Evaluating the value of lactic dehydrogenase in anti-MDA5-positive Dermatomyositis associated with interstitial lung disease
Wenhan Huang, Feifeng Ren, Kechen Qian, Yanqiu Jiang, Yichen Zhang, Lin Tang

TL;DR
This study shows that high lactic dehydrogenase levels are linked to worse outcomes and disease severity in a specific type of muscle disease with lung involvement.
Contribution
The study identifies lactic dehydrogenase as a potential biomarker for disease severity and prognosis in anti-MDA5-positive dermatomyositis with ILD.
Findings
LDH levels are significantly higher in anti-MDA5-positive DM patients with ILD compared to controls.
Elevated LDH levels correlate with disease severity and are associated with poor prognosis in these patients.
LDH levels change in response to ILD progression or improvement, suggesting its utility as a monitoring tool.
Abstract
This retrospective cohort study aimed to investigate the relationship between lactic dehydrogenase (LDH) and anti-melanoma differentiation-associated gene 5 antibodies-positive dermatomyositis (anti-MDA5-positive DM) associated with interstitial lung disease (ILD). A total of 168 anti-MDA5-positive DM patients with ILD underwent comprehensive evaluation, including LDH, anti-Ro-52 antibodies, serum ferritin determination, and lung high-resolution computed tomography (CT). The levels of LDH were significantly elevated in anti-MDA5-positive DM patients compared with the control group (p < 0.01). Anti-Ro-52-positive patients exhibited significantly higher LDH levels than anti-Ro-52-negative patients (p < 0.01). Patients with elevated serum ferritin exhibited markedly increased LDH levels compared with those with lower serum ferritin (p < 0.01). After treatment, LDH levels significantly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
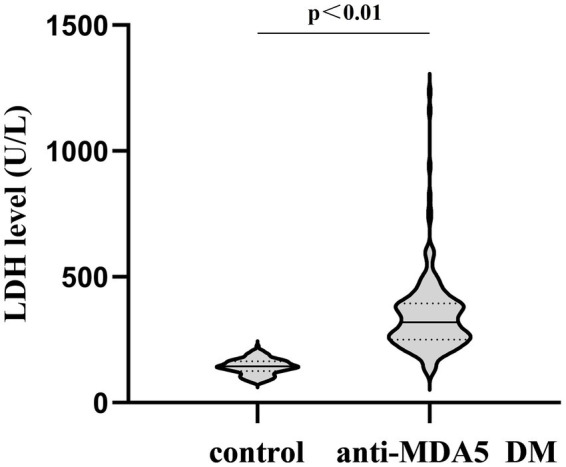 Figure 1
Figure 1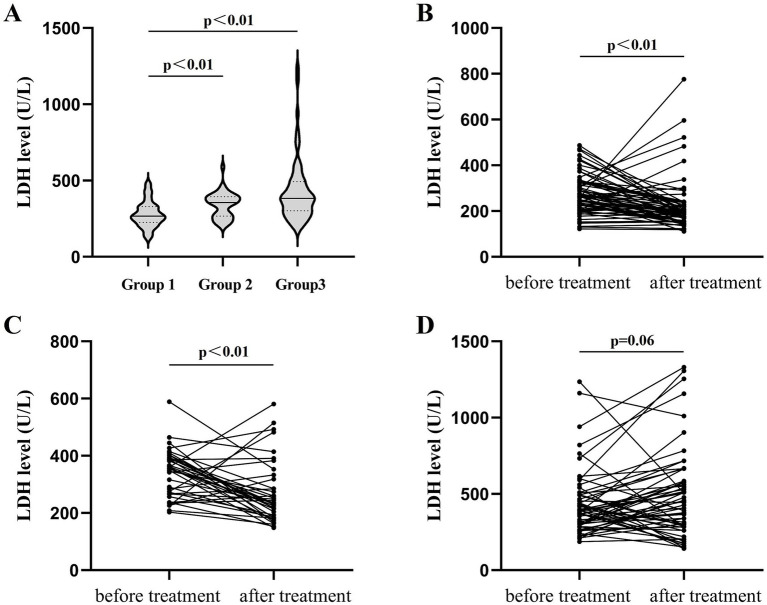 Figure 2
Figure 2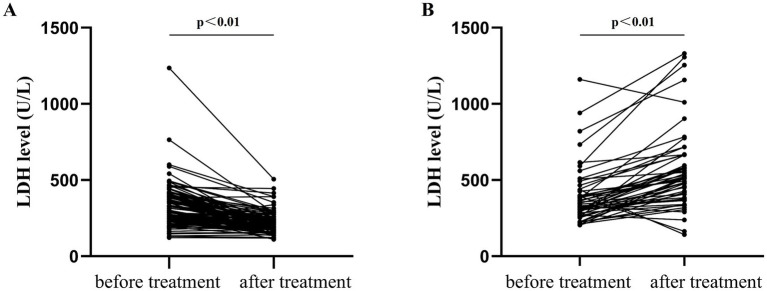 Figure 3
Figure 3| Control cohort ( | Anti-MDA5-positive DM cohort ( | |
|---|---|---|
| Male | 52 | 57 |
| Female | 108 | 111 |
| Age | 51.3 ± 9.6 | 51.7 ± 13.0 |
| Steroid pulse | – | 16 (9.5%) |
| Prednisolone | – | 168 (100%) |
| IVIG | – | 62 (36.9%) |
| Cyclophosphamide | – | 101 (60.1%) |
| Mycophenolate mofetil | – | 11 (6.5%) |
| Tacrolimus | – | 83 (49.4%) |
| Cyclosporine | – | 8 (4.8%) |
| JAK inhibitor | – | 25 (14.9%) |
| Methotrexate | – | 13 (7.7%) |
| Anti-Ro-52 antibodies positive cohort ( | Anti-Ro-52 antibodies negative cohort ( | ||
|---|---|---|---|
| Before treatment (U/L) | 336 [(267, 403)] | 299.6 ± 107.7 | <0.01 |
| After treatment (U/L) | 279 [(193, 482)] | 203 [(156, 776)] | <0.01 |
| 0.45 | <0.01 |
| Survival patients of anti-MDA5-positive DM ( | Deceased patients of anti-MDA5-positive DM ( | ||
|---|---|---|---|
| Before treatment (U/L) | 299.5 [(241.5, 392.3)] | 345.0 [(298.8, 472.0)] | 0.02 |
| After treatment (U/L) | 203.5 [(174.8, 259.3)] | 534.5 [(444.3, 666.5)] | <0.01 |
| <0.01 | <0.01 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Myopathies and Dermatomyositis · Systemic Sclerosis and Related Diseases · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
1
Sato et al. (1, 2) initially characterized anti-melanoma differentiation-associated gene 5 antibodies-positive dermatomyositis (anti-MDA5-positive DM); this disease has garnered considerable clinical attention owing to its propensity for rapidly progressive interstitial lung disease (RP-ILD) development, culminating in elevated mortality rates (3, 4). Undoubtedly, pulmonary assessment in anti-MDA5-positive DM patients is the core of the clinical work. Contemporary evaluation modalities predominantly encompass chest CT and pulmonary function assessments. Furthermore, patients showing elevated serum Krebs Von den Lungen-6 levels exhibit heightened predisposition toward RP-ILD development (5). Nevertheless, an urgent clinical imperative persists for a straightforward, efficacious indicator facilitating ILD severity assessment in anti-MDA5-positive DM patients.
Lactic dehydrogenase represents a pivotal redox enzyme catalyzing pyruvate-to-lactate conversion. LDH is abundantly distributed in tissues of the heart, the liver, the skeletal muscle, and the lungs. When cells were damaged or ruptured, enhanced permeability facilitated LDH release into systemic circulation, thereby elevating serum concentrations. Consequently, LDH serves as a significant tissue injury biomarker. Currently, LDH detection finds widespread application in myocardial infarction (6), liver injury (7), and tumors (8). Recent investigations have validated LDH’s crucial role in pulmonary injury evaluation, with LDH levels closely correlating with acute respiratory distress syndrome prognosis (9). Nevertheless, LDH research regarding anti-MDA5-positive DM-associated interstitial lung disease remains limited. This study retrospectively analyzed 168 anti-MDA5-positive DM patients from the Department of Rheumatology and Immunology at the Second Affiliated Hospital of Chongqing Medical University and explored the relationship between LDH and ILD to provide assistance for clinical guidance.
Methods
2
From September 2015 to July 2025, 168 anti-MDA5-positive DM patients with ILD were hospitalized at the Second Affiliated Hospital of Chongqing Medical University. Patients with comorbidities such as cardiac disease, skeletal muscle and myocardial involvement, and malignancies were excluded from the study. Pulmonary infections were excluded using sputum culture, procalcitonin test, serum galactomannan detection, (1,3)-β-D-glucan detection assay, Epstein–Barr virus DNA test, and human cytomegalovirus DNA test. The control group comprised individuals who underwent health examinations at the same institution. In accordance with the Helsinki Declaration, surviving patients and relatives of deceased patients provided informed consent for participation and data publication. The Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University approved this study.
LDH levels were quantified using the lactic acid substrate methodology (reference range: 120–250 U/L; Fosun Diagnostics, Shanghai, China). Anti-MDA5 and anti-Ro-52 antibodies were tested using OMRMUN assay kits (EUROIMMUN, Beijing, China). Serum ferritin levels were measured using the chemiluminescence method using an Access Ferritin kit (reference range: 11–306 ng/mL; Beckman Coulter, CA, USA).
Grouping: (1) LDH levels were evaluated by comparing 168 patients with anti-MDA5-positive DM to the control group before treatment. (2) High-resolution pulmonary computed tomography was performed in 168 patients with anti-MDA5-positive DM before and after treatment to assess the relationship between LDH and ILD. Based on radiological findings, patients were dichotomized: the improvement group (n = 116) showed reduction or no significant changes in pulmonary lesions after treatment and the worsening group (n = 52) exhibited newly emerged infiltrative shadows in the lungs on post-treatment imaging, defined as disease progression, excluding factors such as infection, pulmonary embolism, or heart failure (10). All CT evaluations were conducted by an experienced radiologist and respiratory specialist. (3) The 168 anti-MDA5-positive DM patients were stratified according to anti-Ro-52 antibody status, ferritin concentrations, and prognostic outcomes to examine LDH variations.
For stable patients, LDH levels and lung CT were reevaluated after receiving treatment for 3 months. For patients with exacerbations, the above examinations were rechecked after receiving treatment for 2 weeks or 1 month.
Statistical analysis
2.1
All analyses used SPSS 19.0 (IBM, Armonk, NY, USA). Normally distributed data were presented as mean ± standard deviation, while non-normal distribution data were expressed as median and interquartile range. The Mann–Whitney test was used to compare the two groups. The Wilcoxon test was used to compare the difference before and after treatment. Multiple comparisons were assessed using the Kruskal–Wallis test and Dunn’s post-hoc test. Values of P of < 0.05 were considered significant.
Results
3
Baseline information
3.1
The normal group encompassed 160 individuals (52 male participants, 108 female participants; male: female ratio: 1:2.07; mean age: 51.3 ± 9.6 years). The total number of anti-MDA5-positive DM patients was 168, including 57 male and 111 female patients (male: female: ratio 1:1.95; mean age: 51.7 ± 13.0 years) (Table 1). The LDH level was 143.5 ± 30.2 U/L in the control group and 319 U/L (250.2, 394) in patients with anti-MDA5-positive DM before treatment, which was significantly elevated versus controls (p < 0.01, Figure 1).
Comparison of LDH levels between the control group and patients with anti-MDA5-positive DM before treatment, p < 0.01.
The relationship between LDH and anti-Ro52 antibody
3.2
A total of 168 anti-MDA5-positive DM patients were dichotomized based on anti-Ro-52 antibody status. The results revealed: (1) among the 111 patients with anti-Ro-52 antibody, the LDH level before treatment was 336 U/L (267, 403). In contrast, among the 57 patients without anti-Ro-52 antibody, the LDH level before treatment was 299.6 ± 107.7 U/L. A statistically significant difference was observed between the two groups, p < 0.01. (2) The LDH level of patients with positive anti-Ro-52 antibodies was 279 U/L (193, 482) after treatment, which was not significantly different from that before treatment (p = 0.45). (3) The LDH level of patients without anti-Ro-52 antibodies was 203 U/L (156, 776) after treatment, which was significantly reduced compared to that before treatment (p < 0.01, Table 2).
Relationship between LDH and serum ferritin
3.3
A total of 168 anti-MDA5-positive DM patients were categorized into three groups based on their ferritin levels. Group 1: serum ferritin<500 ng/mL (n = 69); Group 2: 500 ng/mL ≤ serum ferritin < 1,000 ng/mL (n = 39); and Group 3: 1,000 ng/mL ≤ serum ferritin≤1,500 ng/mL (n = 60). The LDH level of patients in Group 1 was 278.2 ± 84.6 U/L before treatment, significantly lower than that of patients in Groups 2 and 3 (Group 2: 340.4 ± 82.9 U/L; Group 3: 382.5 [301.3, 492.5 U/L]); respectively (p < 0.01; Figure 2A). After treatment, patients in Group 1 exhibited an LDH level of 193 U/L (158, 232), which was significantly lower than that before treatment (p < 0.01; Figure 2B). The LDH level of patients in Group 2 was 234 U/L (186, 318) after treatment, markedly diminished than that before treatment (p < 0.01; Figure 2C). The LDH level of patients in Group 3 after treatment was 435.5 U/L (285, 577), and the difference was not statistically significant than that before treatment (p = 0.06; Figure 2D).
Relationship between LDH and serum ferritin. (A) Levels of LDH before treatment grouped by serum ferritin. (B) Changes in LDH levels before and after treatment for patients in Group 1 (serum ferritin < 500 ng/mL, n = 69). (C) Changes in LDH levels before and after treatment for patients in Group 2 (500 g/mL ≤ serum ferritin < 1,000 ng/mL, n = 39). (D) Changes in LDH levels before and after treatment for patients in Group 3 (1,000 g/mL ≤ serum ferritin ≤ 1,500 ng/mL, n = 60).
Relationship between LDH and ILD
3.4
To elucidate LDH-ILD correlations before and after treatment, we divided 168 anti-MDA5-positive DM patients into two groups: the improvement group, encompassing patients with improved or stabilized interstitial lung disease after treatment (n = 115), and the worsening group, comprising patients with deteriorated interstitial lung disease after treatment (n = 53). In the improvement group, the LDH level of patients significantly decreased after treatment (before treatment: 297 U/L [242, 392] vs. after treatment: 201 U/L [174, 244], p < 0.01, Figure 3A). Conversely, the worsening group exhibited a significant increase in LDH relative to the baseline when interstitial lung disease deteriorated (before treatment: 342 U/L [279.5, 431.5] vs. after treatment: 512 U/L [395, 664], p < 0.01, Figure 3B).
LDH fluctuations in 168 anti-MDA5-positive DM patients before and after treatment. (A) Improvement group: ILD was improved or stabilized after treatment (n = 115) and (B) Worsening group: ILD was aggravated after treatment (n = 53), p < 0.01.
Relationship between LDH and prognosis
3.5
A total of 168 anti-MDA5-positive DM patients were categorized into a survival group (n = 126) and a deceased group (n = 42) based on their prognosis. (1) The LDH level of patients in the survival group was 299.5 U/L (241.5, 392.3) before treatment, which was significantly lower than that in the deceased group (345.0 U/L [298.8, 472.0], p = 0.02). (2) After treatment, the LDH level in the survival group decreased to 203.5 U/L (174.8, 259.3), which was significantly lower than that before treatment (p < 0.01). (3) In the deceased group, the LDH level increased to 534.5 U/L (444.3, 666.5) after treatment, which was significantly higher than that before treatment (p < 0.01) (Table 3).
Discussion
4
Anti-MDA5-positive DM patients developing RP-ILD frequently exhibit poor prognosis and elevated mortality rates. However, lung lesion assessments in anti-MDA5-positive DM remain relatively scarce with inherent constraints, such as radiation exposure from repeated chest CT scans over a short period of time, the inability of critically ill patients to adequately complete pulmonary function assessments, and the limited practicality of KL-6 testing owing to economic constraints. Consequently, identifying efficacious biomarkers for evaluating ILD severity in anti-MDA5-positive DM patients assumes paramount significance.
Our findings revealed that the LDH levels in anti-MDA5-positive DM patients with ILD were markedly elevated compared with those in the control group before treatment, indicating that LDH is an important indicator that should not be ignored. Subsequently, we explored LDH correlations with anti-MDA5-positive DM comprehensively.
First, extensive research has validated the pivotal role of anti-Ro-52 antibodies in inflammatory myopathies. Patients with positive anti-Ro-52 antibodies were more likely to develop rapidly progressive interstitial lung disease (11), subcutaneous and mediastinal emphysema (12), and pharyngeal lesions (13). Our study revealed that the LDH level before treatment was significantly more elevated in patients with anti-Ro-52 antibodies than in those without anti-Ro-52 antibodies, confirming LDH-anti-Ro-52 antibody associations in anti-MDA5-positive DM patients. Furthermore, no significant differences were found in the LDH level of patients positive for anti-Ro-52 antibodies before and after treatment, whereas the level of LDH in patients negative for anti-Ro-52 antibodies decreased significantly after treatment. This is potentially attributable to more severe interstitial lung disease in anti-Ro-52-positive patients.
Second, serum ferritin is also an important evaluation indicator for anti-MDA5-positive DM. Takahisa et al. (14) suggested that anti-MDA5-positive DM represents macrophage activation occurring in the lungs, distinguished by pronounced ferritin elevation. By stratifying ferritin levels, we determined that LDH levels in anti-MDA5-positive DM patients exhibited concordance with ferritin levels, exhibiting a direct correlation between inflammatory magnitude and LDH elevation. Additionally, we found that, under different inflammatory states, the difference in LDH levels of anti-MDA5-positive DM patients was also observed before and after treatment. Patients with serum ferritin <500 ng/mL and 500–1,000 ng/mL showed significant post-treatment LDH attenuation versus baseline, signifying a better treatment response in mild-to-moderate inflammatory states. Conversely, when serum ferritin was between 1,000 and 1,500 ng/mL, no significant difference was found in LDH levels before and after treatment, indicating that glucocorticoids and immunosuppressants have no improvement effect on LDH in severe inflammatory conditions. This finding bears profound clinical implications, underscoring the imperative for rheumatologists to judiciously modulate inflammatory burden in anti-MDA5-positive DM patients, thereby attenuating disease activity and improving the prognosis.
Given anti-MDA5-positive DM’s predominant lung manifestations, we prioritized LDH-ILD correlational analysis. Our data indicated that LDH levels diminish relative to the baseline when ILD lesions are improved or stabilized post-treatment. Conversely, progressive ILD deterioration and intensified pulmonary injury precipitate substantial tissue LDH efflux into systemic circulation, markedly elevating serum concentrations versus pretreatment values. These observations establish a positive correlation between LDH levels and ILD severity in anti-MDA5-positive DM patients. On the one hand, extracellular LDH functions as a damage-associated molecular pattern, promoting the release of inflammatory factors and exacerbating pulmonary inflammation. On the other hand, LDH’s fundamental physiological role is to catalyze pyruvic acid into lactic acid. A high concentration of lactic acid in tissues can activate TGF-β, inducing myofibroblast differentiation and thus accelerating the pulmonary fibrosis process (15). Our study confirmed that LDH was a simple yet effective biomarker to evaluate the changes in ILD in patients with anti-MDA5-positive DM.
Finally, we found that the LDH levels were substantially more elevated in the deceased group than in the survival group before treatment. After treatment, LDH levels in the deceased group escalated further while exhibiting marked amelioration in the survival group, indicating LDH’s prognostic significance in anti-MDA5-positive DM. Analogous findings (16, 17) in COVID-19 patients characterized by acute lung injury showed that non-survivors had significantly higher levels of LDH than survivors. As a result, LDH was regarded as an important indicator for evaluating patients’ respiratory function and predicting their prognosis. Combined with the above findings and our study, it was strongly confirmed that LDH plays a pivotal role in lung lesion assessment in anti-MDA5-positive DM patients.
It is worth noting that this is a retrospective study; therefore, inherent limitations should not be ignored. First, our study exclusively examined LDH’s relationship with anti-MDA5-positive DM, precluding characterization of other inflammatory myopathy types, such as antisynthetase syndrome. Second, mechanistic exploration remains superficial, requiring deeper investigation. Finally, single-center clinical data necessitate multicenter validation with expanded sample sizes.
In conclusion, this study elucidated LDH’s associations with serological markers, lung interstitial lesions, and prognosis in anti-MDA5-positive DM patients, furnishing clinically relevant insights and establishing groundwork for subsequent research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sato S Hirakata M Kuwana M Suwa A Inada S Mimori T . Autoantibodies to a 140-kd polypeptide, CADM-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis Rheum. (2005) 52:1571–6. doi: 10.1002/art.21023, 15880816 · doi ↗ · pubmed ↗
- 2Sato S Hoshino K Satoh T Fujita T Kawakami Y Kuwana M. RNA helicase encoded by melanoma differentiation-associated gene 5 is a major autoantigen in patients with clinically amyopathic dermatomyositis: association with rapidly progressive interstitial lung disease. Arthritis Rheum. (2009) 60:2193–200. doi: 10.1002/art.24621, 19565506 · doi ↗ · pubmed ↗
- 3Yang Y Li Y Yuan W Zhang S He X Ji J. Risk factors for mortality in anti-MDA 5 antibody-positive dermatomyositis with interstitial lung disease: a systematic review and meta-analysis. Front Immunol. (2025) 16:1628748. doi: 10.3389/fimmu.2025.1628748, 40746563 PMC 12310698 · doi ↗ · pubmed ↗
- 4Li H Zou R Xin H He P Xi B Tian Y . Mortality risk prediction in patients with Antimelanoma differentiation-associated, gene 5 antibody-positive, Dermatomyositis-associated interstitial lung disease: algorithm development and validation. J Med Internet Res. (2025) 27:e 62836. doi: 10.2196/62836, 39908093 PMC 11840371 · doi ↗ · pubmed ↗
- 5Ye Y Fu Q Wang R Guo Q Bao C. Serum KL-6 level is a prognostic marker in patients with anti-MDA 5 antibody-positive dermatomyositis associated with interstitial lung disease. J Clin Lab Anal. (2019) 33:e 22978. doi: 10.1002/jcla.22978, 31301087 PMC 6805307 · doi ↗ · pubmed ↗
- 6Wroblewski F Ruegsegger P Ladue JS. Serum lactic dehydrogenase activity in acute transmural myocardial infarction. Science. (1956) 123:1122–3. doi: 10.1126/science.123.3208.1122, 13324162 · doi ↗ · pubmed ↗
- 7Cassidy WM Reynolds TB. Serum lactic dehydrogenase in the differential diagnosis of acute hepatocellular injury. J Clin Gastroenterol. (1994) 19:118–21. doi: 10.1097/00004836-199409000-00008, 7963356 · doi ↗ · pubmed ↗
- 8Gallo M Sapio L Spina A Naviglio D Calogero A Naviglio S. Lactic dehydrogenase and cancer: an overview. Front Biosci. (2015) 20:1234–49. doi: 10.2741/4368, 25961554 · doi ↗ · pubmed ↗