Efficacy and safety of camrelizumab-based regimens in advanced squamous cell carcinoma patients: a prospective multicenter study
Weijia Jiang, Wanren Peng, Dong Qian, Genhe Wang, Hong Qian, Wenxia Deng, Zishu Wang, Zhiyong Wei, Tai Ma, Dong Zhao, Yifu He, Chenghui Li, Gang Wang, Zhongxian Zheng, Xinglai Guo, Shaojin Zhu, Liming Xia, Xiangde Jiang, Jie Wei, Xinzhong Li, Guoping Sun

TL;DR
This study finds that camrelizumab-based treatments are effective and safe for advanced esophageal cancer patients in real-world settings.
Contribution
The study evaluates camrelizumab's efficacy and safety in a broader patient population beyond clinical trial settings.
Findings
Camrelizumab combination therapy prolonged progression-free survival compared to monotherapy.
Most adverse events were mild (grade 1-2), with fatigue and anorexia being the most common.
Median overall survival was 17.4 months with camrelizumab-based regimens.
Abstract
Camrelizumab-based regimens show promising efficacy in esophageal cancer patients, according to previous pivotal trials. Given the strict eligibility criteria in pivotal trials, real-world studies are essential to evaluate the efficacy and safety of camrelizumab-based regimens in a broader patient population under routine clinical practice. Therefore, this study aimed to explore the efficacy and safety of camrelizumab-based regimens for the treatment of advanced esophageal cancer patients in real world settings. A total of 192 advanced esophageal cancer patients receiving camrelizumab-based regimens were included in this study. The specific camrelizumab-based regimens were decided by the investigators according to the patients’ physical condition. For efficacy assessment, treatment response and survival were assessed. For safety assessment, adverse events were collected. The median…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
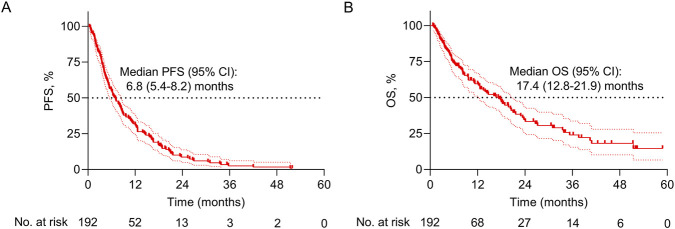 FIGURE 1
FIGURE 1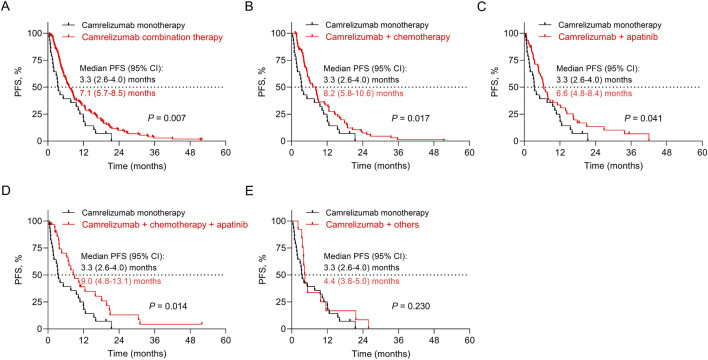 FIGURE 2
FIGURE 2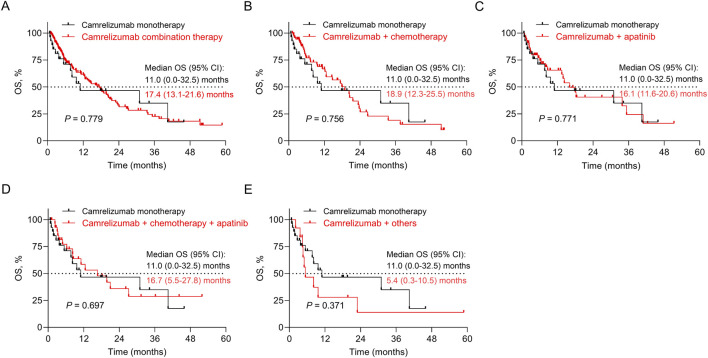 FIGURE 3
FIGURE 3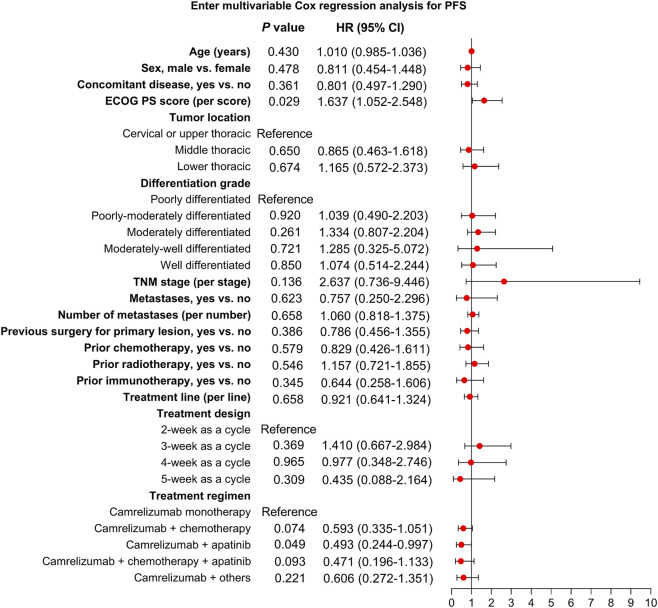 FIGURE 4
FIGURE 4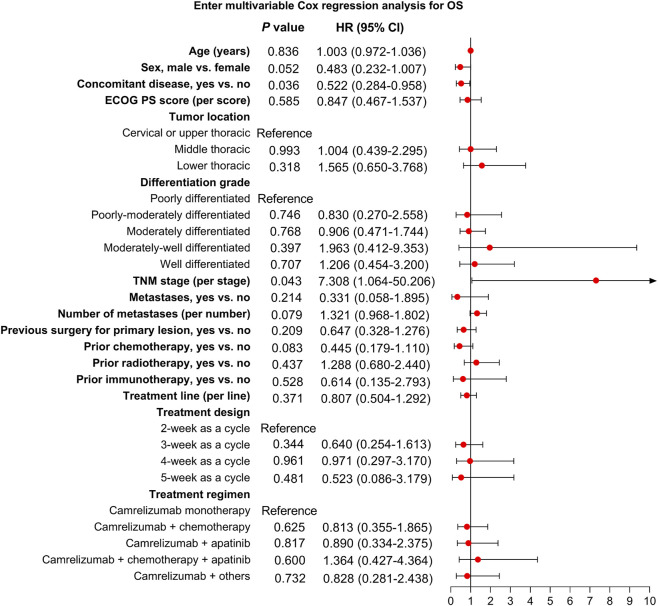 FIGURE 5
FIGURE 5| Items | Patients (N = 192) |
|---|---|
| Age (years), mean ± SD | 65.5 ± 9.8 |
| Sex, n (%) | |
| Female | 34 (17.7) |
| Male | 158 (82.3) |
| Concomitant disease, n (%) | |
| No | 114 (59.4) |
| Yes | 77 (40.1) |
| Unknown | 1 (0.5) |
| ECOG PS score, n (%) | |
| 0 | 33 (17.2) |
| 1 | 141 (73.4) |
| 2 | 18 (9.4) |
| Tumor location, n (%) | |
| Cervical spine or upper chest | 32 (16.7) |
| Middle chest | 85 (44.3) |
| Lower chest | 58 (30.2) |
| Unknown | 17 (8.9) |
| Histological classification, n (%) | |
| Squamous cell carcinoma | 186 (96.9) |
| Adenocarcinoma | 4 (2.1) |
| Adenosquamous carcinoma | 1 (0.5) |
| Small cell carcinoma | 1 (0.5) |
| Differentiation grade, n (%) | |
| Poorly differentiated | 52 (27.1) |
| Poorly-moderately differentiated | 17 (8.9) |
| Moderately differentiated | 69 (35.9) |
| Moderately-well differentiated | 3 (1.6) |
| Well differentiated | 14 (7.3) |
| Unknown | 37 (19.3) |
| TNM stage, n (%) | |
| III | 18 (9.4) |
| IV | 174 (90.6) |
| Metastases, n (%) | |
| No | 20 (10.4) |
| Yes | 172 (89.6) |
| Number of metastases, median (range) | 1.0 (0.0, 8.0) |
| Items | Patients (N = 192) |
|---|---|
| Previous surgery for primary lesion, n (%) | |
| No | 95 (49.5) |
| Yes | 96 (50.0) |
| Unknown | 1 (0.5) |
| Prior chemotherapy, n (%) | |
| No | 43 (22.4) |
| Yes | 148 (77.1) |
| Unknown | 1 (0.5) |
| Prior radiotherapy, n (%) | |
| No | 79 (41.1) |
| Yes | 113 (58.9) |
| Prior immunotherapy, n (%) | |
| No | 185 (96.4) |
| Yes | 7 (3.6) |
| Treatment line, n (%) | |
| 1st | 58 (30.2) |
| 2nd | 75 (39.1) |
| ≥3rd | 59 (30.7) |
| Duration of each cycle, n (%) | |
| 2-week | 22 (11.5) |
| 3-week | 151 (78.6) |
| 4-week | 16 (8.3) |
| 5-week | 3 (1.6) |
| Treatment regimen, n (%) | |
| Camrelizumab monotherapy | 29 (15.1) |
| Camrelizumab + chemotherapy | 74 (38.5) |
| Camrelizumab + apatinib | 46 (24.0) |
| Camrelizumab + chemotherapy + apatinib | 30 (15.6) |
| Camrelizumab + others | 13 (6.7) |
| Items | Patients (N = 192) |
|---|---|
| CR, n (%) | 0 (0.0) |
| PR, n (%) | 36 (18.8) |
| SD, n (%) | 126 (65.6) |
| PD, n (%) | 30 (15.6) |
| ORR, n (%) | 36 (18.8) |
| DCR, n (%) | 162 (84.4) |
| Items | Total | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|---|
| Total adverse events, n (%) | 136 (71.4) | 50 (26.0) | 73 (38.0) | 12 (6.3) | 2 (1.0) |
| Fatigue, n (%) | 40 (20.8) | 31 (16.1) | 9 (4.7) | 0 (0.0) | 0 (0.0) |
| Anorexia, n (%) | 37 (19.3) | 24 (12.5) | 13 (6.8) | 0 (0.0) | 0 (0.0) |
| Leukopenia, n (%) | 29 (15.6) | 10 (5.2) | 19 (9.9) | 1 (0.5) | 0 (0.0) |
| Nausea and vomiting, n (%) | 19 (9.9) | 15 (7.8) | 4 (2.1) | 0 (0.0) | 0 (0.0) |
| Pneumonia, n (%) | 19 (9.9) | 5 (2.6) | 11 (5.7) | 3 (1.6) | 0 (0.0) |
| Cough, n (%) | 16 (8.3) | 11 (5.7) | 4 (2.1) | 1 (0.5) | 0 (0.0) |
| Myelosuppression, n (%) | 16 (8.3) | 3 (1.6) | 9 (4.7) | 2 (1.0) | 2 (1.0) |
| RCCEP, n (%) | 15 (7.8) | 7 (3.6) | 8 (4.2) | 0 (0.0) | 0 (0.0) |
| Hypothyroidism, n (%) | 13 (6.8) | 3 (1.6) | 9 (4.7) | 1 (0.5) | 0 (0.0) |
| Anemia, n (%) | 12 (6.3) | 4 (2.1) | 6 (3.1) | 2 (1.0) | 0 (0.0) |
| Thrombocytopenia, n (%) | 12 (6.3) | 4 (2.1) | 6 (3.1) | 2 (1.0) | 0 (0.0) |
| Fever, n (%) | 10 (5.2) | 3 (1.6) | 7 (3.6) | 0 (0.0) | 0 (0.0) |
| Rash, n (%) | 9 (4.7) | 4 (2.1) | 5 (2.6) | 0 (0.0) | 0 (0.0) |
| Gastroenteritis, n (%) | 8 (4.2) | 7 (3.6) | 1 (0.5) | 0 (0.0) | 0 (0.0) |
| Hypertension, n (%) | 8 (4.2) | 3 (1.6) | 5 (2.6) | 0 (0.0) | 0 (0.0) |
| Neutropenia, n (%) | 5 (2.6) | 0 (0.0) | 5 (2.6) | 0 (0.0) | 0 (0.0) |
| Abdominal pain, n (%) | 4 (2.1) | 4 (2.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Decreased hemoglobin, n (%) | 1 (0.5) | 0 (0.0) | 1 (0.5) | 0 (0.0) | 0 (0.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Cancer Immunotherapy and Biomarkers · Inflammatory Biomarkers in Disease Prognosis
Introduction
1
Esophageal cancer is a prevalent malignancy accounting for approximately 0.51 million new cases and 0.45 million fatalities in 2022, worldwide (Bray et al., 2024). Surgery remains the standard therapy for early-stage esophageal cancer patients, but most esophageal cancer patients are diagnosed at an advanced stage (Deboever et al., 2024; Sheikh et al., 2023). Despite the progress in the treatment of advanced esophageal cancer, the prognosis of these patients remains poor (He et al., 2021; Puhr et al., 2023; Siegel et al., 2025; Waters and Reznik, 2022). Thus, investigating potential treatments is crucial in improving the prognosis of advanced esophageal cancer patients.
Currently, programmed cell death-1 (PD-1) inhibitors have emerged as a crucial treatment regimen for advanced esophageal cancer (Shoji et al., 2024; Yang et al., 2023; Yang et al., 2024). PD-1 inhibitors exert their effect by inhibiting the interaction between PD-1 and its ligands, which enhances T cell activity, thereby strengthening the capability of the immune system to recognize and eliminate cancer cells (Yang et al., 2023). Previous studies have illustrated that several PD-1 inhibitors, such as nivolumab and pembrolizumab, have exhibited promising efficacy in various malignancies, including esophageal cancer (Doki et al., 2022; Janjigian et al., 2024; Janjigian et al., 2021; Rha et al., 2023; Sun et al., 2018; Sun et al., 2021).
Camrelizumab, a humanized high-affinity immunoglobulin G4-kappa monoclonal antibody targeting PD-1, has been developed to treat diverse cancers, including esophageal cancer (Markham and Keam, 2019). As reported by the ESCORT study, camrelizumab as a second-line treatment achieved objective response rate (ORR) and disease control rate (DCR) of 20.2% and 44.7% in advanced or metastatic esophageal squamous cell carcinoma (ESCC) patients (Huang et al., 2020). Additionally, the ESCORT-1^st^ study indicated that camrelizumab plus chemotherapy as a first-line treatment achieved progression-free survival (PFS) and overall survival (OS) of 6.9 months and 15.3 months in advanced or metastatic ESCC patients (Luo et al., 2021). Based on these promising outcomes from the pivotal clinical trials, camrelizumab has been recommended as a first or second-line treatment for advanced ESCC patients in the Chinese Society of Clinical Oncology (CSCO) guidelines. However, the strict selection criteria of the previous trials often exclude patients with poor performance status or prior treatments (common characteristics in clinical practice), limiting the generalizability of their results to broader patient populations.
Accordingly, this real-world study aimed to evaluate the efficacy and safety of camrelizumab-based regimens in patients with advanced esophageal cancer in real-world settings. In particular, this study provided additional evidence on the comparative outcomes of different camrelizumab-based combinations and explored prognostic factors associated with survival, thereby offering novel insights into the optimal real-world use of camrelizumab beyond controlled trial populations. We hypothesized that camrelizumab-based regimens would demonstrate acceptable efficacy and manageable safety, with combination therapy potentially conferring survival advantages over monotherapy in the real-world setting.
Methods
2
Patients
2.1
In this prospective, open-label, multicenter, observational study, 192 advanced esophageal cancer patients who were about to receive camrelizumab were consecutively enrolled. The inclusion criteria contained: i) aged ≥18 years; ii) histologically or cytologically confirmed as esophageal cancer; iii) tumor-node-metastasis (TNM) stage III-IV; iv) about to receive camrelizumab; v) had at least one measurable lesion according to Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria; vi) Eastern Cooperative Oncology Group Performance Status (ECOG PS) score 0-2; vii) estimated survival time ≥3 months; viii) voluntary for participation; ix) were considered to benefit from the treatment by the investigator. The exclusion criteria contained: i) had a proven allergy to the drug and/or its excipients used in the study; ii) had immunodeficiency diseases or a history of organ transplantation; iii) pregnant or lactating women; iv) were deemed to be ineligible for inclusion by the investigators. This study adhered to the Declaration of Helsinki and received approval from the Ethics Committee of The First Affiliated Hospital of Anhui Medical University (PJ 2019-13-07). Each patient signed the informed consent. The study was registered with the Chinese Clinical Trial Registry under registration numbers ChiCTR1900027275 and ChiCTR2000040062.
Treatment
2.2
After screening by the inclusion/exclusion criteria, the eligible patients received camrelizumab-based regimens. Treatment allocation followed routine clinical decision-making. Investigators selected specific regimens based on a comprehensive assessment of patients’ clinical condition, including ECOG PS, comorbidities, tumor burden, previous therapy history, etc. The recommended regimens were as follows: i) camrelizumab monotherapy: camrelizumab 200 mg intravenous (IV) infusion every 2 weeks (Q2W) or 3 weeks (Q3W); ii) camrelizumab plus apatinib: camrelizumab 200 mg IV Q2W plus apatinib 250 mg orally once daily within 30 min postprandially, in 28-day cycles; iii) camrelizumab plus chemotherapy: camrelizumab 200 mg IV Q3W paired with chemotherapy. The chemotherapy regimens were chosen per the National Comprehensive Cancer Network (NCCN) guidelines. Specific treatment parameters, including therapeutic cycles and drug dosage, were subject to adjustment based on individual disease status and were meticulously documented throughout the study. The treatment was maintained until disease progression or intolerable toxicity.
Assessments
2.3
For efficacy assessment, the best response, including complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD), was evaluated via RECIST 1.1 criteria. Then, ORR and DCR were calculated. Besides, PFS and OS were assessed. The PFS was calculated from inclusion to disease progression or death from any cause. The OS was calculated from inclusion to death from any cause. The patients who were still alive at the last follow-up were recorded as censored, and the PFS/OS for the censored patients was calculated as the time from inclusion to censoring. For safety assessment, the adverse events were collected and evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0.
Statistics
2.4
No sample size calculation was performed, and we included as many eligible patients as possible. SPSS version 26.0 was applied to analyze clinical data. Mean, standard deviation, median, range, count, and percentage were utilized for data presentation, as appropriate. The Kaplan-Meier curve was used for the display of the PFS and OS. Log-rank test was used for comparison of PFS and OS in patients with different treatment regimens. P values from multiple comparisons were adjusted using the Benjamini–Hochberg false discovery rate (FDR) method. The enter multivariable Cox regression analysis was conducted to evaluate independent influencing factors for the PFS and OS. All clinical and treatment characteristics were included in the multivariable Cox regression analysis except for histological classification due to the imbalanced data distribution (only 6 patients were not squamous cell carcinoma, of which 5 progressed and 1 died). To address concerns regarding potential overfitting, a sensitivity analysis was performed using a parsimonious Cox regression model with a reduced set of clinically relevant covariates (age, sex, concomitant disease, ECOG PS score, tumor location, differentiation grade, TNM stage, treatment line, and treatment regimen). Subgroup analyses were conducted to evaluate the differences in PFS and OS across various subgroups stratified by sex, histological classification, and TNM stage. P < 0.05 indicated significance. The summary of methodology and key outcomes is shown in Supplementary Table S1.
Results
3
Study flow
3.1
This study enrolled patients from two clinical trials: ChiCTR1900027275 (N = 165) and ChiCTR2000040062 (N = 145). From the ChiCTR2000040062 cohort, 108 patients were excluded, leaving 37 patients treated with apatinib plus camrelizumab. Subsequently, a combined cohort of 202 patients was screened, and 10 patients who failed to meet the inclusion/exclusion criteria were excluded. Finally, 192 patients with advanced esophageal cancer receiving camrelizumab-based therapy were included in the study. Among these 192 patients, all discontinued treatment due to disease progression (N = 95), adverse events (N = 37), loss to follow-up (N = 38), death (N = 19), or other reasons (N = 3). The full analysis set, efficacy analysis set, and safety analysis set all comprised 192 patients (Supplementary Figure S1).
Baseline characteristics and treatment information
3.2
The mean age of the patients was 65.5 ± 9.8 years. There were 34 (17.7%) females and 158 (82.3%) males. The ECOG PS score was 0, 1, and 2 in 33 (17.2%), 141 (73.4%), and 18 (9.4%) patients, respectively. Regarding histological subtypes, 186 (96.9%) patients had squamous cell carcinoma, 4 (2.1%) patients had adenocarcinoma, 1 (0.5%) patient had adenosquamous carcinoma, and 1 (0.5%) patient had small cell carcinoma. Eighteen (9.4%) patients had a TNM stage of III, and 174 (90.6%) patients had a stage of IV. A total of 172 (89.6%) patients had metastases. The median (range) number of metastases was 1.0 (0.0, 8.0). The detailed baseline information is shown in Table 1.
A total of 29 (15.1%) patients received camrelizumab monotherapy, 74 (38.5%) patients received camrelizumab plus chemotherapy, 46 (24.0%) patients received camrelizumab plus apatinib, 30 (15.6%) patients received camrelizumab plus chemotherapy and apatinib, and 13 (6.7%) patients received camrelizumab plus others. The detailed treatment information is shown in Table 2.
Efficacy
3.3
No patients achieved CR. The rates of PR, SD, and PD were 18.8%, 65.6%, and 15.6%, respectively. The ORR and DCR were 18.8% and 84.4%, respectively, in patients who received camrelizumab-based regimens (Table 3).
The median [95% confidence interval (CI)] PFS was 6.8 (5.4–8.2) months (Figure 1A); the median OS (95% CI) was 17.4 (12.8–21.9) months in patients who received camrelizumab-based regimens (Figure 1B).
PFS and OS information. Kaplan-Meier curves for PFS (A) and OS (B).
Subgroup analyses for survival stratified by camrelizumab-based regimens
3.4
PFS was prolonged in patients who received camrelizumab combination therapy compared to those receiving camrelizumab monotherapy (P = 0.007, adjusted P = 0.028). Specifically, compared to patients who received camrelizumab monotherapy, PFS was longer in patients receiving camrelizumab plus chemotherapy (P = 0.017, adjusted P = 0.028), camrelizumab plus apatinib (P = 0.041, adjusted P = 0.051), and camrelizumab plus chemotherapy and apatinib (P = 0.014, adjusted P = 0.028). However, PFS was not different between patients who received camrelizumab plus others and those receiving camrelizumab monotherapy (P = 0.230, adjusted P = 0.230) (Figures 2A–E) (Supplementary Table S2).
Impact of different camrelizumab-based regimens on PFS. Comparison of PFS between patients receiving camrelizumab combination therapy and camrelizumab monotherapy (A), between patients receiving camrelizumab plus chemotherapy and camrelizumab monotherapy (B), between patients receiving camrelizumab plus apatinib and camrelizumab monotherapy (C), between patients receiving camrelizumab plus chemotherapy and apatinib and camrelizumab monotherapy (D), and between patients receiving camrelizumab plus others and camrelizumab monotherapy (E).
OS did not differ between patients who received camrelizumab combination therapy and those receiving camrelizumab monotherapy (P = 0.779, adjusted P = 0.779). Specifically, OS was not different between patients who received camrelizumab plus any therapy and those receiving camrelizumab monotherapy (all P > 0.05, all adjusted P > 0.05) (Figures 3A–E) (Supplementary Table S2).
Impact of different camrelizumab-based regimens on OS. Comparison of OS between patients receiving camrelizumab combination therapy and camrelizumab monotherapy (A), between patients receiving camrelizumab plus chemotherapy and camrelizumab monotherapy (B), between patients receiving camrelizumab plus apatinib and camrelizumab monotherapy (C), between patients receiving camrelizumab plus chemotherapy and apatinib and camrelizumab monotherapy (D), and between patients receiving camrelizumab plus others and camrelizumab monotherapy (E).
Subgroup analyses for survival stratified by sex, histological classification, and TNM stage
3.5
Subgroup analyses suggested that PFS and OS did not differ between male and female subgroups, squamous cell carcinoma and non-squamous cell carcinoma subgroups, or TNM stage III and IV subgroups (all P > 0.05) (Supplementary Table S3).
Independent factors related to survival
3.6
According to multivariable Cox regression analysis, the ECOG PS score was independently related to shorter PFS [hazard ratio (HR) = 1.637, P = 0.029]. Camrelizumab plus apatinib (vs. camrelizumab monotherapy) was independently associated with prolonged PFS (HR = 0.493, P = 0.049). Other factors, including age, sex, concomitant disease, tumor location, differentiation grade, TNM stage, metastases, number of metastases, previous surgery for primary lesion, prior chemotherapy, prior radiotherapy, prior immunotherapy, treatment line, and treatment design were not linked to PFS (all P > 0.05) (Figure 4).
Independent factors related to PFS.
Concomitant disease was independently related to prolonged OS (HR = 0.522, P = 0.036). However, TNM stage was independently related to shorter OS (HR = 7.308, P = 0.043). Other factors were not related to OS (all P > 0.05) (Figure 5).
Independent factors related to OS.
To validate the robustness of our findings from multivariable Cox regression analyses, a parsimonious Cox regression model was performed. The findings showed a similar trend to the multivariable Cox regression analysis, further supporting the robustness of our findings (Supplementary Table S4).
Safety
3.7
The total incidence of adverse events was 71.4%. Most adverse events were grade 1-2 (64.0%). The grade 3-4 adverse event incidence was 7.3%. The most frequent adverse events of any grade were fatigue (20.8%), anorexia (19.3%), and leukopenia (15.6%). Grade 3 adverse events included pneumonia (1.6%), myelosuppression (1.0%), anemia (1.0%), thrombocytopenia (1.0%), leukopenia (0.5%), cough (0.5%), and hypothyroidism (0.5%). The grade 4 adverse event was myelosuppression (1.0%). The incidence of immune-related adverse events, including reactive cutaneous capillary endothelial proliferation (RCCEP) and hypothyroidism, was 7.8% and 6.8%, respectively. All RCCEP (7.8%) and most hypothyroidism (6.3%) were graded 1-2 (Table 4).
Discussion
4
Camrelizumab-based regimens, such as camrelizumab monotherapy and camrelizumab plus chemotherapy or targeted therapy, achieve acceptable treatment response in esophageal cancer patients (Huang et al., 2020; Lu et al., 2025; Luo et al., 2021; Meng et al., 2024; Zhang et al., 2020). For example, camrelizumab combined with apatinib and chemotherapy as a first-line treatment achieved ORR and DCR of 80.0% and 96.7%, respectively, in advanced ESCC patients (Zhang et al., 2020). Additionally, the ESCORT-1^st^ study reported that camrelizumab plus chemotherapy as a first-line treatment achieved an ORR of 72.1% and a DCR of 91.3% in advanced or metastatic ESCC patients (Luo et al., 2021). Moreover, the CAP 02 Re-challenge study indicated that the ORR and DCR were 10.2% and 69.4% in advanced ESCC patients who had a history of immune checkpoint inhibitors (Meng et al., 2024). Overall, the previously reported range of ORR was 10.2%–80.0%, and the range of DCR was 69.4%–96.7% in advanced esophageal cancer patients receiving camrelizumab-based regimens (Huang et al., 2020; Lu et al., 2025; Luo et al., 2021; Meng et al., 2024; Zhang et al., 2020). In this study, the ORR and DCR were 18.8% and 84.4%, respectively, in advanced esophageal cancer patients. The ORR and DCR identified in this study were within the ranges reported by previous studies (Huang et al., 2020; Lu et al., 2025; Luo et al., 2021; Meng et al., 2024; Zhang et al., 2020). Therefore, in real-world clinical practice, camrelizumab-based regimens could exhibit potentially satisfactory efficacy in advanced esophageal cancer patients. According to previous real-world clinical studies, the ORR and DCR ranged from 15.1% to 72.0% and 35.8%–92.0% in advanced esophageal cancer patients receiving PD-1 inhibitor-based regimens (Kao et al., 2023; Kim et al., 2022; Makino et al., 2024). Compared to these data, camrelizumab appeared to show comparable efficacy to other PD-1 inhibitors. Therefore, camrelizumab might serve as a potential immunotherapy option for the treatment of advanced esophageal cancer.
PD-1 inhibitors have dramatically revolutionized the treatment landscape of esophageal cancer and prolonged the survival of patients (Shoji et al., 2024). According to previous studies, camrelizumab-based regimens achieved median PFS of 5.7–9.9 months and OS of 10.9–19.4 months in advanced esophageal cancer patients (Lu et al., 2025; Luo et al., 2021; Zhang et al., 2020). Similar to the findings of the previous studies, this study discovered that camrelizumab-based regimens achieved median PFS and OS of 6.8 and 17.4 months in advanced esophageal cancer patients. Some real-world clinical studies reported that PD-1 inhibitor-based regimens achieved median PFS of 1.9–9.8 months and OS of 6.4–20.3 months in advanced esophageal cancer patients (Kao et al., 2023; Kim et al., 2022; Makino et al., 2024). Compared to these real-world data, camrelizumab seemed to provide similar survival outcomes to other PD-1 inhibitors. In real-world clinical practice, the strategies of camrelizumab-based regimens are largely different, with camrelizumab plus chemotherapy being the most frequently prescribed regimen for advanced esophageal cancer patients (Lu et al., 2025). Therefore, it is meaningful to explore the impact of camrelizumab-based treatment strategies on the survival of advanced esophageal cancer patients. We found that PFS was prolonged in advanced esophageal cancer patients receiving camrelizumab combination therapy compared to those receiving camrelizumab monotherapy. In detail, compared with patients receiving camrelizumab monotherapy, PFS was longer in patients receiving camrelizumab plus chemotherapy, camrelizumab plus apatinib, and camrelizumab plus chemotherapy and apatinib. According to previous evidence, we speculated that camrelizumab, apatinib, and chemotherapy might possess a synergistic anti-tumor effect, which could reprogram the immunosuppressive tumor microenvironment, thereby achieving a better PFS compared to camrelizumab alone (Li et al., 2022; Ramakrishnan and Gabrilovich, 2011). Regarding OS, it seemed to be prolonged in patients receiving camrelizumab combined with other regimens compared to those receiving camrelizumab monotherapy, but it did not achieve statistical significance. The inconsistency between PFS and OS outcomes might be as follows: (1) the sample size in each subgroup was small, limiting the statistical power. (2) the improvement in PFS reflected earlier disease control, while OS was influenced by multiple post-progression factors, such as subsequent systemic therapy, patient performance status, and tumor heterogeneity. The presence of these factors might inhibit the translation of PFS improvement in OS.
Furthermore, we explored independent factors associated with PFS and OS in advanced esophageal cancer patients. (1) ECOG PS score was independently related to a shorter PFS in advanced esophageal cancer patients. A possible explanation would be that patients with a higher ECOG PS score tended to have difficulty tolerating cancer treatments, such as immunotherapy-based treatments, resulting in a poor PFS in these patients (Zhang et al., 2021). (2) Camrelizumab plus apatinib (vs. camrelizumab monotherapy) was independently associated with a longer PFS in advanced esophageal cancer patients. A reason behind this could be that camrelizumab plus apatinib could synergistically enhance anti-tumor immune responses by increasing the ratio of cluster of differentiation (CD)8^+^ cytotoxic T cells to forkhead box protein 3^+^ Treg cells, the accumulation of CD20^+^ B cells, and the T-helper (Th)1/Th2 cytokine ratio, which led to a prolonged PFS (Zhang et al., 2021). (3) Concomitant disease was independently related to a longer OS in advanced esophageal cancer patients. However, more evidence is required to validate this finding. (4) TNM stage was independently associated with a poor OS in advanced esophageal cancer patients. Advanced TNM stage reflected a greater tumor burden (Marom, 2022). Therefore, patients with advanced TNM stage might benefit less from camrelizumab-based regimens, leading to a poor OS.
The incidence of adverse events following camrelizumab-based regimens ranged from 73.0% to 100.0% in advanced esophageal cancer patients according to previous studies (Lu et al., 2025; Luo et al., 2021; Meng et al., 2022; Zhang et al., 2020). Most common adverse events were anemia, alopecia, decreased neutrophil count, increased alanine aminotransferase level, decreased white blood cell count, anorexia, and fatigue (Lu et al., 2025; Luo et al., 2021; Zhang et al., 2020). However, in this study, the incidence of adverse events was 71.4% in advanced esophageal cancer patients receiving camrelizumab-based regimens, which was slightly lower than the data in previous studies. We speculated that this discrepancy might be attributable to the inherent limitations of real-world studies, where adverse event reporting was primarily driven by clinical relevance, potentially leading to underreporting of mild or transient adverse events. In this study, the most frequently encountered adverse events were fatigue, anorexia, and leukopenia. The majority of adverse events were grade 1-2 (64.0%). The incidence of grade 3-4 adverse events was relatively low (7.3%). Additionally, immune-related adverse events, such as RCCEP and hypothyroidism, were also observed in this study, with the overall incidence of 7.8% and 6.8%, respectively. Most of these two immune-related adverse events were grade 1-2, suggesting that they were mild to moderate and manageable. Overall, our findings suggested that camrelizumab-based regimens appeared to be generally safe and tolerable, but further large-scale studies are needed to confirm their safety profile.
Although promising findings were discovered in this study, limitations could not be omitted. (1) The single-arm design hindered us from comparing the efficacy and safety of camrelizumab-based regimens with other treatments, such as chemotherapy, in advanced esophageal cancer patients, which in turn limited our capacity to attribute the observed therapeutic effects solely to the treatment itself. (2) Our study presented real-world insights into the use of camrelizumab-based regimens in advanced esophageal cancer patients. However, this study was conducted in China, which restricted the generalizability of our findings. (3) We conducted subgroup analyses to explore the advantages of specific camrelizumab-based regimens in prolonging the survival of advanced esophageal cancer patients. Nevertheless, the sample size in each subgroup was relatively small, which might restrain the statistical power. (4) Some eligibility criteria in this study were based on investigators’ subjective judgment, which reflected common practice in real-world clinical settings. However, such subjective judgment might introduce selection bias. (5) Due to the observational nature of the study, confounding factors may have influenced the results. (6) Patients in this study received different camrelizumab-based regimens. This treatment heterogeneity, while reflective of real-world clinical practice, may have contributed to variability in efficacy and safety outcomes. (7) No prior statistical justification was performed, which might limit confidence in the negative findings of the survival analyses.
In conclusion, camrelizumab-based regimens achieve a median PFS and OS and 6.8 and 17.4 months, respectively, with an adverse event incidence of 71.4%, in advanced esophageal cancer patients. In clinical practice, the camrelizumab combination regimens may prolong PFS compared with its monotherapy; however, these findings are based on subgroup analyses with limited sample size and should be interpreted cautiously. Further validation in larger, controlled, and prospective studies is warranted to confirm these observations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R. L. Soerjomataram I. (2024). Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263. 10.3322/caac.21834 38572751 · doi ↗ · pubmed ↗
- 2Deboever N. Jones C. M. Yamashita K. Ajani J. A. Hofstetter W. L. (2024). Advances in diagnosis and management of cancer of the esophagus. BMJ 385, e 074962. 10.1136/bmj-2023-074962 38830686 · doi ↗ · pubmed ↗
- 3Doki Y. Ajani J. A. Kato K. Xu J. Wyrwicz L. Motoyama S. (2022). Nivolumab combination therapy in advanced esophageal squamous-cell carcinoma. N. Engl. J. Med. 386, 449–462. 10.1056/NEJ Moa 2111380 35108470 · doi ↗ · pubmed ↗
- 4He S. Xu J. Liu X. Zhen Y. (2021). Advances and challenges in the treatment of esophageal cancer. Acta Pharm. Sin. B 11, 3379–3392. 10.1016/j.apsb.2021.03.008 34900524 PMC 8642427 · doi ↗ · pubmed ↗
- 5Huang J. Xu J. Chen Y. Zhuang W. Zhang Y. Chen Z. (2020). Camrelizumab versus investigator's choice of chemotherapy as second-line therapy for advanced or metastatic oesophageal squamous cell carcinoma (ESCORT): a multicentre, randomised, open-label, phase 3 study. Lancet. Oncol. 21, 832–842. 10.1016/S 1470-2045(20)30110-8 32416073 · doi ↗ · pubmed ↗
- 6Janjigian Y. Y. Shitara K. Moehler M. Garrido M. Salman P. Shen L. (2021). First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (check Mate 649): a randomised, open-label, phase 3 trial. Lancet 398, 27–40. 10.1016/S 0140-6736(21)00797-2 34102137 PMC 8436782 · doi ↗ · pubmed ↗
- 7Janjigian Y. Y. Ajani J. A. Moehler M. Shen L. Garrido M. Gallardo C. (2024). First-line nivolumab plus chemotherapy for advanced gastric, gastroesophageal junction, and esophageal adenocarcinoma: 3-year Follow-Up of the phase III Check Mate 649 trial. J. Clin. Oncol. 42, 2012–2020. 10.1200/JCO.23.01601 38382001 PMC 11185916 · doi ↗ · pubmed ↗
- 8Kao M. W. Kuo Y. H. Hsieh K. C. Lee C. T. Wu S. C. Yang W. C. (2023). Immune checkpoint inhibitor, nivolumab, combined with chemotherapy improved the survival of unresectable advanced and metastatic esophageal squamous cell carcinoma: a real-world experience. Int. J. Mol. Sci. 24, 7312. 10.3390/ijms 24087312 37108474 PMC 10139434 · doi ↗ · pubmed ↗