PAINscape—Exploring patient experiences with ketamine for chronic neuropathic pain: A qualitative study
Nandana Parakh, Danielle Lessor, Kevin Dang, Paul Ritvo, Duminda N. Wijeysundera, Victoria Tucci, Mariela Leda, Mindy Lu, Gabriella Mattina, Janneth Pazmino-Canizares, Zaaria Thomas, Roshni Nayar, John G. Hanlon, Sérgio M. Pereira, Karim S. Ladha, Hance Clarke, Sakina J. Rizvi

TL;DR
This study explores how patients with chronic neuropathic pain experience ketamine treatment, highlighting benefits and challenges in accessing this therapy.
Contribution
The study provides novel qualitative insights into patient experiences with ketamine for chronic neuropathic pain and identifies barriers and facilitators to treatment access.
Findings
All participants reported decreased pain intensity and improved functionality after ketamine treatment.
Barriers included fragmented health systems, long wait times, and lack of pain validation by healthcare providers.
Facilitators included supportive healthcare providers and a safe treatment environment.
Abstract
Chronic pain affects approximately 8 million Canadians annually and is defined by persistent pain lasting over 3 months. Ketamine is an anesthetic drug used to treat chronic neuropathic pain, a subset of chronic pain. To better understand ketamine’s therapeutic benefits and feasibility as a treatment for chronic neuropathic pain, it is important to characterize patient experiences and perspectives with ketamine, as well as barriers and facilitators to accessing this treatment. Thirteen participants were recruited from the chronic pain ketamine infusion program at St. Michael’s Hospital in Toronto, Canada. Each participant completed a survey that captured demographic information and chronic pain features, followed by a semistructured interview. Interview data were analyzed, and themes were generated using content analysis. All participants described decreased pain intensity and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
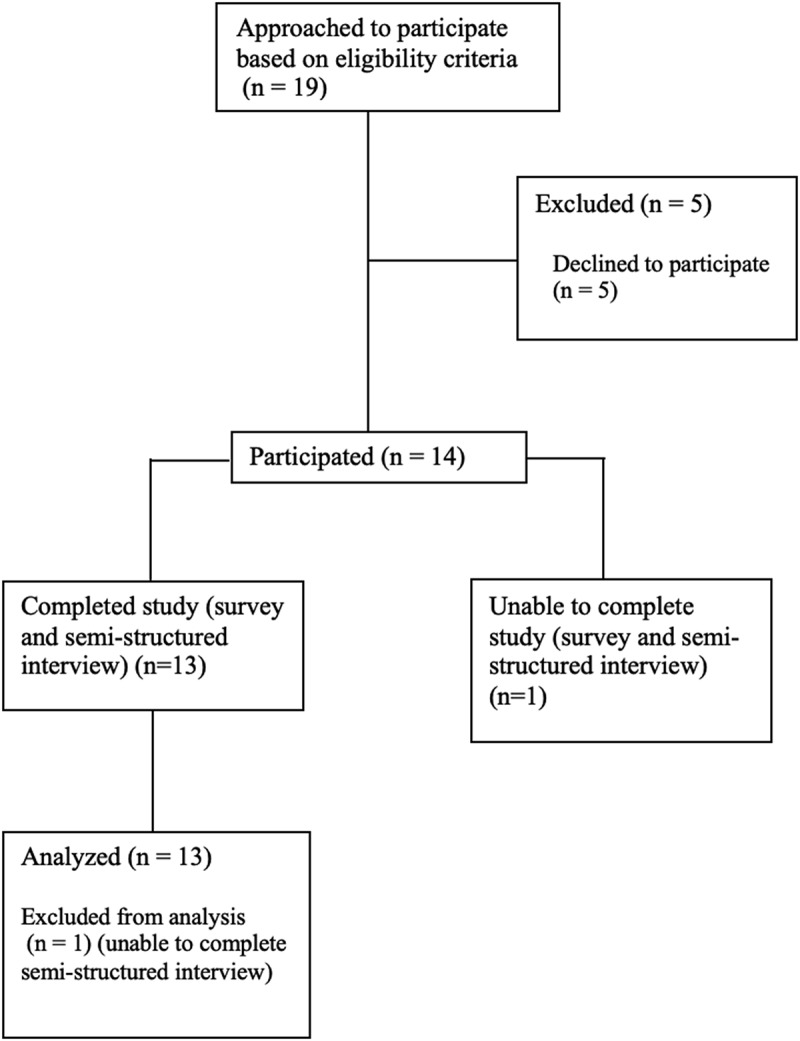 Figure 1
Figure 1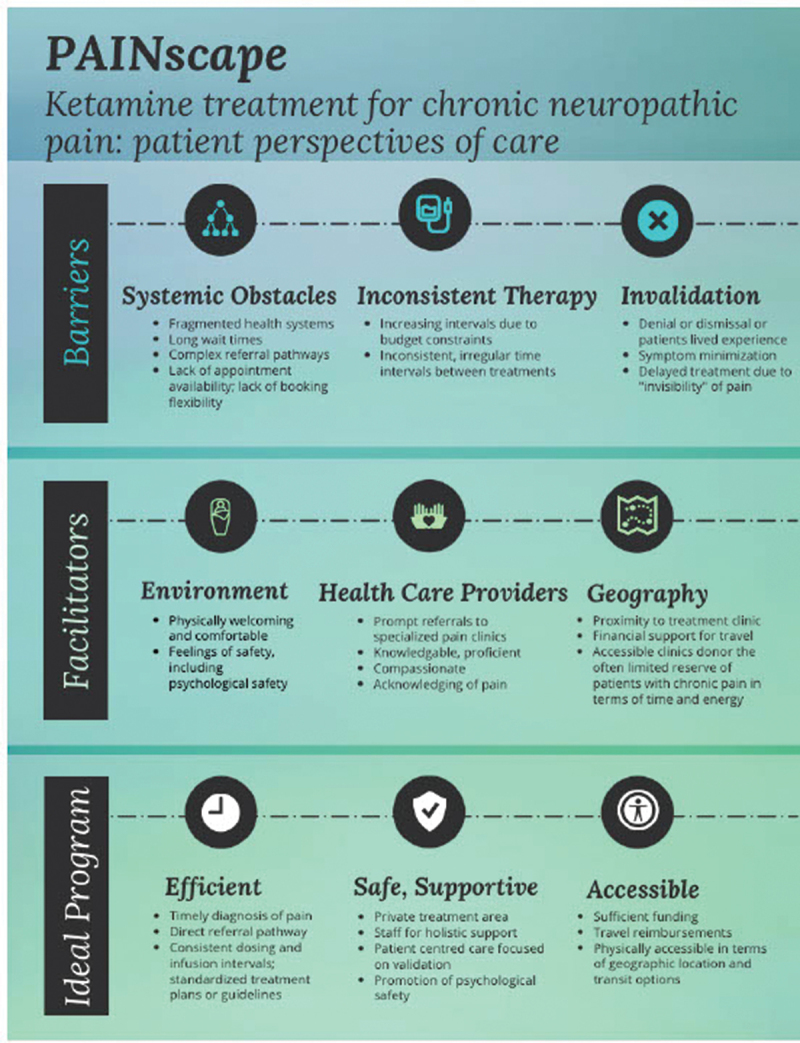 Figure 2
Figure 2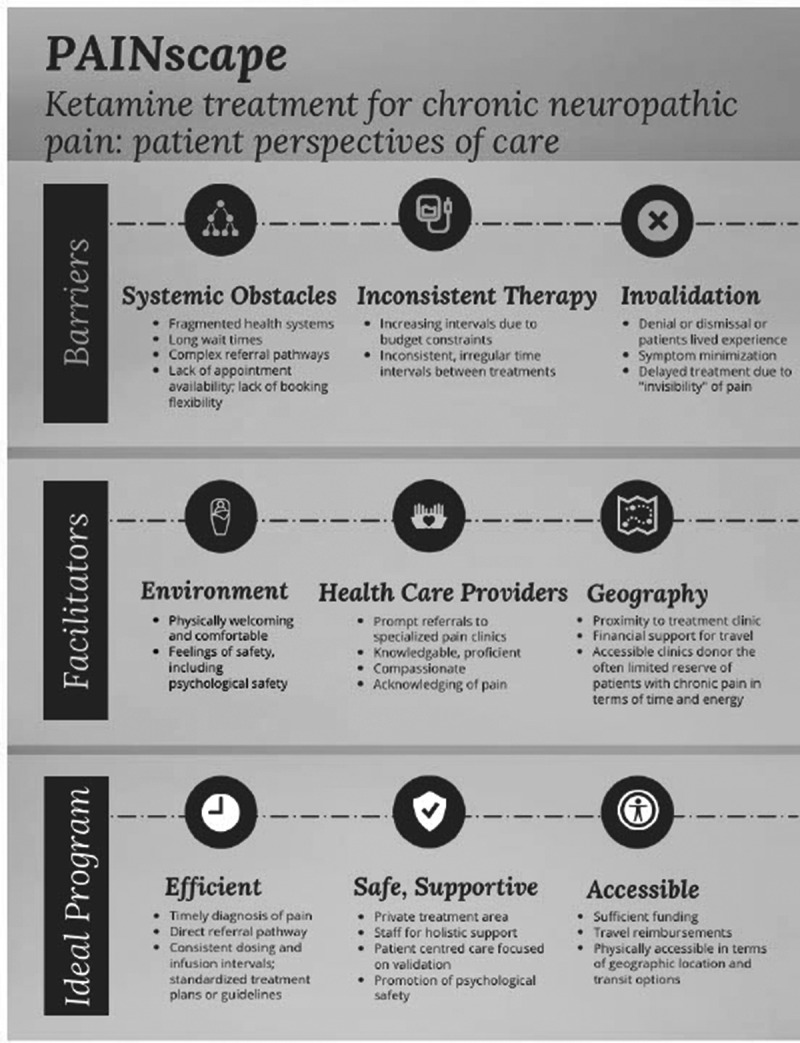 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTreatment of Major Depression · Opioid Use Disorder Treatment · Anesthesia and Neurotoxicity Research
Introduction
Chronic pain is defined as pain persisting for more than 3 months and affects approximately 8 million Canadians a year.^1^ Chronic neuropathic pain (CNP) is a subset of chronic pain caused by injury to or disease of the somatosensory nervous system.^2,3^ This pain is often characterized by sensations of burning, shooting, stabbing, and electrical shocks, but other sensations can also occur.^2,3^ Chronic pain can have a variety of physical, social, functional, and economic impacts, leading to increased rates of comorbidities such as depression, diabetes, and heart disease, along with poorer quality of life, limited mobility, and decreased physical activity.^4^ The economic burden of chronic pain is significant, with total direct and indirect costs in Canada in 2019 estimated between 40.3 billion.^1^
The urgent need for more effective, feasible, and accessible treatments has increased the interest in ketamine, an anesthetic drug with multiple uses including the treatment of CNP.^5,6^ Ketamine was first approved for in-hospital use in 1970.^7^ It is a noncompetitive antagonist at the phencyclidine binding site of the N-methyl-d-aspartate central nervous system receptors.^4^ Ketamine has been proven to have psychomimetic, antidepressant, and, importantly, analgesic effects.^4,8^ Quantitative research demonstrates evidence of short-term pain relief of CNP with ketamine infusions.^9^ Much of the literature on ketamine has focused on its effects on treatment-resistant depression, with limited qualitative research on its application in treating CNP.^10^ Furthermore, there is a lack of understanding around patient experiences regarding the administration of ketamine for CNP, which could impact the way ketamine is prescribed and utilized for pain.
This qualitative study explored patients’ experiences and perceived impacts of ketamine treatment in their management of CNP. Our ketamine infusion program is funded through the Ontario Health Insurance Plan. There are no out-of-pocket expenses for patients. Our goal was to better understand patient-reported barriers to the treatment of CNP and factors influencing health care availability for this patient population. Additionally, we sought to understand factors that facilitated access to treatments for CNP to inform future directions of patient-centered chronic pain care. Lastly, we wanted to examine various systemic and patient- level determinants of engaging in ketamine treatment, to better understand motivations for trialing ketamine, and factors that may hinder the acceptance of this treatment. By exploring patient perspectives around ketamine, as well as its accessibility and impact, we aim to improve access to treatments for CNP.
Methods
Study design
Ethics approval was obtained from the Unity Health Research Ethics Board (REB) prior to beginning the study (Ethics Approval Number REB 20-113). Prior to patient participation in the study, both verbal and written informed consent were obtained.
We adopted a qualitative descriptive study design to explore patient experiences with ketamine infusion therapy for CNP. Qualitative descriptive methods are widely utilized in health care research, particularly in areas where evidence is limited, to delve into lived experiences and to address critical clinical, service, and policy challenges.^11^ This approach acknowledges the subjective and diverse nature of individual experiences, grounding our findings in the real-world challenges and perspectives of participants.
Participant selection
Participants were recruited from the chronic pain clinic at St. Michael’s Hospital in Toronto, Canada. The selected participants included all participants presenting to the clinic for a ketamine infusion for pharmacological pain management between July 23, 2024, and August 13, 2024, on the days the researchers visited. Participants who were 18 years or older, diagnosed with CNP (>3 months), receiving in-person ketamine infusions for pharmacological pain management, and able to complete both the survey and semistructured interview were included in the study. Participants had to have received at least one ketamine infusion to participate in the study. Patients not receiving ketamine infusions and those who did not possess sufficient communication abilities in the English language were excluded. Nineteen participants were approached based on eligibility criteria, and 14 participants elected to participate in the study. One participant was unable to complete the interview and was subsequently excluded from the study. Please see Figure 1 for a flow diagram of participant recruitment. Figure 1.Flow diagram for participant recruitment.
Data generation
A data analysis and statistical plan was written and filed with our institutional review board before data were accessed. A survey was administered to collect demographic information and baseline treatment-related factors specific to their CNP. The survey included multiple-choice questions, binary responses (e.g., yes or no), and short-answer questions (Appendix A). Upon completing the survey, participants took part in a semistructured interview designed to explore their experiences with CNP and the barriers and facilitators associated with ketamine infusions (Appendix B). A semistructured interview approach was chosen for its flexible format, which allowed for the collection of open-ended data and a deeper understanding of participants’ perspectives.^12^ All interviews were conducted in English and held in person at the St. Michael’s Hospital chronic pain clinic.
Survey responses and audio recordings were securely stored on a password protected hospital server. Survey responses and interview transcripts were deidentified and labeled with an alphanumeric code.
Data analysis
The interviews were conducted, audio-recorded, and transcribed by the lead author (N.P.), who also ensured the removal of identifiable information to protect participants’ privacy. Transcripts were uploaded to NVivo 12 software to facilitate systematic data organization and analysis.^13^
Thematic saturation of the data was continually evaluated. Based on the protocol, we targeted a minimum sample size of 12 participants. Once reaching 12 participants, transcripts were analyzed, at which point it was determined that thematic saturation had been reached. We completed one more interview to ensure full thematic saturation.
Employing content analysis, N.P. and A.G. engaged in multiple readings of the transcripts to ensure a comprehensive understanding of the data.^14^ N.P. developed an initial coding framework by analyzing a subset of four transcripts, which guided the coding process, through an inductive framework. This framework was iteratively refined as additional transcripts were analyzed, resulting in the creation of a detailed codebook containing code names, definitions, and example data. To ensure consistency and reliability, a second round of coding was conducted across all transcripts. Once data coding was completed, major themes were identified and reviewed in relation to coded extracts to ensure they reflected participants’ voices.
Results
Survey results
A total of 13 individuals participated in the study, at which point it was determined that thematic saturation had been reached.^15,16^ Participants ranged in age from 23 to 74. The sample for this study was notably well-educated, with the majority of participants having attained higher levels of formal education. Nearly half of participants completed graduate school (46%), and an additional five completed postsecondary education (38%), collectively accounting for 84% of the sample. Full participant characteristics are reported in Table 1.Table 1.Participant demographic characteristics.CharacteristicParticipants (n = 13)Age 18–30431–60561–804Assigned sex at birth Male3Female10Gender (open-text response) Woman3Female6Male3Did not answer1Ethnicity European7First Nations, Inuit, and Métis1Middle Eastern1Other3Prefer not to answer1Educational attainment Grade/high school (1–12)2Postsecondary (13–16)5Graduate school (17–20+)6Employment status Employed4Retired4Student2Unable to work2Did not answer1
With respect to chronic pain characteristics, eight participants reported experiencing chronic pain for 1 to 10 years (62%), two for 11 to 20 years (15%), and three for 21 to 30 years (23%). The number of ketamine infusions varied from 1 to 40 infusions over their lifetime. Participants also reported other medications they use for chronic pain, such as selective serotonin reuptake inhibitors (SSRIs), serotonin–norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), opioids, and gabapentinoids. Full chronic pain characteristics are reported in Table 2.Table 2.Chronic pain characteristics.CharacteristicParticipants (n = 13)Length of chronic pain diagnosis 1–10 years811–20 years221–30 years3Pain severity 0–314–788–104Little interest or pleasure in doing things over the last 2 weeks Not at all3Several days6More than half the days3Nearly every day1Feeling down, depressed, or hopeless in the last 2 weeks Not at all5Several days6More than half the days1Nearly every day1Number of ketamine infusions 1–10511–20321–30231–402Multiple1Other medications for chronic pain SSRIs (i.e., sertraline, paroxetine, fluoxetine)7SNRIs (i.e., venlafaxine, duloxetine)6TCAs (i.e., amitriptyline, imipramine, nortriptyline)5Opioids (i.e., morphine, oxycodone, codeine, etc.)8Gabapentinoid (i.e., gabapentin, pregabalin)7Other5Other treatments for chronic pain Yes6No7Treatments for depression–Past Yes6No7Treatments for depression–Present Yes5No8
Semistructured interview results
We identified three overarching themes from the semistructured interviews: (1) impact of ketamine on pain, (2) barriers to accessing pain relief, and (3) facilitators to chronic pain treatment. A brief overview of each theme along with sample illustrative quotes is provided below, followed by a more detailed reporting of results and quotes in Appendix C.
Though the degree and consistency of pain relief varied among participants and across individual infusion experiences, all participants reported that ketamine significantly reduced pain and improved their quality of life (100%). Ketamine had not only a physical impact but a profound mental and emotional impact on participants. Most participants described their CNP as profound and life-altering, with some expressing that its intensity left them yearning for an escape, even through death, to find relief. Ketamine infusions helped reduce the pervasive fear associated with CNP and helped to restore a sense of self and agency. Many participants also noted that ketamine infusions allowed a return to daily activities and overall contributed to improved quality of life. Table 3 provides sample illustrative quotes.Table 3.Sample illustrative quotes around impact of ketamine on pain.Participant IDParticipant quotesPID 002“Well probably the most significant thing with the ketamine infusions that I was living with soul-destroying pain. It was ruining my life to the point that I didn’t want to go on living. The ketamine has resolved the pain issue, it’s amazing.”PID 003“I’ll feel no pain when I walk out of here. So, there’s an immediate relief in that sense. But the gradual relief, my opinion of ketamine, is more from the mental side. You’re positively thinking about the outlook of your recovery, the trajectory of your recovery.”PID 001“I always just look forward to being able to feel like me again afterwards and being able to do things a little bit more than I can do the last few weeks, and getting back into that.”
Despite the profound relief and renewed functionality that ketamine infusions provided, participants also revealed substantial barriers to accessing this treatment and other essential pain management supports, including, fragmented systems and wait times, infusion interval and inconsistencies, and the struggle for pain validation, which encompasses both a general invalidation of chronic pain, along with a lack of acceptance of ketamine infusions as a viable treatment for CNP. Participants described the arduous task of navigating between multiple clinics and providers, with each step contributing to frustration and delays in receiving essential treatment. Furthermore, many participants stated that infusion intervals had increased due to budget constraints and resource availability (54%), leading to increased pain and decreased quality of life. Lastly, 54% of participants reported that their pain was initially dismissed or undiagnosed. The intangible and often invisible nature of chronic pain, where individuals may appear outwardly “normal” or lack clear indicators of suffering, frequently leads to skepticism or dismissal from health care providers, rendering it difficult to secure needed care. Participants also experienced stigma around utilizing ketamine for pain management. Table 4 provides sample illustrative quotes.Table 4.Sample illustrative quotes around barriers.Participant IDParticipant quotesPID 004“The wait times can be really bad. I think I’ve been to seven different pain clinics for different purposes and each time, its 6 months to a year, if not a year and a half or 2 years, so that’s the biggest [barrier].”PID 010“[Ketamine] lasts around 3-ish weeks, and I would get it every 4 weeks. But now it has to be every 5 to 6 weeks, and that’s sad. I now have to use my wheelchair a lot more, because I’m in too much pain to walk, for the last weeks of it, since it’s been longer.”PID 005“A lot of people, including my pain specialist, did not believe me. That’s the truth.”
Though there were significant barriers to accessing ketamine infusions, participants also spoke about factors that improved their overall experience with ketamine infusions, such as comfortable and supportive environment, support from individual health care providers, and geographical factors. A secure and comfortable environment for participants led to increased feelings of safety and improved the overall treatment experience. Access to health care providers who were inclusive and believed patients about their pain were able to facilitate the entire treatment process. Physical proximity to the infusion centers was also a significant facilitator. Table 5 provides sample illustrative quotes.Table 5.Sample illustrative quotes around facilitators.Participant IDParticipant quotesPID 002“I feel safe, is the other thing. I think safety, feeling safe, is very important.”PID 004“Having a family doctor that acknowledges the chronic pain helps.”PID 012“I live [close], so I’m very close to all the hospitals and all the doctors’ offices, which makes things very easy for me, and am able to take cabs places, so makes things more accessible.”
Additional participant quotes and full semistructured interview results are included in Appendix C.
Discussion
This study explores the experiences of 13 patients receiving ketamine infusions for CNP to better understand the impact of treatment and the barriers and facilitators to treatment access. Our findings can be broken up into three major themes: (1) impact of ketamine on pain, (2) barriers to accessing pain relief, and (3) facilitators to chronic pain treatment.
Positive impact of ketamine on pain
All participants found that ketamine infusions improved both physical and emotional pain, and many found that it transformed their lives. Even though the extent and duration of relief varied, many explained that ketamine helped to transform their lives by alleviating not only the physical pain but also its emotional toll (e.g., the fear of pain). Notably, ketamine helped to restore a sense of self and agency, along with improving participants’ functionality and quality of life. Indeed, even short periods of relief from pain were described as impactful, restoring functionality and enabling a return to daily activities. These findings are concordant with other studies that found that, overall, ketamine leads to clinically significant reductions in chronic pain, which in turn leads to improved functionality and quality of life.^4,5,9,17,18^
Barriers
Participants faced three main barriers. They described how fragmented systems and long wait times produced frustration and delays in achieving pain relief. These problems could be addressed by streamlining pain management systems. One approach to streamlining care involves a multidisciplinary approach to chronic pain management, which incorporates the expertise of both physicians and nonphysicians, along with nonmedical specialists. This approach leads to increased continuity of care, greater psychological advantages, increased pain relief, and improved physical functionality.^19,20^
Another key barrier that was brought up by participants was related to the time interval between ketamine infusions and how it impacted pain relief. Participants often found that the unpredictable intervals between infusions led to pain intensity being perceived as higher because it impacted their expectations of their pain management. Additionally, longer intervals between ketamine infusions due to budget constraints or appointment/resource availability led to poorer pain control. The ketamine infusion rate is patient specific and variable; ketamine treatment programs approach this variability differently. For instance, at the Cleveland Clinic (Ohio), ketamine infusions are given at a rate of 0.5 mg/kg over 40 min, over 5 days. Individuals attend these infusions every 3 to 4 months.^21,22^ Our ketamine infusion program, on the other hand, uses an infusion rate between 0.5 and 1 mg/kg per hour, and the number of hours for the infusion is determined by patient characteristics. Due to the variability in patient preferences regarding how often ketamine infusions are required, the “ideal” interval is patient specific, and further research in this area can help to better explore this. Furthermore, better understanding how to augment the durability of ketamine would be helpful. Other studies are also investigating ketamine-assisted psychotherapy to increase durability and efficacy for chronic pain.^23^ The qualitative work of our study can inform future clinical trials seeking to create more robust and efficacious treatment regimens for chronic pain, because it provides a better understanding of the impact ketamine can have on CNP.
Lastly, participants reported that because pain is complex, subjective, and often stigmatized, they were not always believed about the nature and intensity of their chronic pain in general. Some participants described experiencing pain invalidation and stigma from their health care providers earlier in their care, prior to being referred to specialized pain care. These experiences often delayed referral to pain specialists. Additionally, it often took months and visits to multiple providers to receive an official diagnosis of chronic pain, which led to a more intense perception of pain and negatively impacted pain management. Furthermore, ketamine for CNP is often stigmatized due to its potential for misuse.^24^ Participants reported how popular culture has increased stigma around ketamine and how this led to participants feeling uncomfortable sharing their experiences with ketamine infusions with family members or friends. There is limited research around the stigma associated with ketamine infusions as a treatment for CNP; in contrast, this stigma is better discussed in other domains of ketamine use, such as for treatment-resistant depression.^25,26^ Some authors suggest the need to conduct more research on ketamine to fully elucidate its mechanism of action and address concerns around ketamine’s potential for misuse.^27,28^ Other studies recommend better public education around the use of ketamine for medical conditions, as well as disseminating research around the long-term effects of ketamine.^28^ There is stigma related to ketamine infusions both at the individual patient level and at the health care provider level. It is important to address providers’ beliefs and bias around using ketamine therapeutically.^27,28^ Continued education for health care professionals, along with increased research conducted on the long-term effects of ketamine, can help reduce provider stigma.^29,30^
Facilitators
Participants reported three main facilitators to receiving ketamine for chronic pain. Having a supportive environment in which ketamine was administered was a significant facilitator, because it increased psychological safety. Our approach is to provide a private treatment area where participants receive ketamine infusions with nursing care before, during, and after their infusion. This improves both physical and psychological safety and helps to improve the overall treatment experience. Research asserts that comfort and care in the treatment setting are important institutional factors that improve the overall patient experience.^31,32^ Widely implementing this model of comfort and care during ketamine infusions can have a positive impact on those living with chronic pain.
Furthermore, individual health care providers can have significant impacts on the overall health of a patient; this has been well established in pain management strategies. Provider and patient alignment in terms of their approach to and expectations of pain management can improve patient outcomes.^27,33^ Therefore, enhancing patient–provider communication, in addition to resolving physician bias (which was reported as a barrier above), is paramount in effectively treating CNP.
Lastly, living near ketamine provision centers was a significant facilitator for treatment access, as stated by various participants. Individuals living farther from urban centers, where ketamine infusions for CNP are typically available, have difficulty accessing care, poorer pain control, and increased perception of pain.^34^ It is well established that rural and remote populations experience higher rates of chronic pain, likely reflecting limited access to specialized chronic pain care.^35–37^ Some suggested strategies to address these disparities in care include interventions like mobile ketamine clinics. Currently, mobile ketamine clinics in the United States offer door-to-door treatments for chronic pain and various mental health conditions for those living in remote areas or those with limited mobility.^38^ Further research on this type of treatment can be considered in Canada, in terms of both feasibility and funding. Furthermore, though the current landscape of ketamine treatment requires patients to be physically present, other parts of the process, such as intake and initial appointments, can be streamlined through virtual care.
In addition to the three major themes, we noted the unusually high level of education among the interviewed participants. This may not reflect the broader representation of participants in our clinic because our selected sample was a convenience sample. We approached 19 participants and 5 declined to participate, which limits our ability to compare the education levels of respondents with nonrespondents. Several factors may contribute to why our sample included participants with a high degree of education. Individuals with more education may be better equipped to overcome the various barriers to initiate ketamine infusion treatment. Furthermore, though the treatment is publicly funded at our site through the Ontario Health Insurance Plan, socioeconomic factors may still favor those with more resources, highlighting a need to improve accessibility and reduce structural barriers to access this treatment.
Strengths and limitations
In terms of strengths, this study promotes patient-centered care by qualitatively exploring patient perspectives regarding experiences with chronic pain and ketamine treatment to gain an appreciation for barriers and facilitators to treatment. Though similar qualitative studies have been conducted to examine the impact of ketamine on depression, there is limited qualitative research surrounding the impact of ketamine on CNP, making this study an important contribution to pain medicine scholarship.
Our study is limited in its generalizability by its single-site nature, small number of participants, higher than average education level, and uneven gender ratio. Due to these limitations, we were unable to engage in comparative analysis by demographic variables including social determinants of health. Given what is known about the differences in pain experiences and management between men and women, future research exploring the use of ketamine as a pain management strategy should engage in comparative analysis across demographically diverse participants.
Practical implications
This research has multiple implications for future programmatic development, at both our site and others offering or intending to offer treatment for CNP. Future clinical trials are seeking to create more durable and effective treatment regimens for chronic pain.^23^ Our research can help provide a window into the lived experiences of individuals undergoing ketamine treatment for chronic pain, which can help guide treatment decisions and create more effective programs for managing CNP.
Improving communication strategies between health care providers and patients
Many patients with CNP often feel like their pain is dismissed or invalidated by health care professionals. Strategies to improve communication between health care professionals and those living with chronic pain include providing validation and endorsing belief of the patient, active listening and practicing empathy, being open and nonjudgmental, and providing support while collaborating with the patient.^39^ Henry and Matthias proposed a model that incorporates clinician, interaction, and patient factors into communication and encourages setting visit outcomes that both the clinician and patient can work toward.^40^ It is hoped that implementing these strategies into communicating with our patients at every step of the treatment process will allow patients to feel better supported by health care providers and create a sense of belonging, thus fostering healing.
Ideal ketamine program
An ideal ketamine treatment program should consider patient, clinician, and institutional factors. It is important to note that it is difficult to determine an ideal ketamine infusion interval. Rather, it appears that the ideal interval is patient specific and must be addressed on an individual basis. Figure 2 outlines the general principles that can contribute to creating an efficient, safe, and accessible program for ketamine infusions. Figure 2.An ideal ketamine infusion program: patient preferences.
Conclusion
Chronic pain imposes a significant burden on both individuals living with pain and the health care system. Ketamine has a positive analgesic effect and can significantly relieve pain in those living with CNP. Barriers to ketamine use include long wait times resulting from fragmented health systems, inconsistencies in infusion intervals, accessibility of appointments, difficulty receiving a timely chronic pain diagnosis, and difficulties being believed about chronic pain. Facilitators to ketamine use include a safe and positive treatment environment, support from individual health care providers, and proximity to chronic pain centers. Addressing stigma around CNP and ketamine, along with identifying strategies to provide ketamine to those living at a distance from chronic pain centers, is important in improving the overall ketamine treatment experience. More research is needed to further explore the timing around infusion schedules, along with novel methods for improving ketamine’s durability in treating chronic pain. Overall, these findings will help inform our ongoing work at St. Michael’s Hospital and other pain centers in providing ketamine to improve pain management and quality of life for those with CNP.
Supplementary Material
PAINscape_CJP_Jan 2 2026_Tracked Changes.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Government of Canada. Canadian pain task force report: an action plan for pain in Canada. Ottawa; 2021 May [accessed 2024 Sept 15]. https://www.canada.ca/content/dam/hc-sc/documents/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021-rapport/report-rapport-2021-eng.pdf
- 2Scholz J, Finnerup NB, Attal N, Aziz Q, Baron R, Bennett MI, Benoliel R, Cohen M, Cruccu G, Davis K, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–19. doi:10.1097/j.pain.0000000000001365.30586071 PMC 6310153 · doi ↗ · pubmed ↗
- 3Johannes CB, Le TK, Zhou X, Johnston JA, Dworkin RH. The prevalence of chronic pain in United States adults: sesults of an internet-based survey. J Pain. 2010;11(11):1230–39. doi:10.1016/j.jpain.2010.07.002.20797916 · doi ↗ · pubmed ↗
- 4Cohen SP, Bhatia A, Buvanendran A, Schwenk ES, Wasan AD, Hurley RW, Viscusi ER, Narouze S, Davis FN, Ritchie EC, et al. Consensus guidelines on the use of intravenous ketamine infusions for chronic pain from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):521–46. doi:10.1097/aap.0000000000000808.29870458 PMC 6023575 · doi ↗ · pubmed ↗
- 5Niesters M, Martini C, Dahan A. Ketamine for chronic pain: risks and benefits. Br J Clin Pharmacol. 2014;77(2):357–67. doi:10.1111/bcp.12094.23432384 PMC 4014022 · doi ↗ · pubmed ↗
- 6Buhrman M, Syk M, Burvall O, Hartig T, Gordh T, Andersson G. Individualized guided internet-delivered cognitive-behavior therapy for chronic pain patients with comorbid depression and anxiety: a randomized controlled trial. Clin J Pain. 2015;31(6):504–16. doi:10.1097/AJP.0000000000000176.25380222 · doi ↗ · pubmed ↗
- 7Krupitsky E, Kolp E. Ketamine psychedelic psychotherapy. In: Winkelman MJ, Roberts TB editors. Psychedelic medicine: new evidence for hallucinogenic substances as treatments. Westport (CT): Praeger Publishers/Greenwood Publishing Group; 2007. p. 67–85.
- 8Goldfine CE, Tom JJ, Im DD, Yudkoff B, Anand A, Taylor JJ, Chai PR, Suzuki J. The therapeutic use and efficacy of ketamine in alcohol use disorder and alcohol withdrawal syndrome: a scoping review. Front Psych. 2023;14:1141836. doi:10.3389/fpsyt.2023.1141836.PMC 1017266637181899 · doi ↗ · pubmed ↗