Clinicopathologic and molecular characterization of a series of sporadic trichoblastic neoplasms
Carina A. Dehner, Eric C. Honaker, Asma K. Abu-Salah, Brandon A. Umphress, Rohini Mopuri, Numrah Fadra, Bryan Piatkowski, Rachel Kowal, Simon J. Warren, Ahmed Al-Omari, Ruifeng Guo

TL;DR
This study characterizes sporadic trichoblastic neoplasms, identifying their clinicopathologic features, molecular profiles, and a rare case of malignant transformation.
Contribution
The study reports a novel FOXK1::GRHL1 fusion in a trichogerminoma and high tumor mutational burden without UV signature in sporadic trichoblastic tumors.
Findings
RNA sequencing revealed high tumor mutational burden and absence of UV-related mutational signature in sporadic trichoblastic tumors.
A FOXK1::GRHL1 fusion was identified in a case of trichogerminoma.
One case showed malignant transformation with increased atypia and mitotic activity.
Abstract
Trichoblastoma (TB) is a benign primitive follicular neoplasm that can occur in the setting of Brooke-Spiegler syndrome (CYLD mutations), in association with nevus sebaceous (mosaic HRAS mutations), or sporadically. We studied the histopathologic and molecular features of 16 sporadic trichoblastic neoplasms, including a case of trichogerminoma and a case of trichoblastic carcinoma arising within a TB. Sixteen tumors were identified in nine males and seven females (median age 64 years, range 33–97 years) involving the scalp (4), back (2), nasolabial fold (1), cheek (1), skin overlying the parotid gland (1), nasal ala (1), ear (1), upper chest (1), gluteal region (1), thigh (1), leg (1), and ankle (1) with a median size of 1.6 cm (range 1.2–7.0 cm). Histologically, 16 cases consisted of a dermal multinodular growth of basaloid epithelial cells surrounded by fibrotic stroma without…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
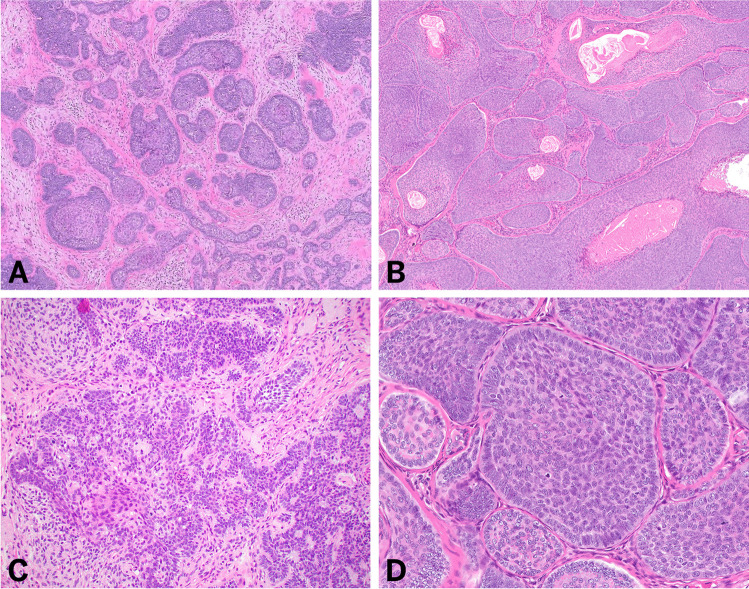 Figure 1
Figure 1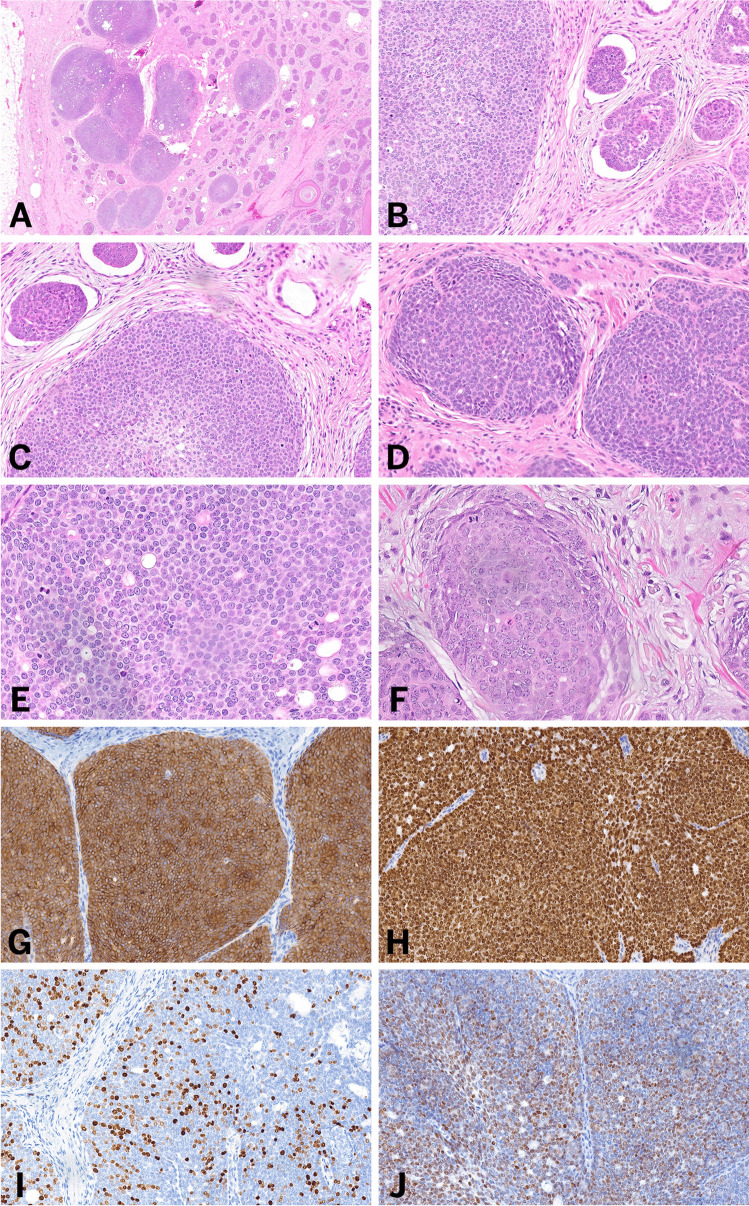 Figure 2
Figure 2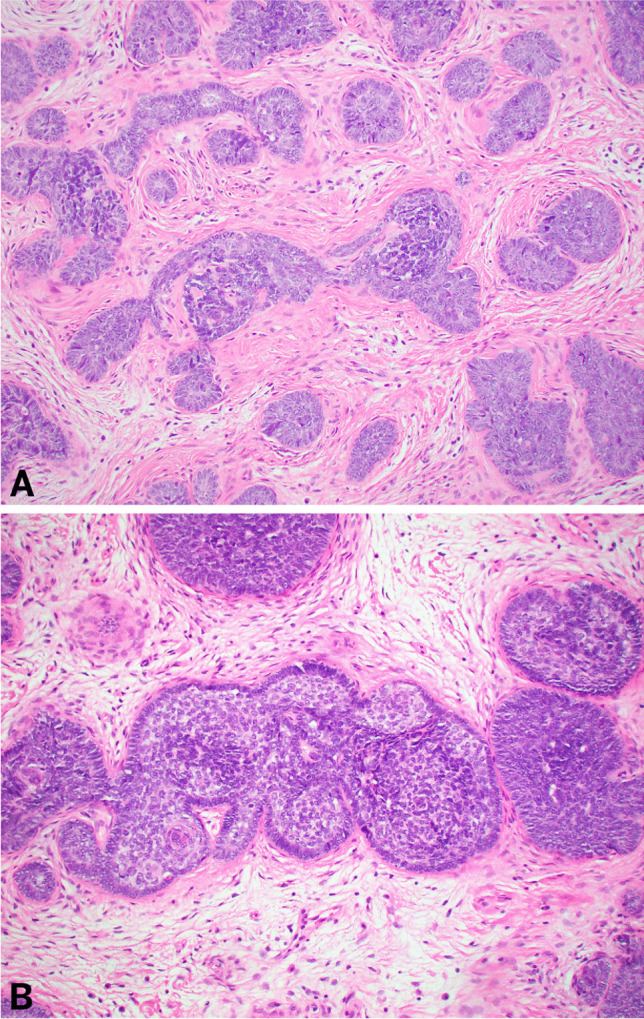 Figure 3
Figure 3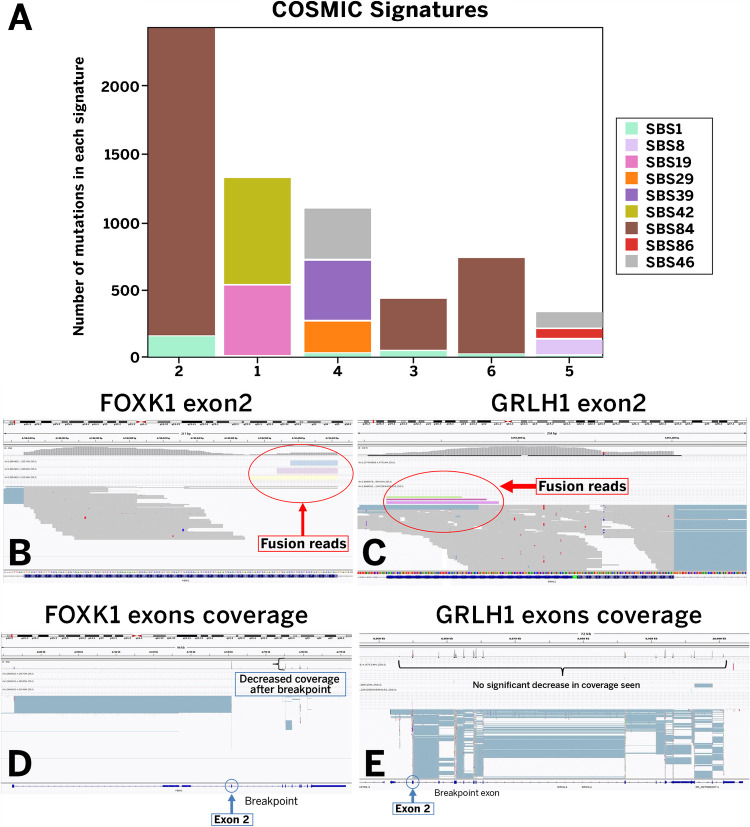 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Genetic and rare skin diseases. · Histiocytic Disorders and Treatments
Introduction
Trichoblastomas (TBs) are relatively rare cutaneous adnexal neoplasms arising from both follicular germinative cells and the surrounding fibrous root sheath [1]. Clinically, they are often slow-growing well-circumscribed nodules and show a predilection for the head and neck [2]. While these tumors can be part of the constellation of findings in Brooke-Spiegler syndrome or seen in association with nevus sebaceus, they also occur sporadically [3]. Morphologically, these tumors may resemble basal cell carcinoma due to their basaloid appearance and peripheral palisading [4–6]. However, they typically lack the mucinous stroma and artifactual clefting characteristic of basal cell carcinoma [4, 5]. Instead, they are often associated with a fibrotic stroma and may contain foci of papillary mesenchymal bodies [2, 4, 7]. Ultimately, histologic examination remains the diagnostic gold standard.
TBs are often benign; however, rare malignant transformation has been reported which may manifest de novo or as a trichoblastic carcinoma, trichoblastic sarcoma, or trichoblastic carcinosarcoma arising within a background TB [8, 9]. Benign TBs may show concerning features, such as deeply infiltrative growth or poor circumscription. These may be referred to as plaque-type TB or trichoblastic fibroma [10]. More specifically, these plaque-type variants have been shown to harbor somatic mutations in the Hedgehog pathway such as PTCH, although a prior study found that sporadic TBs lacked PTCH mutations [11, 12]. Additionally, a recent study on trichogerminoma showed evidence that these tumors were driven by GRHL1/2/3 gene rearrangements [13]. Despite these findings, the molecular landscape of TBs remains poorly understood.
To further elucidate the molecular underpinnings of trichoblastic neoplasms, we performed a comprehensive clinicopathologic analysis of 16 cases, including RNA sequencing on a subset of six tumors.
Materials and methods
This study was approved by the Institutional Review Board at the authors’ institutions. The cohort consisted of 16 cases of sporadic trichoblastic neoplasms which were retrieved from the internal archives and external consult services of the Indiana University School of Medicine and Mayo Clinic Department of Laboratory Medicine and Pathology by searching for “trichoblastoma/trichoblastic” with date restrictions from 2008 to 2023. Cases of tumors in the context of Brooke-Spiegler syndrome or those arising within a nevus sebaceous were excluded. All available hematoxylin and eosin (H&E) stained slides and immunohistochemical studies were reviewed by two dermatopathologists at the Indiana University School of Medicine with consensus on diagnosis and interpretation. Clinical information including age, gender, location, clinical follow-up, and molecular findings were obtained from the requisition and the electronic medical record system.
Histologic examination
Formalin-fixed paraffin-embedded (FFPE) tissue from each case was stained with hematoxylin and eosin (H&E). The diagnosis of trichoblastoma, trichogerminoma, and trichoblastic carcinoma was rendered following strict morphologic characteristics outlined in the literature. The identification of malignant transformation in trichoblastic carcinoma was based on increased atypia and mitotic activity within a background of “conventional” trichoblastoma.
Immunohistochemistry
Immunohistochemistry was performed on formalin-fixed paraffin-embedded tissue from one case (trichoblastic carcinoma) sectioned at 4 µm using the Dako Omnis instrument by Agilent Technologies Inc. (Santa Clara, CA) at the Indiana University Health Pathology Laboratory using antibodies against the following antigens: Ber-Ep4 (Dako, clone BerEp4, RTU), p63 (Dako, clone DAK-P63, RTU), CK20 (Dako, clone Ks20.8, RTU), Adipophilin (Dako, clone polyclonal, RTU), INSM1 (Dako, MRQ-70, RTU), SOX-10 (Dako, clone EP268, RTU), CEA (Dako, polyclonal, RTU), and EMA (Dako, clone E29, RTU) as well as Androgen receptor (Dako, clone SP107, RTU), c-MYB (Dako, clone Y69, RTU), S100 (Dako, polyclonal, RTU), Ki-67 (Dako, MIB-1, RTU), and p53 (Dako, clone DO-7, RTU).
Molecular analysis
RNA sequencing (RNAseq) was performed on six cases, including the case of trichogerminoma, at the Mayo Clinic Department of Laboratory Medicine and Pathology to assess for fusions, tumor mutational burden (TMB), and mutation signature.
MAPR-seq pipeline v3.1.4 was used for alignment against the human hg38 reference genome using the STAR aligner, and fusions were identified using the STAR-fusion caller. Fusions present in GTEX normal tissues and candidates with breakpoints less than 100 kb apart were excluded. Only potential fusion candidates determined to be in-frame with a cut-off of at least five total reads supporting the fusion (spanning reads and split reads) were included.
Putative somatic SNVs for TMB calculation were derived by applying five filters to RNAseq variants called using GATK HaplotypeCaller and scored with RV Boost. Five filters were applied: (1) SNVs (single nucleotide variation) supported by > 25 reads, RVBoost Qscore > 0.05, and genotype quality > 30 were retained; (2) SNVs with FFPE probability ≥ 0.5, as predicted by Excerno, were removed; (3) SNVs with allele frequencies between 0.45 and 0.55 or 0.95 and 1.0 were excluded; (4) variants present in dbSNP were removed; and (5) variants detected in GTEx skin samples were excluded. TMB was calculated using the following equation:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathrm{TMB}=\frac{\mathrm{Number\,of}\;\mathrm{somatic}\;\mathrm{mutations}\;(\mathrm{post}\;\mathrm{filter})}{\mathrm{Number}\;\mathrm{of}\;\mathrm{bases}\;\mathrm{covered}\geq50\mathrm x}\times1\times10^6$$\end{document}SNVs identified from the RNAseq data underwent analysis by the SigProfilerAssignment tool to identify and quantify the mutation signature. The tool assigns reference mutational signatures from Cosmic v3.3 to the extracted mutation signatures for a user-provided sample genome.
Results
Clinical features
Sixteen tumors were identified which occurred in nine males (56.3%) and seven females (43.7%) with a median age of 64 years (range 33–97 years). Of these, 14 were diagnosed as “conventional” trichoblastomas with a slight male predominance (nine cases, 64.3%). The tumors were located on the scalp (4), back (2), nasolabial fold (1), cheek (1), skin overlying the parotid gland (1), nasal ala (1), ear (1), upper chest (1), leg (1), and ankle (1). Additionally, a single case of trichogerminoma was identified in the right medial thigh (1) of a male, and a single case of trichoblastic carcinoma was identified in the right gluteal region (1) of a female. The median size was 1.6 cm (range 1.2–7.0 cm). Clinical follow-up data were available for 15 of 16 patients (94%), with a median duration of 65 months (range 2.5–106.5 months). At the time of last follow-up, 12 patients (80%) were disease-free, while three patients (20%) had died from unrelated causes, including metastatic breast cancer and lung cancer (Table 1). Table 1. Comprehensive clinicopathologic findings in 16 cases of trichoblastic tumors, including a single case of trichogerminoma () and a single case of trichoblastic carcinoma (**)Case noSpecimen typeAge (years)SexTumor locationMolecular findingsFollow-up duration (months)Disease status at follow-upCause of death (if applicable)1Excision62MRight medial thighFOXK1::GRHL1 fusion, high TMB47No evidence of disease—2Shave biopsy65FLeft nasolabial foldHigh TMB59No evidence of disease—3Shave biopsy81MLeft upper chestHigh TMB45No evidence of disease—4Excision95FRight legHigh TMB37Disease-freeMetastatic breast cancer5Excision33FLeft cheekHigh TMB78No evidence of disease—6Shave biopsy97MRight nasal alaHigh TMB84Disease-freeUnknown7Excision71MScalp—Lost to follow-up——8**Re-excision56FRight gluteal mass—2.5No evidence of disease—9Excision44MBack-thoracic region—78No evidence of disease—10Excision39MBack—106.5No evidence of disease—11Excision72FRight upper lip—65Disease-freeLung cancer12Excision78FCrown of scalp—96No evidence of disease—13Excision83FApex of scalp—46No evidence of disease—14Excision57MSkin overlying parotid gland—102No evidence of disease—15Shave biopsy48MRight scalp—27No evidence of disease—16Excision59MLeft medial ankle—97No evidence of disease—TMB tumor mutation burden, MS mutation signature
Morphologic features
Fourteen of 16 cases demonstrated similar histologic features characterized by a predominately lobular architecture with a dermal, multinodular follicular proliferation of basaloid epithelial cells arranged in nests and strands surrounded by a dense cellular and fibrotic stroma (Fig. 1). Occasional keratin cysts, rare papillary mesenchymal bodies, and focal pseudoglandular formation associated with mucin deposition were observed. In all cases, the epidermis was uninvolved.Fig. 1. Histologic features of “conventional” trichoblastoma. Low magnification (A–B) hematoxylin and eosin-stained sections shows a multinodular proliferation of lesion cells arranged in nests surrounded by a dense cellular and fibrotic stroma with occasional keratin cysts. High magnification (C–D) hematoxylin and eosin-stained sections demonstrates nests of basaloid cells with rare pseudoglandular formation
One case demonstrated large, circumscribed aggregates of cytologically atypical basaloid cells with frequent mitotic figures and abundant apoptosis (Fig. 2). These aggregates involved the full thickness of the dermis and extended into the subcutaneous fat. Within the background, smaller nests and strands of basaloid epithelial cells with benign cytologic features, morphologically similar to the 14 cases of “conventional” trichoblastoma described above, were observed. These findings were consistent with trichoblastic carcinoma arising in the setting of a “conventional” trichoblastoma.Fig. 2. Histologic features of trichoblastic carcinoma. Low magnification (A) hematoxylin and eosin-stained sections shows similar findings to Fig. 1, including a dermal proliferation of basaloid cells arranged in nests. However, low (B) and high magnification (C) hematoxylin and eosin-stained sections show a clear demarcation between malignant nests and benign trichoblastoma components. On high magnification of the malignant nests (D–F), nuclear atypia, increased mitotic activity, and apoptosis are observed. Immunohistochemical studies demonstrate that the nests of atypical cells show diffuse expression of BerEP4 (G) and p63 (H), as well as a high Ki-67 proliferative index (I) and increased p53 expression (J)
Another case demonstrated focal areas of tightly packed round clusters of basaloid cells (“cell balls”) with peripheral palisading with a background of fibrous and myxoid stroma, consistent with trichogerminoma-like morphology (Fig. 3).Fig. 3. Histologic features of trichogerminoma. Low magnification (A–B) hematoxylin and eosin-stained sections show tightly packed round clusters of basaloid cells (“cell balls”) with peripheral palisading and a background of fibrous and myxoid stroma
Immunohistochemical features
Six cases of conventional trichoblastoma were tested for CK20 expression and five of six cases showed a few isolated CK20-positive cells, consistent with the expected staining pattern.
In a single case of trichoblastic carcinoma, immunohistochemical analysis revealed diffuse cytoplasmic Ber-Ep4 and p63 reactivity. The tumor cells were negative for CK20, adipophilin, INSM1, SOX-10, CEA, EMA, androgen receptor (AR), c-MYB, and S100. The Ki-67 proliferative index was elevated, reaching up to 60% within larger basaloid aggregates, highlighting increased cellular proliferation. Additionally, p53 expression was notably increased in the large aggregates of lesional cells.
Molecular findings
RNA sequencing identified a FOXK1(chr7 exon 2)::GRHL1(chr2 exon 2) fusion in the case of trichogerminoma, accompanied by decreased FOXK1 expression downstream of the fusion breakpoint. Additionally, several MALAT1 fusions were identified with MALAT1 as the 3′ partner and 5′ partner (Fig. 4).Fig. 4. Molecular findings of the studied cases. A Cosmic signatures per individual tested case. The x-axis indicates the respective case number. B Fusion diagram of the FOXKR1::GRLH1 fusion identified in the case of trichogerminoma
All cases that underwent RNA sequencing (6/6, 100%) demonstrated a high TMB. Mutation signature analysis, using COSMIC mutation signatures as a background, revealed universal (6/6) presence of SBS1 (albeit a small number in a subset of cases), substitutions resulting from 5-methylcytosine deamination. The second most prevalent signature, SBS84, attributed to activation-induced cytidine deaminase (AID) activity, was observed in 50% of cases. Interestingly, SBS38, the COSMIC signature most commonly associated with UV-light damage, was uniquely absent in all six tested samples.
Discussion
Trichoblastomas (TB) are relatively uncommon cutaneous adnexal neoplasms of follicular origin with a predilection for the head and neck region. These tumors may arise in the setting of Brooke-Spiegler [3–16], or Rombo syndrome [17, 18], in which case they are most commonly seen in young female patients [16], or they may arise sporadically in middle-aged to older adults [17]. Genetically, CYLD mutations are found in syndromic settings, while sporadic cases may show mutations involving HRAS, especially if arising in the background of nevus sebaceous [3]. One of the major challenges clinically and pathologically is that there is significant overlap between TB and other basaloid neoplasms, such as basal cell carcinoma (BCC).
Several previous studies have investigated the immunohistochemical phenotype of TB and trichoblastic carcinoma to aid in differentiating them from histologic mimics [5, 9, 19]. While not shown in the present study, trichoblastic tumors have been shown to typically be Ber-EP4 and AR negative [4]. However, rare exceptions exist as demonstrated in the present study which identified a trichoblastic carcinoma with diffuse Ber-EP4 expression. Additionally, trichoblastic tumors have been reported to show focal and sparse CK20 reactivity in Merkel cells [4, 5]. CD10 reactivity within surrounding stroma is also supportive [5, 9, 19]. In the present case of trichoblastic carcinoma, increased p53 expression and Ki-67 index were observed. However, given the absence of comparative staining in the benign trichoblastomas within this cohort and the lack of evidence on this topic in the literature, these findings should be interpreted with caution until further research identifies the diagnostic utility of this observation.
Just like many other mimics of BCC, trichoblastic tumors may originally be misdiagnosed. It is accepted that BCC is typically driven by alterations impacting the Sonic Hedgehog (Hh) pathway (i.e. PTCH1 and TP53) and often harbors hallmark ultraviolet (UV)-related mutation signatures, including C > T transitions at dipyrimidine sites [20, 21]. While TBs usually lack mutations involving PTCH1, to the best of our knowledge, comprehensive molecular studies focusing on sporadic TB have not been conducted. Our study identified a possible unique aberrant molecular pattern which has the potential to serve as a diagnostic tool in delineating between these two entities. Specifically, RNA sequencing of six cases of TB identified a universal high TMB and a mutational signature of SBS1, substitutions resulting from 5-methylcytosine deamination. While this may not be entirely specific, it is noteworthy that none of the cases harbored a known UV-related mutational signature. Thus, in the appropriate clinical and histologic context, the absence of UV-related mutational signatures may provide supportive molecular evidence for trichoblastic tumors and serve as a distinguishing feature from BCC. However, due to the limitation of RNA sequencing in detecting mutational signatures (see below), this finding requires further investigation to establish its legitimacy. Ultimately, evaluating a combination of morphology, immunohistochemistry, and the presence or absence of molecular aberrations is most helpful when differentiating between trichoblastic tumors and BCC (see Table 2). Table 2A comparison of the morphologic, immunohistochemical, and molecular features of trichoblastoma, trichogerminoma, trichoblastic carcinoma, and basal cell carcinomaFeatureTrichoblastoma (TB)TrichogerminomaTrichoblastic carcinomaBasal cell carcinoma (BCC)MorphologyMultinodular follicular proliferation of basaloid epithelial cells, papillary mesenchymal bodies, keratin cystsLobules of basaloid cells with central “cell balls” and peripheral palisadingBasaloid nests with atypia, mitoses, apoptosis, necrosis; may have adjacent benign TB componentBasaloid nests; peripheral palisading; clefting; mucinous stroma, vary based on subtypeLocationDermis to subcutisDermis to subcutisDermis to subcutisEpidermis to dermisMarginsPushingPushingInfiltrativeInfiltrativeNecrosisAbsentOften absentPresentMay be presentImmunohistochemistryCK20 + Merkel cells (retained); CD10 + (stromal); BerEP4-(typically); AR-CK5/6 +; P63 +; CD10 + (stromal); Bcl-2 + (ring-like peripheral rim of “cell balls”)Variable; often show high Ki-67BerEP4 +; CD10 + (epithelial); AR ±; CK20 − Molecular featuresCYLD mutations in syndromic cases; may be negative for UV-related* mutation signatures; possible fusions: YAP1::MAML2, YAP1::NUTM1, and RNF13::PAK2Existing data suggests fusions involving GRHL1/2/3, such as FOXK1::GRHL1May show p53 and PI3-AKT aberrationsPTCH1 mutations common; Hedgehog pathway activation; often show UV-related* mutation signaturesClinical behaviorBenignBenignMalignantLocally aggressive; rarely metastasizesAssociated syndromesNevus sebaceus; Brooke-Spiegler (CYLD)None currently knownMay arise from TB or de novoGorlin syndrome (PTCH1)
As stated above, all cases of trichoblastoma which underwent RNA sequencing exhibited a mutational signature of SBS1. Previous reports have shown that the number of SBS1 mutations correlates with cell age and type, as well as may reflect the number of mitoses a cell has undergone in its lifetime [22, 23]. The second most prevalent signature in 50% of cases, SBS84, has been previously reported in lymphoid neoplasms [22]. Notably, a recent case series by Kervarrec et al. identified YAP1::MAML2, YAP1::NUTM1, and RNF13::PAK2 in-frame fusions in four cases of benign TB as well as other adnexal neoplasms, suggesting possible oncogenic drivers [24]. Although both, the present study and the study by Kervarrec et al., employed RNA sequencing to detect gene alterations, no recurrent or recognized fusion was detected in our analysis. This discrepancy may be due to many factors, including the technical limitations of RNA sequencing on formalin-fixed, paraffin-embedded tissue (outlined below), primer-related limitations, as well as the potential biological heterogeneity of trichoblastomas, which may be driven by a diverse range of oncogenic mechanisms beyond gene fusions [25].
We also reported one case of trichoblastic carcinoma, which may arise de novo or within an existing benign TB [8, 9, 25–29]. Malignant transformation has been described in sporadic and syndromic (i.e., CYLD mutation) trichoblastomas [26, 29–33]. The diagnosis of malignant transformation relies on the identification of cytologic atypia and mitotic activity within basaloid tumor nests with or without apoptosis and necrosis [8, 9, 25–27]. These tumors have been stratified into low-grade and high-grade categories with the low-grade variants demonstrating more indolent behavior, while their high-grade counterparts are associated with a poor prognosis [26, 29]. A more recent investigation, however, has suggested that these tumors may be less aggressive than previously thought [27]. The pathogenesis of malignant transformation to trichoblastic carcinoma remains poorly understood, although p53 and PI3-AKT aberrations are thought to possibly play a role [8, 28]. While we believe that it would be highly informative to pursue molecular testing on the precursor and malignant components, regrettably, we were unable to perform additional testing in our case.
We herein also identified a case of trichogerminoma, often referred to as the trichogerminoma variant of TB, which is a distinct adnexal follicular neoplasm that exhibits a characteristic histologic appearance of well-circumscribed nodules of densely packed rounded nests of basaloid cells forming “cell balls” with variably cellular stroma [13, 33–38]. Given the distinct and characteristic morphologic and molecular features of trichogerminoma, this may indeed be a unique entity and not a “true” variant of TB. Malignant transformation of a trichogerminoma is exceedingly rare, with only two cases reported in literature [39]. Recurrent FOXK1::GRHL1 fusions have been identified in a previous case series of trichogerminomas by Kervarrec et al. which also share the histologic manifestations of the present case [13]. The clinical significance of this fusion remains unclear; however, it is hypothesized that fusions involving GRHL1/2/3 may be the oncogenic driver and identification of such may represent a helpful diagnostic tool to separate it from other morphologic mimics.
FOXK1 (forkhead box K1) is localized to chromosome 7p22.1 and is involved in many physiologic processes including regulation of metabolism (i.e., aerobic glycolysis), autophagy, and cell differentiation, migration, and proliferation [40, 41]. FOXK1-related fusions have been identified in previous reports of trichogerminoma [13], malignant melanoma [42, 43], adenocarcinoma of the prostate [42], ovary [42], and breast [43].
In contrast, the fusion partner GRHL1 is located on chromosome 2p25.1 and encodes grainyhead like transcription factor 1 which is involved in human development [44]. Fusions involving GRHL1 have been identified in previous reports of trichogerminomas [13] and sebaceomas [45].
As a case series, there are several limitations to the present study. Most notably, while RNA sequencing provides insight into expressed gene fusions and potential somatic variants, there are many limitations in its use for analyzing TMB and mutational signatures [46]. Unlike DNA-based methods, RNA sequencing has reduced sensitivity and specificity for detecting single nucleotide variants and small insertions/deletions (indels), particularly in low-expression or non-expressed genes, as it has a bias toward highly expressed genes [46]. Furthermore, without matched normal tissue, distinguishing somatic mutations from germline variants with RNA sequencing remains challenging and may lead to an overestimation of TMB due to residual germline contamination and technical artifacts, even after stringent filtering [46, 47]. Similarly, while mutational signature analysis from RNAseq data is feasible, it remains less robust compared to DNA-derived signatures, especially for detecting UV-related patterns, which may be underrepresented or missed if the relevant genes are not expressed at sufficient levels. This is a key limiting point of the present study, as we highlight the lack of UV-related signature in TB as a diagnostic tool when trying to exclude BCC. Given these limitations, our observations regarding high TMB, the presence of SBS1 and SBS84 mutational signatures, and the absence of a UV-related mutational signature should be interpreted as preliminary until further validation using DNA-based sequencing with matched normal tissue is performed to confirm these findings and assess their clinical relevance.
In conclusion, trichoblastoma is a rare cutaneous adnexal neoplasm composed of nested basaloid cells that may undergo malignant transformation. Trichogerminoma, traditionally thought to be a variant of trichoblastoma, has been shown to commonly harbor GRHL1/2/3-related fusions. While immunohistochemistry can aid in distinguishing trichoblastic tumors from other cutaneous basaloid entities, its utility remains limited. While additional studies with larger case numbers and additional comprehensive molecular analyses are needed, our study provides evidence that a non-UV-related mutational signature, specifically SBS1, may serve as a helpful diagnostic feature in differentiating basal cell carcinoma from trichoblastic tumors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thomas M, Bruant-Rodier C, Bodin F, Cribier B, Huther M, Dissaux C (2017) De l’intérêt de différencier les carcinomes trichoblastiques (CT) des carcinomes basocellulaires (CBC). À propos de 21 cas [Why is it important to differentiate trichoblastic carcinomas (CT) from basal cell carcinomas (CBC). About 21 cases]. Annales de Chirurgie Plastique Esthétique 62(3):212–218. 10.1016/j.anplas.2017.03.00110.1016/j.anplas.2017.03.00128385570 · doi ↗ · pubmed ↗
- 2National Center for Biotechnology Information (NCBI). FOXK 1 forkhead box K 1 [Homo sapiens (human)]. www.ncbi.nlm.nih.gov. Accessed 08 June 2025
- 3National Center for Biotechnology Information (NCBI). GRHL 1 grainyhead like transcription factor 1 [Homo sapiens (human)]. www.ncbi.nlm.nih.gov. Accessed 08 June 2025