Case Report of Acute Severe Hyponatremia Induced by Desmopressin Administration During Chemotherapy
Koutaro Ono, Shugo Uematsu, Aya Yoshihara, Ayako Tsuboya, Shoichi Mori, Takashi Yoshioka, Shuichi Nawata

TL;DR
A 70-year-old man developed severe low sodium levels after resuming a medication called desmopressin during chemotherapy, highlighting the need to carefully manage this drug during cancer treatment.
Contribution
This case highlights the risk of desmopressin-induced hyponatremia during chemotherapy and advocates for its discontinuation to ensure treatment safety.
Findings
Resuming desmopressin during chemotherapy led to CTCAE Grade 4 hyponatremia.
Discontinuing desmopressin prevented recurrence of hyponatremia in subsequent chemotherapy cycles.
The patient completed all planned chemotherapy cycles after desmopressin was stopped.
Abstract
Patients undergoing chemotherapy are prone to developing hyponatremia due to insufficient oral intake because of nausea and vomiting, administration of large volumes of intravenous fluids, syndrome of inappropriate antidiuretic hormone secretion induced by chemotherapeutic agents, adrenal insufficiency, and drug interactions. Severe hyponatremia during chemotherapy interferes with continuation of cancer treatment. In addition, it may be difficult to distinguish hyponatremia from chemotherapy‐related adverse effects because of symptom similarity. This report presented a case of desmopressin‐induced severe hyponatremia during chemotherapy and discussed the appropriateness of discontinuing desmopressin administration. A 70‐year‐old male was hospitalized for postoperative adjuvant chemotherapy with cisplatin and vinorelbine for a pathological stage IIB adenocarcinoma of the right lower lung…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
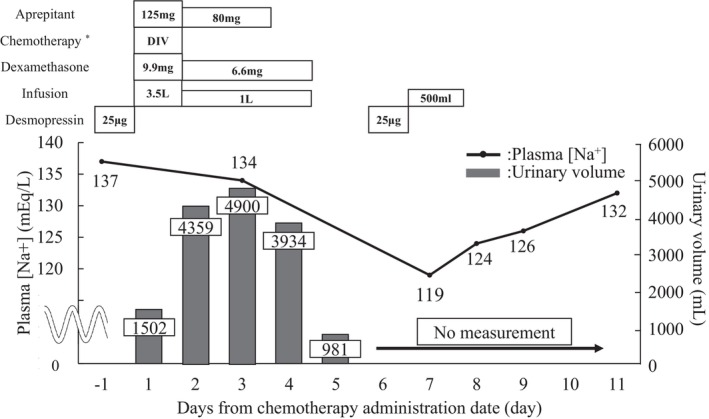 FIGURE 1
FIGURE 1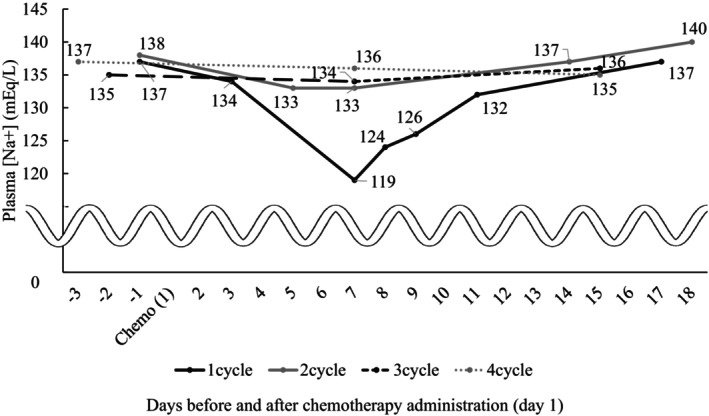 FIGURE 2
FIGURE 2| Date | Unit | Before Chemotherapy | 3 | 7 | 8 | 9 | 11 |
|---|---|---|---|---|---|---|---|
| Body temperature | °C | 36.3 | 36.8 | 36.4 | 36.4 | 36.4 | 36.3 |
| Heart rate | bpm | 69 | 85 | 76 | 79 | 78 | 69 |
| Blood pressure | mmHg | 124/86 | 145/83 | 133/98 | 108/70 | 111/76 | 126/78 |
| Respiratory rate | /min | 18 | 16 | 16 | 17 | 17 | 18 |
| WBC | /μL | 6160 | 9260 | 5310 | 3930 | 5010 | |
| Hb | g/dL | 15.1 | 15.3 | 15.9 | 16.9 | 16.3 | |
| Plt | /μL | 217,000 | 166,000 | 149,000 | 196,000 | 235,000 | |
| Neutophil | /μL | 4040 | 8450 | 3880 | 2740 | 3260 | |
| Alb | /μL | 4.2 | 3.9 | 3.5 | 3.7 | 3.8 | |
| Creatinine | mg/dL | 0.75 | 0.86 | 0.75 | 0.79 | 0.9 | 0.8 |
| eGFR | mL/min/1.73 m2 | 78.5 | 67.6 | 78.5 | 74.2 | 64.3 | 73.2 |
| BUN | mg/dL | 14 | 18.6 | 18.7 | 14.9 | 16.9 | 9.0 |
| Serum Na | mEq/L | 137 | 134 | 119 | 124 | 126 | 132 |
| Serum Cl | mEq/L | 103 | 98 | 85 | 90 | 91 | 97 |
| Serum K | mEq/L | 4.2 | 4.5 | 4.5 | 4.5 | 4.9 | 43 |
| Total bilirubin | mg/dL | 1.2 | 1.2 | 1.3 | 1.2 | 0.9 | |
| AST | mg/dL | 34 | 35 | 29 | 34 | 32 | |
| ALT | mg/dL | 45 | 49 | 58 | 63 | 66 | |
| CRP | mg/dL | 2.69 | 0.39 | 1.16 | 0.94 | 0.5 | |
| Blood glucose | mg/dL | 121 | 169 | 104 | 147 | 109 | |
| Urine specific gravity | 1.005 | 1.012 | |||||
| Urine creatinine | mg/dL | 0.1 | 1.0 | ||||
| Urine Na | mEq/L | 40 | 18 | ||||
| Urine Cl | mEq/L | 32 | 14 | ||||
| Urine K | mEq/L | 5.7 | 16.9 | ||||
| Urine osmolality | mOSM/kg H2O | 167 | 368 | ||||
| Serum osmolality | mOSM/kg | 260 | 270 | ||||
| TSH | μIU/mL | 1.01 | |||||
| FT3 | pg/mL | 2.35 | |||||
| FT4 | ng/dL | 1.91 | |||||
| Renin activity | ng/mL/h | 11.1 | |||||
| Adrenocorticotropic hormone | pg/mL | 26.1 | |||||
| Cortisol | μg/dL | 18 | |||||
| ADH | pg/mL | 0.8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectrolyte and hormonal disorders · Nausea and vomiting management · Chemotherapy-related skin toxicity
Introduction
1
Hyponatremia is an important clinical condition that occurs during chemotherapy. It may be accompanied by severe symptoms such as nausea, vomiting, fatigue, and neurological disorders [1], which may necessitate chemotherapy discontinuation. Causes may include excessive fluid intake, poor oral intake, adrenal insufficiency, syndrome of inappropriate antidiuretic hormone secretion (SIADH), diabetes mellitus, electrolyte disturbances caused by cisplatin (CDDP), and drug interactions [1]. Although hyponatremia can be fatal in severe cases, its clinical manifestations are similar to chemotherapy‐associated symptoms, making it difficult to differentiate. Therefore, it is critical to monitor patient‐related factors and medications that may predispose patients to hyponatremia during chemotherapy and implement early detection and prompt intervention.
Desmopressin, which is widely used to treat diabetes insipidus and nocturnal polyuria, acts on vasopressin V2 receptors in the renal‐collecting ducts to enhance water reabsorption into the bloodstream and reduce urine output. However, it can also lead to intravascular fluid retention and dilutional hyponatremia and, therefore, requires careful monitoring [2], particularly during chemotherapy. In addition, dexamethasone, which is commonly used as an antiemetic agent during chemotherapy, is contraindicated when used concurrently with desmopressin [3]. This is likely due to dexamethasone‐induced fluid retention enhancing the antidiuretic effect of desmopressin and causing hyponatremia. Thus, dose adjustment of each medication and careful monitoring are essential [4, 5, 6]. When administering agents such as desmopressin that may induce hyponatremia, careful consideration of treatment necessity and appropriate timing of reinitiation are critical.
This report presents a case wherein desmopressin was discontinued during chemotherapy because of an elevated risk of hyponatremia.
Case History and Examination
2
A 70‐year‐old male underwent a robot‐assisted right lower lobectomy for clinical stage IB (cT2aN0M0) adenocarcinoma of the right lower lobe and was diagnosed with pathological stage IIB (pT3N0M0) adenocarcinoma. Two months later, the patient was hospitalized for adjuvant chemotherapy with CDDP and vinorelbine (VNR). The medical history of the patient included nocturnal polyuria, type 2 diabetes mellitus, myocardial infarction, bronchial asthma, benign prostatic hyperplasia, and hypertension. To manage nocturnal polyuria, the patient had been taking oral desmopressin (25 μg daily) for the previous 4 years. The patient was also receiving mirabegron, linagliptin, pioglitazone, azilsartan, mecobalamin, a combination tablet of low‐dose aspirin and lansoprazole, rebamipide, omega‐3‐acid ethyl esters, and magnesium oxide to treat other comorbidities. The patient had a smoking history of 20 cigarettes per day for 30 years, no history of alcohol consumption, and no drug allergies. The height and weight of the patient were 171 cm and 75 kg, respectively. Blood and biochemical test results were as follows: white blood cell count 6160/μL, hemoglobin 15.1 g/dL, platelets 217,000/μL, neutrophil count 4040/μL, blood urea nitrogen 14.0 mg/dL, creatinine 0.75 mg/dL, estimated glomerular filtration rate 78.5 mL/min/1.73 m^2^, serum sodium (Na) concentration 137 mEq/L, serum chlorine (Cl) concentration 103 mEq/L, serum potassium (K) concentration 4.2 mEq/L, total bilirubin 1.2 mg/dL, aspartate aminotransferase 34 mg/dL, alanine aminotransferase 45 mg/dL, C‐reactive protein 2.69 mg/dL, and blood glucose 121 mg/dL.
Differential Diagnosis, Investigations, and Treatment
3
Adjuvant chemotherapy with CDDP plus VNR was administered according to our institutional chemotherapy schedule (Data S1). The patient received antiemetic therapy for highly emetogenic chemotherapy and hydration therapy to prevent CDDP‐induced nephrotoxicity, with CDDP administered at 80 mg/m^2^ on day 1 and VNR administered at 25 mg/m^2^ on days 1 and 8. At chemotherapy, the patient received 3500 mL of intravenous fluids, and 20 mg of furosemide was administered, followed by 1000 mL per day for the next 3 d, and oral fluid intake of 1.5–2.5 L per day. Although urine output of approximately 4000 mL/day was maintained for 3 day post‐chemotherapy, the overall fluid balance was considered positive. Oral desmopressin was discontinued from day 1 of chemotherapy as dexamethasone is contraindicated. Following chemotherapy initiation, the patient developed Common Terminology Criteria for Adverse Events (CTCAE) Grade 2 nausea, which improved following administration of 5 mg oral metoclopramide; however, oral intake by the patient remained low. The patient developed CTCAE Grade 3 nausea and a decreased appetite on day 7 after resuming desmopressin administration. Blood tests revealed a serum Na concentration of 119 mEq/L, corresponding to CTCAE Grade 4 hyponatremia (Figure 1). VNR administration was discontinued on day 8. No abnormalities were detected in the other electrolyte concentrations and no renal dysfunction was observed (Table 1). The urinary Na concentration increased to 40.0 mEq/L. No increase in antidiuretic hormone secretion or decrease in adrenocorticotropic hormone or cortisol concentration was observed; therefore, we eliminated SIADH and adrenal insufficiency.
*Serum sodium concentration in first cycle. Changes in plasma sodium concentration and urinary volume during the first chemotherapy cycle and timing of concomitant medication administration Cisplatin 80 mg/m2, vinorelbine 25 mg/m2, infusion 3 L, Mg 10 mEq, furosemide 20 mg, palonosetron 0.75 mg, and dexamethasone 9.9 mg.
Outcome and Follow‐Up
4
Following the discontinuation of oral administration of desmopressin, administration of 500 mL intravenous normal saline and restriction of oral fluid intake, the serum Na concentration of the patient gradually improved and nausea was resolved. Desmopressin was not resumed thereafter, and the patient continued the same chemotherapy regimen of CDDP plus VNR without hyponatremia recurrence during subsequent cycles (Figure 2).
Serum sodium concentration for each cycle. Changes in plasma sodium concentration pre‐ and post‐chemotherapy across four treatment cycles.
Discussion
5
Hyponatremia incidence associated with oral desmopressin was higher in the first 12 weeks of treatment. Among patients with a baseline serum Na concentration ≥ 140 mEq/L, hyponatremia occurs in approximately 5.1%. In contrast, those with lower baseline concentration (135–139 mEq/L) experience an incidence as high as 14.9% [7]. Since hyponatremia incidence (serum Na concentration < 135 mEq/L) among patients with cancer is approximately 20%–40%, the risk of desmopressin‐induced hyponatremia is considered high [8, 9]. Additionally, the effect of chemotherapy differs depending on the agents used; hyponatremia incidence is reported to be 11.9% with platinum‐based agents and 3.8% with non‐platinum agents. In the present case, no hyponatremia occurred following the discontinuation of oral desmopressin from the second cycle onward. Collectively, oral desmopressin may be a major contributor to the development of severe hyponatremia in this patient. However, as this patient had been taking oral desmopressin for a long period, the risk of hyponatremia due to desmopressin monotherapy was considered low. Therefore, severe hyponatremia was caused by reduced serum Na concentration, due to multiple factors (e.g., reduced Na intake, fluid overload, and enhanced urinary Na excretion due to furosemide administration), along with desmopressin‐induced fluid retention.
Patients with cancer are prone to developing hyponatremia [10], and SIADH accounts for a significant proportion of these cases. It is also well‐established that CDDP carries a high risk of hyponatremia through either renal salt‐wasting syndrome (RSWS) or SIADH [11, 12]. This patient was initially suspected of having drug‐induced SIADH or RSWS, as we found elevated urinary Na excretion, a decrease in serum osmolality, and an increase in urinary osmolality. However, the acute onset of symptoms following desmopressin administration, rapid improvement of symptoms after desmopressin discontinuation, and the absence of symptoms after the second cycle of chemotherapy during desmopressin interruption suggested that CDDP and VNR were not the causes. Furosemide‐induced increases in Na excretion were thought to be the most likely cause. Cisplatin‐induced RSWS was also evaluated; however, the decrease in urine Na levels 2 days after the onset of hyponatremia, as well as the absence of hyponatremia during the second and subsequent cycles of treatment, indicate that cisplatin's involvement was small.
However, oral desmopressin was discontinued on day 1 of chemotherapy because the concomitant use of dexamethasone, an antiemetic agent, is contraindicated. Considering the half‐life of desmopressin (approximately 2.5 h), a sufficient interval was allowed before chemotherapy initiation. Additionly, no decrease in serum Na concentration was observed on day 3, suggesting that no interaction with dexamethasone had occurred. Although the biological half‐life of dexamethasone (approximately 36–54 h) may have allowed its effects to persist at desmopressin resumption, the cortisol concentration was not suppressed when hyponatremia developed, indicating that residual effects of dexamethasone were unlikely. Thus, hyponatremia in this case was not caused by an interaction between desmopressin and dexamethasone. However, owing to this interaction, we could not eliminate the possibility that severe hyponatremia could develop early if desmopressin administration was continued during chemotherapy. Therefore, waiting at least 1 week before continuing desmopressin administration is necessary for avoiding any adverse effects.
Conclusions
6
Patients undergoing chemotherapy are at risk of developing hyponatremia owing to the side effects of anticancer drugs. As in the present case, desmopressin to treat nocturnal polyuria should not be administered under potential hyponatremic conditions. When administering anticancer drugs, it is advisable to assess the necessity of continuing hyponatremia‐prone agents, such as desmopressin, and temporarily suspend their administration during the anticancer drug administration period. Additionally, the decision to resume desmopressin administration should be made after considering the potential interactions with anticancer agents and dexamethasone, ensuring an interval of approximately 1 week between dexamethasone administration and the resumption of desmopressin administration.
Author Contributions
Koutaro Ono: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. Shugo Uematsu: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. Aya Yoshihara: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. Ayako Tsuboya: conceptualization, formal analysis, investigation, methodology, project administration, resources, writing – original draft, writing – review and editing. Shoichi Mori: conceptualization, resources. Takashi Yoshioka: conceptualization, data curation, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. Shuichi Nawata: formal analysis, project administration, writing – original draft, writing – review and editing.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
Written informed consent was obtained from the patient. All specific patient information was obtained.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1: Cisplatin plus vinorelbine regimen schedule.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. J. Castillo , M. Vincent , and E. Justice , “Diagnosis and Management of Hyponatremia in Cancer Patients,” Oncologist 17, no. 6 (2012): 756–765, 10.1634/theoncologist.2011-0400.22618570 PMC 3380874 · doi ↗ · pubmed ↗
- 2G. Narayen and S. N. Mandal , “Vasopressin Receptor Antagonists and Their Role in Clinical Medicine,” Indian Journal of Endocrinology and Metabolism 16, no. 2 (2012): 183–191, 10.4103/2230-8210.93734.22470853 PMC 3313734 · doi ↗ · pubmed ↗
- 3US FDA , “Desmopressin Acetate (NDA 018938) Approval History/Drug Application Overview. U.S. FDA. NDA 018938 Approval Actions and Application Overview,” (2026), https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&Appl No=018938.
- 4D. J. Greenblatt and J. Koch‐Weser , “Clinical Pharmacokinetics (Second of Two Parts),” New England Journal of Medicine 293, no. 19 (1975): 964–970, 10.1056/NEJM 197511062931905.1101062 · doi ↗ · pubmed ↗
- 5International Council for Harmonisation (ICH) , M 12 Drug Interaction Studies: Guidance for Industry. Final Guidance Adopted by FDA (2024), https://www.fda.gov/regulatory‐information/search‐fda‐guidance‐documents/m 12‐drug‐interaction‐studies Pharmaceuticals Safety and Environmental Health Bureau, Japan. Guideline on Drug Interaction for Drug Development and Appropriate Provision of Information. PSEHB Notification No. 0723–4, July 23 2018. Tokyo: Ministry of Health, Labour and Welfare; 2018, acces
- 6Y. Ogawa , S. Murata , K. Kuramoto , and A. Nakano , “Long‐Term Safety of Desmopressin Orally Disintegrating Tablets in Men With Nocturia due to Nocturnal Polyuria: Interim Results of a Specified Drug Use‐Results Survey in Japan,” LUTS: Lower Urinary Tract Symptoms 16, no. 3 (2024): e 12513, 10.1111/luts.12513.38616722 PMC 11500684 · doi ↗ · pubmed ↗
- 7A. J. Shaikh , S. A. Bawany , N. Masood , et al., “Incidence and Impact of Baseline Electrolyte Abnormalities in Patients Admitted With Chemotherapy Induced Febrile Neutropenia,” Journal of Cancer 2 (2011): 62–66, 10.7150/jca.2.62.21326626 PMC 3039222 · doi ↗ · pubmed ↗
- 8S. M. Doshi , P. Shah , X. Lei , A. Lahoti , and A. K. Salahudeen , “Hyponatremia in Hospitalized Cancer Patients and Its Impact on Clinical Outcomes,” American Journal of Kidney Diseases 59, no. 2 (2012): 222–228, 10.1053/j.ajkd.2011.08.029.22001181 · doi ↗ · pubmed ↗