Drug-related problems and their determinants among stroke patients in suburban China: a PCNE-based analysis with targeted initiatives
Ying Liu, Mingfen Wu, Jing Zhao, Wenhua Yang, Qi Wu, Li He, Sijie Zhang, Fengzhao Han

TL;DR
This study identifies common drug-related problems among stroke patients in suburban China and finds behavioral and health factors that increase the risk, suggesting pharmacist-led interventions could improve drug use.
Contribution
The study applies the PCNE classification system to identify DRPs in stroke patients and proposes targeted initiatives for better drug management.
Findings
482 DRPs were identified, with suboptimal treatment effectiveness and unclear issues being most common.
Patient-related factors like intentional underuse and inappropriate dosing were major causes of DRPs.
Alcohol use, diabetes, depression/anxiety, and high animal fat intake significantly increased DRP risk.
Abstract
Stroke remains a major public health burden in China, and the complexity of long-term pharmacotherapy often places stroke survivors at high risk for drug-related problems (DRPs). This study aimed to identify determinants of DRPs among community-dwelling stroke patients in suburban Beijing and to propose targeted initiatives for improving rational drug use. A cross-sectional study was conducted from August 2022 to December 2024 among 481 stroke patients. Pharmacists performed face-to-face interviews to collect demographic, clinical, and drug-related information. DRPs were identified and categorized using the Pharmaceutical Care Network Europe (PCNE) Classification System (V9.1). Chi-square tests and multivariate logistic regression were used to determine factors associated with DRPs. A total of 482 DRPs were identified, corresponding to 575 cause entries. The most common problems…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
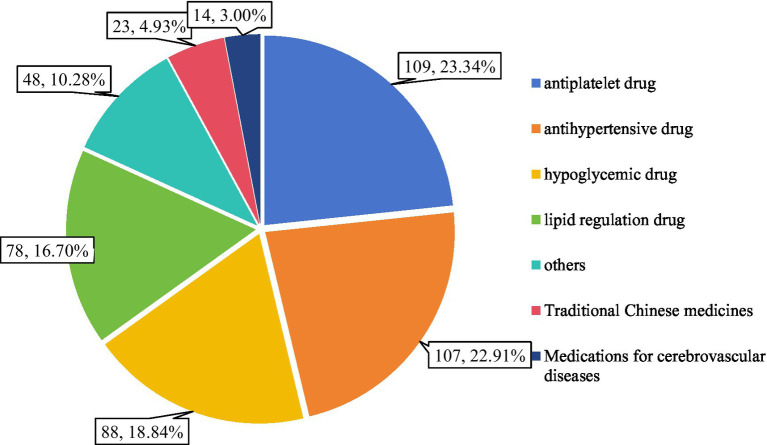 Figure 1
Figure 1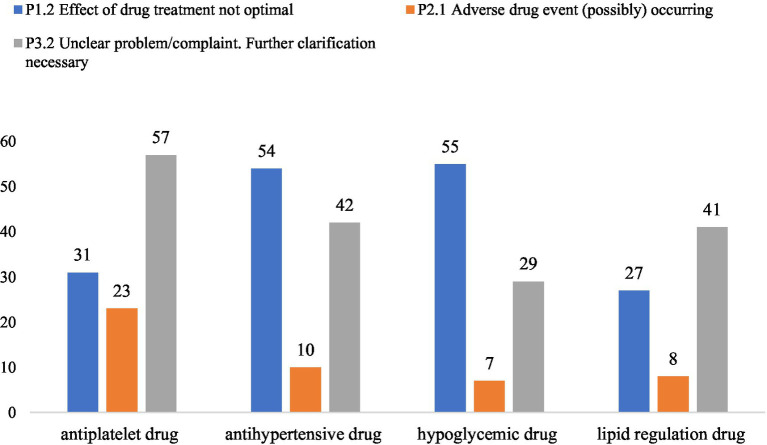 Figure 2
Figure 2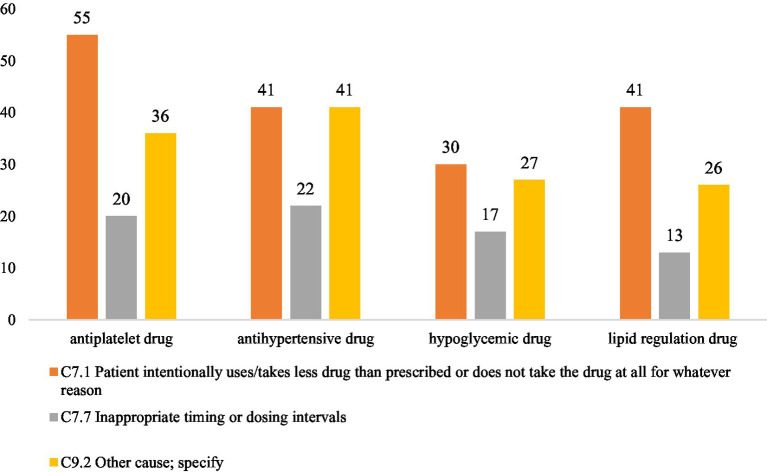 Figure 3
Figure 3| Characteristics | Total, | DRPs, |
|
| |||
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| Basic information | Gender | Male | 295 | 166 | 129 | 1.805 | 0.179 |
| Female | 186 | 93 | 93 | ||||
| Age | 18–59, | 154 | 86 | 68 | 0.364 | 0.546 | |
| ≥60, | 327 | 173 | 154 | ||||
| Education level | Primary/Junior high school | 330 | 180 | 150 | 0.695 | 0.706 | |
| Senior high school or Junior college | 117 | 63 | 54 | ||||
| Bachelor’s/Master’s degree | 34 | 16 | 18 | ||||
| Marital status | Married | 435 | 238 | 197 | 1.950 | 0.583 | |
| Divorced | 7 | 4 | 3 | ||||
| Widowed | 36 | 16 | 20 | ||||
| Single | 3 | 1 | 2 | ||||
| Expenses | Monthly income, CNY | <5,000 | 393 | 203 | 190 | 4.154 | 0.042 |
| ≥5,000 | 88 | 56 | 32 | ||||
| Monthly cost on drug, CNY | <500 | 354 | 186 | 168 | 0.931 | 0.628 | |
| 500–1,000 | 110 | 63 | 47 | ||||
| >1,000 | 17 | 10 | 7 | ||||
| Reimbursement type | Self-funded/other types | 46 | 26 | 20 | 0.170 | 0.680 | |
| Full or partial | 435 | 232 | 203 | ||||
| Living habits | Smoking | Yes | 136 | 78 | 58 | 2.727 | 0.256 |
| No | 247 | 124 | 123 | ||||
| Quit smoking | 98 | 57 | 41 | ||||
| Alcohol consumption | Yes | 140 | 88 | 52 | 6.452 | 0.011 | |
| No | 341 | 171 | 170 | ||||
| Tea consumption | Yes | 274 | 141 | 133 | 1.459 | 0.227 | |
| No | 207 | 118 | 89 | ||||
| Coffee | Yes | 54 | 33 | 21 | 1.292 | 0.256 | |
| No | 427 | 226 | 201 | ||||
| Regular exercise | Yes | 372 | 200 | 172 | 0.005 | 0.946 | |
| No | 109 | 59 | 50 | ||||
| Comorbidity | Hypertension | Yes | 341 | 187 | 154 | 0.464 | 0.496 |
| No | 140 | 72 | 68 | ||||
| With diabetes | Yes | 165 | 105 | 60 | 9.686 | 0.002 | |
| No | 316 | 154 | 162 | ||||
| With hyperlipidemia | Yes | 268 | 139 | 129 | 0.955 | 0.328 | |
| No | 213 | 120 | 93 | ||||
| With coronary heart disease | Yes | 91 | 47 | 44 | 0.218 | 0.640 | |
| No | 390 | 212 | 178 | ||||
| Eating habits | Intaking of animal fat | Yes | 132 | 84 | 48 | 7.016 | 0.008 |
| Sometimes or no | 349 | 175 | 174 | ||||
| Intaking of seafood | Yes | 65 | 34 | 31 | 0.072 | 0.789 | |
| Sometimes or no | 416 | 225 | 191 | ||||
| Intaking of roughage | Yes | 199 | 112 | 87 | 0.810 | 0.368 | |
| Sometimes or no | 282 | 147 | 135 | ||||
| Intaking of vegetables | Yes | 319 | 171 | 148 | 0.022 | 0.882 | |
| Sometimes or no | 162 | 88 | 74 | ||||
| Intaking of nuts | Yes | 67 | 36 | 31 | 0.000 | 0.984 | |
| Sometimes or no | 414 | 223 | 191 | ||||
| Taste | mild | 192 | 108 | 84 | 0.743 | 0.389 | |
| heavy | 289 | 151 | 138 | ||||
| Drug | Number of medicines | <5 | 139 | 59 | 80 | 10.223 | 0.001 |
| ≥5 | 342 | 200 | 142 | ||||
| Emotion | Depression and anxiety | Yes | 88 | 57 | 31 | 5.174 | 0.023 |
| No | 393 | 202 | 191 | ||||
| Variables |
| SE | Wald |
| OR | 95%CI | |
|---|---|---|---|---|---|---|---|
| Month income (ref = <5,000) | >5,000 | 0.278 | 0.274 | 1.093 | 0.296 | 1.332 | 0.778–2.281 |
| Alcohol consumption (ref = No) | Yes | 0.571 | 0.222 | 6.604 | 0.010 | 1.770 | 1.145–2.735 |
| With diabetes (ref = No) | Yes | 0.598 | 0.213 | 7.896 | 0.005 | 1.818 | 1.198–2.758 |
| Intaking of animal fat (ref = sometimes or no) | Yes | 0.537 | 0.224 | 5.758 | 0.016 | 1.711 | 1.103–2.652 |
| Number of medicines (ref = <5) | >5 | 0.289 | 0.200 | 2.090 | 0.148 | 1.335 | 0.902–1.977 |
| Depression and anxiety (ref = No) | Yes | 0.550 | 0.264 | 4.332 | 0.037 | 1.733 | 1.033–2.909 |
| Self-assessed health score | −0.01 | 0.006 | 3.344 | 0.067 | 0.990 | 0.979–1.001 | |
| DRPs | First-level directory | Second-level directory | Types of problems | ||
|---|---|---|---|---|---|
| Code |
| Code |
| ||
| Treatment effectiveness | P1 | 197 | P1.1 | 4 | No effect of drug treatment despite correct use |
| P1.2 | 188 | Effect of drug treatment not optimal | |||
| P1.3 | 5 | Untreated symptoms or indication | |||
| Treatment safety | P2 | 52 | P2.1 | 52 | Adverse drug event (possibly) occurring |
| Other | P3 | 233 | P3.1 | 14 | Unnecessary drug-treatment |
| P3.2 | 219 | Unclear problem/complaint. Further clarification necessary (please use as escape only) | |||
| Total | 482 | 482 | |||
| Code | Antiplatelet drug | Antihypertensive drug | Hypoglycemic drug | Lipid regulation drug | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Aspirin | Clopidogrel | Total | CCB | ARB | Compound preparation | Others | Total | Biguanides | Insulin and its analogues | SGLT-2i | DDP4 inhibitor | Sulfonylureas | Ohers | Total | Statins | Antioxidant class | ||||
| P1 | P1.1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | |||||||||||||
| P1.2 | 31 | 27 | 4 | 54 | 31 | 14 | 3 | 3 | 3 | 55 | 25 | 10 | 8 | 3 | 3 | 2 | 4 | 27 | 27 | ||
| P1.3 | 1 | 1 | 1 | 1 | 1 | ||||||||||||||||
| P2 | P2.1 | 23 | 21 | 2 | 10 | 7 | 2 | 1 | 7 | 3 | 2 | 1 | 1 | 8 | 7 | 1 | |||||
| P3 | P3.1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||||||
| P3.2 | 57 | 52 | 5 | 42 | 21 | 13 | 4 | 3 | 1 | 29 | 17 | 6 | 2 | 1 | 1 | 2 | 41 | 41 | |||
| Total | 113 | 110 | 93 | 79 | |||||||||||||||||
| C1 | C1.1 | 3 | 1 | 1 | 1 | 2 | 1 | 1 | |||||||||||||
| C1.4 | 3 | 3 | |||||||||||||||||||
| C1.5 | 12 | 5 | 2 | 3 | 1 | 1 | 2 | 2 | |||||||||||||
| C2 | C2.1 | 2 | 1 | 1 | 3 | 1 | 2 | 1 | 1 | ||||||||||||
| C3 | C3.1 | 7 | 3 | 3 | 1 | 14 | 6 | 4 | 4 | ||||||||||||
| C3.2 | 3 | 2 | 1 | ||||||||||||||||||
| C3.3 | 1 | 1 | 2 | 1 | 1 | ||||||||||||||||
| C3.5 | 3 | 3 | 1 | 1 | 1 | 1 | |||||||||||||||
| C4 | C4.1 | 2 | 1 | 1 | |||||||||||||||||
| C6 | C6.1 | 2 | 2 | 1 | 1 | 4 | 3 | 1 | 1 | 1 | |||||||||||
| C6.2 | 1 | 1 | 9 | 3 | 3 | 2 | 1 | 1 | 1 | ||||||||||||
| C6.3 | 1 | 1 | |||||||||||||||||||
| C6.4 | 1 | 1 | |||||||||||||||||||
| C7 | C7.1 | 55 | 50 | 5 | 41 | 23 | 12 | 3 | 3 | 30 | 18 | 4 | 2 | 2 | 3 | 1 | 41 | 41 | |||
| C7.2 | 1 | 1 | 1 | 1 | 3 | 1 | 2 | ||||||||||||||
| C7.4 | 1 | 1 | |||||||||||||||||||
| C7.6 | 2 | 1 | 1 | ||||||||||||||||||
| C7.7 | 20 | 17 | 3 | 22 | 16 | 5 | 1 | 17 | 10 | 4 | 3 | 13 | 12 | 1 | |||||||
| C7.8 | 6 | 6 | 2 | 1 | 1 | 5 | 2 | 2 | 1 | ||||||||||||
| C7.9 | 4 | 3 | 1 | 3 | 1 | 2 | 2 | 2 | |||||||||||||
| C7.10 | 1 | 1 | |||||||||||||||||||
| C9 | C9.1 | 1 | 1 | ||||||||||||||||||
| C9.2 | 36 | 30 | 6 | 41 | 21 | 11 | 4 | 3 | 2 | 27 | 14 | 5 | 2 | 1 | 1 | 1 | 3 | 26 | 25 | 1 | |
| C9.3 | 1 | 1 | 2 | 1 | 1 | ||||||||||||||||
| Total | 131 | 137 | 129 | 90 | |||||||||||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Acute Ischemic Stroke Management · Antiplatelet Therapy and Cardiovascular Diseases
Introduction
Stroke has long been recognized as the leading cause of death in China (1), and in recent years it has also become one of the major contributors to disability across both urban and rural regions. What makes the situation more concerning is that the incidence is still climbing year by year (2). As a disease characterized by high morbidity, high disability, high mortality, and a remarkable tendency to recur, stroke requires long-term and standardized secondary prevention. International and national guidelines (3–5) consistently emphasize that appropriate pharmacotherapy is one of the most effective ways to reduce the risk of recurrent stroke and to secure better clinical outcomes.
Yet, the reality in everyday clinical practice is far from simple. Many stroke survivors live with multiple comorbidities (6), and the accumulation of drugs over time easily leads to polypharmacy (7). Polypharmacy increases the likelihood of potentially inappropriate drug use and consequently raises the incidence of drug-related problems (DRPs) (8). A substantial body of literature (9–11) has shown that DRPs are not trivial, they are linked to increased morbidity, higher hospitalization and mortality rates, and escalating healthcare expenditures. For patients living in the community, where long-term management after stroke is critical, identifying and preventing DRPs becomes even more essential (12).
The Pharmaceutical Care Network Europe (PCNE) classification system provides a structured and internationally adopted framework for describing and analyzing DRPs (13). Applying this system to community-dwelling stroke patients allows healthcare providers to detect issues early, trace the underlying causes, and intervene more systematically.
In suburban districts such as those around Beijing, stroke survivors often rely heavily on community medical services and pharmacist follow-up. However, evidence on DRPs in this specific population remains scarce. Understanding which factors drive DRPs, and how these factors interact with patients’ drug behaviors, comorbidities, and psychological status could offer practical guidance for improving community-level pharmaceutical care.
Therefore, this study aimed to classify DRPs among stroke patients living in the community using the PCNE system and to explore the determinants associated with their occurrence. By mapping out the key contributors to DRPs, we hope to provide evidence-based recommendations that support pharmacist-led home drug services, enhance community drug management, and ultimately promote safe and rational drug use among stroke survivors in suburban of China.
Materials and methods
Study design and ethics
This study was conducted as part of the Capital’s Funds for Health Improvement and Research (Grant No. CFH2022-3-7141). We employed a cross-sectional design in the Huairou District of Beijing, with data collected from August 1, 2022 to December 31, 2024. The sample size was determined through a power analysis (90% power), with reference to similar community-based stroke studies regarding key outcome proportions (14), and convenience sampling was used to recruit participants. A total of 481 community-dwelling stroke patients completed the survey.
All participants provided informed consent before the interviews. Each face-to-face interview was carried out by qualified clinical pharmacists, lasted approximately 20 min, and involved an electronic questionnaire. To ensure consistency and minimize bias in the assessment of DRPs, all interviews and subsequent evaluations were conducted by clinical pharmacists who had obtained certification and possessed over 3 years of work experience. The evaluation process followed standardized criteria based on drug labels, clinical guidelines, and expert consensus. All DRP classifications were independently reviewed by a senior pharmacist. Any discrepancies were resolved through discussion by a dedicated quality control panel. The study protocol was reviewed and approved by the Ethics Committee of Beijing Huairou Hospital (Approval No. (2022)-(016)-02).
Data collection
Inclusion criteria: (1) age≥18 years; (2) had experienced a stroke within the past 6 months and were not currently hospitalized; (3) used three or more prescribed drugs daily; (4) willing and able to participate in face-to-face interviews conducted by clinical pharmacists.
Procedure of visits and collaboration: The initial pharmacist visit was conducted face-to-face at various settings including hospitals, community clinics, or patients’ homes. Follow-up contacts were carried out via face-to-face meetings, phone calls, or WeChat as needed. For recruitment, some patients were referred to the study by their neurologists or family physicians after an assessment confirming they met the inclusion criteria. During the subsequent intervention phase, pharmacists communicated directly with the patients’ neurologists and/or family physicians to discuss and collaboratively adjust medication regimens.
Exclusion criteria: (1) patients with severe or terminal illnesses; (2) those with mental disorders or severe cognitive impairment; (3) inability to complete questionnaires; (4) incomplete clinical data precluding statistical analysis.
Questionnaire content
The questionnaire was developed by a multidisciplinary expert group including pharmacists, clinicians, sociologists, and health management specialists. Its development process involved literature review, expert consultation, and multiple rounds of discussion. The final instrument consisted of two major sections: (1) Influencing Factors Questionnaire. Collected demographic information, health status, comorbidities, and drug-use history. (2) DRPs Assessment. DRPs were evaluated using the Pharmaceutical Care Network Europe (PCNE) Classification System (Version 9.1). The PCNE structure includes Problem (P), Cause (C), Planned intervention (I), Intervention acceptance (A) and Outcome (O). For the purposes of this study, only the first two components, problems and causes were analyzed. Pharmacists reviewed each case sequentially within the PCNE framework and selected corresponding classifications to achieve both qualitative and quantitative evaluation of DRPs.
Data analysis
All analyses were performed using SPSS 26.0. Descriptive statistics were used to summarize participant characteristics. Chi-square tests were conducted to examine associations between the presence of DRPs and individual variables. Multiple logistic regression was then used to identify independent factors associated with DRPs. DRPs (yes/no) served as the dependent variable. Independent variables included marital status, education level, monthly income, monthly drug expenditure, medical reimbursement type, number of chronic diseases, comorbidities, lifestyle behaviors, health status indicators, disease-related factors, and history of adverse drug reactions. Gender and age were included as covariates. Variables for the multivariate logistic regression model were selected based on clinical relevance and a univariate screening threshold of p < 0.05. A sensitivity analysis using a threshold of p < 0.10 confirmed no additional variables warranted inclusion. The final model was built using the Enter method to include all preselected variables simultaneously.
Results
Participant characteristics
A total of 481 stroke patients were included in the analysis. Their basic demographic and clinical characteristics are summarized in Table 1. Among them, 295 (61.3%) were male and 186 (38.7%) were female. Most participants were aged 60 years or older (68.0%) and had a primary or junior high school education (68.6%). The majority reported a monthly income below 5,000 CNY.
Regarding lifestyle behaviors, about one-third reported current smoking or alcohol consumption, and most participants engaged in some form of regular physical activity. Comorbidities were common, particularly hypertension (70.9%), hyperlipidemia (55.7%), and diabetes (34.3%). Nearly 30% reported high intake of animal fat.
Polypharmacy was prevalent, more than 70% used five or more drugs daily. Almost half of the participants exhibited poor drug adherence, and around 18% reported symptoms of depression or anxiety. Continuous variables showed that the average BMI fell within the overweight range, and self-assessed health scores were moderate.
Two hundred fifty-nine stroke patients were detected having DRPs. Chi-square analysis indicated that several factors including monthly income, alcohol use, comorbid diabetes, high animal fat intake, polypharmacy, depressive/anxiety symptoms, and lower self-assessed health scores were significantly associated with the presence of DRPs.
Logistic regression analysis
Table 2 presents the multivariate logistic regression results. Several variables remained independently associated with DRPs after adjustment. Alcohol consumption significantly increased the likelihood of experiencing DRPs (OR = 1.770, p = 0.01). Comorbid diabetes was also an important determinant (OR = 1.818, p = 0.005). Higher animal fat intake (OR = 1.711, p = 0.016) significantly increased DRP risk. Depressive or anxiety symptoms were associated with the risk of DRPs (OR = 1.773, p = 0.037). Overall, the regression model suggests that behavioral, psychological, eating habits, and disease-related factors all contribute to DRP risk.
Assessment of DRPs and their causes
A total of 482 DRPs were identified in 259 patients according to the PCNE classification system (Table 3). The majority of DRPs were categorized under “other problems” (P3), primarily comprising unclear complaints or issues requiring further clarification (P3.2, n = 219). Problems related to treatment effectiveness were also frequent (P1; n = 197), with suboptimal treatment effect (P1.2; n = 188) being the most common subtype. A total of 52 treatment safety problems (P2.1) involved actual or potential adverse drug events.
Regarding causes, 482 DRPs can be attributed to 575 causes. Patient-related factors (C7) were the dominant category (n = 330). The most common issues included intentional underuse or non-use of drugs (C7.1; n = 198) and inappropriate timing or dosing intervals (C7.7; n = 88). Other notable causes included dosage-related problems (C3; n = 32), prescribing or drug selection issues (C1; n = 33), administration errors by healthcare professionals (C6; n = 23), and inadequate outcome monitoring (C9; n = 143).
Together, these findings indicate that DRPs among community-dwelling stroke patients primarily arise from suboptimal treatment effectiveness and patient-driven behaviors, particularly non-adherence and improper drug use.
Distribution of DRPs by drug category
Figure 1 shows the distribution of 482 DRPs across drug categories. The top four drugs most frequently associated with DRPs were antiplatelet agents, antihypertensives, antidiabetic drugs, and lipid-lowering drugs. The four drug categories with the highest number of DRPs are exhibited in Figure 2. For antiplatelet and lipid-lowering agents, the most common DRP type was “unclear problem/complaint,” often reflecting concerns requiring further clarification. For antihypertensives and antidiabetic agents, “suboptimal treatment effect” was the dominant issue.
Distribution of drug categories associated with identified DRPs among stroke patients.
The four drug categories with the highest number of DRPs.
Figure 3 shows the distribution of PCNE-classified causes for DRPs in the top four drug categories. Across all four categories, the leading cause was intentional underuse or discontinuation (C7.1), followed by “other causes” (C9.2) and inappropriate timing or dosing intervals (C7.7). A deeper examination suggested that antihypertensive and antidiabetic problems often emerged when blood pressure or blood glucose levels remained uncontrolled. In contrast, DRPs related to antiplatelet and lipid-lowering drugs frequently stemmed from patients discontinuing therapy due to concerns about potential adverse effects, thereby increasing their risk of recurrent ischemic events.
Distribution of PCNE-classified causes for DRPs in the top four drug categories.
Table 4 shows the distribution of active ingredient of four drug categories with the highest number of DRPs. In the analysis of the four types of drugs with a relatively high incidence of DRPS, antiplatelet drugs are mainly aspirin, antihypertensive drugs are mainly CCBs and ARBs, hypoglycemic drugs are mainly biguanides, alpha-glucosidase inhibitors and insulin, and lipid-regulating drugs are mainly statins. The causes of occurrence are consistent with the overall distribution.
Targeted initiatives for improving rational drug use
Based on the major determinants identified in this study, such as alcohol consumption, comorbid diabetes, higher animal fat intake, depressive or anxiety symptoms, and polypharmacy, as well as the distribution of PCNE-classified DRPs, several focused and feasible intervention strategies are suggested for community settings.
Strengthen drug adherence support. Our study found that poor drug adherence is a common type of DRPs in stroke patients. Implement structured pharmacist follow-up through home visits, phone calls, or digital reminders. When possible, simplify drug regimens and provide clear, user-friendly instructions to help patients take their drugs correctly.Address alcohol-related risks. Offer brief, evidence-based counselling on the impact of alcohol on stroke recurrence and drug effectiveness. Develop stepwise reduction plans and link patients to psychological or behavioral support when necessary.Optimize drug management for patients with diabetes. Encourage regular self-monitoring of blood glucose and ensure pharmacist involvement in adjusting therapy. Monitor for potential interactions between antidiabetic and antithrombotic agents and assess hypoglycemia risk.Provide psychological screening and support. Routinely screen for depression and anxiety using validated tools. Establish referral pathways for mental health services and closely monitor the safety and effectiveness of antidepressant therapy where applicable.Improve polypharmacy management. Conduct regular pharmacist-led drug reviews to identify therapeutic duplication, unnecessary drugs, and inappropriate dosages. Strengthen communication among healthcare providers to reduce inconsistent prescribing.Promote healthy lifestyle and dietary habits. Encourage dietary adjustments, such as reducing animal fat intake and following heart-healthy eating patterns, and provide clear guidance regarding food–drug interactions.Enhance community-based pharmaceutical care. Expand pharmacist-led services such as home drug reviews, chronic disease management clinics, and digital drug management systems to create a continuous and traceable model of care.
Overall, these targeted strategies support the development of a pharmacist-centered, closed-loop drug management system aimed at reducing DRPs and improving therapeutic outcomes among community-dwelling stroke patients.
Discussion
This study provides a detailed examination of DRPs among community-dwelling stroke patients in suburban Beijing and shows that DRPs are not only common but also closely tied to patient behavior, drug management practices, and psychological factors. Using the PCNE classification system, we observed that patient-related causes, especially intentional underuse, non-use, and timing errors, far exceeded prescriber- or system-related causes. This pattern is consistent with previous research showing that stroke survivors often struggle with long-term drug self-management and maintaining adherence over time (15–17).
One notable finding was the high proportion of DRPs categorized as **“**Unclear problem/complaint” (P3.2, 45%). This reflects a significant real-world challenge in post-stroke care management. Our analysis suggests that this category was predominantly composed of cases where patients intentionally discontinued essential secondary prevention medications (e.g., aspirin, atorvastatin), citing a belief that these drugs were unnecessary or ineffective for their condition. This perception constitutes a critical gap in patient understanding of the long-term, preventive benefits of such therapies, which are often not immediately tangible. The high frequency of P3.2 classifications underscores that in clinical practice, a major category of drug-related “problems” is not a pharmacological issue, but rather a knowledge and adherence barrier rooted in patient health beliefs (18). This finding powerfully reinforces the indispensable role of clinical pharmacists in moving beyond simple medication review to providing tailored, persistent patient education. Future interventions should focus on improving patients’ perception of treatment necessity and long-term benefit to address this fundamental cause of non-adherence (19).
Almost half of the participants exhibited poor drug adherence, this finding echoes robust evidence from large clinical registries and cohort studies demonstrating that greater adherence to secondary prevention drugs significantly reduces mortality and improves long-term outcomes after stroke or transient ischemic attack (20). A meta-analysis of post-stroke adherence also showed that non-adherence remains a widespread challenge, with adherence declining markedly over the first year after stroke (16). These data support the present study’s result, highlighting the need for structured, pharmacist-led interventions, such as pharmacist follow-up, regimen simplification, and digital adherence tools to support long-term drug persistence.
Behavioral factors, including alcohol consumption, also contributed significantly to DRPs. Daily alcohol consumption is directly and closely associated with the occurrence of DRPs. For some patients with chronic conditions, drinking may exacerbate or destabilize their illnesses, such as hypertension, gastric ulcers, and gout (21). Additionally, under the influence of alcohol, patients may exhibit behaviors like forgetting to take medication or taking duplicate doses. Therefore, for patients with chronic diseases and those on long-term medication, pharmacists educating them to abstain from or strictly limit alcohol is a crucial guarantee for safe and effective treatment. High-fat dietary habits have a clear and significant association with the occurrence of drug-related problems (DRPs) (p < 0.05). Such habits can induce or exacerbate underlying conditions such as hypertension and hyperlipidemia (22), complicating pharmacotherapy, while also interfering with the absorption of certain medications. Therefore, for patients requiring long-term medication, especially those with chronic diseases, maintaining a balanced diet and controlling fat intake is not only essential for disease management but also serves as a fundamental measure to ensure medication safety and reduce the risk of DRPs.
Comorbid diabetes further complicated drug regimens. Diabetic patients often take multiple long-term drugs and are more susceptible to drug–drug interactions, hypoglycemia risk, and increased treatment burden, as documented in diabetes-related polypharmacy studies (23). These findings reinforce the importance of integrated chronic care and pharmacist involvement for patients with multiple comorbid conditions.
Psychological conditions, particularly depression and anxiety were identified as additional drivers of DRPs. Post-stroke affective disorders are known to impair motivation, reduce engagement in health behaviors, and negatively affect drug-taking routines. Previous meta-analyses found that depression after stroke is associated with poorer adherence and worse functional outcomes (24, 25). Our findings align with this evidence, suggesting that screening for depression and anxiety and offering timely mental health support should be essential components of community-based stroke management.
Notably, we found that income remained statistically insignificant. We speculate that this may be due to China’s healthcare insurance policies and centralized procurement measures, which keep patients’ drug costs low enough to be covered by their monthly income. As a result, low income does not have a significant impact on the incidence of DRPs among patients.
Taken together, this study emphasizes that DRPs among stroke survivors are largely preventable and driven by modifiable patient-related factors. Previous work has shown that chronic disease management programs, particularly those involving pharmacists, can improve long-term drug adherence, simplify regimens, and reduce drug errors (26). The present findings support adopting similar models in community settings, where pharmacists play a central role in counseling, monitoring outcomes, performing drug reviews, and addressing patients’ concerns about their therapy.
The cause analysis using PCNE further demonstrated that DRPs were predominantly patient-related rather than prescriber-related. While some dosage or prescribing issues were present, patient-driven causes far outnumbered them, echoing previous studies in community and chronic disease populations (12, 27). These results underscore the need for pharmacist-led interventions, such as home drug reviews, simplified dosing schedules, clear communication through pictorial instructions, and outcome monitoring to reduce preventable DRPs.
Limitations
Our study still has some limitations. First, it was conducted in a single suburban district, which may limit generalizability. Second, data on adherence and lifestyle behaviors were self-reported, possibly introducing bias. Thirdly, we employed a convenience sampling method, with patients primarily sourced from hospital outpatient departments, referrals by neurologists, and recommendations from family physicians. As a result, data from bedridden patients or those unable to attend hospital visits were not comprehensively collected, which constitutes a limitation of this study. Future studies could employ longitudinal designs, objective adherence measures, and multi-site recruitment to validate and extend these findings.
Conclusion
DRPs are highly prevalent among community-dwelling stroke survivors in suburban Beijing. Their occurrence is strongly influenced by behavioral and lifestyle factors, comorbidities, and psychological status. Patient-related causes, especially intentional underuse and inappropriate drug timing dominated the PCNE cause spectrum. A pharmacist-centered, community-based care model that integrates DRP identification, personalized counseling, adherence support, and coordinated chronic disease management holds promise for reducing DRPs and improving therapeutic outcomes. Implementing such interventions may ultimately strengthen secondary prevention and reduce the long-term burden of stroke.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tu WJ Wang LD. China stroke surveillance report 2021. Mil Med Res. (2023) 10:33. doi: 10.1186/s 40779-023-00463-x 37468952 PMC 10355019 · doi ↗ · pubmed ↗
- 2Tu WJ Zhao Z Yin P Cao L Zeng J Chen H . Estimated burden of stroke in China in 2020. JAMA Netw Open. (2023) 6:e 231455. doi: 10.1001/jamanetworkopen.2023.145536862407 PMC 9982699 · doi ↗ · pubmed ↗
- 3Kleindorfer DO Towfighi A Chaturvedi S Cockroft KM Gutierrez J Lombardi-Hill D . 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. (2021) 52:e 364–467. doi: 10.1161/STR.0000000000000375, 34024117 · doi ↗ · pubmed ↗
- 4Dawson J Béjot Y Christensen LM De Marchis GM Dichgans M Hagberg G . European Stroke Organisation (ESO) guideline on pharmacological interventions for long-term secondary prevention after ischaemic stroke or transient ischaemic attack. Eur Stroke J. (2022) 7:II–I. doi: 10.1177/23969873221100032, 36082250 PMC 9446324 · doi ↗ · pubmed ↗
- 5Chinese Medical Association, Chinese Medical Association publishing house, Chinese Society of General Practice, editorial Board of Chinese Journal of general practitioners of Chinese Medical Association, expert Group of Guidelines for primary Care of Nervous System Disease. Guidelines for primary care management of ischemic stroke (practical edition 2021). Chin J General Pract. (2021) 20:947–58. doi: 10.3760/cma.j.cn 114798-20210804-00591 · doi ↗
- 6Gallacher KI Jani BD Hanlon P Nicholl BI Mair FS. Multimorbidity in stroke. Stroke. (2019) 50:1919–26. doi: 10.1161/STROKEAHA.118.02037631233391 · doi ↗ · pubmed ↗
- 7Matsumoto A Yoshimura Y Nagano F Bise T Kido Y Shimazu S . Polypharmacy and potentially inappropriate medications in stroke rehabilitation: prevalence and association with outcomes. Int J Clin Pharm. (2022) 44:749–61. doi: 10.1007/s 11096-022-01416-5, 35578145 · doi ↗ · pubmed ↗
- 8Krustev T Milushewa P Tachkov K. Impact of polypharmacy, drug-related problems, and potentially inappropriate medications in geriatric patients and its implications for Bulgaria-narrative review and meta-analysis. Front Public Health. (2022) 10:743138. doi: 10.3389/fpubh.2022.743138, 35309221 PMC 8927684 · doi ↗ · pubmed ↗