Yuquan Pill (multi-botanical pill; composition/processing/QC markers in | Supported by some clinical trials | Insulin secretion, glucose control, cognitive decline |
| Metabolism–inflammation–neuro crosstalk module (integrative) | Cross-module integration | Combination of above metabolites (source species/authorities/families specified in respective rows; taxonomically validated; see | Huanglian Jiedu Decoction (composition/processing/QC markers in | Supported by integrated multi-omics studies | Systemic metabolic syndrome, multi-organ complications |
| Lineage/Therapeutic principle | Representative classical formula (English name; abbreviation) | Common modern derivatives/Commercial Chinese polyherbal preparation (CCPP) (examples) | Typical mechanistic modules (examples) | Composition & processing/Taxonomic validation (required; where not reported, record as NR)** |
|---|---|---|---|---|
| Heat-clearing and damp-heat resolving | Gegen Qinlian Decoction (GQD) | GQD granules; related decoction derivatives used in trials | PI3K/Akt; AMPK; NF-κB/NLRP3; gut microbiota–SCFA | Provide full composition for GQD (all component drugs) with taxonomically validated source species (authority + family), plant part, and voucher specimen (if reported); specify preparation (decoction/granule), extraction solvent, drug:solvent ratio, concentration, dosing, and quantitative QC markers/fingerprint; otherwise mark NR. |
| Qi–Yin replenishing (Xiaoke-related) | Yuquan Pill (YQP) | Yuquan-based commercial Chinese polyherbal preparation (CCPP) (where applicable) | AMPK; PI3K/Akt; oxidative-stress modules; gut–endocrine relay (reported) | For YQP/patent derivatives: report manufacturer/pharmacopeial reference (if applicable), dosage form, complete composition with validated species (authority + family), processing (Paozhi), and quantitative QC markers; otherwise mark NR. |
| Yin-nourishing and deficiency-heat clearing | Liuwei Dihuang Pill (LDP; LWDHW) | LWDHW-based derivatives (e.g., modified pills/granules in trials) | Gut microbiota–SCFA–GLP-1 (reported); anti-inflammatory and redox modules | Report complete composition for LWDHW-based interventions with validated species (authority + family), plant part, voucher (if reported), and preparation/QC details (dosage form, extraction/processing, marker quantification, batch consistency); otherwise mark NR. |
| Kidney-supporting (chronic deficiency patterns) | Jin Gui Shen Qi Wan (JGSQW; also known as Shenqi Wan) | JGSQW-based pills/granules; related “kidney-supporting” derivatives | PI3K/Akt; AMPK; redox/inflammation modules (reported) | Define the preparation unambiguously (JGSQW/Shenqi Wan; classical formula source if stated in primary study) and report complete composition with validated species (authority + family), processing/preparation, dosage form, and quantitative QC markers; otherwise mark NR. |
| Complication-oriented derivatives (microvascular protection) | — (lineage includes formula-derived complication prescriptions) | Qiming Granules (DR adjunct); Huang Kui Capsules (DN); others as applicable | VEGF/HIF-1α; NRF2/ROS; TGF-β/SMAD; inflammatory modules | For multi-botanical proprietary preparations: report complete composition with validated species (authority + family), plant part, voucher (if reported), dosage form, manufacturer, preparation/extraction details, and quantitative QC markers/batch numbers; otherwise mark NR. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBerberine and alkaloids research · Traditional Chinese Medicine Analysis · Ginseng Biological Effects and Applications
Introduction
1
Type 2 diabetes mellitus (T2DM) is a complex systemic metabolic disease characterized by insulin resistance, β-cell dysfunction, chronic low-grade inflammation, and oxidative stress (Butler et al., 2003; Samuel and Shulman, 2012; Du et al., 2003; Defronzo, 2009; Fu et al., 2021; Goldfine et al., 2013; Ryuk et al., 2017; Shi et al., 2019; Peng et al., 2021). According to the International Diabetes Federation (IDF) Diabetes Atlas (2025), an estimated 589 million adults (20–79 years) were living with diabetes worldwide in 2024 (≈1 in 9), and the total number is projected to rise to 853 million by 2050 (≈1 in 8) (International Diabetes Federation, 2025; GBD 2021 Diabetes Collaborators, 2023; An et al., 2023). According to the International Diabetes Federation (IDF) Diabetes Atlas (11th edition), China has the highest number of adults (20–79 years) living with diabetes, with an estimated adult prevalence of approximately 11.9% by 2024. Notably, prevalence estimates can vary by data source and diagnostic criteria; for example, a large nationally representative survey in China reported an overall diabetes prevalence of 12.4% in 2018 (Li et al., 2017; Wang L et al., 2021). In addition to chronic hyperglycemia, T2DM frequently manifests with cardiovascular and microvascular complications (e.g., diabetic kidney disease, neuropathy, and retinopathy), collectively forming a complex and interconnected pathological network (Luo et al., 2009). Contemporary guideline-recommended therapies for T2DM, including metformin and agents with proven cardio–renal benefits, such as sodium–glucose cotransporter 2 (SGLT2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists, can improve glycemic control and reduce major cardiovascular and/or kidney outcomes. However, residual risk and incomplete prevention of complication progression remain in many patients, underscoring the need for complementary strategies that target broader pathogenic modules beyond glycemia. In this context, TCM-related multi-botanical preparations (formula-based botanical preparations), which comprise multiple constituents and diverse plant metabolites, may offer a complementary, formula-centered framework to co-modulate overlapping disease-relevant modules (e.g., inflammation, oxidative stress, insulin signaling, and neuroendocrine regulation), provided that botanical drug identity, preparation standardization/quality control, dosing ranges, appropriate controls, and outcome-linked endpoints are transparently reported and evidence graded (Yao et al., 2024). Accordingly, for each multi-botanical preparation (including classical formulas such as Jin-Gui Shen-Qi Wan [Jin Gui Shen Qi Pill]), we extracted and reported intervention identity unambiguously, including dosage form, complete composition, and processing/extraction/standardization, as described in the primary studies. Missing identity items were recorded as NR (not reported) and were not inferred. Studies have shown that the bioactive plant metabolites of TCM-related botanical drugs cooperatively regulate key metabolic and inflammatory signaling pathways, including PI3K/Akt, AMPK, NF-κB, and NLRP3, influencing the signaling interactions within the gut-liver-brain–immune axis, thereby exerting systemic regulatory effects (Ng et al., 2024; Wu et al., 2025; Ghafouri-Fard et al., 2022; Lin et al., 2023; Wang et al., 2025).
Systems-level framework linking TCM interventions to the gut–liver–brain–immune axis in T2DM. (A) Multi-botanical, formula-based TCM preparations provide diverse bioactive candidates with standardization and quality control. (B) Guideline therapies (metformin, GLP-1 RA, SGLT2i) improve glycemia; however, residual risk may persist. (C) Gut–liver–brain–immune crosstalk converges on a pro-inflammatory/stress hub (NF-κB–linked transcription, NLRP3 inflammasome) and a pro-metabolic/survival hub (AMPK, PI3K/Akt), with immune imbalance (macrophage polarization, T-cell skewing) reinforcing chronic low-grade inflammation. (D) These interactions drive insulin resistance, β-cell dysfunction, and other major complications. Line semantics: solid, direct regulation; dashed, indirect associations; red, pathological promotion; green, therapeutic restoration; blunt-ended, inhibition.
Methods: literature search, study selection, and critical appraisal
1.1
We conducted a structured literature search to identify preclinical and clinical studies evaluating Traditional Chinese Medicine (TCM) formulas, botanical extracts, and representative plant metabolites relevant to type 2 diabetes mellitus (T2DM) and its major complications. Searches were performed in PubMed/MEDLINE, Web of Science, and Scopus from January 2000 to December 2025 using combinations of controlled vocabularies and free text terms. The core PubMed search string was: (“type 2 diabetes” OR T2DM OR “diabetic complications”) AND (“traditional Chinese medicine” OR TCM OR “Chinese herbal” OR decoction OR formula OR “herbal extract”) AND (trial OR randomized OR RCT OR clinical OR preclinical OR in vivo OR in vitro OR “network pharmacology” OR “systems pharmacology” OR multi-omics), with additional compound/formula terms (e.g., berberine, baicalin, curcumin, Gegen Qinlian Decoction, Huanglian Jiedu Decoction, Jin-Gui Shen-Qi Wan [Jin Gui Shen Qi Pill]) used where appropriate. The reference lists of relevant reviews were screened to identify additional eligible studies. Titles and abstracts were screened first, followed by a full-text assessment. We included studies that (i) investigated a defined TCM formula/extract or a clearly specified phytochemical, (ii) used a T2DM-relevant model or patient population, and (iii) reported metabolic outcomes and/or complication-related endpoints. We excluded articles lacking sufficient methodological detail to evaluate the central pharmacological/clinical claims, studies with unclear intervention identity/standardization, and purely speculative discussions without primary data. The evidence was stratified into tiers (human/RCT, animal, and in vitro/in silico). For pharmacological studies, we extracted the model type, dose range and/or minimal active concentration (where reported), exposure duration, extract/compound characterization, and presence of appropriate positive/negative controls. For clinical studies, we extracted the study design, sample size, intervention standardization, concomitant therapies, clinically meaningful endpoints (e.g., HbA1c and complication-related outcomes), safety reporting, and follow-up duration. Where key information (e.g., dose–response/MAC, controls, extract characterization, composition and processing/standardization, or taxonomic validation) was not reported in the primary study, we did not infer missing details and instead recorded these items as NR (not reported) and considered them in the limitations appraisal of the study. All source organisms were taxonomically validated using authoritative resources (e.g., Kew MPNS and/or Plants of the World Online), and full scientific names including author citation and family (e.g., “Salvia”) are provided in the Supplementary Tables/Supplementary Material. To ensure a rigorous appraisal of the phytopharmacological evidence, we assessed the reporting quality and extract characterization using the GA-online Best Practice in Research–ConPhyMP tool (Supplementary Tables 1, 2A; sections relevant to reviews), provided as Supplementary File S2 (Heinrich et al., 2022; GA-online, 2025). The reporting is summarized in Supplementary Tables S1, S2, and a PRISMA-style study selection flow diagram is provided in Supplementary Figure S1.
Targeted modulation of key signaling pathways by TCM in T2DM
2
The pathogenesis of T2DM involves multiple tightly coupled processes governed by core signaling modules (e.g., PI3K/Akt, AMPK, NF-κB, and NLRP3). Rather than implying a strict “single-target vs. multi-target” dichotomy, we used a systems-pharmacology lens to organize evidence on botanical formulas and constituents across shared T2DM-relevant modules, prioritizing studies in which pathway modulation is accompanied by metabolic or complication-related endpoints (e.g., HbA1c, HOMA-IR, and tissue injury markers) (Figure 2).
Systems pharmacology map linking TCM formulas/metabolites to functional modules and T2DM outcomes. Classical formulas and modern derivatives (left) provide representative metabolites that act on four interconnected modules: energy metabolism (AMPK–PI3K/Akt–GLUT4), inflammatory immunity (TLR4–MyD88–NF-κB and NLRP3 inflammasome), oxidative stress (NRF2–ARE/HO-1 axis), and neuroendocrine crosstalk (gut microbiota–SCFA/GLP-1 and α7nAChR–gut–brain signaling). The coordinated modulation of these modules ameliorates insulin resistance, metabolic dysregulation, systemic inflammation, oxidative stress, and gut–brain dysfunction, thereby improving T2DM and major complications (DN, DR, and cognitive decline). Arrows indicate activation/promotion or inhibition/suppression, and colors denote module categories.
Systematic pharmacological explanation of TCM intervention in T2DM
2.1
While multiple studies indicate that TCM-related botanical drugs and botanical preparations modulate key signaling pathways such as PI3K/Akt, AMPK, NF-κB, and NRF2, these findings are often fragmented and may over-emphasize isolated target “hits.” To reduce over-interpretation, we explicitly distinguished evidence tiers (human/RCT vs. animal vs. in vitro/in silico) and interpreted compound–target claims cautiously because some plant metabolites may exhibit assay-interference liabilities (including PAINS) or non-specific effects; whenever possible, conclusions should rely on orthogonal validation and outcome-linked readouts rather than single-assay target engagement (Baell and Holloway, 2010; Dahlin et al., 2021). In this section, we use a systems-pharmacology lens to organize the evidence into multilayer networks linking formulas–plant metabolites–targets–pathways, and then map the targets into higher-order functional modules (e.g., energy metabolism, immune–inflammatory regulation, oxidative stress, and neuroendocrine regulation). By applying pathway enrichment (e.g., KEGG/GO), network clustering, and pathway mapping, the regulatory effects of TCM-related interventions can be aligned with core pathogenic characteristics of T2DM, thereby advancing from “point-target regulation” to “system module intervention.” Notably, many representative metabolites summarized in Table 1 (e.g., berberine, baicalin, and curcumin) are widely distributed natural products and are not unique to TCM; they are included here as exemplars frequently studied in the TCM research context to support ingredient–target–module mapping. Importantly, multi-target pharmacology is also observed in conventional single-molecule drugs (e.g., metformin). Here, we used a system pharmacology framework primarily to structure and compare formula-centered evidence into functional modules for T2DM (Table 1).
Interpreting classical formula compatibility (Jun–Chen–Zuo–Shi) within a multi-target network-module framework
2.2
In classical formula design, the “Jun–Chen–Zuo–Shi” (monarch–minister–assistant–courier) hierarchy provides a principled rationale for herb compatibility and dose allocation. The Jun (monarch) directly targets the core pathogenesis and contributes the primary therapeutic force; the Chen (minister) reinforces the monarch and/or addresses key co-pathologies; the Zuo (assistant) supports the main actions, moderates toxicity or excessive properties, and may treat accompanying symptoms; and the Shi (courier) harmonizes the formula and may guide actions to specific meridians, organs, or functional axes. This framework is widely used to structure multi-herb prescriptions and explain why the entire formula can outperform individual constituents in complex diseases (Luan et al., 2020; Wu et al., 2014). Mechanistically, the hierarchy can be mapped to multi-target regulation: monarchs/ministers tend to cover high-centrality nodes and dominant pathways, whereas assistants/couriers fine-tune network topology, pharmacokinetics, and tissue distribution, thereby improving the efficacy–safety balance of the drug. Recent systems approaches, such as network pharmacology and multi-omics integration, provide quantitative tools to test such role assignments by linking herb-derived compounds to targets, pathways, and phenotypes at the module level. These approaches align with the broader concept of network pharmacology, in which polypharmacology is leveraged to modulate disease networks rather than isolated targets (Hopkins, 2008; Wu et al., 2014; Zhou et al., 2016). Therefore, making the compatibility principle explicit in anti-T2DM formulas helps readers interpret how “multi-component–multi-target” actions are organized, facilitates more reproducible mechanism annotation across studies, and provides clearer mapping between mechanistic modules and clinical outcomes (Luan et al., 2020; Cheng et al., 2017).
Major anti-T2DM classical formula lineages and their modernization derivatives
2.3
To address the potential incompleteness of the formula coverage, we expanded the anti-T2DM TCM formula section by adding a lineage-oriented summary table (Table 2). The table includes representative classical core prescriptions and their modern derivatives/commercial Chinese polyherbal preparation (CCPP) that are frequently discussed in contemporary clinical literature, spanning major TCM pattern types relevant to T2DM (e.g., heat, dampness, qi–yin deficiency, and kidney deficiency) and key complication domains (e.g., diabetic nephropathy and retinopathy). For each formula-based preparation listed in Table 2 (including proprietary/commercial Chinese polyherbal preparation (CCPP)), we report intervention identity unambiguously—dosage form, complete composition, and processing/standardization/quality control as described in the primary sources—and record missing items as NR (not reported) without inference, consistent with the GA-online Best Practice/ConPhyMP requirements. All source organisms for component botanical drugs were taxonomically validated using authoritative databases (e.g., Kew MPNS and/or Plants of the World Online), and full scientific names, including author citation and family, are provided in Table 2 and/or the accompanying identity table. We also indicated the typical mechanistic modules for each lineage to facilitate cross-study comparisons with the pathway framework in Table 1 (Tian et al., 2019; Tan et al., 2024; Hu et al., 2021a; Zhang et al., 2024).
Activation of the PI3K/Akt pathway to enhance insulin sensitivity
2.4
The PI3K/Akt module is a core insulin signaling axis that supports glucose homeostasis by promoting GLUT4 membrane translocation in skeletal muscle/adipose tissue and restraining hepatic gluconeogenesis, thereby contributing to insulin sensitivity (Schultze et al., 2012; Huang et al., 2018). In T2DM, impaired signaling is commonly reflected by reduced Akt phosphorylation and attenuated GLUT4 translocation, which correlates with insulin resistance (Tonks et al., 2013). In this review, we discuss PI3K/Akt primarily as a T2DM-relevant functional module and prioritize studies in which PI3K/Akt modulation is accompanied by metabolic outcome-linked readouts (e.g., fasting glucose, HOMA-IR/insulin tolerance, and skeletal muscle glucose uptake markers) rather than pathway readouts alone. Preclinical studies have reported that plant metabolites or defined botanical preparations can engage this module; for example, polysaccharides from Astragali Radix (source species taxonomically validated; e.g., Astragalus membranaceus (Fisch.) Bunge [Fabaceae], as reported in the primary study), have been described to enhance insulin receptor substrate (IRS)–PI3K coupling and Akt activation in diabetes-relevant models, with concurrent improvements in insulin-sensitivity-related phenotypes (Kearney et al., 2021). Puerarin (an isoflavone primarily associated with Pueraria lobata (Willd.) Ohwi [Fabaceae], as reported) has been reported to attenuates JNK-associated inhibitory signaling and preserves IRS-1/2 signaling integrity, together with improved glucose handling in experimental diabetes settings (Huang et al., 2012). At the formula level, Gegen Qinlian Decoction (GQD) is a classical multi-herb decoction; its complete composition and processing/standardization (as reported; NR if not reported) are provided in Table 2/Supplementary Table S1 GQD has been associated with reduced SOCS3 expression and enhanced skeletal muscle glucose uptake with concurrent insulin resistance improvement in preclinical studies (Jorgensen et al., 2013). Nevertheless, because PI3K/Akt is pleiotropic and broadly involved in apoptosis, lipid metabolism, and inflammatory signaling, we interpret PI3K/Akt modulation as supportive mechanistic evidence and emphasize the need for dose-plausible designs, appropriate controls, and outcome-linked endpoints when translating these findings into T2DM management.
AMPK pathway: restoring cellular energy homeostasis
2.5
AMP-activated protein kinase (AMPK) is a central energy-sensing kinase that coordinates glycolysis, fatty acid oxidation, and mitochondrial function to maintain metabolic homeostasis (Herzig and Shaw, 2018). In T2DM, nutrient overload and impaired insulin signaling are commonly associated with reduced AMPK activity, which contributes to metabolic dysregulation. In this review, we discuss AMPK primarily as a T2DM-relevant functional module and prioritize studies in which AMPK activation is accompanied by metabolic outcome-linked readouts (e.g., fasting glucose, insulin sensitivity indices, and lipid accumulation markers) rather than AMPK phosphorylation alone. Preclinical studies have reported that representative plant metabolites investigated in the TCM research context can activate this pathway. For instance, berberine (a protoberberine alkaloid commonly associated with Coptidis Rhizoma; source species taxonomically validated and provided in the Supplementary Tables/Supplementary Material) promotes AMPK phosphorylation and increases GLUT4 expression and membrane translocation in diabetes-relevant experimental settings with concurrent improvements in insulin-resistance–related phenotypes (Lee et al., 2006). Tanshinone IIA (a diterpenoid quinone from Salvia) has been reported to attenuate lipogenesis via the AMPK–ACC axis and improve lipid-related readouts in experimental models (Gao et al., 2021). Astragalus glycosides (from Astragali Radix; source species taxonomically validated and provided in the Supplementary Tables/Supplementary Material, as reported) have been described to activate AMPK and PI3K/Akt signaling in animal studies, with a concomitant enhancement of glucose uptake and insulin sensitivity (Gong et al., 2023). At the formula level, Huanglian Jiedu Decoction (Huanglian-Jiedu Decoction; HLJDT) is a classical multi-herb decoction, and its complete composition and processing/standardization (as reported; NR if not reported) are provided in Table 2/Supplementary Table S1. It has been reported to modulate fatty acid utilization markers (e.g., upregulating CPT1 and suppressing fatty acid synthase), consistent with a shift toward improved energy metabolism in preclinical studies (Hu et al., 2021b). Nevertheless, because AMPK intersects multiple biological programs beyond glucose control, we interpret AMPK-related modulation as supportive mechanistic evidence and emphasize the need for dose-plausible designs (Wang M. et al., 2024), appropriate controls, and clinically meaningful endpoints when translating these findings into T2DM management strategies.
NF-κB pathway: inhibiting inflammation and preserving insulin signaling
2.6
The NF-κB program represents a convergent inflammatory transcriptional output that is chronically engaged in obesity/T2DM and is closely linked to insulin resistance and tissue injury in the metabolic organs. In T2DM, sustained inflammatory signaling in the adipose tissue, liver, skeletal muscle, and pancreatic islets can impair insulin action and exacerbate β-cell stress, making NF-κB a disease-relevant module, rather than a purely generic pathway. Importantly, clinical proof-of-concept exists that dampening upstream inflammatory signaling (including IKKβ/NF-κB–related activity) can improve glycemic control and inflammatory biomarkers in patients with T2DM (Goldfine et al., 2010; Goldfine and Shoelson, 2017). As evidence-linked examples from the literature on TCM-related botanical drugs and plant metabolites, baicalin (a flavone glycoside primarily associated with Scutellaria baicalensis Georgi [Lamiaceae], as reported) has been reported to suppress NF-κB activation (e.g., reduced IKKβ phosphorylation and p65 nuclear translocation) in models where improvements in inflammatory readouts co-occur with better metabolic phenotypes (Shen et al., 2019). Curcumin, a widely studied plant metabolite (primarily associated with Curcuma longa L. [Zingiberaceae], as reported) has been associated with reduced inflammatory signaling alongside antioxidant responses (e.g., NRF2-related markers) in diabetes-relevant settings (Ghareghomi et al., 2021). At the formula level, Qingre Huashi Formula, a botanical preparation, was treated as a formula-based intervention with explicitly extracted intervention identity (dosage form, complete composition, and processing/standardization as reported; NR if not reported), provided in Table 2/Supplementary Table S1, and has been reported to modulate upstream innate-immune signaling (e.g., TLR4/MyD88) with concurrent reductions in pro-inflammatory cytokines and improvements in insulin signaling or vascular-related readouts (Tian et al., 2021). Nevertheless, NF-κB is pleiotropic and widely involved in many biological processes; therefore, we interpret NF-κB modulation as supportive mechanistic evidence only when accompanied by robust metabolic/complication-related endpoints. We highlight the need to account for heterogeneity in preparations, dosing forms, and study quality across preclinical and clinical datasets (including transparent reporting of composition/processing and taxonomically validated source organisms, consistent with GA-online Best Practice/ConPhyMP).
NLRP3 inflammasome: linking inflammatory stress to multi-organ injury
2.7
The NLRP3 inflammasome is a vital inflammatory module implicated in T2DM, and its activation promotes caspase-1–dependent maturation of IL-1β and IL-18, thereby contributing to β-cell stress and tissue inflammation. Human- and disease-relevant evidence links NLRP3 activation to T2DM-associated inflammatory outputs, including islet amyloid polypeptide (IAPP)-triggered inflammasome activation and obesity-associated insulin resistance (Masters et al., 2010; Vandanmagsar et al., 2011). Mechanistically, oxidative stress can promote inflammasome activation through the TXNIP–NLRP3 interaction, and NEK7 acts downstream of potassium efflux to enable NLRP3 inflammasome assembly, providing key molecular checkpoints for pathway interpretation (Zhou et al., 2010; He et al., 2016). In this review, we prioritized botanical evidence only when NLRP3-related readouts were accompanied by metabolic or complication-related endpoints. As evidence-linked examples, triptolidiol (a diterpenoid primarily derived from Tripterygium wilfordii Hook. f. Celastrol [Celastraceae] inhibits NLRP3 activation by disrupting the NLRP3–NEK7 interaction in cellular and biochemical settings (Ding MY et al., 2025). Triptolide (also primarily associated with Tripterygium wilfordii Hook.f. [Celastraceae], as reported) has been reported to ameliorates diabetic nephropathy by inhibiting the NLRP3 inflammasome pathway in vivo (Lv et al., 2023). Nevertheless, because inflammasome signaling is pleiotropic, we interpreted NLRP3 modulation as supportive mechanistic evidence only when accompanied by robust outcome-linked readouts (e.g., glycemic indices, tissue injury markers, or complication-related endpoints) and when study quality, controls, and intervention characterization were sufficiently reported (Supplementary Tables S1, S2). Step-specific clarification (revised): In the canonical two-step model, NLRP3 activation involves (i) priming (NF-κB–dependent induction of NLRP3 and pro-IL-1β) and (ii) activation/assembly (NEK7 engagement, ASC oligomerization, caspase-1 cleavage, and IL-1β/IL-18 maturation). Accordingly, we now distinguish that emodin (an anthraquinone commonly associated with Rheum palmatum L. [Polygonaceae] and related sources, as reported) is supported mainly as an activation/assembly inhibitor (blocking ASC oligomerization/pro-caspase-1 processing), whereas triptolide is supported mainly as a priming inhibitor via NF-κB. For direct assembly blockade, we cite evidence from the triptolide derivative triptolidiol, which disrupts the NLRP3–NEK7 interaction (Han et al., 2015; Shen et al., 2021; Ding X et al., 2025).
Cross-organ regulation of the gut–liver–brain–immune axis by TCM in T2DM
3
In recent years, the understanding of T2DM pathogenesis has increasingly moved beyond a purely “insulin metabolic disorder” model toward a framework that emphasizes dysregulated multi-organ crosstalk in systemic metabolic syndrome. In particular, the gut–liver–brain–immune axis is a key cross-organ network governing metabolic homeostasis, neuroendocrine regulation, and inflammatory outputs, and has been implicated in the initiation and progression of T2DM and its multi-system complications. This axis transmits gut microbiota–derived signals to the liver, brain, and immune system through mechanisms that include gut barrier integrity, bile acid signaling, short-chain fatty acids (SCFAs), and vagal-afferent sensing, thereby shaping cross-organ metabolic and immunological regulation. In this context, TCM-related botanical drugs and preparations may offer a complementary, formula-centered framework for modulating multiple nodes of this axis. However, we interpret mechanistic claims cautiously and prioritize evidence supported by outcome-linked readouts and reproducible intervention definitions (including botanical authentication and chemical characterization/QC). Where specific plant metabolites are discussed, we distinguish analytical marker metabolites (used for standardization/QC) from bioactive metabolites (hypothesis-generating candidates requiring orthogonal validation). For the formula-based botanical preparations discussed in this section, complete intervention identity (dosage form, composition, and processing/standardization as reported; NR if not reported) and taxonomically validated source organisms (full scientific names with author citation and family) are provided in Table 2 and Supplementary Table S1. To operationalize this cross-organ axis for formula interpretation, we highlight three relay nodes that connect intestinal ecology to systemic glucose–inflammation phenotypes: (i) bile acid sensing through farnesoid X receptor (FXR) and Takeda G-protein-coupled receptor 5 (TGR5), which tunes enterohepatic metabolism and incretin release; (ii) microbial short-chain fatty acids (SCFAs) engaging GPR41/43 to promote GLP-1 secretion and improve insulin sensitivity; and (iii) neuroimmune signaling via the vagus nerve and α7 nicotinic acetylcholine receptor (α7nAChR) that restrains inflammatory outputs. Using this node-based lens, we further summarized evidence that Huanglian Jiedu Decoction (Huang-Lian-Jie-Du Decoction; HLJDT), a classical multi-herb decoction (identity/QC as reported; NR if not reported; see Table 2/Supplementary Table S1), improves hyperglycemia with concomitant restoration of SCFA-producing microbiota, whereas Liuwei Dihuang Wan (Liu-Wei-Di-Huang Pills; LWDHW), a classical multi-herb pill preparation (identity/QC as reported; NR if not reported; see Table 2/Supplementary Table S1), modulates gut microbiota–SCFA profiles with a proposed SCFAs–GPR43/41–GLP-1 link, thereby providing a tractable mechanistic bridge from classical formulas to cross-organ communication (Katsuma et al., 2005; Trabelsi et al., 2015; Chen et al., 2018; Yi et al., 2022; Tracey, 2002; Wang et al., 2003; Wang D et al., 2022) (Figure 3).
Node-based model of TCM regulation of the gut–liver–brain–immune axis in T2DM. HLJDT and LWDHW (and representative metabolites such as berberine, gardenoside, and rhein) remodel dysbiotic microbiota, increasing SCFA-producing taxa and reshaping the bile acid (BA) pool. SCFAs and BA signaling enhance enteroendocrine GLP-1 release and engage the intestinal FXR/TGR5 pathways, improving insulin secretion and metabolic control. Concurrently, vagus–α7nAChR neuroimmune signaling suppresses NF-κB–linked macrophage cytokine output, whereas hepatic FXR–SHP and CYP7A1-related regulation reduce gluconeogenesis, lipogenesis, and inflammation. Green/blue arrows indicate restorative effects; red/dashed arrows indicate pathological routes; T-bars indicate inhibition.
Gut–liver–bile-acid–FXR/TGR5 axis
3.1
In addition to lipid absorption, bile acids act as endogenous signaling molecules by activating the farnesoid X receptor (FXR) and G protein-coupled bile acid receptor (TGR5), thereby coordinating glucose–lipid metabolism, inflammatory outputs, and secretion of the gut hormone GLP-1. In T2DM, this axis can be perturbed, with reports describing altered bile acid composition, impaired incretin responses (including reduced GLP-1 output), and amplification of gut–liver inflammatory signaling. Mechanistically, TGR5 activation in enteroendocrine L cells stimulates cAMP signaling and GLP-1 secretion (Katsuma et al., 2005), whereas intestinal FXR activity suppresses proglucagon/GLP-1 production, positioning the BA–FXR/GLP-1 pathway as a bidirectional modulator of glucose homeostasis (Trabelsi et al., 2015). These findings support the view that BA receptor signaling is a “gut–liver–incretin” checkpoint that can be influenced by microbiota-driven bile acid remodeling. In TCM-related research, botanical preparations and representative plant metabolites have been reported to engage multiple nodes within the bile acid receptor network; however, we interpret mechanistic claims cautiously and prioritize studies linking pathway modulation to metabolic or complication-relevant endpoints. For example, the plant metabolite rhein (an anthraquinone primarily associated with Rheum palmatum L.[Polygonaceae] and related sources, as reported) has been reported, suppresses CYP7A1 transcription via epigenetic regulation, thereby reducing primary bile acid synthesis and attenuating hepatic inflammatory readouts (Hu et al., 2024). Gardenoside, a plant metabolite (an iridoid glycoside primarily associated with Gardenia jasminoides J.Ellis [Rubiaceae]), has been described as a TGR5 agonist associated with increased GLP-1 secretion and improved insulin sensitivity in diabetes-relevant conditions. Berberine, a widely studied plant metabolite (commonly associated with Coptidis Rhizoma; source organisms taxonomically validated and provided in the Supplementary Tables/Supplementary Material, as reported), has been reported to remodel the bile acid pool composition and engage both FXR–small heterodimer partner (SHP) and TGR5–GLP-1 signaling axes (Wang Y. et al., 2024; Xie et al., 2020). Notably, some bile-acid–related metabolites may serve as analytical marker metabolites for standardization/QC rather than proven bioactive metabolites; therefore, causal claims should be supported by orthogonal validation and outcome-linked readouts. Collectively, these studies support the bile acid receptor network as a plausible cross-organ regulatory module relevant to gut–liver axis dysfunction in T2DM.HLJDT has been reported to ameliorate hyperglycemia and insulin resistance in T2DM rats while restoring dysregulated gut microbiota structure and function, notably increasing SCFA-producing taxa and modulating bile acid biosynthesis-related functions (Chen et al., 2018). Consistently, Liuwei Dihuang Wan (Liu-Wei-Di-Huang Pills; LWDHW), a classical multi-herb pill preparation (complete composition and processing/standardization as reported; NR if not reported; see Table 2/Supplementary Table S1), improved glycemic indices and SCFA profiles in GK rats, with mechanistic analyses suggesting the involvement of the SCFAs–GPR43/41–GLP-1 pathway (Yi et al., 2022). Together, these studies illustrate how classical formulas can be interpreted through a microbiota–SCFA–incretin relay, linking intestinal ecology to systemic metabolic control.
Modulating the gut microbiota–SCFA–GLP-1 axis to restore metabolic homeostasis
3.2
Beyond metabolic relays, the vagus-mediated cholinergic anti-inflammatory pathway provides a neuroimmune gate in which α7nAChR signaling suppresses pro-inflammatory cytokine release (Tracey, 2002; Pavlov and Tracey, 2005; Wang et al., 2003). In experimental diabetes models, berberine, an isoquinoline alkaloid abundant in Coptis chinensis Franch. [Ranunculaceae] and commonly present in HLJDT-related prescriptions, has been shown to improve glucose metabolism via an α7nAChR-dependent mechanism, supporting a plausible vagus–α7nAChR node for formula-related neuroimmune modulation (Wang X et al., 2022). Nevertheless, direct formula-level evidence linking HLJDT/LWDHW to vagal tone or α7nAChR activation remains limited; therefore, we frame this node as hypothesis-generating and requiring targeted validation in formula- and complication-specific settings in the future. As our understanding of the systemic pathogenic mechanisms of T2DM advances, the gut microbiota–SCFA–GLP-1 axis, which links microbiota-derived signals to pancreatic and enteroendocrine function, has emerged as a plausible cross-organ regulatory module relevant to the restoration of metabolic dysregulation. High-fat diets and metabolic dysregulation commonly disrupt the gut microbiota, with reports describing reductions in butyrate-producing taxa (e.g., Faecalibacterium and Roseburia) and decreased SCFA production, particularly butyrate (Zhang et al., 2023). SCFA deficiency is associated with impaired Treg differentiation, compromised gut barrier integrity, and attenuated incretin responses (including TGR5-associated GLP-1 output), thereby worsening insulin resistance and glycemic control (Lin et al., 2025). In the context of TCM-related research, botanical preparations and representative plant metabolites have been reported to engage multiple nodes within this axis; however, we prioritized studies in which microbiota/SCFA changes were accompanied by outcome-linked metabolic readouts (e.g., glycemia and insulin sensitivity indices) and interpreted the associative microbiome findings cautiously. Berberine, a widely studied plant metabolite, has been reported to increase microbiota diversity and enrich butyrate-producing taxa, with concurrent increases in SCFA/butyrate levels and improved metabolic phenotypes, and to modulate gut endocrine signaling, including GLP-1-related pathways (Wang Y et al., 2017; Zhang et al., 2020; Li M. et al., 2020). Gardenoside, a plant metabolite primarily associated with Gardenia jasminoides J.Ellis [Rubiaceae], as reported) a plant metabolite described as a TGR5 agonist, has been reported to stimulate GLP-1 secretion and improve insulin-related outcomes (Wang et al., 2022). Rhein, an anthraquinone primarily associated with Rheum palmatum L. [Polygonaceae] and related sources, has been reported to attenuate hepatic inflammation via FXR/SHP-related signaling, supporting improved gut–liver metabolic coupling in diabetes-relevant settings (Zhao et al., 2024). For formula-based botanical preparations mentioned in this section (e.g., HLJDT/LWDHW), complete intervention identity (dosage form, composition, and processing.
Standardization, as reported (NR, if not reported), and taxonomically validated source organisms (full scientific names with author citation and family) are provided in Table 2 and Supplementary Table S1. Notably, some microbiota- and SCFA-associated metabolites may be used as analytical marker metabolites for standardization/QC rather than proven bioactive metabolites; therefore, causal claims should be supported by orthogonal validation and well-controlled experimental designs. These plant metabolites act through a three-stage sequence—“metabolite recognition → immune metabolic remodeling → GLP-1-axis activation”—to restore metabolic homeostasis in the host.
Modulating the gut–brain–vagus nerve axis to enhance central energy sensing
3.3
The gut–brain axis integrates neuronal sensing, immune responses, and endocrine signaling to regulate energy intake and systemic metabolic homeostasis. The vagus nerve, a principal conduit linking the gastrointestinal tract to the central nervous system (CNS), plays a key role in conveying gut-derived signals relevant to energy balance (Mayer, 2011). In T2DM, pathological alterations, including impaired gut sensory signaling, hypothalamic inflammation, and POMC neuron dysfunction, are linked to abnormal central nutrient sensing and downstream metabolic dysregulation (Thaler et al., 2012; Caudy et al., 2003). In TCM-related research, multi-botanical preparations and representative plant metabolites have been reported to modulate nodes within gut–brain signaling (e.g., such as vagal-afferent sensing, neuroinflammation, and neuroendocrine outputs). However, we prioritized evidence supported by outcome-linked metabolic readouts and reproducible intervention definitions (including botanical authentication and chemical characterization/quality control). For example, ginsenoside Rg1 (a triterpenoid saponin primarily derived from Panax ginseng C.A.Mey. [Araliaceae], as reported) has been reported to modulate cholinergic anti-inflammatory signaling, including its effects on α7 nicotinic acetylcholine receptor (α7nAChR) expression/function in preclinical neuroinflammation-related settings (Feng et al., 2022). In addition, polysaccharides from Wolfiporia extensa (Peck) Ginns [Polyporaceae] (*syn. Poria cocos (*as reported) has been reported to engage innate immune signaling (e.g., TLR2/4–MyD88–NF-κB–related pathways) in preclinical systems, which may indirectly influence gut–brain inflammatory tone, although diabetes-specific causal evidence and gut–vagal endocrine readouts remain limited and should be interpreted cautiously (Chang et al., 2009; Jia et al., 2016). Collectively, these studies support a plausible gut–brain modulatory role for TCM-related interventions, but stronger translational inference requires standardized preparations, appropriate controls, and replication in T2DM-relevant models with clinically meaningful or outcome-linked endpoints (including transparent reporting of source organism identity and extract characterization as reported; NR if not reported, consistent with GA-online Best Practice/ConPhyMP).
Pharmacological mechanisms of TCM in managing major complications of T2DM
4
T2DM is not merely a disorder of glucose metabolism but a multifaceted metabolic syndrome characterized by multi-system dysregulation (Forbes and Cooper, 2013). The clinical burden of diabetes is largely driven by the onset and progression of multi-organ complications, including diabetic nephropathy (DN), diabetic retinopathy (DR), diabetic cardiomyopathy (DCM), and diabetes-associated cognitive decline (DCD) (Forbes and Cooper, 2013). Although these complications involve diverse tissues and organs, their pathogenic mechanisms substantially overlap, featuring chronic inflammatory activation, impaired redox homeostasis/oxidative stress, compromised insulin signaling, and dysregulated cell death pathways (Forbes and Cooper, 2013; Giacco and Brownlee, 2010). Contemporary standard-of-care therapies (e.g., glucose-lowering agents with cardio–renal benefits) improve glycemic control and reduce complication risk; however, residual risk remains, and disease progression is not fully prevented in many patients, highlighting the need for complementary strategies targeting broader pathogenic modules (American Diabetes Association Professional Practice Committee, 2025a; American Diabetes Association Professional Practice Committee, 2025b). Conventional antidiabetic drugs can also exhibit multi-target and multi-organ actions (e.g.,metformin), reflecting the complexity of T2DM pathophysiology (Rena et al., 2017). In this context, TCM-related multi-botanical preparations (formula-based interventions)—because they comprise multiple constituents—provide a complementary, formula-centered framework that may co-modulate overlapping pathogenic modules (e.g., inflammation, oxidative stress, insulin signaling, and neuroendocrine regulation), thereby supporting integrative organ protection and complication management. Where relevant, we distinguished plant metabolites (e.g., bioactive candidates) from analytical marker metabolites used for standardization/quality control and prioritized evidence in which mechanistic readouts were accompanied by outcome-linked endpoints. This section systematically reviews the research progress and preclinical and clinical evidence on TCM-related botanical preparations for these four representative complications, aiming to offer theoretical support and evidence-based strategies for the comprehensive prevention and treatment of T2DM complications (Figure 4).
Convergence-module framework linking multi-component TCM to shared drivers and organ-specific complications of T2DM. Upstream metabolic insults (chronic hyperglycemia, insulin resistance, and lipotoxicity) feed into a shared inflammation–oxidation–stress network composed of three clusters: oxidative stress/mitochondrial dysfunction (ROS; NRF2/HO-1 redox defense), innate inflammatory signaling (TLR4/RAGE–NF-κB and NLRP3 inflammasome with IL-1β/TNF-α output), and cellular stress and remodeling (ER stress IRE1α–XBP1; TGF-β/SMADs fibrosis; VEGF angiogenesis). TCM formulas and bioactive metabolites act as integrated, multi-target interventions to restore redox balance and suppress inflammatory cascades, thereby modulating downstream organ-specific pathways in diabetic nephropathy, retinopathy, cognitive decline, cardiomyopathy, and peripheral neuropathy, with corresponding clinical readouts.
Alleviating renal fibrosis and oxidative stress in DN
4.1
DN is one of the most common microvascular complications of T2DM and is characterized by thickening of the glomerular basement membrane, mesangial matrix expansion, and interstitial fibrosis (Tervaert et al., 2010). Under persistent hyperglycemia, the TGF-β/SMAD signaling pathway is activated, while advanced glycation end-products (AGEs) and their receptor for advanced glycation end-products (RAGE)-mediated inflammatory cascades are enhanced, accompanied by downregulation of the NRF2 pathway, thereby increasing oxidative stress and aggravating renal injury (Li et al., 2019; Bakris et al., 2010; Guo et al., 2022). Multiple studies have shown that TCM can effectively slow DN progression through multiple target mechanisms. Astragali Radix–related interventions (source species taxonomically validated; e.g., Astragalus membranaceus (Fisch.) Bunge [Fabaceae], as reported) downregulates TGF-β expression and activity, thereby reducing collagen deposition and attenuating glomerulosclerosis (Chen and Gould, 2008). Tanshinone IIA (primarily derived from Salvia miltiorrhiza Bge. [Lamiaceae], as reported) significantly activates the NRF2/HO-1 pathway, enhancing antioxidant capacity, diminishing reactive oxygen species (ROS) accumulation, and inhibiting cell apoptosis (Wang F et al., 2017). Moreover, Huang Kui capsules (a proprietary botanical preparation; complete composition, dosage form, and processing/standardization/QC as reported; NR if not reported; see Table 2 and Supplementary Table S1) improved the estimated glomerular filtration rate (eGFR) and reduced proteinuria in a multicenter clinical trial, suggesting its potential for renal protection (Gao et al., 2020; Munyangi et al., 2018). Systems pharmacology and network analysis further revealed that TCM formulas in DN intervention can co-regulate core pathways of “inflammation–oxidation–apoptosis,” thereby achieving system-level control of the pathological network. For instance, animal experiments have demonstrated that HLJDT significantly reduces 24-hour urine protein excretion in STZ-induced diabetic rats (∼35% reduction, as reported) and reduces TGF-β1 and collagen I expression in renal tissues (∼40% reduction in immunohistochemistry score, as reported), further supporting its multi-pathway mechanism (Cai et al., 2025).
Suppressing pathological angiogenesis in DR
4.2
DR is a predominant cause of adult blindness, with pathogenesis centered on hypoxia-induced upregulation of hypoxia-inducible factor-1α (HIF-1α), which promotes vascular endothelial growth factor (VEGF) expression and triggers aberrant neovascularization (Helmerhorst et al., 2009). Concurrently, hyperglycemia elevates ROS levels and increases vascular permeability, contributing to retinal injury and persistent loss of vision (Hinton et al., 2002). In the context of TCM-related research, botanical preparations and representative plant metabolites have been reported to engage in DR-relevant pathogenic modules (e.g., hypoxia–angiogenesis signaling, oxidative stress, and inflammatory outputs); however, we prioritized studies in which mechanistic readouts were accompanied by outcome-linked retinal endpoints and reproducible intervention definitions. Specifically, ginsenoside Rg1 suppresses HIF-1α expression, thereby attenuating hypoxia-induced angiogenic signaling (Niu et al., 2016). Baicalin inhibits vascular endothelial growth factor receptor 2 (VEGFR2) signaling, with reported reductions in retinal neovascularization in diabetes-relevant settings (Rossino and Casini, 2019). Curcumin and flavonoids from Cassia obtusifolia L. [Fabaceae] have been linked to NRF2-related redox responses, mitigating hyperglycemia-associated oxidative stress (Forman and Davies, 2016; Shao et al., 2020). Preclinical evidence further supports these mechanistic observations when paired with disease-relevant outcomes in humans. For example, baicalin has been reported to reduce VEGF expression in high-glucose-induced ARPE-19 retinal epithelial cells and downregulate the TLR4/NF-κB inflammatory pathway (Sabry et al., 2024). In STZ-induced diabetic mice, oral baicalin (50 mg/kg) was associated with a decreased retinal neovascularization area (Gong et al., 2025). At the clinical evidence level, Qiming Granules (a formula-based botanical preparation; complete composition, dosage form, and processing/standardization/QC as reported; NR if not reported; see Table 2 and Supplementary Table S1) in combination with anti-VEGF therapy have been reported to reduce the frequency of vitreous injections and improve macular edema and visual-function–related outcomes, supporting its potential as an adjunctive strategy; nevertheless, these findings should be interpreted in light of trial design, intervention standardization/QC, and outcome definitions (Hu et al., 2021c).
Modulating neuroinflammation and mitochondrial function in diabetes-associated cognitive decline
4.3
DCD is a major CNS complication of T2DM that clinically manifests as impaired learning and memory, spatial disorientation, and executive dysfunction (Guimaraes et al., 2023). Studies indicate that DCD pathogenesis reflects convergent mechanisms, including PI3K/Akt dysregulation, mitochondrial dysfunction, and polarization of microglia toward an M1 pro-inflammatory phenotype, which together contribute to neuronal damage and synaptic dysfunction. Meanwhile, sustained activation of TLR4/NF-κB inflammatory signaling is proposed as a disease-relevant inflammatory module in DCD progression, promoting the release of inflammatory mediators (e.g., IL-1β, TNF-α) that can intensify neurotoxicity and cognitive deficits (Mohrin et al., 2021; Lin and Beal, 2006; Miah et al., 2020; Peters et al., 2021). With the proposal of the “neuro-inflammation–metabolism coupling” network concept, regulating key nodes within this network has gradually become a potential intervention for diabetes-related brain dysfunction. In this context, TCM-related research has garnered interest because of its reported ability to modulate neuroimmune–metabolic interactions. Multiple studies suggest that TCM-related botanical preparations and representative plant metabolites may confer system-level protection in DCD via multi-target mechanisms, although we prioritized evidence in which mechanistic readouts are accompanied by outcome-linked neurobehavioral or neuropathological endpoints and reproducible intervention definitions. For example, Ginkgo biloba L. [Ginkgoaceae] extract (standardization/characterization as reported; NR if not reported) has been reported to engage the PI3K/Akt/BDNF axis, with associated improvements in synaptic plasticity and neurorepair-related outcomes (Diaz-Amarilla et al., 2022). Gastrodin (a phenolic glycoside primarily associated with Gastrodia elata Blume [Orchidaceae]) has been reported to inhibit TLR4/NF-κB signaling, with concurrent reductions in CNS inflammatory markers (Wong et al., 2023). Liuwei Dihuang Pill has been reported to upregulate hippocampal BDNF levels and improve learning and memory in T2DM animal models (Behl et al., 2022). Subsequent experimental studies have further supported the neuroprotective potential of TCM-related interventions in cognitive impairment models. In the APP/PS1 transgenic mouse model, ginsenoside Rg1 has been reported to improve spatial memory performance, with concurrent changes in hippocampal BDNF protein expression and Akt phosphorylation, suggesting that its cognitive effects may involve PI3K/Akt–BDNF-linked signaling in that model context (Zhang et al., 2025; Nie et al., 2017). For formula-based botanical preparations and extracts discussed in this section, intervention identity (composition and processing/standardization as reported; NR if not reported) and taxonomically validated source organisms (full scientific names including author citation and family) are provided in Table 2 and Supplementary Table S1.
Enhancing antioxidant defense and reducing myocardial stress in diabetic cardiomyopathy
4.4
DCM is a common and severe cardiovascular complication in T2DM patients, characterized by myocardial hypertrophy, impaired diastolic function, and a substantially increased risk of heart failure (Badran et al., 2024). Unlike vascular heart diseases such as atherosclerosis, DCM primarily manifests as intrinsic myocardial structural and functional abnormalities that are not solely explained by epicardial coronary artery disease. This pathological progression is associated with mitochondrial dysfunction, sustained endoplasmic reticulum stress (ERS), and disrupted calcium homeostasis (Bugger and Abel, 2014; Jia et al., 2018). At the molecular level, convergent stress responses involving redox dysregulation and ERS signaling have been proposed as key drivers of cardiomyocyte injury and functional decline in DCM patients. Notably, downregulation of the NRF2–antioxidant response element (ARE) pathway compromises the endogenous antioxidant capacity of the cardiomyocytes (Barancik et al., 2016). In parallel, abnormal activation of the IRE1α–XBP1 axis may amplify cellular stress and pro-apoptotic signaling, thereby exacerbating myocardial damage and decompensation. In TCM-related research, botanical preparations and representative plant metabolites have been reported to engage stress response modules in DCM-relevant models. For example, icariin (a prenylated flavonol glycoside primarily associated with Epimedium brevicornu Maxim. [Berberidaceae] and related Epimedium sources, as reported) has been reported to activates NRF2-related signaling, increases SOD2-associated antioxidant readouts, reduces lipid peroxidation (MDA-related readouts), and suppresses the IRE1α–XBP1 axis, consistent with a reduced ERS burden (Li C et al., 2022; Zheng Y. et al., 2022; Zheng J. et al., 2022). Network pharmacology analyses further suggested that TCM-related interventions may co-modulate multiple nodes across the AMPK, PI3K/Akt, Ca2+/calmodulin-dependent protein kinase II (CaMKII), and related signaling pathways. However, we interpret in silico pathway–target networks as hypothesis-generating unless supported by outcome-linked experimental validation. For the formula-based botanical preparations discussed in this section, intervention identity (dosage form, complete composition, and processing/standardization as reported; NR if not reported) and taxonomically validated source organisms (full scientific names including author citation and family) are provided in Table 2 and Supplementary Table S1. At the metabolite level, tanshinone IIA, a representative plant metabolite from the TCM-related botanical drug Salvia, has been reported to exhibit antioxidant and antiapoptotic properties in cell-based and animal models. In high-glucose-treated H9c2 cardiomyocytes, the reported IC_50_ is 12.6 μM (as reported), with concurrent increases in SOD2 expression and reductions in malondialdehyde (MDA) content (Ji et al., 2018). In STZ-induced diabetic mice, tanshinone IIA treatment was associated with reduced cardiac TUNEL-positive cells, suggesting potential myocardial protection in that model, possibly involving Nrf2/HO-1–linked responses (Moura et al., 2021). Nevertheless, mechanistic reports remain heterogeneous in terms of model choice, exposure/dose ranges, and intervention definition/standardization (including botanical authentication and chemical characterization/QC), and pathway interactions are not consistently tested using orthogonal readouts. Therefore, further studies should prioritize reproducible intervention definitions, dose–response characterization with appropriate controls and outcome-linked endpoints to clarify the key regulatory targets and translational potential of anti-DCM strategies.
Addressing diabetic peripheral neuropathy (DPN): transient receptor potential vanilloid 1 (TRPV1)-Linked nociceptive sensitization and PI3K/Akt-mediated neurorepair
4.5
Diabetic peripheral neuropathy (DPN) is one of the most prevalent and disabling complications of T2DM and commonly presents as distal symmetric neuropathy with pain, paresthesia, and sensory loss, substantially impairing the quality of life and increasing the risk of foot ulceration and amputation (Pop-Busui et al., 2017; Eid et al., 2023). Given its high disease burden and close association with metabolic stress and microvascular dysfunction, we added DPN as a dedicated complication section to align the chapter structure with clinical epidemiology and therapeutic needs. Mechanistically, DPN reflects the convergence of hyperglycemia- and dyslipidemia-driven bioenergetic failure, axon–Schwann cell dysfunction, and neuroimmune activation. In painful DPN, peripheral sensitization is critically shaped by the remodeling of nociceptors and ion channels. TRPV1 in dorsal root ganglion neurons is a well-supported effector of diabetic neuropathic pain and can be potentiated by upstream inflammatory signaling (Xie et al., 2022; Wang A et al., 2021; Chen et al., 2022). Accordingly, an integrative anti-DPN strategy should combine the suppression of neuroinflammatory amplification with the restoration of neurorepair programs (e.g., Schwann-cell autophagy/myelination and axonal support), rather than focusing on analgesia alone (Eid et al., 2023; Yang et al., 2025). From the TCM perspective, “blood-activating” and “Qi-tonifying” herbs frequently used in T2DM-related neuropathic symptom clusters—such as Angelica sinensis (Oliv.) Diels [Apiaceae], Ligusticum chuanxiong Hort. [Apiaceae], and Astragalus membranaceus (Fisch.) Bunge [Fabaceae]can be interpreted in modern neurobiology as modulators of pain-related ion channels and pro-repair signaling. A TRP-channel-oriented literature synthesis indicates that multiple TCM herbs/ingredients regulate thermo-TRP channels (including TRPV1) relevant to nociceptive sensitization (Yan et al., 2022). Importantly, astragaloside IV—a triterpenoid saponin primarily associated with Astragalus membranaceus (Fisch.) Bunge [Fabaceae], as reported, attenuates Schwann cell injury and improves peripheral nerve function in DPN models, in part through miR-155–linked autophagy regulation, with involvement of the upstream PI3K/Akt/mTOR axis (Yin et al., 2021). In addition, Danggui-containing classical prescriptions, such as Danggui Sini Decoction (Danggui-Sini Decoction; a classical multi-herb decoction; complete composition, dosage form, and processing/standardization/QC as reported; NR if not reported; see Table 2 and Supplementary Table S1), have shown experimental/clinical evidence of alleviating diabetic neuropathic pain with reduced glial activation and pro-inflammatory cytokines in the spinal cord, providing a tractable bridge between traditional practice and neuroinflammation-focused mechanisms (Liu et al., 2017).
Integrated TCM strategies for multi-organ complication management in T2DM: common mechanisms and graph-based therapeutic modeling
4.6
Shared pathophysiological mechanisms among T2DM complications
4.6.1
Although DN, DR, DCM, and DCD manifest in distinct organs, they share a hierarchical pathobiological cascade rather than a single linear axis. Upstream metabolic insults (chronic hyperglycemia, insulin resistance, and lipotoxicity) activate canonical biochemical pathways (AGE–RAGE signaling, polyol/hexosamine flux, and PKC activation) and establish metabolic/epigenetic “memory,” which drives endothelial dysfunction and microvascular injury. These vascular changes intersect with mitochondrial dysfunction/redox imbalance, ER stress, impaired autophagy/mitophagy, and inflammatory signaling (including TLR4–NF-κB and NLRP3 inflammasome activation with downstream IL-1β/IL-18 and pyroptotic cell death). Downstream, each organ expresses dominant remodeling outputs: transforming growth factor beta (TGF-β)/SMAD-mediated fibrosis in the kidney and heart (DN/DCM), vascular endothelial growth factor (VEGF)-driven pathological angiogenesis and barrier breakdown in the retina (DR), and neurovascular unit dysfunction with mixed vascular–neurodegenerative pathology in the brain (DCD). Therefore, we revise the “oxidative stress–inflammation/NLRP3” triad from a unifying label to a central convergence module embedded within a broader network that includes vascular dysfunction, metabolic memory, and organ-specific remodeling programs, providing a more accurate and comprehensive integrative framework for multi-organ complication management in T2DM (Brownlee, 2005; Forbes and Cooper, 2013; Chen and Natarajan, 2022; Xue et al., 2023; Li et al., 2023; Biessels and Despa, 2018).
Multi-target synergy of TCM in multi-organ regulation
4.6.2
TCM emphasizes a strategy of “syndrome differentiation–based treatment, multi-pathway integration, and holistic regulation,” conferring multi-target and multi-system synergy for system-level disease intervention. Research indicates that certain TCM formulas can target multiple pathological aspects of T2DM in a single intervention. Botanical preparations containing Astragali Radix (source species taxonomically validated; e.g., Astragalus membranaceus (Fisch.) Bunge [Fabaceae], as reported) and Salvia miltiorrhiza Bge. [Lamiaceae] have been reported to engage PI3K/Akt- and NRF2–HO-1–related signaling, consistent with the mitigation of oxidative-stress–linked injury in cardiovascular and nervous-system–relevant models. Furthermore, Panax ginseng C. A. Meyer [Araliaceae] and Scutellaria baicalensis Georgi [Lamiaceae]-related interventions have been reported to modulate TLR4/NF-κB and HIF-1α/VEGF signaling, consistent with the suppression of pathological angiogenesis in retinal and neurovascular contexts. The clinical evidence was interpreted in an evidence-graded manner and is summarized in Supplementary Table S2. For ocular outcomes in diabetic retinopathy, randomized trial syntheses of oral Chinese commercial Chinese polyherbal preparation (CCPP) support improvements in visual and retinal endpoints, although the primary study reporting quality is frequently limited (Liu et al., 2023). For diabetic nephropathy–related renal outcomes, meta-analytic evidence suggests the potential benefits of Liuwei Dihuang–based interventions (formula identity, composition, and processing/standardization as reported; NR if not reported; see Table 2 and Supplementary Table S1) on renal function/proteinuria, but heterogeneity and trial-quality limitations remain important (Gao et al., 2018). Accordingly, we avoid over-interpreting pathway “hits” from network pharmacology or single-assay readouts, given assay interference/PAINS liabilities, and prioritize studies with outcome-linked endpoints and reproducible intervention definitions (Baell and Holloway, 2010; Dahlin et al., 2021).
Building a multi-dimensionall graph-based TCM intervention map for T2DM
4.6.3
It is essential to establish a Five-Dimensional Intervention Map (FDIM) centered on the core dimensions of “botanical preparation (formula)–plant metabolite–pathway–organ–disease” to enable systematic modeling and visual representation of TCM interventions for T2DM complications. This map, which integrates system pharmacology, multi-omics, and graph neural networks (GNNs), comprehensively describes the cross-level regulatory pathways of multi-botanical formulations. By embedding “botanical preparation–plant metabolite–target–pathway–organ–disease–phenotype” relationships in a heterogeneous GNN, intervention pathway inference, plant metabolite contribution ranking, and key target identification can be achieved in the context of comorbid diseases (Lin et al., 2020; Shi et al., 2022). Graph attention networks (GATs) may further improve the identification of core action nodes (e.g., PI3K, NLRP3, and BDNF) and enhance the biological interpretability of the model (Wolf et al., 2011; Paparozzi et al., 2025). Moreover, the integration of spatial transcriptomics with organoid platforms enables tissue-level validation of map-predicted targets and pathways, thereby closing the loop from mechanistic prediction to experimental verification and advancing the systematic modernization of TCM pharmacological research (Wesemann, 2022; Ho et al., 2020). In conclusion, the potential value of TCM-related interventions for T2DM multi-organ complications may stem from integrated module-level co-regulation. Building a multi-dimensional graph map model could help uncover action networks of multi-botanical preparations and provide a structured decision-support framework for personalized intervention strategies, while distinguishing analytical marker metabolites (for QC) from bioactive candidate metabolites (for efficacy hypotheses).
Clinical evidence and modernization challenges of TCM in T2DM
5
Although TCM-related botanical preparations (multi-botanical preparations) have accumulated substantial experimental and theoretical evidence for engaging multiple T2DM-relevant pathogenic modules, their clinical translation within contemporary healthcare systems is constrained by several limitations. Key bottlenecks include an insufficiently evidence-graded clinical evaluation framework, delayed or inconsistent safety assessments, and a lack of standardized and internationally aligned pathways for implementation and dissemination. In addition, translation is often hindered by variability in botanical drug sourcing and the standardization of botanical preparations, including incomplete quality control strategies that distinguish analytical marker metabolites (for QC/standardization) from bioactive candidate metabolites (for efficacy). In recent years, advances in evidence-based medicine have yielded an increasing number of higher-quality randomized controlled trials (RCTs) evaluating TCM-related botanical preparations for T2DM, which helps strengthen the clinical evidence base for modernization and supports more standardized clinical application (Figure 5).
Roadmap for modernizing evidence-based integrated TCM in T2DM care. The schematic summarizes the current bottlenecks in clinical evidence/evaluation, safety and pharmacovigilance (including herb–drug interactions and compound-specific risks), and standardization/quality control of botanical preparations. Proposed solutions include integrative system models (formula–metabolite–target–phenotype mapping), multi-omics profiling to quantify exposure-linked signatures, harmonized multicenter clinical trials with standardized endpoints, and GMP-aligned manufacturing with third-party quality control and traceability. Together, these steps support a future vision of robust clinical evidence, standardized and reproducible interventions, and pragmatic integration of TCM into T2DM care pathways with proactive safety monitoring and personalized systems-level management.
Accumulated evidence from randomized controlled trials
5.1
Numerous randomized controlled trials (RCTs) and meta-analyses have reported that TCM-related multi-botanical preparations (formula-based interventions) can improve key metabolic endpoints in T2DM, supporting an evidence base that is strongest when the intervention is clearly defined and standardized. HLJDT combined with metformin has been reported to decrease HbA1c levels by approximately 1.3% (as reported) and improve (reduce) insulin resistance (replace “(18)” with a standard author–year citation). Regarding complications, Qiming Granules (a formula-based botanical preparation; intervention identity and QC/standardization as reported; NR if not reported; see Table 2 and Supplementary Table S1) combined with anti-VEGF therapy have been reported to reduce intravitreal injection frequency and alleviate macular edema (Zhang et al., 2024). In renal protection, a multicenter RCT study involving 268 T2DM patients demonstrated that Huang Kui Capsules (a proprietary botanical preparation; intervention identity and QC/standardization as reported; NR if not reported; see Table 2 and Supplementary Table S1) stabilized the estimated glomerular filtration rate (eGFR) and reduced proteinuria levels (Wen et al., 2025). Across studies, interpretation should consider concomitant therapies, dosage forms, and quality control, including the use of analytical marker metabolites for standardization (distinct from hypothesized bioactive candidate metabolites). Collectively, these findings suggest that TCM-related botanical preparations may provide multi-endpoint, multi-organ benefits in glycemic control, organ protection, and complication management, and motivate further well-designed trials and pragmatic/real-world evaluations to support their integration into contemporary T2DM care.
Pharmacovigilance and safety profiling of TCM interventions
5.2
Although most TCM formulas are derived from classic pharmacopoeias and are widely used in practice, potential safety risks remain in contemporary clinical settings, especially in long-term interventions and multi-drug combinations. Certain bioactive plant metabolites, such as triptolide and rhein, may induce transaminase elevation or nephrotoxicity at high doses (Hu et al., 2022; Cheng et al., 2020). Several studies have indicated that TCM-related botanical drugs (e.g., Angelica sinensis (Oliv.) Diels [Apiaceae], Salvia miltiorrhiza Bge. [Lamiaceae], Glycyrrhiza uralensis Fisch. ex DC. [Fabaceae] (and/or other Glycyrrhiza source species, as reported)) may markedly increase the risk of bleeding when used in conjunction with anticoagulants or antiplatelet medications (e.g., warfarin and aspirin) (Li LR et al., 2022). Although the Chinese Pharmacopoeia institutes certain quality control criteria for TCM, systematic construction of adverse event databases, dose–toxicity thresholds, and evidence of chronic toxicology remain insufficient. Therefore, it is urgent to build a multi-dimensional safety assessment framework focused on “plant metabolite identification (including analytical marker metabolites for QC)–metabolic characteristics–toxicity mechanisms–pharmacokinetics,” combining real-world evidence and pharmacoepidemiology platforms to achieve dynamic monitoring and precise management of TCM clinical safety. Notably, the diterpenoid epoxide triptolide (primarily derived from Tripterygium wilfordii Hook. f. [Celastraceae], as reported) represents a well-recognized high-risk TCM-derived compound with a narrow therapeutic window. Experimental and clinical reports have linked it to dose- and time-dependent hepatotoxicity (e.g., ALT/AST elevation and cholestatic features) and nephrotoxicity. Although certain Tripterygium preparations (intervention identity and processing/standardization as reported; NR if not reported) provide approximate clinical dosing ranges (e.g., daily triptolide exposure in the hundreds of micrograms), a universally accepted human “toxicity threshold” is not clearly defined and is further modified by CYP/P-gp–mediated exposure, co-medications, and host susceptibility. For anthraquinones, emodin (present in Rheum spp.; source species taxonomically validated as reported; see Supplementary Table S1) has been reported to show bidirectional hepatic effects with toxicity signals at high concentrations/prolonged exposure and kidney injury signals in some toxicology datasets. However, dose–toxicity boundaries remain inconsistent across models, and sub-chronic animal studies at moderate doses may show minimal hepatic/renal injury. Therefore, in long-term administration and polypharmacy settings, we emphasize a pragmatic safety principle: prioritize standardized preparations, avoid concomitant hepatotoxic/nephrotoxic drugs when Possible, and implement periodic liver and renal function monitoring (ALT/AST, bilirubin, creatinine/eGFR), especially when the formulas contain Tripterygium-derived components or anthraquinone-rich herbs (Hu et al., 2022; Xi et al., 2017; Dong et al., 2016; Sougiannis et al., 2021).
Standardization challenges and strategies for modern integration
5.3
TCM emphasizes “syndrome differentiation–based treatment,” which may offer advantages for personalized care but also poses substantial challenges for modern drug evaluation in terms of the standardization and reproducibility of results. These challenges include variability between botanical preparations (e.g., decoctions, granules, and pills), inconsistent sources of raw botanical drugs, diverse processing methods, large batch-to-batch fluctuations in key plant metabolites, and a lack of systematic comparisons of bioavailability and pharmacokinetic (PK) profiles across preparations. To promote the modernization of TCM evaluation systems, four areas should be prioritized: (i) building a “formula–plant metabolite–target–phenotype” integrative model and establishing mechanistic fingerprinting to improve interpretability and consistency; (ii) applying multi-omics and high-throughput platforms (e.g.,transcriptomics, metabolomics, proteomics) to quantify exposure-linked molecular response signatures and activity features of botanical preparations; (iii) developing harmonized RCT design standards and enabling cross-center verification through national-level clinical research platforms; and (iv) advancing GMP-aligned manufacturing and supply chain controls, including third-party quality control and traceability systems, to achieve controlled consistency in formula quality, with an explicit distinction between analytical marker metabolites (for QC) and bioactive metabolites (as candidate effectors).
Integrating cutting-edge technologies into TCM research for T2DM: from mechanistic discovery to predictive modeling
6
With rapid advances in systems biology, artificial intelligence (AI), spatial multi-omics, and graph neural networks (GNNs), research on TCM-related botanical drugs and multi-botanical preparations is increasingly shifting from an experience-driven paradigm to an integrated “mechanistic discovery–model prediction” workflow. In complex metabolic diseases such as T2DM, these technologies can enhance the systems-level interpretation of how botanical preparations and their plant metabolites relate to disease-relevant modules, while also enabling data-driven optimization of formula composition, prioritization of candidate targets, and hypothesis generation for personalized strategies. Importantly, such modeling frameworks should explicitly distinguish analytical marker metabolites (used for standardization/quality control) from bioactive metabolites (candidate effectors) to improve reproducibility and translational interpretability. The following sections summarize how these emerging approaches can support mechanistic discoveries and model-driven predictions in TCM-related research.
AI for mechanism elucidation and compound-formula prioritization in TCM
6.1
AI, particularly natural language processing (NLP) and graph-based learning algorithms, is gradually becoming a core tool for knowledge mining and mechanism modeling in TCM research (Duan et al., 2024; Long et al., 2025). NLP enables the automatic extraction of entities such as “botanical drug–syndrome–target–signaling pathway–disease” and their interrelationships from classical TCM literature, structured databases, and modern clinical research. This facilitates the construction of TCM knowledge graphs (KGs) to achieve cross-hierarchical mechanism inference and multi-botanical preparation intervention pathway prediction (Weng et al., 2022; Zhuang et al., 2025). Graph neural networks (GNNs), built on KGs, can model complex heterogeneous relationships among “formula-based botanical preparations–plant metabolites–targets–pathways–phenotypes,” integrating topological structures and attribute features to identify key plant metabolites and generate hypotheses on synergistic mechanisms. For example, in studies of Gegen Qinlian Decoction (Gegen-Qinlian Decoction; GQD; a classical multi-herb decoction; complete composition and processing/standardization/QC as reported; NR if not reported; see Table 2 and Supplementary Table S1) in T2DM, GNN-based analyses have been used to prioritize key signaling pathways, such as PI3K/Akt, NF-κB, and AMPK, and to map putative high-contribution plant metabolites and pathway-level action networks (Xu et al., 2021). Further integration of classical machine-learning models, such as Random Forest (RF) and XGBoost, can enable the efficient screening of candidate bioactive metabolites and target prediction scoring, thereby proposing an efficient methodology for the accelerated development and more precise evaluation of candidate multi-botanical preparations (with experimental and outcome-linked validation required for translational inference).
Multi-omics integration for mechanism-compound formulation-phenotype closed-loop modeling in TCM
6.2
The systemic metabolic dysregulation characteristic of T2DM, combined with the multi-target nature of multi-botanical preparation interventions, underscores the limitations of single-omics approaches in holistically elucidating their mechanisms of action. Integrated multi-omics strategies, including metabolomics, transcriptomics (particularly single-cell RNA sequencing (scRNA-seq)), proteomics, and spatial transcriptomics, have emerged as pivotal methodologies for deciphering the pharmacological mechanisms underlying TCM-related botanical preparations. Metabolomics enables the comprehensive profiling of TCM-related botanical preparation–associated remodeling of glucose, lipid, and bile acid metabolic networks (Shao et al., 2022). Transcriptomics reveals pathway-specific alterations and cell subtype-specific responses (Wang et al., 2020), whereas spatial transcriptomics further delineates the spatial localization of formula-level actions at the tissue microenvironment level (Qian et al., 2024). For instance, a multi-omics study on Huanglian Jiedu Decoction (Huanglian-Jiedu Decoction; HLJDT) suggests that its intervention mechanism involves the “gut–liver–brain–adipose” multi-axis network, with putative engagement of key nodes such as AMPK, FXR, and NLRP3, and supports a multi-level workflow that encompasses mechanism identification, tissue localization, and phenotypic validation (Dai et al., 2024). These strategies can support systematic pharmacodynamic modeling and outcome-linked mechanism validation for multi-botanical preparations, provided that intervention definition/standardization and appropriate controls are transparently reported, thereby advancing the interpretability of TCM-related research.
Advancing TCM mechanistic research: novel biological models for innovation and validation
6.3
To enhance the biological explanatory power of mechanistic modeling, an increasing number of studies on TCM-related botanical preparations have incorporated advanced functional validation platforms such as organoids, organ-on-a-chip (OoC) systems, and spatial multi-omics. These models more faithfully recapitulate the structural and functional complexity of in vivo tissue microenvironments, enabling dynamic and tissue-specific analyses of multi-botanical preparations (Zhao et al., 2022; Low et al., 2021; Larsson et al., 2021). For instance, evidence suggests that ginsenoside Rg1, a representative plant metabolite frequently investigated in the TCM research context (primarily associated with Panax ginseng C. A. Mey. [Araliaceae], as reported), may improve central energy homeostasis and ameliorate cognitive impairment in T2DM models by activating POMC neurons and the PI3K/Akt–BDNF pathway, a mechanism amenable to precise spatial and functional validation using hypothalamic organoid platforms (Feng et al., 2022; Jiang et al., 2023). This integrated “mechanism–botanical preparation–tissue” experimental framework may help strengthen standardization, reproducibility, and spatially resolved mechanistic validation in TCM-related research.
Deciphering multi-target mechanisms of TCM with GNNs
6.4
GNNs are emerging as pivotal technical tools in system pharmacology research on TCM, owing to their capacity to model complex, heterogeneous relational structures and their growing adoption in molecular/drug-discovery graph learning (Abate et al., 2023). By constructing multi-layered graphs encompassing “botanical preparation–plant metabolite–target–pathway–organ–disease” relationships, GNNs can be used to support multiple core functions: (1) intervention path inference, predicting potential multi-pathway regulatory trajectories of multi-botanical preparations within comorbidity networks; (2) node importance ranking, identifying key plant metabolites or targets with central regulatory roles; and (3) synergistic target mapping, identifying shared targets across pathways to elucidate convergent mechanisms and network-level integration. For instance, a study utilized a GNN-based pharmacology graph model to predict that Yuquan Pill (a formula-based botanical preparation; complete composition, dosage form, and processing/standardization/QC as reported; NR if not reported; see Table 2 and Supplementary Table S1) may synergistically improve cardiac and renal functions via the AMPK–ACC–NRF2 signaling axis, suggesting its potential mechanism in the intervention of multiple organ complications in T2DM (Jiang et al., 2023). Looking ahead, coupling graph learning with spatially resolved multi-omics can improve biological interpretability by anchoring predictions to tissue microenvironments and cell-type-specific contexts (Marx, 2021). In summary, emerging technologies such as AI, multi-omics, spatial biology, and graph learning are profoundly reshaping the paradigm of TCM research, providing hypothesis-generating and decision-support capabilities for the systematic analysis and mechanism modeling of TCM-related botanical preparations (with translational inference requiring standardized interventions, appropriate controls, and outcome-linked validation).
Conclusion and future perspectives
7
Type 2 diabetes mellitus (T2DM) is a complex systemic metabolic syndrome characterized by multi-system dysregulation involving interconnected pathological mechanisms, such as insulin resistance, chronic inflammation, oxidative stress, and neuro-immune dysregulation. It is frequently accompanied by multi-organ complications involving the heart, kidneys, brain, and eyes. TCM-related botanical drugs and preparations are commonly delivered as multi-constituent, formula-based interventions that can engage multiple biological targets and pathways in the body. In this review, we use this feature primarily as a systems-level framework to organize evidence across shared pathogenic modules in T2DM rather than implying that “multi-target” pharmacology is unique to TCM formulations. This review systematically synthesizes the key mechanisms through which TCM-related interventions may ameliorate T2DM, including modulation of signaling pathways, such as PI3K/Akt and AMPK, inflammatory outputs (NF-κB/NLRP3), remodeling of the gut–liver–brain–immune network, and pathways relevant to diabetic complications. Where available, we prioritized evidence in which pathway modulation was accompanied by metabolic or complication-relevant endpoints (e.g., HbA1c, insulin sensitivity indices, and tissue injury markers) and interpreted pathway-only findings with caution. Given this substantial epidemiological burden, the real-world impact of TCM on diabetes management should be interpreted through an evidence-based lens. Beyond mechanistic studies, future work should prioritize well-designed randomized trials, pragmatic studies, and real-world evaluations with transparent reporting of botanical preparation standardization, dosage forms, concomitant therapies, safety outcomes, and clinically meaningful endpoints (e.g., HbA1c, complication progression, and patient-reported outcomes). In line with GA-online best-practice recommendations, intervention identity is treated as a prerequisite for interpretation: for each botanical preparation discussed, composition and processing/standardization (including quality control/chemical characterization) are recorded as reported, and items not provided in the primary study are explicitly marked as NR (not reported), rather than being inferred. All botanical source species mentioned in this review are taxonomically validated and reported with full scientific names (including authorities) and families, with details provided in Table 2 and in Supplementary Table S1.
Assay interference and PAINS considerations are particularly important when interpreting the effects of plant metabolites. Some molecules may appear active across multiple biochemical or cell-based assays because of non-target-specific mechanisms (e.g., redox cycling, fluorescence/absorbance interference, or colloidal aggregation) rather than genuine target engagement. To strengthen translational confidence, future studies should incorporate orthogonal assay formats and counter-screens (e.g., detergent sensitivity for aggregation, alternative readouts, and appropriate negative controls) before concluding the target-specific pharmacology of plant metabolites. Taken together, these assay-level considerations highlight the broader limitations of the current evidence base and motivate clear research priorities for future translation. In line with the individualized practice emphasized by TCM, an emerging direction is to operationalize constitution typing (e.g., Wang Qi’s nine-constitution framework) as a stratification layer for the integrated risk prediction and management of T2DM. Standardized questionnaires, such as the Constitution in Chinese Medicine Questionnaire (CCMQ), enable scalable phenotyping, and multiple studies have linked unbalanced constitutions (e.g., phlegm-dampness, damp-heat, and qi deficiency) to inflammatory/adipokine profiles and a higher risk of diabetes or adverse outcomes. Therefore, future “TCM + systems” models could incorporate constitution types as interpretable nodes alongside clinical variables, multi-omics signatures, and medication exposure to support constitution-informed prevention, complication surveillance, and personalized formula selection (Wong et al., 2013; You et al., 2017; Bai YL et al., 2021; Lee et al., 2024). Limitations and research requirements First, the clinical evidence is heterogeneous and frequently limited by suboptimal trial design and reporting (e.g., incomplete randomization/blinding details, short follow-up, and variable endpoints), underscoring the need to follow established guidelines for herbal interventions and systematic reviews (Gagnier et al., 2006; Page et al., 2021). Second, many mechanistic findings rely on simplified in vitro/in silico models or non-physiological exposures, with insufficient dose–response characterization and unclear minimal active concentrations/doses, which constrain model-to-human extrapolations. Third, reproducibility is weakened by inadequate intervention standardization and extract characterization (e.g., missing marker quantification, batch consistency, and chemical profiling). Future studies should align with the best practice recommendations for phytopharmacological reporting and characterization (Heinrich et al., 2022). Fourth, rigorous controls and orthogonal validation are inconsistently applied, and phytochemical “target” claims should be interpreted cautiously, given assay interference/PAINS liabilities, and other non-specific effects (Baell and Holloway, 2010; Dahlin et al., 2021). Finally, to close the translation gap, more pragmatic trials and high-quality real-world evaluations with transparent standardization and clinically meaningful endpoints are needed, complemented by target trial emulation principles when RCTs are not feasible (Ford and Norrie, 2016; Hernán and Robins, 2016).
Furthermore, emerging technologies, such as GNNs, multi-omics integration, spatial transcriptomics, and organoid modeling, are progressively enabling the construction of a five-dimensional interventional map linking “formula–plant metabolite–pathway–organ–disease.” This structured framework supports the transition of TCM from an experience-based system to a mechanism-driven research platform. Based on these limitations, we outline the following translational priorities and future research directions: Looking ahead, the systematic integration of TCM in T2DM therapy holds promise through advances in five key areas: ① closed-loop validation of “mechanism–plant metabolite–phenotype” links to establish causal evidence chains; ② spatially resolved target engagement and pathway verification enabled by spatial multi-omics, organoids, and organ-on-a-chip platforms; ③ GNN-enhanced systems-pharmacology modeling to improve the interpretability of multi-botanical preparation effects and to prioritize testable hypotheses; ④ development of dynamic safety databases and internationally aligned standardization/quality-control frameworks (including botanical authentication, marker-based QC, batch consistency, and dosage-form transparency) to support reproducibility and clinical reliability; and ⑤ AI-assisted knowledge mining to guide indication expansion and rational, personalized combination strategies, with explicit attention to drug–botanical interaction risk and real-world implementability. In summary, TCM research is evolving toward a modern pharmacology platform characterized by mechanism-oriented, evidence-graded analyses, reproducible intervention definitions, and clinically meaningful translational endpoints. Its potential role in managing complex chronic diseases, such as T2DM, should be judged based on outcome-linked evidence and reproducible reporting standards, with translation strengthened by rigorous trials, pragmatic designs, and real-world evaluations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abate C. Decherchi S. Cavalli A. (2023). Graph neural networks for conditional de novo drug design. WIR Es Comput. Mol. Sci. 13, e 1651. 10.1002/wcms.1651 · doi ↗
- 2American Diabetes Association Professional Practice Committee (2025 a). Cardiovascular disease and risk management: standards of care in Diabetes—2025. Diabetes Care 48 (Suppl. 1), S 207–S 238. 10.2337/dc 25-S 010 39651970 PMC 11635050 · doi ↗ · pubmed ↗
- 3American Diabetes Association Professional Practice Committee (2025 b). Chronic kidney disease and risk management: standards of care in Diabetes—2025. Diabetes Care 48 (Suppl. 1), S 239–S 251. 10.2337/dc 25-S 011 39651975 PMC 11635029 · doi ↗ · pubmed ↗
- 4An Y. Xu B.-T. Wan S.-R. Ma X.-M. Long Y. Xu Y. (2023). The role of oxidative stress in diabetes mellitus-induced vascular endothelial dysfunction. Cardiovasc Diabetol. 22, 237. 10.1186/s 12933-023-01965-7 37660030 PMC 10475205 · doi ↗ · pubmed ↗
- 5Badran H. M. Helmy J. A. Ahmed N. F. Yacoub M. (2024). Impact of diabetes mellitus on left ventricular mechanics and long-term outcome in patients with hypertrophic cardiomyopathy. Echocardiography 41 (12), e 70048. 10.1111/echo.70048 39661017 · doi ↗ · pubmed ↗
- 6Baell J. B. Holloway G. A. (2010). New substructure filters for removal of pan assay interference compounds (PAINS) from screening libraries and for their exclusion in bioassays. J. Med. Chem. 53, 2719–2740. 10.1021/jm 901137 j 20131845 · doi ↗ · pubmed ↗
- 7Bai F. Luo H. Wang L. Zhu L. Guan Y. Zheng Y. (2021). A meta-analysis of the association between diabetes mellitus and traditional Chinese medicine constitution. Evid. Based Complement. Altern. Med. 2021, 6390530. 10.1155/2021/6390530 34394389 PMC 8357480 · doi ↗ · pubmed ↗
- 8Bai Y. Mu Q. Bao X. Zuo J. Fang X. Hua J. (2021). Targeting NLRP 3 inflammasome in the treatment of diabetes and diabetic complications: role of natural compounds from herbal medicine. Aging Dis. 12 (7), 1587–1604. 10.14336/AD.2021.0318 34631209 PMC 8460305 · doi ↗ · pubmed ↗