Endoscopic ultrasound-guided injection-assisted precise localization for endoscopic removal of a penetrating foreign body in the gastric antrum: a case report
Tian-Xing Yuan, Long Huang, Miao-Miao Li, Yu Bao, Rui Zhao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
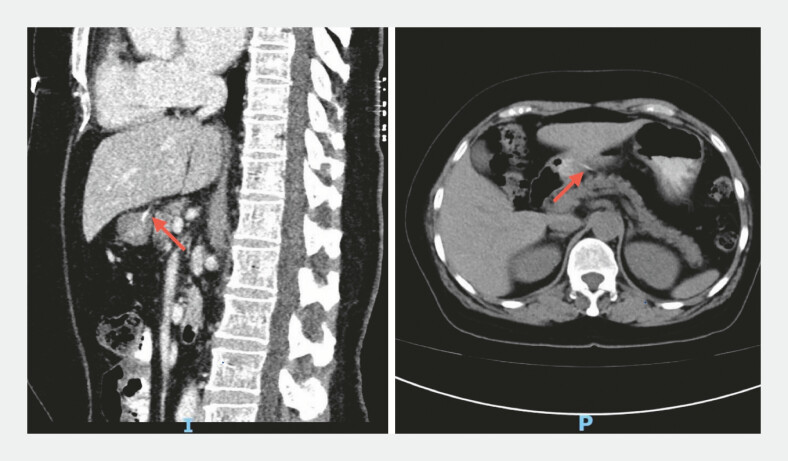 Fig. 1
Fig. 1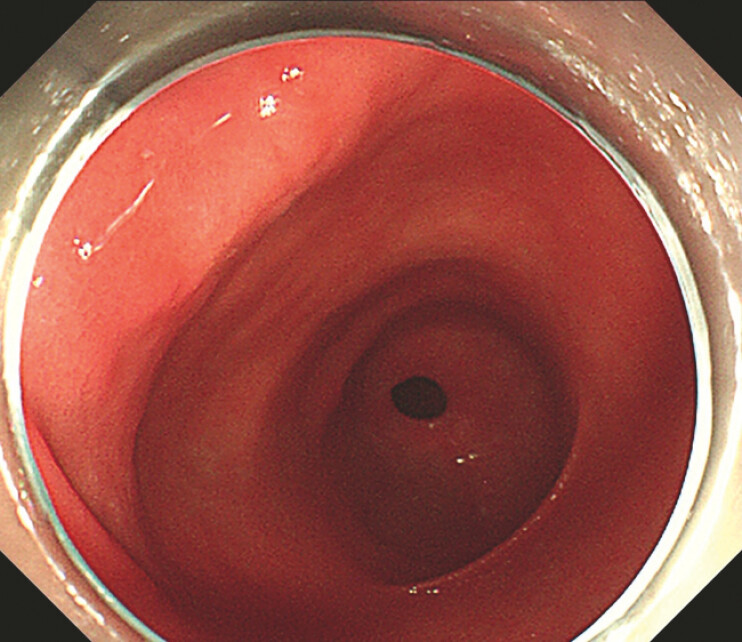 Fig. 2
Fig. 2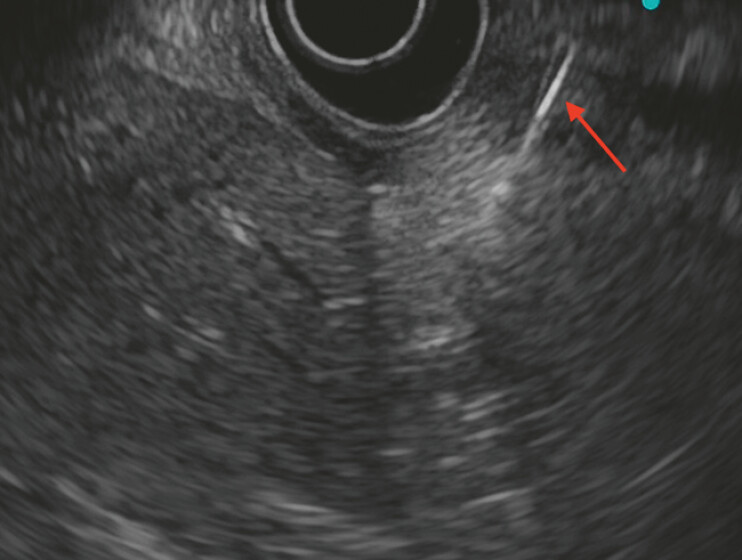 Fig. 3
Fig. 3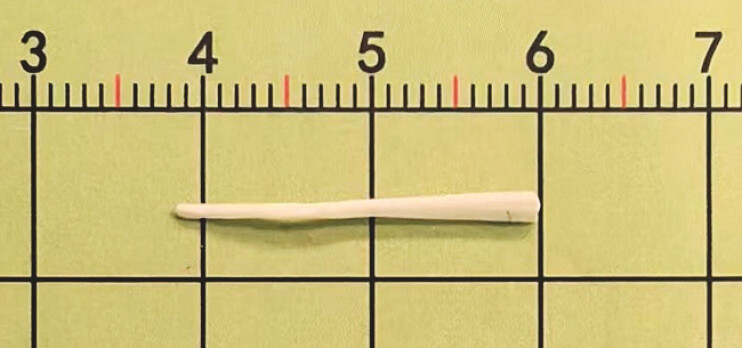 Fig. 4
Fig. 4- —Chengdu Science and Technology Bureau10.13039/501100010822
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
A 61-year-old woman presented with a 2-week history of a foreign body at the lesser curvature of the gastric antrum after accidental fish bone ingestion, accompanied by upper abdominal pain radiating to the back.
Contrast-enhanced computed tomography revealed a linear hyperdense foreign body in the gastric antrum penetrating the gastric wall into the peritoneal cavity ( Fig. 1 ). Conventional gastroscopy showed no obvious abnormalities ( Fig. 2 ). Endoscopic ultrasound demonstrated a linear foreign body embedded within the wall of the lesser curvature of the gastric antrum ( Fig. 3 ).
Contrast-enhanced computed tomography showed high-density linear shadows of the antrum and penetrated the stomach wall into the abdominal cavity.
No significant abnormalities were observed under endoscopy.
Endoscopic ultrasound shows the location and depth of the fishbone.
Based on the clinical history and imaging findings, endoscopic submucosal dissection (ESD) was planned. Under endoscopic ultrasound (EUS) guidance, methylene blue was injected to localize the lesion. A focal mucosal incision at the marked site revealed a whitish fibrotic capsule, within which the distal end of the foreign body was exposed and gently extracted with forceps. A white, triangular-shaped foreign body was removed ( Fig. 4 ). No residual foreign material was observed, and the defect was closed with titanium clips. ( Video 1 ).
A 2.2cm fish bone.
Injection under the guidance of endoscopic ultrasound assists the endoscope to remove the penetrating foreign body of the antrum.Video 1
Fish bones penetrating the gastric wall are often insidious and may not produce obvious mucosal changes on conventional endoscopy, leading many cases to be managed surgically or via laparoscopy 1 . Previous studies have also highlighted the critical role of EUS in locating deeply embedded or impacted foreign bodies, assessing penetration depth, and guiding subsequent interventions 2 . However, most reports describe the need for full-thickness ESD or surgical exposure after localization. In contrast, in our case, EUS-guided methylene blue injection enabled precise surface localization, allowing successful removal through a limited mucosal incision without extensive submucosal dissection or surgical intervention. This approach is both feasible and simplified, suggesting that EUS-assisted targeted localization may substantially reduce procedural complexity and offer a minimally invasive alternative for managing deeply embedded gastric foreign bodies.
Endoscopy_UCTN_Code_TTT_1AO_2AL
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li J Wang QQ Xue S Gastric submucosal lesion caused by an embedded fish bone: A case report World J Clin Cases 202210109910510.12998/wjcc.v 10.i 3.109935127925 PMC 8790457 · doi ↗ · pubmed ↗
- 2Jugnundan S Gupta S Gupta S Deeply embedded esophageal fishbone removed by endoscopic submucosal dissection Endoscopy 20245601 E 94910.1055/a-2436-129839515766 PMC 11548993 · doi ↗ · pubmed ↗