Endoscopic full-thickness resection of a rectal submucosal tumor with the double-tunnel bridge formation method: a case report
Naoya Toyoshima, Masau Sekiguchi, Hiroyuki Takamaru, Yukihide Kanemitsu, Susumu Hijioka, Toshihiro Haga, Yutaka Saito

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
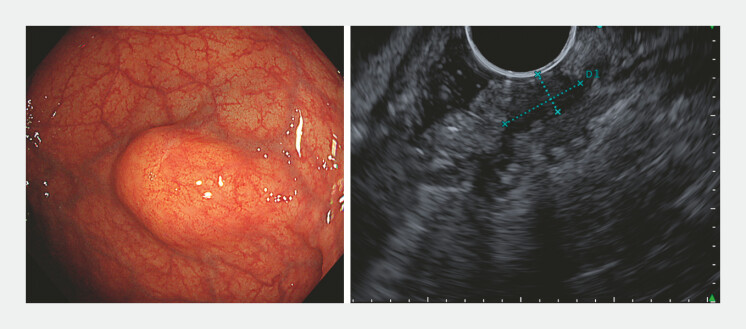 Fig. 1
Fig. 1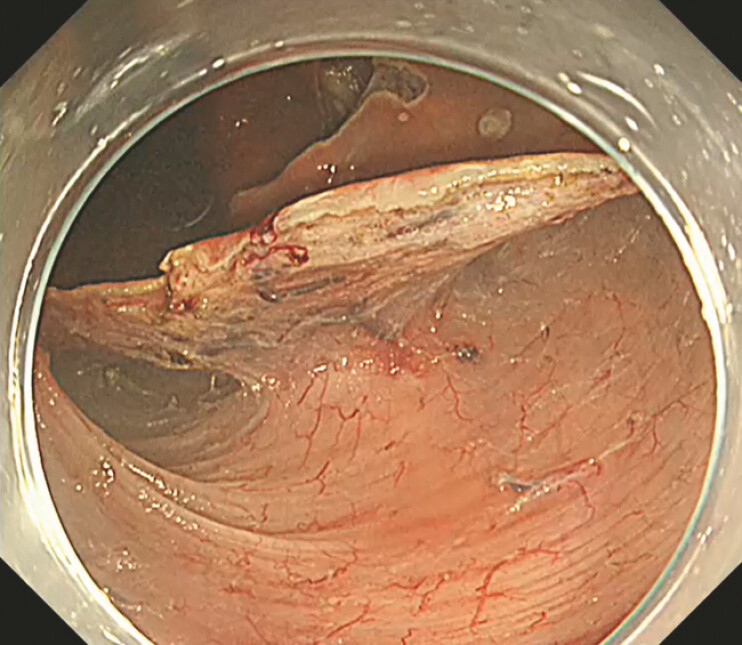 Fig. 2
Fig. 2 Fig. 3
Fig. 3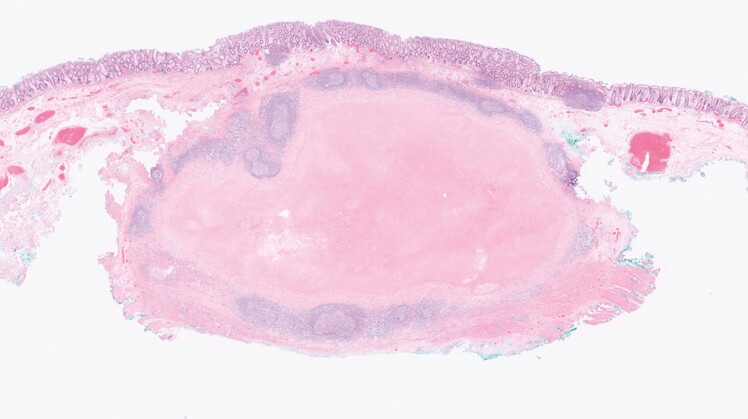 Fig. 4
Fig. 4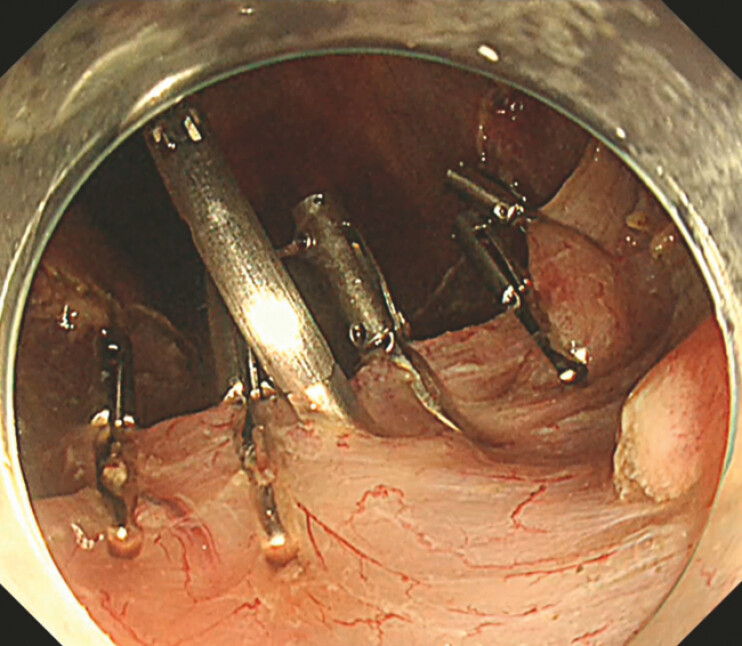 Fig. 5
Fig. 5- —Bringing the gap between R&d and the Ideal society and Generating Economic and social value (BRIDGE)
- —NCC MIRAI project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Gastric Cancer Management and Outcomes
Endoscopic submucosal dissection (ESD) is a treatment option for colorectal epithelial lesions that enables en bloc resection of large or fibrotic lesions 1 . In Western countries, endoscopic full-thickness resection (EFTR) is often selected for difficult lesions, particularly those with severe fibrosis or non-lifting characteristics 2 3 . In Japan, where ESD originated, several technical methods – such as the double-tunnel method and the bridge formation method (BFM) – have been developed to facilitate resection in challenging cases 4 . In addition, peranal endoscopic myectomy (PAEM) has recently emerged as a minimally invasive option for lesions involving the muscularis propria, highlighting the usefulness of double-tunnel creation for controlled myectomy 5 . Building on these advancements, we applied double-tunnel formation and BFM to EFTR to achieve precise dissection and safe full-thickness resection of deeply invasive submucosal tumors (SMTs).
A 74-year-old woman was referred after a positive fecal immunochemical test. Colonoscopy revealed a rectal SMT, and both boring biopsy and endoscopic ultrasound (EUS)-guided fine-needle aspiration were non-diagnostic. EUS showed an 11-mm hypoechoic submucosal mass partially extending into the muscularis propria ( Fig. 1 ). Endoscopic resection was performed for diagnosis ( Video 1 ). Two submucosal tunnels were created, but the lesion was not visualized, suggesting deeper involvement ( Fig. 2 ). Inner circular muscle resection was initiated, and with the BFM approach, the overlying mucosa was preserved to provide natural traction and clarify the dissection plane 2 . The lesion penetrated the muscularis propria and was removed en bloc as a full-thickness specimen ( Fig. 3 , Fig. 4 ). The defect was closed with a Mantis clip and additional standard clips, achieving secure ( Fig. 5 ) closure. The patient recovered uneventfully.
A 15-mm submucosal tumor located in the lower rectum. Endoscopic ultrasonography showing an 11-mm extramural hypoechoic lesion.
Wide mucosal incision and creation of two submucosal tunnels using the bridge formation method (BFM).
Full-thickness resection performed only at the area containing the tumor by utilizing natural traction.
Granulomatous inflammation observed in the SMT-like lesion. SMT, submucosal tumor.
Closure of the full-thickness defect using clips.
DBFR-assisted endoscopic full-thickness resection of a rectal submucosal tumor, showing double-tunnel creation, natural traction using the mucosal bridge, selective full-thickness dissection, and clip closure of the defect. DBFR, double-tunnel bridge formation.Video 1
This novel technique, termed the double-tunnel bridge formation method-assisted EFTR (DBFR), offers three major advantages: (i) the double-tunnel approach limits the extent of muscle resection; (ii) BFM provides natural traction and a clear dissection plane without additional devices; and (iii) the limited full-thickness defect permits secure closure with clips.
Endoscopy_UCTN_Code_TTT_1AQ_2AD_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiba H Ohata K Hayashi A Outcomes in colorectal endoscopic submucosal dissection for large protruded lesions: a retrospective multicenter study Endosc Int Open 202412 E 757E 76310.1055/a-2316-775538847018 PMC 11156516 · doi ↗ · pubmed ↗
- 2Schmidt A Beyna T Schumacher B Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications Gut 2018671280128910.1136/gutjnl-2016-31367728798042 · doi ↗ · pubmed ↗
- 3Zwager LW Bastiaansen BAJ Bronzwaer MES Endoscopic full-thickness resection (e FTR) of colorectal lesions: results from the Dutch colorectal e FTR registry Endoscopy 2020521014102310.1055/a-1195-122332498100 · doi ↗ · pubmed ↗
- 4Abe M Oda I Ishihara R Usefulness of the Bridge Formation Method for colorectal endoscopic submucosal dissection JGH Open 20259566410.1002/jgh 3.70149 PMC 1197645640201338 · doi ↗ · pubmed ↗
- 5Toyonaga T Ohara Y Baba S Peranal endoscopic myectomy (PAEM) for rectal lesions with severe fibrosis and exhibiting the muscle-retracting sign Endoscopy 20185081381710.1055/a-0602-390529883977 · doi ↗ · pubmed ↗