Bronchogenic cyst of pancreas: a rare case report
Ruiqi Zou, Yushi Dai, Fuyu Li, Fei Liu, Yixin Lin

TL;DR
This paper reports a rare case of a bronchogenic cyst in the pancreas and emphasizes the importance of surgery for treatment.
Contribution
The contribution is a detailed case report of a rare peri-pancreatic bronchogenic cyst with successful surgical treatment.
Findings
A 21-year-old male was diagnosed with a bronchogenic cyst in the pancreas after imaging and surgery.
Complete surgical resection led to no recurrence over two years.
Radical surgery is recommended for bronchogenic cysts larger than 3 cm or with complications.
Abstract
Bronchogenic cyst is a rare congenital developmental abnormality of the anterior bowel. Peri-pancreatic bronchogenic cyst (PBC) is extremely rare, when only a few cases reported worldwide. Diagnosis of PBC is difficult due to the lack of specific clinical features and symptoms, laboratory and imaging findings. Currently, the diagnosis of PBC mainly relies on the comprehensive judgment of multidisciplinary collaboration, combined with clinical manifestations, imaging features and pathological verification. Most bronchogenic cysts are benign and the long-term survival rate after complete resection is close to 100%. A 21-year-old male with a pancreatic mass was admitted to our hospital. CT scan showed a low-density cystic shadow about 3.6 × 3.5 cm2 on the pancreatic body, with clear boundaries, no enhancement, and no dilation of the main pancreatic duct. The patient underwent open distal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
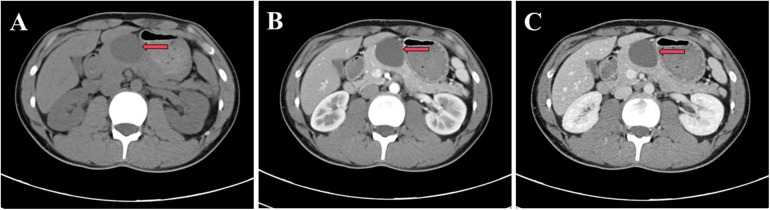 Figure 1
Figure 1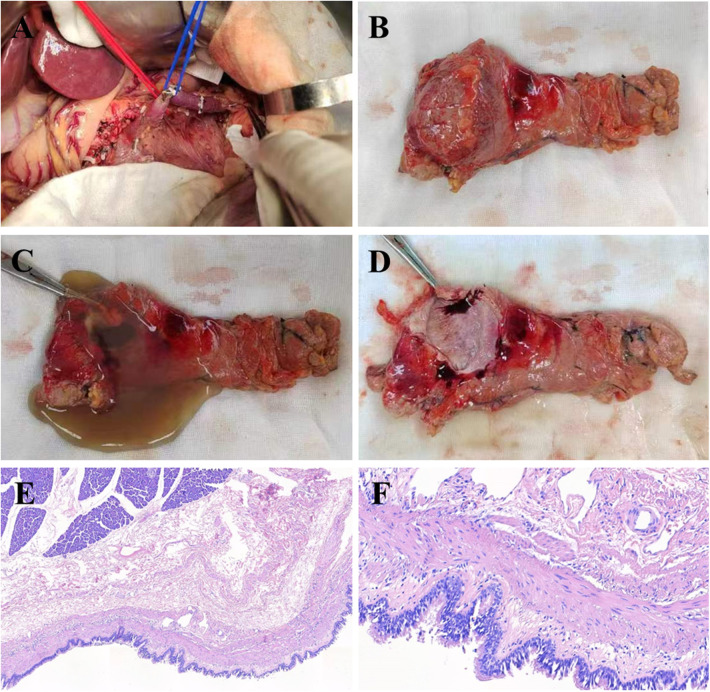 Figure 2
Figure 2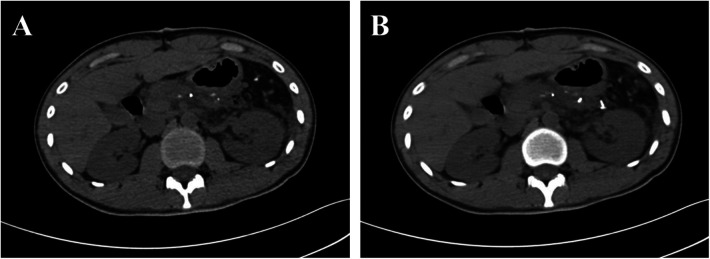 Figure 3
Figure 3| Location | Age (Year) | Sex | Symptom | Size (Maximum diameter) | Intervention | Reference |
|---|---|---|---|---|---|---|
| Head and Neck | ||||||
| Tongue | 5-month | Male | Feeding difficulty | 3.0 cm | Resection | ( |
| Suprasternal fossa | 31 | Female | Asymptomatic | 2.5 cm | Resection | ( |
| Peri-Thyroid | 27 | Female | Hoarseness | 4.0 cm | Resection | ( |
| Peri-Thyroid | 28 | Female | Asymptomatic | 5.0 cm | Resection | ( |
| Thorax | ||||||
| Interatrial septum | 42 | Male | Palpitation | 2.9 cm | Thoracotomy resection | ( |
| Diaphragmatic | 50 | Male | Asymptomatic | 7.0 cm | Thoracotomy resection | ( |
| Posterior mediastinum | 37 | Male | Asymptomatic | 3.7 cm | Thoracoscopic resection | ( |
| Mediastinum | 59 | Male | Dysphagia | 3.0 cm | Thoracoscopic resection | ( |
| Abdomen | ||||||
| Peri-Splenic | 48 | Female | Asymptomatic | 2.6 cm | Laparoscopic resection | ( |
| Peri-Stomach | 21 | Female | Asymptomatic | 6.2 cm | Laparoscopic resection | ( |
| Peri-Hepatic | Not mentioned | Male | Abdominal pain | 8.0 cm | Fenestration drainage | ( |
| Retroperitoneal | 51 | Male | Asymptomatic | 5.9 cm | Laparoscopic resection | ( |
| Others | ||||||
| Intradural extramedullary | 35 | Male | Dysuria | 1.3 cm | Resection | ( |
| Cutaneous of back | 9 | Female | Exudation | Not mentioned | Biopsy | ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyasthenia Gravis and Thymoma · Gastrointestinal disorders and treatments · Cystic Fibrosis Research Advances
Introduction
Bronchogenic cysts are rare congenital abnormalities of foregut development that originate from lung buds and are present at birth (1). While most commonly located in the mediastinum, these cysts can also manifest in other locations, including the diaphragm, abdominal cavity, and subcutaneous tissues (1). Among these ectopic presentations, peri-pancreatic bronchogenic cysts (PBCs) are exceptionally rare, with only a few cases documented globally (2). Although histologically benign, PBC poses significant diagnostic challenges. This difficulty stems from the absence of specific clinical symptoms, laboratory markers, or pathognomonic imaging features. Furthermore, their clinical presentation is often insidious, and their radiological appearance closely mimics that of other more common pancreatic cystic lesions, such as pseudocysts and mucinous cystadenomas. Consequently, PBCs are frequently misdiagnosed or overlooked (3, 4). Current diagnostic strategies therefore necessitate a multidisciplinary approach, relying on the integration of clinical findings, detailed imaging characteristics, and ultimately, definitive pathological confirmation (5). Endoscopic ultrasonography (EUS)-guided through-the-needle biopsy (EUS-TTNB) is a feasible method for precise histological diagnoses before operation (6, 7). It is noteworthy that, similar to mucinous cystic neoplasms, bronchogenic cysts have been reported to harbor malignant potential (8). However, the specific triggers for malignant transformation in PBC remain entirely unknown. Given its rarity and diagnostic complexity, accumulating detailed case reports describing the comprehensive clinical, radiological, and pathological features of PBC is crucial to enhance our understanding of this entity. In this context, we present a case of PBC successfully managed with open distal pancreatectomy and splenectomy, contributing to the limited literature on this condition.
Case presentation
A 21-year-old male presented with intermittent upper abdominal discomfort. Diagnostic evaluation revealed a pancreatic mass. The patient reported no history of industrial chemical exposure or prior radiotherapy. Physical examination was unremarkable. Laboratory investigations, including comprehensive metabolic panel, hepatic and renal function tests, and tumor markers [carcinoembryonic antigen (CEA), cancer antigen19-9 (CA19-9), carbohydrate antigen 125 (CA125)]—were within normal limits. Contrast-enhanced abdominal CT demonstrated a well-circumscribed, non-enhancing hypodense cystic lesion (3.6 × 3.5 cm^2^) in the pancreatic body without main pancreatic duct dilation (Figures 1A–C). Subsequent contrast-enhanced ultrasound corroborated these findings, identifying a 4.2 × 3.2 cm^2^ cystic structure in the same location. Based on these features, a preoperative diagnosis of pancreatic cystic lesion was established. Following multidisciplinary review, the patient underwent open distal pancreatectomy with splenectomy (Figure 2A). Intraoperative inspection identified a discrete mass within the pancreatic body (Figure 2B). Upon incision, the cyst released viscous, light-yellow gelatinous material; the cystic cavity exhibited a smooth lining without mural nodules or neoplastic growth (Figures 2C,D). Histopathological analysis confirmed the diagnosis: the cyst wall was lined by pseudostratified ciliated columnar epithelium supported by fibroconnective tissue containing submucosal glands and smooth muscle bundles—pathognomonic features of a bronchogenic cyst (Figures 2E,F).
The lesion in the pancreatic body was detected on CT scan, which was marked by red arrows. (A, plain scan; B, arterial phase; C, venous phase).
The patient underwent open distal pancreatectomy (A), gross examination showed a pancreatic mass are located in the body of pancreas (B) after the pancreatic mass was opened, a light yellow, soft, gelatinous substance flowed out, and the cystic cavity was smooth and no new organisms were found (C,D). Histopathological analysis showed that the cyst wall of the pancreatic mass was lined with a pseudo-lamellar fibrous columnar epithelium, which was considered to be a bronchogenic cyst of the pancreas (E. HE staining, ×100; F. HE staining, ×400).
The patient's postoperative course was uneventful. He was discharged on postoperative day 7 with stable vital signs and normalized laboratory parameters. Surveillance protocol included regular outpatient follow-up with serial imaging. At 24-month follow-up, contrast-enhanced CT confirmed no evidence of recurrence, supporting the benign nature of this rare entity (Figures 3A,B).
CT showed the patient was free from tumor recurrence after 2 years' following up. (A and B, Plain scan).
Discussion
Bronchogenic cyst is a rare congenital developmental abnormality of the anterior bowel (1), which is commonly found in the mediastinum (9) or lung (10), and occasionally in the diaphragm (11), neck (12), and abdominal cavity (13) (Table 1). Bronchogenic cysts of the pancreas are extremely rare (2). Clinical manifestations of PBCs are notably nonspecific. Most remain clinically silent unless complications develop, such as: Secondary infection leading to inflammatory symptoms; Significant cyst enlargement causing mass effect on adjacent viscera. Symptomatic presentations typically reflect mechanical compression, including nausea, vomiting, and epigastric discomfort when substantial cyst expansion impinges on neighboring structures like the stomach or duodenum.
Diagnostic challenges persist due to the absence of pathognomonic features across clinical presentation, laboratory parameters, and conventional imaging. Symptom emergence often serves as the primary indicator necessitating further investigation (14). While contrast-enhanced CT and MRI provide essential morphological characterization, several factors complicate radiographic differentiation: Variable cyst fluid composition (proteinaceous content, calcium deposits); Size-dependent enhancement patterns; Secondary inflammatory changes from superinfection; Similar appearance to more common pancreatic cystic neoplasms (15, 16).
It is reported that EUS-guided through-the-needle biopsy (EUS-TTNB) facilitates definitive histological characterization prior to intervention (17). Cytological diagnosis via EUS-FNA predominantly relies on demonstrating ciliated epithelial cells within aspirated fluid samples (18). Current diagnostic paradigms necessitate multidisciplinary integration of clinical context, advanced imaging, and ultimately histopathological verification (5). However, a wrong diagnosis of nature is common in pancreatic cystic neoplasms (PCNs). About one-fifth of resected PCNs remained preoperatively misdiagnosed, despite according to international consensus guidelines, the EUS has been widespread used (19).
Surgical management remains controversial, particularly for asymptomatic cysts. Conservative observation may be considered for incidentally discovered, radiologically classic lesions. Several authorities advocate prophylactic excision given the diagnostic uncertainty and oncological concerns (20). Compelling arguments for resection include: Parallels with mucinous cystic neoplasms (10%–15% malignancy rate, size-dependent risk) (21); Established malignant potential, with documented cases of carcinomatous transformation (22, 23); Prevention of infectious, hemorrhagic, or obstructive complications; Resolution of symptomatic mass effect (23).
In the present case, preoperative evaluation could not exclude a mucinous cystic neoplasm, prompting open distal pancreatectomy. Prognostically, complete resection of benign bronchogenic cysts typically yields excellent outcomes with near 100% long-term survival (3, 24). Nevertheless, critical considerations include: Mandatory histopathological confirmation to exclude malignant elements; Documentation of cyst wall integrity and epithelial characteristics; Need for longitudinal surveillance data to establish PBC-specific malignant risk profiles.
Conclusions
In summary, we have documented a rare case of pancreatic bronchogenic cyst (PBC). The patient underwent open distal pancreatectomy following preoperative identification of a pancreatic cystic lesion, with definitive histopathological confirmation of PBC. Current evidence indicates that complete surgical resection remains the optimal therapeutic approach for bronchogenic cysts presenting with: Significant mass effect; Infectious complications; Hemorrhagic manifestations; Rupture risk; Diameter exceeding 3 cm. Notably, radical excision generally yields excellent long-term outcomes. Further research is warranted to refine diagnostic algorithms and optimize management strategies for this rare entity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Altieri MS Zheng R Pryor AD Heimann A Ahn S Telem DA. Esophageal bronchogenic cyst and review of the literature. Surg Endosc. (2015) 29:3010–5. 10.1007/s 00464-015-4082-425669636 · doi ↗ · pubmed ↗
- 2Gómez Alonso MI Lomeña Álvarez G Pinto García I Cruz Portero S. An intrapancreatic bronchogenic cyst simulating a mucinous cystadenoma. A case report. Rev Esp Enferm Dig. (2021) 113:292–3. 10.17235/reed.2020.7367/202033267599 · doi ↗ · pubmed ↗
- 3Brugge WR Lauwers GY Sahani D Fernandez-del Castillo C Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med. (2004) 351:1218–26. 10.1056/NEJ Mra 03162315371579 · doi ↗ · pubmed ↗
- 4Kouanda A Umetsu S Dai SC. Microforceps in the diagnosis of pancreatic bronchogenic cyst under endoscopic ultrasound guidance. ACG Case Rep J. (2020) 7:e 00356. 10.14309/crj.000000000000035632337317 PMC 7162121 · doi ↗ · pubmed ↗
- 5European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms. Gut. (2018) 67:789–804. 10.1136/gutjnl-2018-31602729574408 PMC 5890653 · doi ↗ · pubmed ↗
- 6Larghi A Manfrin E Fabbri C CrinòSF Correale L Chiarello G Interobserver agreement among expert pathologists on through-the-needle microforceps biopsy samples for evaluation of pancreatic cystic lesions. Gastrointest Endosc. (2019) 90:784–92.e 784. 10.1016/j.gie.2019.07.01131323232 · doi ↗ · pubmed ↗
- 7Conti Bellocchi MC Manfrin E Brillo A Bernardoni L Lisotti A Fusaroli P Rare pancreatic/peripancreatic cystic lesions can be accurately characterized by EUS with through-the-needle biopsy-A unique pictorial essay with clinical and histopathological correlations. Diagnostics (Basel, Switzerland). (2023) 13:3663. 10.3390/diagnostics 1324366338132247 PMC 10743172 · doi ↗ · pubmed ↗
- 8Kluger MD Tayar C Belli A Salceda JA van Nhieu JT Luciani A A foregut cystic neoplasm with diagnostic and therapeutic similarities to mucinous cystic neoplasms of the pancreas. JOP. (2013) 14:446–9. 10.6092/1590-8577/140223846945 · doi ↗ · pubmed ↗