A Retrospective Analysis of Extended Hospital Stays in Patients With Pneumonia and Diabetic Comorbidities in a Rural Midwestern Area
Shlok Rathi, Abbigail Niewchas, Max Balla, Brendan Lamboglia, Mariam Akhtar, Nova Beyersdorfer, Kerry Johnson, John Paulson

TL;DR
This study found that pneumonia is the main factor causing longer hospital stays, even when diabetes is present, especially in older patients.
Contribution
The study provides new insights into how pneumonia affects hospital stay duration more than diabetes in a rural population.
Findings
Pneumonia is the strongest predictor for hospital stays of six days or more.
Older patients (65+) had longer stays for both pneumonia and diabetes compared to younger patients.
Age, but not gender, influenced the proportion of extended stays in pneumonia and diabetes cases.
Abstract
Pneumonia is one of the leading causes of hospitalization in the United States, resulting in many hospitalizations and deaths per year. Diabetes is an often-concurrent diagnosis that affects a large population. There is little research regarding the relationship between diabetes and the length of stay for patients hospitalized with pneumonia. This retrospective study aims to analyze whether the presence of diabetes mellitus in patients diagnosed with pneumonia increases the length of stay. Electronic medical records (EMR) from Freeman Health System in Southwest Missouri were utilized to analyze this relationship. Results of this study demonstrated that, in patients diagnosed with diabetes (type I or type II), pneumonia, or a combination of diabetes and pneumonia, pneumonia is the strongest predictor for a hospital stay ≥6 days. Further analysis, looking at age and gender, supported this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
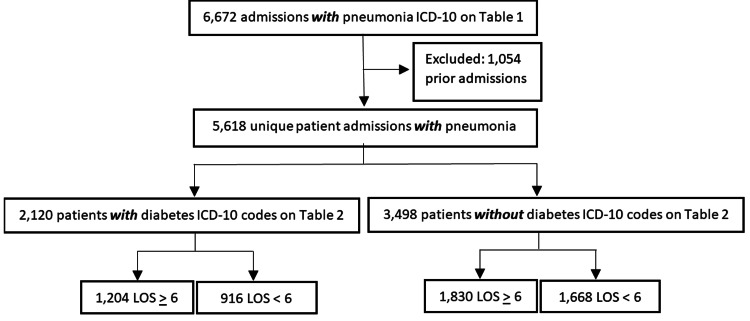 Figure 1
Figure 1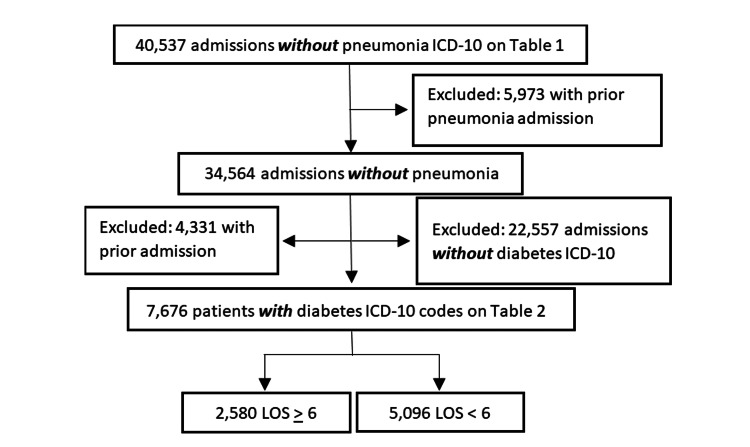 Figure 2
Figure 2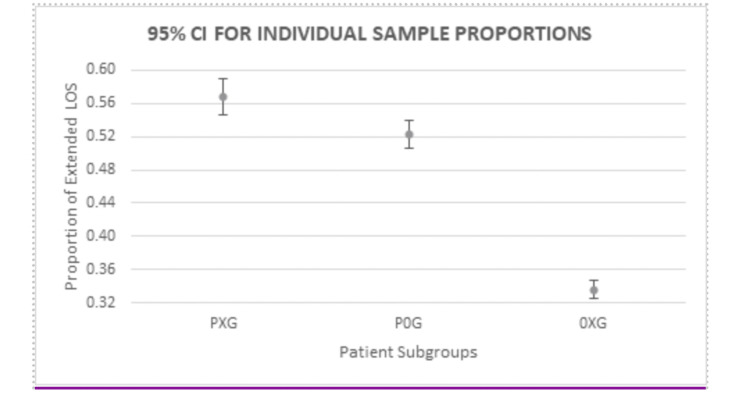 Figure 3
Figure 3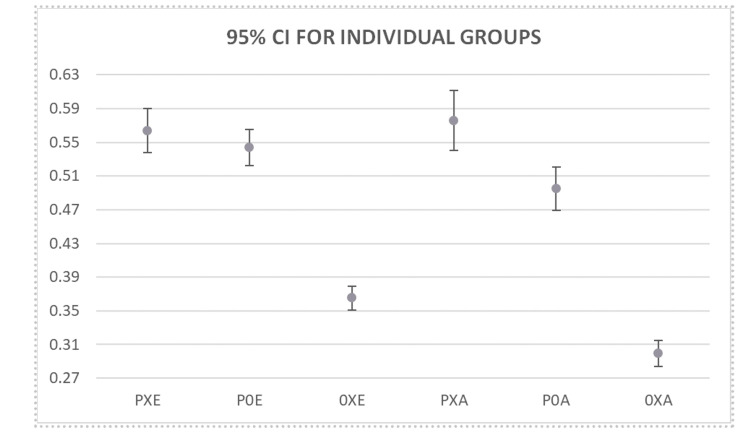 Figure 4
Figure 4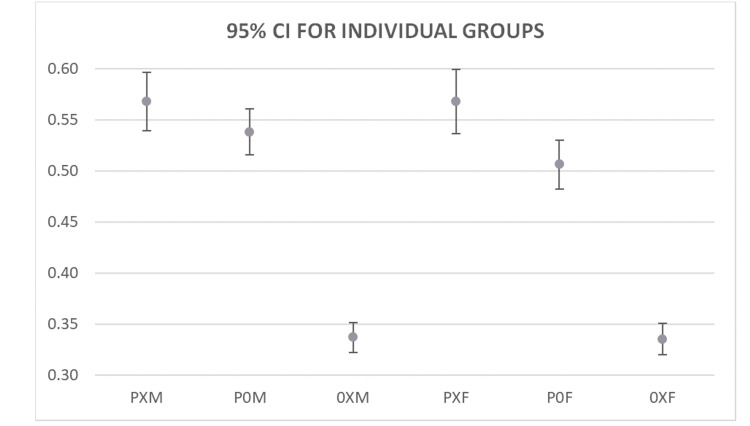 Figure 5
Figure 5| ICD-10 Codes | Description |
| J1000 | Influenza due to other identified influenza virus with unspecified type of pneumonia |
| J1001 | Influenza due to other identified influenza virus with the same other identified influenza virus pneumonia |
| J1008 | Influenza due to other identified influenza virus with other specified pneumonia |
| J1100 | Influenza due to unidentified influenza virus with unspecified type of pneumonia |
| J1108 | Influenza due to unidentified influenza virus with specified pneumonia |
| J120 | Adenoviral pneumonia |
| J121 | Respiratory syncytial virus pneumonia |
| J122 | Parainfluenza virus pneumonia |
| J123 | Human metapneumovirus pneumonia |
| J1281 | Pneumonia due to SARS-associated coronavirus |
| J1282 | Pneumonia due to coronavirus disease 2019 |
| J1289 | Other viral pneumonia |
| J129 | Viral pneumonia, unspecified |
| J13 | Pneumonia due to Streptococcus pneumoniae |
| J14 | Pneumonia due to Hemophilus influenzae |
| J150 | Pneumonia due to Klebsiella pneumoniae |
| J151 | Pneumonia due to Pseudomonas |
| J1520 | Pneumonia due to staphylococcus, unspecified |
| J15211 | Pneumonia due to Methicillin susceptible Staphylococcus aureus |
| J15212 | Pneumonia due to Methicillin resistant Staphylococcus aureus |
| J1529 | Pneumonia due to other staphylococcus |
| J153 | Pneumonia due to streptococcus, group B |
| J154 | Pneumonia due to other streptococci |
| J155 | Pneumonia due to Escherichia coli |
| J156 | Pneumonia due to other Gram-negative bacteria |
| J157 | Pneumonia due to Mycoplasma pneumoniae |
| J158 | Pneumonia due to other specified bacteria |
| J159 | Unspecified bacterial pneumonia |
| J160 | Chlamydial pneumonia |
| J168 | Pneumonia due to other specified infectious organisms |
| J17 | Pneumonia in diseases classified elsewhere |
| J180 | Bronchopneumonia, unspecified organism |
| J181 | Lobar pneumonia, unspecified organism |
| J188 | Other pneumonia, unspecified organism |
| J189 | Pneumonia, unspecified organism |
| J84116 | Cryptogenic organizing pneumonia |
| J851 | Abscess of lung with pneumonia |
| J95851 | Ventilator associated pneumonia |
| ICD-10 Codes | Diagnosis |
| E0822 | Diabetes mellitus due to underlying condition with diabetic chronic kidney disease |
| E0840 | Diabetes mellitus due to underlying condition with diabetic neuropathy, unspecified |
|
| Diabetes mellitus due to underlying condition with hypoglycemia without coma |
| E0865 | Diabetes mellitus due to underlying condition with hyperglycemia |
| E088 | Diabetes mellitus due to underlying condition with unspecified complications |
| E089 | Diabetes mellitus due to underlying condition without complications |
| E0922 | Drug or chemical induced diabetes mellitus with diabetic chronic kidney disease |
| E0951 | Drug or chemical induced diabetes mellitus with diabetic peripheral angiopathy without gangrene |
|
| Drug or chemical induced diabetes mellitus with hypoglycemia without coma |
| E0965 | Drug or chemical induced diabetes mellitus with hyperglycemia |
| E098 | Drug or chemical induced diabetes mellitus with unspecified complications |
| E099 | Drug or chemical induced diabetes mellitus without complications |
| E1010 | Type 1 diabetes mellitus with ketoacidosis without coma |
| E1011 | Type 1 diabetes mellitus with ketoacidosis with coma |
| E1021 | Type 1 diabetes mellitus with diabetic nephropathy |
| E1022 | Type 1 diabetes mellitus with diabetic chronic kidney disease |
| E1029 | Type 1 diabetes mellitus with other diabetic kidney complication |
|
| Type 1 diabetes mellitus with unspecified diabetic retinopathy without macular edema |
| E103493 | Type 1 diabetes mellitus with severe nonproliferative diabetic retinopathy without macular edema, bilateral |
| E103592 | Type 1 diabetes mellitus with proliferative diabetic retinopathy without macular edema, left eye |
| E103599 | Type 1 diabetes mellitus with proliferative diabetic retinopathy without macular edema, unspecified eye |
| E1039 | Type 1 diabetes mellitus with other diabetic ophthalmic complication |
| E1040 | Type 1 diabetes mellitus with diabetic neuropathy, unspecified |
| E1042 | Type 1 diabetes mellitus with diabetic polyneuropathy |
| E1043 | Type 1 diabetes mellitus with diabetic autonomic (poly)neuropathy |
| E1051 | Type 1 diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E1052 | Type 1 diabetes mellitus with diabetic peripheral angiopathy with gangrene |
|
| Type 1 diabetes mellitus with diabetic neuropathic arthropathy |
|
| Type 1 diabetes mellitus with diabetic dermatitis |
|
| Type 1 diabetes mellitus with foot ulcer |
|
| Type 1 diabetes mellitus with other skin ulcer |
|
| Type 1 diabetes mellitus with other skin complications |
|
| Type 1 diabetes mellitus with hypoglycemia without coma |
| E1065 | Type 1 diabetes mellitus with hyperglycemia |
| E1069 | Type 1 diabetes mellitus with other specified complication |
| E108 | Type 1 diabetes mellitus with unspecified complications |
| E109 | Type 1 diabetes mellitus without complications |
| E1100 | Type 2 diabetes mellitus with hyperosmolarity without nonketotic hyperglycemic-hyperosmolar coma (NKHHC) |
| E1101 | Type 2 diabetes mellitus with hyperosmolarity with coma |
| E1110 | Type 2 diabetes mellitus with ketoacidosis without coma |
| E1111 | Type 2 diabetes mellitus with ketoacidosis with coma |
| E1121 | Type 2 diabetes mellitus with diabetic nephropathy |
| E1122 | Type 2 diabetes mellitus with diabetic chronic kidney disease |
| E1129 | Type 2 diabetes mellitus with other diabetic kidney complication |
|
| Type 2 diabetes mellitus with unspecified diabetic retinopathy with macular edema |
|
| Type 2 diabetes mellitus with unspecified diabetic retinopathy without macular edema |
| E113299 | Type 2 diabetes mellitus with mild nonproliferative diabetic retinopathy without macular edema, unspecified eye |
| E113549 | Type 2 diabetes mellitus with proliferative diabetic retinopathy with combined traction retinal detachment and rhegmatogenous retinal detachment, unspecified eye |
| E113553 | Type 2 diabetes mellitus with stable proliferative diabetic retinopathy, bilateral |
| E113593 | Type 2 diabetes mellitus with proliferative diabetic retinopathy without macular edema, bilateral |
| E113599 | Type 2 diabetes mellitus with proliferative diabetic retinopathy without macular edema, unspecified eye |
| E1136 | Type 2 diabetes mellitus with diabetic cataract |
| E1139 | Type 2 diabetes mellitus with other diabetic ophthalmic complication |
| E1140 | Type 2 diabetes mellitus with diabetic neuropathy, unspecified |
| E1141 | Type 2 diabetes mellitus with diabetic mononeuropathy |
| E1142 | Type 2 diabetes mellitus with diabetic polyneuropathy |
| E1143 | Type 2 diabetes mellitus with diabetic autonomic (poly)neuropathy |
| E1144 | Type 2 diabetes mellitus with diabetic amyotrophy |
| E1149 | Type 2 diabetes mellitus with other diabetic neurological complication |
| E1151 | Type 2 diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E1152 | Type 2 diabetes mellitus with diabetic peripheral angiopathy with gangrene |
| E1159 | Type 2 diabetes mellitus with other circulatory complications |
|
| Type 2 diabetes mellitus with diabetic neuropathic arthropathy |
|
| Type 2 diabetes mellitus with other diabetic arthropathy |
|
| Type 2 diabetes mellitus with diabetic dermatitis |
|
| Type 2 diabetes mellitus with foot ulcer |
|
| Type 2 diabetes mellitus with other skin ulcer |
|
| Type 2 diabetes mellitus with other skin complications |
|
| Type 2 diabetes mellitus with hypoglycemia with coma |
|
| Type 2 diabetes mellitus with hypoglycemia without coma |
| E1165 | Type 2 diabetes mellitus with hyperglycemia |
| E1169 | Type 2 diabetes mellitus with other specified complication |
| E118 | Type 2 diabetes mellitus with unspecified complications |
| E119 | Type 2 diabetes mellitus without complications |
| E1310 | Other specified diabetes mellitus with ketoacidosis without coma |
| E1321 | Other specified diabetes mellitus with diabetic nephropathy |
| E1322 | Other specified diabetes mellitus with diabetic chronic kidney disease |
|
| Other specified diabetes mellitus with unspecified diabetic retinopathy without macular edema |
| E1340 | Other specified diabetes mellitus with diabetic neuropathy, unspecified |
| E1342 | Other specified diabetes mellitus with diabetic polyneuropathy |
| E1343 | Other specified diabetes mellitus with diabetic autonomic (poly)neuropathy |
| E1351 | Other specified diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E1352 | Other specified diabetes mellitus with diabetic peripheral angiopathy with gangrene |
|
| Other specified diabetes mellitus with foot ulcer |
|
| Other specified diabetes mellitus with hypoglycemia without coma |
| E1365 | Other specified diabetes mellitus with hyperglycemia |
| E1369 | Other specified diabetes mellitus with other specified complication |
| E139 | Other specified diabetes mellitus without complications |
| Groups | Description | Quantity |
| PXG | Pneumonia with diabetes (type I & II) | 2,120 |
| P0G | Pneumonia without diabetes (type I & II) | 3,498 |
| 0XG | Diabetes (type I & II) without pneumonia | 7,676 |
| Comparison | LOS Sample 1 | LOS Sample 2 | Sample 1 vs Sample 2 | Lower 95% CI for P1-P2 | Upper 95% CI for P1-P2 | Z-Test | P-value |
| PXG vs P0G | 1204/2120 | 1830/3498 | 0.0448 | 0.0180 | 0.0716 | 3.2635 | 0.0011 |
| (0.5679) | (0.5232) | ||||||
| PXG vs 0XG | 1204/2120 | 2580/7676 | 0.2318 | 0.2082 | 0.2554 | 19.4049 | <0.0001 |
| (0.5679) | (0.3361) | ||||||
| P0G vs 0XG | 1830/3498 (0.5232) | 2580/7676 (0.3361) | 0.1870 | 0.1674 | 0.2067 | 18.7587 | <0.0001 |
| Groups | |
| PXE | Pneumonia with diabetes (type I & II) ≥ 65 |
| P0E | Pneumonia without diabetes (type I & II) ≥ 65 |
| 0XE | Diabetes (type I & II) without pneumonia ≥ 65 |
| PXA | Pneumonia with diabetes (type I & II) < 65 |
| P0A | Pneumonia without diabetes (type I & II) < 65 |
| 0XA | Diabetes (type I & II) without pneumonia < 65 |
| Comparison | LOS Sample 1 | LOS Sample 2 | Sample 1 vs Sample 2 | Lower 95% CI for S1-S2 | Upper 95% CI for S1-S2 | Z-Test | P-value |
| PXE vs P0E | 778/1380 | 1102/2027 | 0.0201 | - | - | 1.1585 | 0.2466 |
| (0.5638) | (0.5437) | ||||||
| PXE vs 0XE | 778/1380 | 1578/4324 | 0.1988 | 0.1690 | 0.2287 | 13.0608 | <0.0001 |
| (0.5638) | (0.3649) | ||||||
| PXE vs PXA | 778/1380 | 426/740 | 0.0119 | - | - | 0.5276 | 0.5978 |
| (0.5638) | (0.5757) | ||||||
| PXE vs P0A | 778/1380 | 728/1471 | 0.0689 | 0.0323 | 0.1054 | 3.6811 | 0.0002 |
| (0.5638) | (0.4949) | ||||||
| PXE vs 0XA | 778/1380 | 1002/3352 | 0.2648 | 0.2344 | 0.2953 | 17.0936 | <0.0001 |
| (0.5638) | (0.2989) | ||||||
| P0E vs 0XE | 1102/2027 | 1578/4324 | 0.1787 | 0.1527 | 0.2047 | 13.4433 | <0.0001 |
| (0.5437) | (0.3649) | ||||||
| P0E vs PXA | 1102/2027 | 426/740 | 0.0320 | - | - | 1.4990 | 0.1339 |
| (0.5437) | (0.5757) | ||||||
| P0E vs P0A | 1102/2027 | 728/1471 | 0.0488 | 0.0152 | 0.0823 | 2.8502 | 0.0044 |
| (0.5437) | (0.4949) | ||||||
| P0E vs 0XA | 1102/2027 | 1002/3352 | 0.2447 | 0.2181 | 0.2714 | 17.8236 | <0.0001 |
| (0.5437) | (0.2989) | ||||||
| 0XE vs PXA | 1578/4324 | 426/740 | 0.2107 | 0.1723 | 0.2491 | 10.8326 | <0.0001 |
| (0.3649) | (0.5757) | ||||||
| 0XE vs P0A | 1578/4324 | 728/1471 | 0.1300 | 0.1007 | 0.1593 | 8.7965 | <0.0001 |
| (0.3649) | (0.4949) | ||||||
| 0XE vs 0XA | 1578/4324 | 1002/3352 | 0.0660 | 0.0449 | 0.0871 | 6.0726 | <0.0001 |
| (0.3649) | (0.2989) | ||||||
| PXA vs P0A | 426/740 | 728/1471 | 0.0808 | 0.0369 | 0.1246 | 3.5880 | 0.0003 |
| (0.5757) | (0.4949) | ||||||
| PXA vs 0XA | 426/740 | 1002/3352 | 0.2767 | 0.2379 | 0.3156 | 14.2952 | <0.0001 |
| (0.5757) | (0.2989) | ||||||
| P0A vs 0XA | 728/1471 | 1002/3352 | 0.1960 | 0.1661 | 0.2259 | 13.0649 | <0.0001 |
| Groups | |
| PXM | Pneumonia with diabetes (type I & II) male |
| P0M | Pneumonia without diabetes (type I & II) male |
| 0XM | Diabetes (type I & II) without pneumonia male |
| PXF | Pneumonia with diabetes (type I & II) female |
| P0F | Pneumonia without diabetes (type I & II) female |
| 0XF | Diabetes (type I & II) without pneumonia female |
| Comparison | LOS Sample 1 | LOS Sample 2 | Sample 1 vs Sample 2 | Lower 95% CI for S1-S2 | Upper 95% CI for S1-S2 | Z-Test | P-value |
| PXM vs P0M | 664/1169 | 987/1833 | 0.0295 | - | - | 1.5866 | 0.1126 |
| (0.5680) | (0.5385) | ||||||
| PXM vs 0XM | 664/1169 | 1373/4075 | 0.2311 | 0.1992 | 0.2630 | 14.2892 | <0.0001 |
| (0.5680) | (0.3369) | ||||||
| PXM vs PXF | 664/1169 | 540/951 | 0.0002 | - | - | 0.0085 | 0.9932 |
| (0.5680) | (0.5678) | ||||||
| PXM vs P0F | 664/1169 | 843/1665 | 0.0617 | 0.0245 | 0.0989 | 3.2405 | 0.0012 |
| (0.5680) | (0.5063) | ||||||
| PXM vs 0XF | 664/1169 | 1207/3601 | 0.2328 | 0.2005 | 0.2651 | 14.1658 | <0.0001 |
| (0.5680) | (0.3352) | ||||||
| P0M vs 0XM | 987/1833 | 1373/4075 | 0.2015 | 0.1745 | 0.2286 | 14.6304 | <0.0001 |
| (0.5385) | (0.3369) | ||||||
| P0M vs PXF | 987/1833 | 540/951 | 0.0294 | - | - | 1.4764 | 0.1398 |
| (0.5385) | (0.5678) | ||||||
| P0M vs P0F | 987/1833 | 843/1665 | 0.0322 | - | - | 1.9016 | 0.0572 |
| (0.5385) | (0.5063) | ||||||
| P0M vs 0XF | 987/1833 | 1207/3601 | 0.2033 | 0.1757 | 0.2308 | 14.4394 | <0.0001 |
| (0.5385) | (0.3352) | ||||||
| 0XM vs PXF | 1373/4075 | 540/951 | 0.2309 | 0.1962 | 0.2656 | 13.2046 | <0.0001 |
| (0.3369) | (0.5678) | ||||||
| 0XM vs P0F | 1373/4075 | 843/1665 | 0.1694 | 0.1413 | 0.1974 | 11.9611 | <0.0001 |
| (0.3369) | (0.5063) | ||||||
| 0XM vs 0XF | 1373/4075 | 1207/3601 | 0.0017 | - | - | 0.1618 | 0.8715 |
| (0.3369) | (0.3352) | ||||||
| PXF vs P0F | 540/951 | 843/1665 | 0.0615 | 0.0219 | 0.1011 | 3.0319 | 0.0024 |
| (0.5678) | (0.5063) | ||||||
| PXF vs 0XF | 540/951 | 1207/3601 | 0.2326 | 0.1976 | 0.2677 | 13.1212 | <0.0001 |
| (0.5678) | (0.3352) | ||||||
| P0F vs 0XF | 843/1665 | 1207/3601 | 0.1711 | 0.1426 | 0.1997 | 11.8421 | <0.0001 |
| (0.5063) | (0.3352) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHyperglycemia and glycemic control in critically ill and hospitalized patients · Pneumonia and Respiratory Infections · Nosocomial Infections in ICU
Introduction
Diabetes Mellitus (DM) and pneumonia are both major contributors to healthcare spending and utilization, morbidity and mortality in the United States. DM, a chronic disorder of insulin production or resistance, affects tens of millions of Americans and was responsible for over 100,000 deaths in 2022 alone, ranking as the eighth leading cause of death nationally [1,2]. Beyond its direct complications on glucose regulation, DM increases the risk of infections, cardiovascular disease, renal impairment, and a wide range of other conditions, placing a substantial strain on healthcare resources.
Pneumonia, an infection of the lung parenchyma by bacteria, viruses, or fungi, accounts for over one million hospitalizations and over 50,000 deaths per year in the US [3,4]. Both DM and pneumonia have been individually associated with longer hospital stays and higher healthcare costs, but studies examining the combined effect of these conditions on the duration of inpatient stays are limited [5,6]. Furthermore, there is limited reporting on how patient age or gender may influence the length of stay in patients suffering from both conditions.
The purpose of this retrospective study is to evaluate whether the presence of DM in patients diagnosed with pneumonia is associated with an extended hospital stay, defined as ≥ 6 days, in a patient population from rural Southwest Missouri.
Materials and methods
This retrospective study evaluated the impact of diabetes mellitus (DM), pneumonia, or both on the proportion of patients requiring an extended hospital stay, defined as ≥ 6 days. Electronic medical records (EMR) from Freeman Health System, encompassing two hospitals in southwest Missouri, were reviewed for admissions between January 1, 2019, and December 31, 2022. Patients were included if they were ≥ 18 years old at discharge and had at least one documented diagnosis listed in Tables 1-2. Only the first admission per patient was analyzed; patients with prior hospitalizations or without relevant diagnoses were excluded.
Patients were classified into three groups based on ICD-10 codes at admission: (1) PXG - pneumonia with DM, (2) P0G - pneumonia without DM, and (3) 0XG - DM without pneumonia. Admissions with pneumonia prior to the index admission were excluded.
The primary outcome was the proportion of patients in each group with a hospital stay ≥ 6 days. Subgroup analyses evaluated the effects of age (< 65 vs ≥ 65 years) and gender (male vs female) on extended hospitalization rates, with 95% confidence intervals (CIs) calculated for individual proportions and group comparisons. Comparisons of proportions between groups were performed using two-sample z-tests for proportions.
All statistical analyses were performed using Microsoft Excel (Microsoft Corp., Redmond, WA). P-values were reported to 15 decimal places and rounded to four decimal places for readability. All formulas utilized for the analysis were independently verified by the study statistician. Two-sample proportion z-tests were performed to compare group differences in the proportion of extended hospital stays. Statistical significance was defined as a two-tailed p-value < 0.05, with 95% confidence intervals reported for all estimates.
ICD-10 Codes Utilized in Screening Process
The ICD-10 codes that qualified patients as having met the inclusion criteria for a diagnosis of pneumonia or DM, respectively (Table 1-2).
Results
Screening Processes
To examine the relationship that a diagnosis of pneumonia, DM, or a combination of both has with the proportion of patients requiring an extended hospital stay, patient admissions data were first screened for an ICD-10 code for pneumonia. As demonstrated in Figure 1, 6,672 patient charts were found to have an ICD-10 code for pneumonia (Table 1) at the time of admission. Of these, 1,054 were determined to be a prior admission and were excluded from the analysis. The remaining 5,618 patient admissions were then screened for the presence of an ICD-10 code for DM. This search yielded 2,120 patient admissions with ICD-10 codes for both diseases (PXG group) and 3,498 patient admissions with a diagnosis of pneumonia that did not have a diagnosis of DM (P0G group).
Flow chart demonstrating the inclusion and exclusion criteria for patients admitted with a diagnosis of pneumonia and with a diagnosis of diabetes.
Next, to investigate the relationship between the diagnosis of DM and the proportion of patients requiring an extended hospital stay, patient admissions without the presence of an ICD-10 code for pneumonia were analyzed for a subsequent ICD-10 code for DM. As shown in Figure 2, 40,537 admissions without an ICD-10 code for pneumonia were included in the initial screening. Of these, 5,973 were excluded for the presence of a prior admission for pneumonia. From the remaining 34,564 admissions, 22,557 were found to lack an ICD-10 code for DM, and 4,331 were prior hospital admissions and were also excluded. This yielded 7,676 patient admissions without an ICD-10 code for pneumonia, or prior admission for pneumonia, who had an ICD-10 code for DM (0XG group).
Flow chart demonstrating the inclusion and exclusion criteria for patients admitted without a diagnosis of pneumonia and with a diagnosis of diabetes.
Analysis
As described in the previous section, patients were placed into one of three groups to determine the correlation of pneumonia, DM, or a combination of the two diagnoses on the proportion of patients requiring an extended hospital stay, defined as ≥6 days. A description and quantity of patients in each of these groups can be found in Table 3.
Individual sample proportions were compared to determine the number of patients in each group requiring an extended hospital stay. As demonstrated 1,204 of 2,120 patients in the PXG group (57%, 95% CI 55-59%) and 1,830 of 3,498 patients in the P0G group (52%, 95% CI 51-54%) required an extended stay, while 2,580 of 7,676 patients in the 0XG group (34%, 95% CI 33-35%) required an extended stay (Figure 3).
95% Confidence Intervals for the proportion of patients in each group requiring an extended stay.PXG: Pneumonia with DM; P0G: Pneumonia without DM; 0XG: DM without pneumonia; LOS: Length of stay
Two-sample proportion tests were then performed to assess the association between pneumonia and/or DM and the likelihood of an extended hospital stay. As shown in Table 4, the proportion of patients requiring an extended stay was slightly but significantly higher in the PXG group compared to the P0G group (95% CI 2-7%, p = 0.0011). Comparing the P0G group to the 0XG group, the difference in proportions was larger and also significant (95% CI 17-21%, p < 0.0001). Finally, the largest difference was observed between the PXG and 0XG groups, with a significantly higher percentage of PXG patients requiring an extended stay compared to 0XG patients (95% CI 21-26%, p < 0.0001).
Age Analysis
Of the 13,294 patients included in this review, 7,731 (58.15%) were elderly (defined as age ≥ 65 years old). An analysis was carried out to determine if age was a driving factor for increasing the proportion of patients requiring an extended hospital stay in the population analyzed. As demonstrated in Table 5, each group from the original analysis was further divided based on patient age. Subgroups ending with an ‘E’ represent the population of patients ≥ 65 years old in each group (elderly), while subgroups ending with ‘A’ represent the population of patients < 65 years old in each group (adult).
Individual sample proportions with 95% confidence intervals (CIs) for patients aged <65 years and ≥ 65 years in each group requiring an extended hospital stay are presented in Figure 4. Among patients aged < 65 years, 778 of 1,380 patients in the PXE group (56%, 95% CI 54-59%) and 1,102 of 2,027 patients in the P0E group (54%, 95% CI 52-57%) required an extended stay, while 1,578 of 4,324 patients in the 0XE group (36%, 95% CI 35-38%) did so. Among patients aged ≥ 65 years, 426 of 740 patients in the PXA group (58%, 95% CI 54-61%) and 728 of 1,471 patients in the P0A group (50%, 95% CI 47-52%) required an extended stay, whereas 1,002 of 3,352 patients in the 0XA group (30%, 95% CI 28-31%) did so. Overall, regardless of age, the presence of pneumonia was associated with a higher proportion of patients requiring an extended hospital stay compared with subgroups without pneumonia.
95% Confidence Intervals for the proportion of patients in each age group requiring an extended stay (E’’: Elderly subgroup, age ≥ 65 ‘A’ suffix: Adult subgroup, age < 65 years old).PXE: Pneumonia with diabetes (type I & II) ≥ 65; P0E: Pneumonia without diabetes (type I & II) ≥ 65; 0XE: Diabetes (type I & II) without pneumonia ≥ 65: PXA: Pneumonia with diabetes (type I & II) < 65; P0A: Pneumonia without diabetes (type I & II) < 65; 0XA: Diabetes (type I & II) without pneumonia < 65.
Two-sample proportion tests were conducted to determine the effect of age on the proportion of patients requiring an extended hospital stay in each subgroup. Among patients aged < 65 years, 778 of 1,380 PXE patients (56%, 95% CI 54-59%) and 1,102 of 2,027 P0E patients (54%, 95% CI 52-57%) had a significantly higher proportion of extended stays compared to 1,578 of 4,324 0XE patients (36%, 95% CI 35-38%) (PXE vs 0XE: difference 20%, 95% CI 17-23%, p < 0.0001; P0E vs 0XE: difference 18%, 95% CI 15-20%, p < 0.0001). There was no significant difference between the PXE and P0E subgroups (difference 2%, p = 0.2466).
Among patients aged ≥ 65 years, 426 of 740 PXA patients (58%, 95% CI 54-61%) and 728 of 1,471 P0A patients (50%, 95% CI 47-52%) had a significantly higher proportion of extended stays compared to 1,002 of 3,352 0XA patients (30%, 95% CI 28-31%) (PXA vs 0XA: difference 28%, 95% CI 24-32%, p < 0.0001; P0A vs 0XA: difference 20%, 95% CI 17-23%, p < 0.0001). Additionally, a small but statistically significant difference was observed between PXA and P0A (difference 8%, 95% CI 4-12%, p = 0.0003).
Comparisons across age groups were also performed. PXE (age ≥ 65, pneumonia with DM) vs PXA (age < 65, pneumonia with DM) showed no significant difference (difference 1%, p = 0.5978). PXE vs P0A (age < 65, pneumonia without DM) showed a small but significant difference (7%, 95% CI 3-11%, p = 0.0002), and PXE vs 0XA (age < 65, DM without pneumonia) showed a larger significant difference (26%, 95% CI 23-30%, p < 0.0001).
For patients with pneumonia without DM ≥ 65 (P0E), comparisons to other subgroups showed no significant difference with PXA (difference 3%, p = 0.1339), but a small yet significant difference compared to P0A (difference 5%, 95% CI 2-8%, p = 0.0044) and a larger significant difference compared to 0XA (difference 24%, 95% CI 22-27%, p < 0.0001).
Finally, for patients with DM without pneumonia ≥ 65 (0XE), significantly higher proportions of extended stays were observed when compared to PXA, P0A, and 0XA subgroups (differences 21%, 95% CI 17-25%; 13%, 95% CI 10-16%; 7%, 95% CI 5-9%; p < 0.0001 for all). A summary of all subgroup comparisons is provided in Table 6.
Table 6: 95% Confidence Intervals for group comparisons (‘-’ indicates that no significant difference was detected; therefore, population parameters may or may not be the same.)PXE: Pneumonia with diabetes (type I & II) ≥ 65; P0E: Pneumonia without diabetes (type I & II) ≥ 65; 0XE: Diabetes (type I & II) without pneumonia ≥ 65: PXA: Pneumonia with diabetes (type I & II) < 65; P0A: Pneumonia without diabetes (type I & II) < 65; 0XA: Diabetes (type I & II) without pneumonia < 65.
Gender Analysis
The final variable analyzed for an association with an increased proportion of patients requiring an extended stay was patient gender. Of the patient population utilized for this analysis, 53.23% were male, and 46.77% were female. Table 7 outlines the subgroup designations when patients were further divided based on gender.
Individual sample proportions with 95% confidence intervals (CIs) were also calculated for male and female patients in each group requiring an extended hospital stay. Among male patients, 664 of 1,169 PXM patients (57%, 95% CI 54-60%) and 987 of 1,833 P0M patients (54%, 95% CI 52-56%) required an extended stay, compared to 1,373 of 4,075 0XM patients (34%, 95% CI 32-35%). Among female patients, 540 of 951 PXF patients (57%, 95% CI 54-60%) and 843 of 1,665 P0F patients (51%, 95% CI 48-53%) required an extended stay, compared to 1,207 of 3,601 0XF patients (34%, 95% CI 32-35%). Overall, pneumonia was associated with a higher proportion of patients requiring extended hospitalization regardless of gender. A summary of these findings is demonstrated in Figure 5.
95% Confidence Intervals for individual groups based on gender.PXM: Pneumonia with diabetes (type I & II) male; P0M: Pneumonia without diabetes (type I & II) male; 0XM Diabetes (type I & II) without pneumonia male; PXF: Pneumonia with diabetes (type I & II) female; P0F: Pneumonia without diabetes (type I & II) female; 0XF: Diabetes (type I & II) without pneumonia female
Two-sample proportion tests were conducted to evaluate gender-specific differences. Among males, both PXM and P0M subgroups had a significantly higher proportion of extended stays compared to 0XM (PXM vs 0XM: difference 23%, 95% CI 20-26%, p < 0.0001; P0M vs 0XM: difference 20%, 95% CI 17-23%, p < 0.0001), while no significant difference was observed between PXM and P0M (difference 3%, p = 0.1126). Among females, both PXF and P0F had a significantly higher proportion of extended stays compared to 0XF (PXF vs 0XF: difference 23%, 95% CI 20-27%, p < 0.0001; P0F vs 0XF: difference 17%, 95% CI 14-20%, p < 0.0001). Unlike males, a small but significant difference was observed between PXF and P0F (difference 6%, 95% CI 2-10%, p = 0.0024).
Comparisons across genders revealed no significant difference between PXM and PXF (difference 0%, p = 0.9932). However, PXM had a slightly higher proportion of extended stays compared to P0F (difference 6%, 95% CI 2-10%, p = 0.0012) and a significantly higher proportion compared to 0XF (difference 23%, 95% CI 20-27%, p < 0.0001). P0M did not differ significantly from PXF or P0F (differences 3%, p = 0.1398 and 3%, p = 0.0572, respectively) but had a significantly higher proportion compared to 0XF (difference 20%, 95% CI 18-23%, p < 0.0001).
Finally, 0XM had significantly higher proportions of extended stays compared to PXF and P0F (differences 23%, 95% CI 20-27% and 17%, 95% CI 14-20%, p < 0.0001 for both), but no significant difference was observed compared to 0XF (difference 0%, p = 0.8715). A summary of all gender-based comparisons is provided in Table 8.
Discussion
This study demonstrates that the coexistence of diabetes mellitus (DM) and pneumonia is associated with a higher likelihood of prolonged hospitalization (greater than or equal to six days) when compared with either condition alone. Patients with both DM and pneumonia had a 56.79% probability of requiring an extended length of stay, compared with 52.23% for pneumonia alone and 33.61% for DM alone. These findings align with prior literature showing that both conditions independently contribute to increased duration of hospitalization and increased risk of complications, suggesting a synergistic effect in patients with both diagnoses.
Previous studies have demonstrated that pneumonia is a stronger driver of prolonged hospitalization compared to DM alone. Bader et al. reported that patients hospitalized with community-acquired pneumonia (CAP) experienced significantly longer lengths of stay in comparison to those admitted for DM without pneumonia, highlighting pneumonia as the primary determinant of hospitalization duration [7]. In contrast, Valent et al. showed that DM is independently associated with increased length of stay and in-hospital mortality, even in the absence of pneumonia, underscoring its role as a meaningful comorbidity rather than a dominant driver [8]. Subsequent cohort studies have further reported that patients with both DM and pneumonia experience longer hospitalizations than those with pneumonia alone, suggesting a synergistic effect on disease severity and recovery [9-11]. Notably, many of these prior analyses did not adjust for age or gender, variables that are known to influence hospitalization patterns and overall outcomes, limiting direct comparisons across patient subgroups and motivating the stratified approach used in this analysis.
This study extends this literature by explicitly examining age and gender as both independent variables and in combination with disease status. When stratified by age, patients aged 65 years or older with either DM or pneumonia alone demonstrated a higher proportion of extended hospital stays, consistent with prior reporting that advanced age is a determinant of pneumonia severity and recovery [11]. However, in patients with both DM and pneumonia, the proportion of extended stays was similar across age groups, suggesting that the combined disease burden may attenuate age-related differences in hospitalization duration. In contrast, no statistically significant differences in the proportion of patients requiring an extended stay were observed between genders, either as a standalone variable or when stratified by disease status.
Consistent with prior observational studies, pneumonia emerged as the strongest predictor of extended hospitalization, with 52.23% of patients experiencing a length of stay greater than or equal to six days compared with 33.61% of patients with DM alone. However, the presence of concomitant DM significantly increased the proportion of extended stays among patients with pneumonia to 56.79%, supporting the notion of a synergistic effect. These findings align with broader consensus data demonstrating modest but clinically meaningful increases in length of stay among patients hospitalized with pneumonia, potentially mediated by metabolic dysregulation and impaired immune responses.
This study has several strengths, including a large sample size, the use of real-world clinical data from multiple hospitals, and stratified analyses by age and gender that provide additional context for interpreting the relationship between pneumonia, diabetes, and extended duration of hospital stay.
This study has several limitations. First, we did not differentiate between type I DM and type II DM or assess glycemic control using POC glucose trends or hemoglobin A1c, both of which have been associated with pneumonia outcomes [12,13]. Additionally, potential confounders, such as obesity, were not included and may independently influence hospitalization duration. Due to the retrospective nature of the study, informed consent was not required for the analysis of previously attained patient data, and the sample was not chosen at random. It is unable to be determined if the sample analyzed is representative of the general population. Future studies incorporating these variables in a broader population may further clarify the mechanisms underlying prolonged length of stay in this patient population. Finally, the statistical analyses relied on two-sample proportion tests, which assume independence of observations and adequate sample sizes for normal approximation. Although the large cohort supports these assumptions, unmeasured confounders inherent to retrospective datasets may still influence the observed associations.
Conclusions
Overall, this study demonstrates that pneumonia is a stronger driver of prolonged hospitalization than DM alone, but that the coexistence of DM significantly increases the proportion of patients requiring an extended length of stay, regardless of age or gender. These findings are consistent with existing literature showing that DM modestly but meaningfully prolongs hospitalization in patients with pneumonia and may compound disease severity, potentially through impaired metabolic and immunologic mechanisms. Future studies incorporating DM subtype, glycemic control metrics, and additional comorbidities such as obesity may further clarify the pathways through which DM influences hospital length of stay and patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diabetes Sapra A Bhandari P Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 551501/
- 2Diabetes Published April 27 8 2025 2024 https://www.cdc.gov/nchs/fastats/diabetes.htm
- 3Pneumonia Published March 24 8 2025 National Heart Lung and Blood Institute 2022 https://www.nhlbi.nih.gov/health/pneumonia
- 4Five facts you should know about pneumonia 8 2025 2024 https://www.lung.org/lung-health-diseases/lung-disease-lookup/pneumonia/five-facts-you-should-know
- 5Pneumonia Published 8 2025 2019 https://www.hopkinsmedicine.org/health/conditions-and-diseases/pneumonia
- 6Diabetes mellitus-related hospital admissions and prescriptions of antidiabetic agents in England and Wales: An ecological study BMC Endocr Disord Abu Hammad GA Naser AY Hassouneh LK 1022320233714960410.1186/s 12902-023-01352-z PMC 10163802 · doi ↗ · pubmed ↗
- 7Community-acquired pneumonia in patients with diabetes mellitus: Predictors of complications and length of hospital stay Am J Med Sci Bader MS Yi Y Abouchehade K Haroon B Bishop LD Hawboldt J 303535220162743203210.1016/j.amjms.2016.02.032 · doi ↗ · pubmed ↗
- 8Does diabetes mellitus comorbidity affect in-hospital mortality and length of stay? Analysis of administrative data in an Italian Academic Hospital Acta Diabetol Valent F Tonutti L Grimaldi F 108110905420172891693610.1007/s 00592-017-1050-6 · doi ↗ · pubmed ↗