Risk Factors for Anastomotic Stricture and Obstructive Symptoms Following Double‐Flap Technique Reconstruction After Proximal Gastrectomy
Shinji Kuroda, Yoshihiko Kakiuchi, Satoru Kikuchi, Hajime Kashima, Nobuhiko Kanaya, Shunya Hanzawa, Kenjiro Kumano, Masahiko Nishizaki, Shunsuke Kagawa, Toshiyoshi Fujiwara

TL;DR
This study identifies risk factors for anastomotic stricture and obstructive symptoms after a surgical technique used in stomach surgery, offering ways to improve patient outcomes.
Contribution
The study identifies mucosal detachment and continuous suturing as novel risk factors for complications after double-flap technique reconstruction.
Findings
Mucosal detachment of the esophagus is a significant risk factor for anastomotic stricture after DFT reconstruction.
Continuous suturing at the E-S fixation site increases intraluminal pressure and obstructive symptoms.
Thermal damage during surgery may contribute to mucosal detachment and subsequent complications.
Abstract
The double‐flap technique (DFT) is a widely used esophagogastrostomy method after proximal gastrectomy (PG) due to its strong anti‐reflux mechanism. However, anastomotic stricture remains a major concern, leading to obstructive symptoms and impaired postoperative quality of life (QOL). This study aimed to identify risk factors for anastomotic stricture and obstructive symptoms after PG with DFT reconstruction. This single‐center, retrospective study analyzed 77 patients who underwent DFT reconstruction between 2014 and 2022. The impact of technical factors, including suturing methods and mucosal detachment, was evaluated. In addition, intraluminal pressure analysis was performed using ex vivo pig stomach models to assess sites contributing to obstructive symptoms. Anastomotic stricture requiring balloon dilatation occurred in 10 patients (13%), with mucosal detachment of the esophagus…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
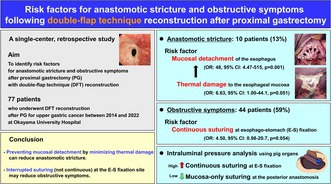 Figure 1
Figure 1 Figure 2
Figure 2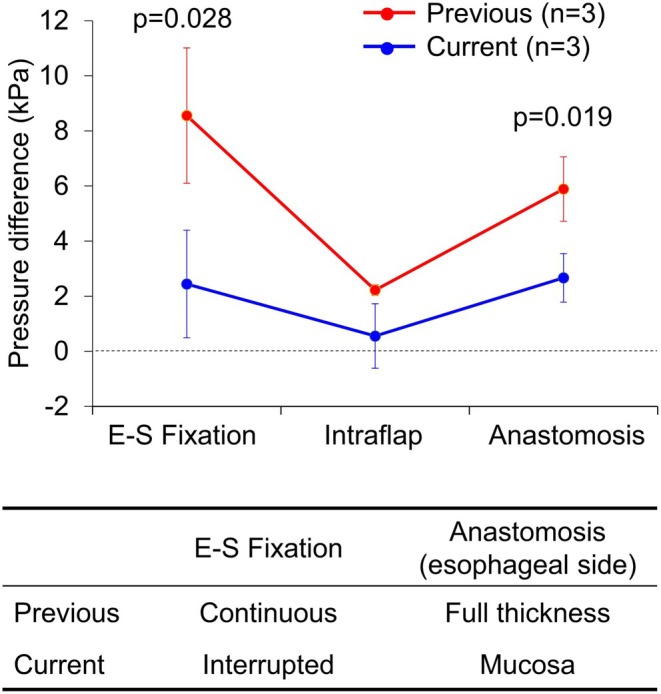 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastric Cancer Management and Outcomes · Bariatric Surgery and Outcomes