Glucagon-like peptide-1 agonists in children with obesity and type 2 diabetes. an umbrella review
Hyder Mirghani, Laila Albishi, Sawsan Mohmmad Alblewi

TL;DR
GLP-1 agonists help reduce weight and improve blood sugar in children with obesity or type 2 diabetes, with few side effects.
Contribution
This umbrella review evaluates the effectiveness and safety of GLP-1 agonists in pediatric obesity and type 2 diabetes.
Findings
GLP-1 agonists significantly reduced body weight, HbA1c, BMI z, and systolic blood pressure in children.
Adverse events and hypoglycemia were comparable to controls, indicating good tolerability.
Only 11 meta-analyses were included due to limited literature on this topic in pediatric populations.
Abstract
Obesity and type 2 diabetes mellitus (Type 2 DM) are rising at an alarming rate among children and adolescents. This population often exhibits suboptimal glycemic control and diabetes-related complications. Glucagon-like peptide-1 receptor agonists (GLP-1 agonists) have emerged as a promising therapeutic option for pediatric patients due to their beneficial effects on weight reduction and glycemic regulation. Literature on this important issue is scarce. We aimed to assess the effects of GLP-1 agonists on body weight, HbA1c, body mass index z (BMI z), and systolic blood pressure (SBP). Additionally, we discussed adverse events and hypoglycemia. We searched PubMed/MEDLINE, Web of Science, and the Cochrane Library from October to November 2025 using the following terms: GLP-1 agonists, semaglutide, tirzepatide, liraglutide, exenatide, children, obesity, adolescents, blood pressure, BMI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
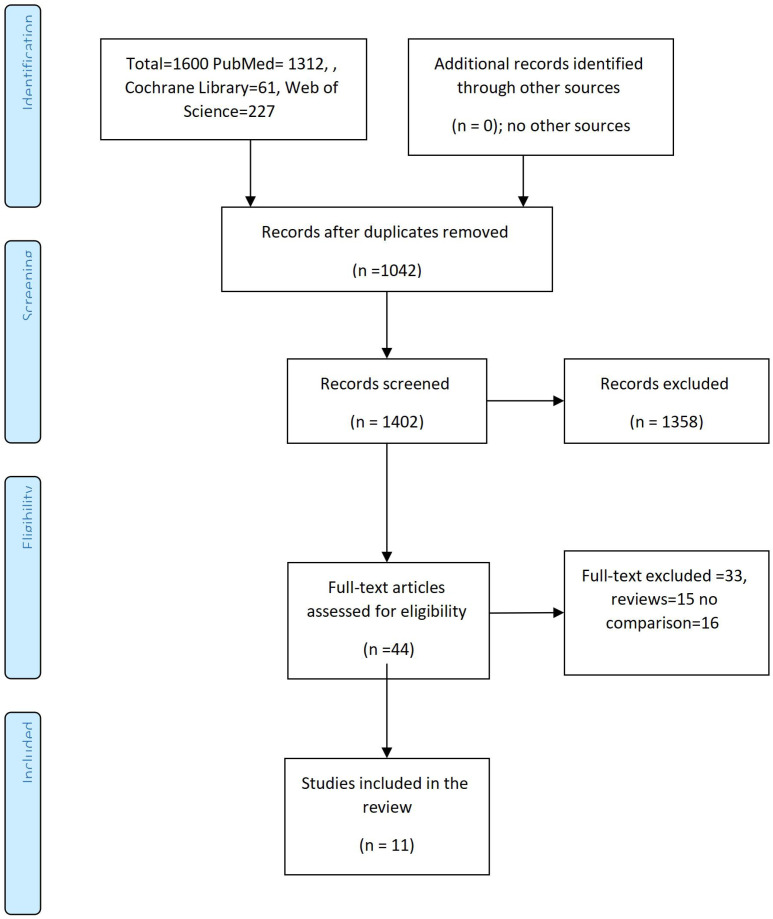 Figure 1
Figure 1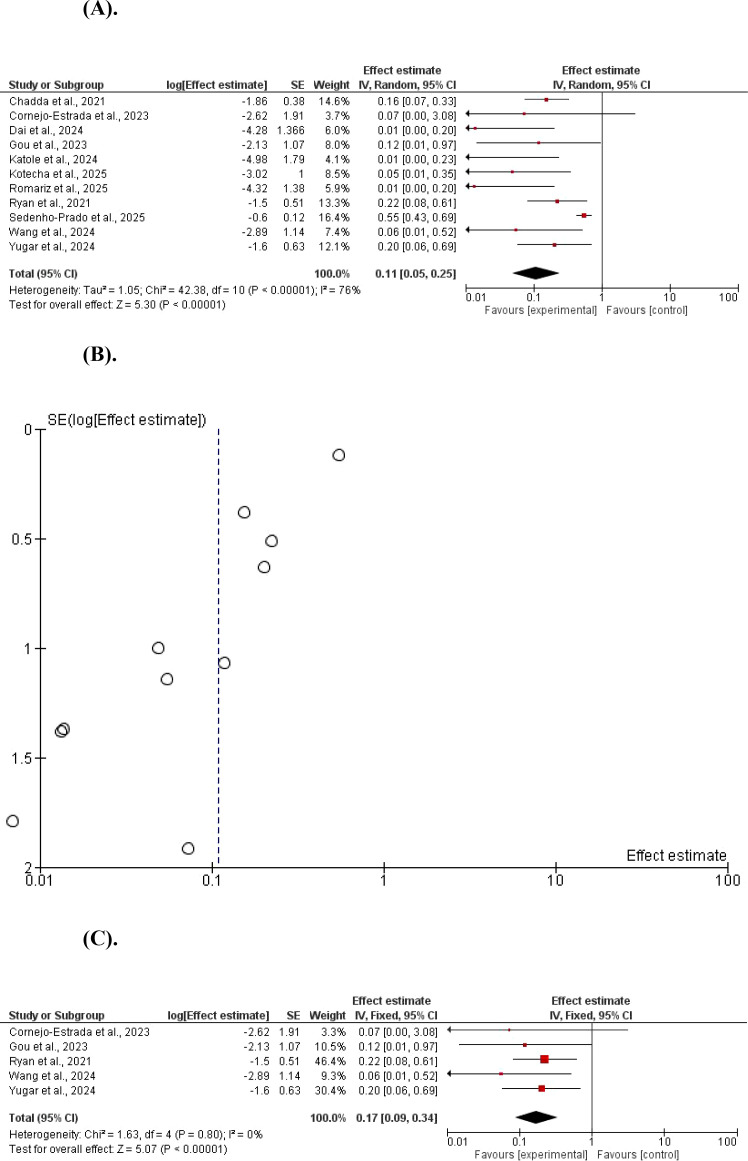 Figure 2
Figure 2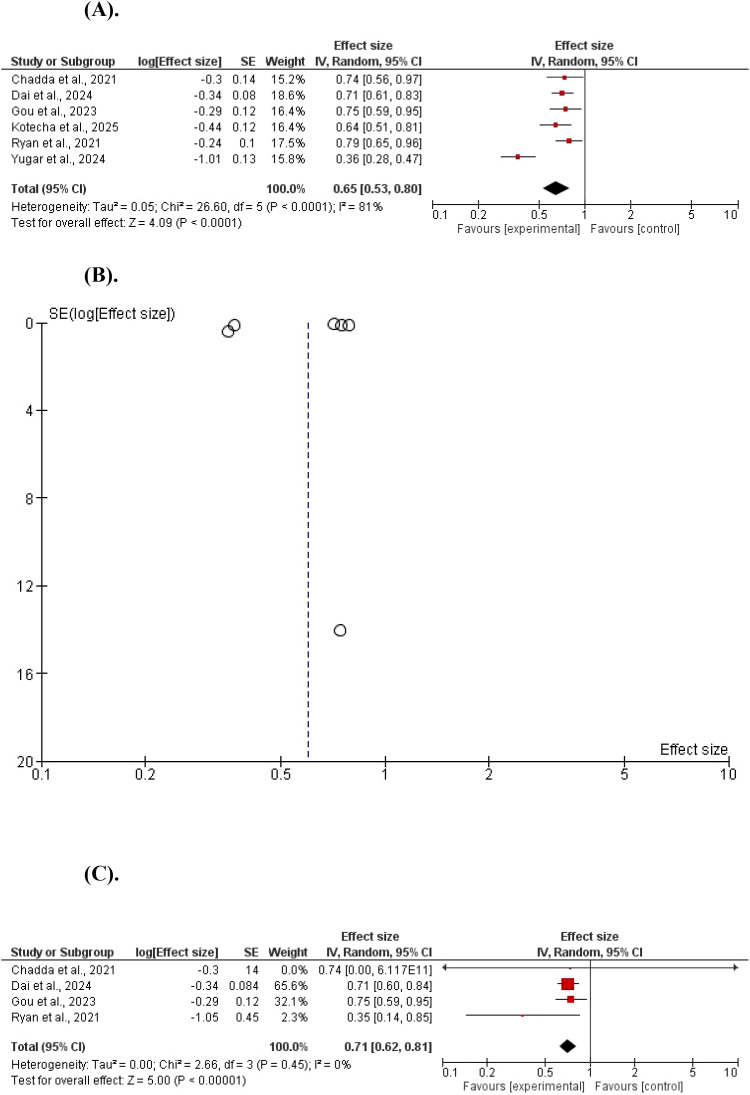 Figure 3
Figure 3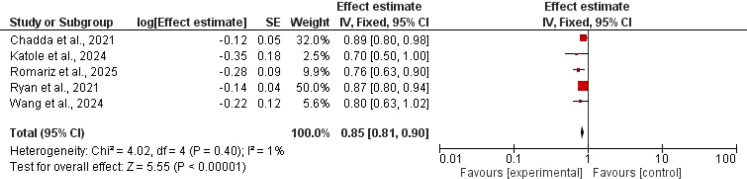 Figure 4
Figure 4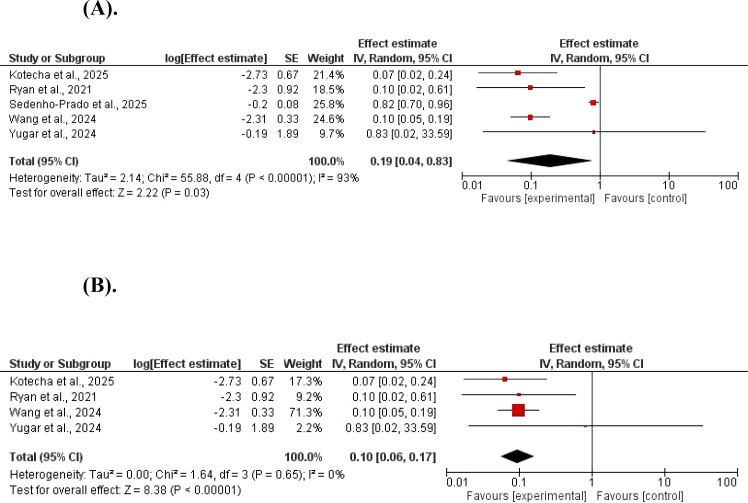 Figure 5
Figure 5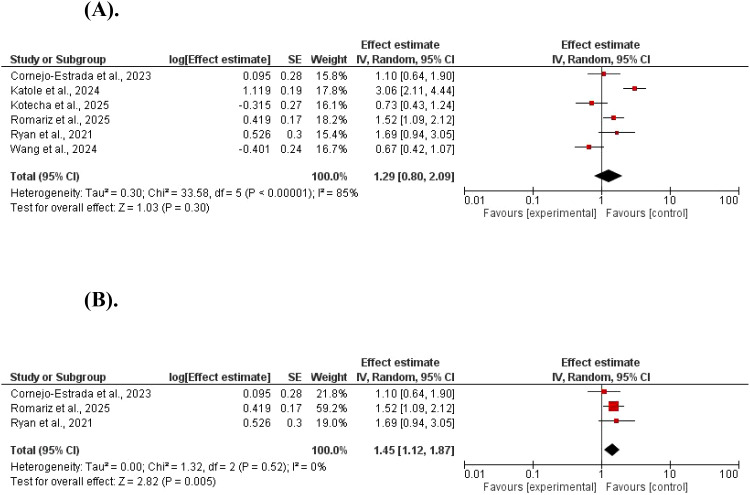 Figure 6
Figure 6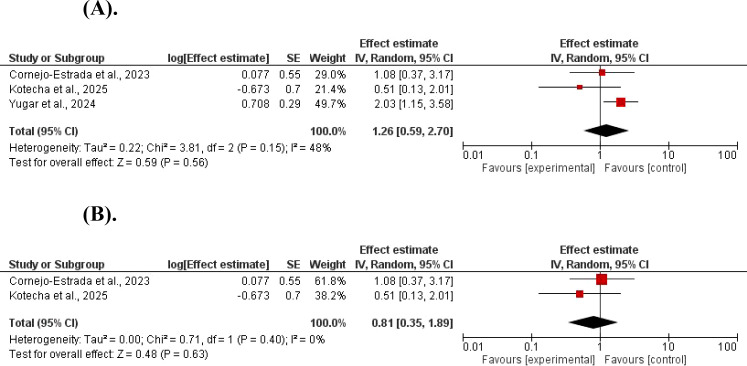 Figure 7
Figure 7| Author | HbA1c outcome | Adverse events outcome | Weight outcome | BMI, Z outcome | SBP outcome | Hypoglycemia outcome |
|---|---|---|---|---|---|---|
| Chadda et al., 2021 ( | MD -0.30; 95% CI -0.57, -0.04 | Not assessed | MD; -1.86; 95% CI -2.60, to -1.13 | MD -0.12; 95% CI -0.22, -0.03 | Not assessed | Not assessed |
| Cornejo-Estrada et al., 2023 ( | RR 1.10; 95%CI, 0.64 to 1.90 total | MD; −2.62, 95%CI, −6.35 to 1.12 | Not assessed | Not assessed | RR 1.08; 95%CI, 0.37 to 3.15 | |
| Dai et al., 2024 ( | RD; -0.34, 95% CI, -0.51, to -0.18 | Not assessed | RD; -4.28 95% CI, 6.95, -1.60 | Not assessed | Not assessed | Not assessed |
| Gou et al., 2023 ( | WMD: -0.29; 95% CI: -0.52, -0.06 | Not assessed | WMD: -2.13; 95%CI: -4.23, to -0.03 | Not assessed | Not assessed | Not assessed |
| Katole et al., 2024 ( | OR; 3.06, 95%CI, 2.12, 4.42, GIT | MD -4.98, 95% CI, -8.49, -1.46 | MD; -0.35, 95%CI -0.72, -0.01 | Not assessed | Not assessed | |
| Kotecha et al., 2025 ( | MD-0.44; 95% CI, -0.68% to -0.21 | RR; 0.73; 95% CI, 0.38 to 1.07 | MD; -3.02; 95% CI, -4.98 to -1.06 | Not assessed | MD; -2.73 mm Hg; 95% CI, -4.04 to -1.43 | RR; 0.51; 95% CI, -0.07 to 1.08 |
| Romariz et al., 2025 ( | RR 1.52; 95% CI 1.09 to 2.12, GIT | MD -4.32; 95% CI -7.02 to -1.63 | MD -0.28; 95% CI -0.45 to -0.1 | Not assessed | Not assessed | |
| Ryan et al., 2021 ( | MD -0.24; 95% CI, -0.44,-0.05 | RR;1.69, 95% CI, 0.95 to 3.10 | MD -1.50; 95% CI, -2.50, to -0.50 | MD -0.14, 95% CI, -0.23, to -0.06 | MD -2.30, 95% CI, -4.11, to -0.49 | Not assessed |
| Sedenho-Prado et al., 2025 ( | Not assessed | Not assessed | SMD −0.60; 95% CI −0.89 to −0.44 | SMD −0.20; 95% CI −0.35 to −0.04 | Not assessed | |
| Wang et al., 2024 ( | 0.37 | RR; 0.67, 95% CI, 0.40 to 1.02 | MD; -2.89; 95% CI, -5.12 to -0.65 | MD; -0.22, 95% CI, -0.45 to 0.01 | MD; -2.31, 95% CI, -2.96 to -1.65 | Not assessed |
| Yugar et al., 2024 ( | MD -1.01, 95% CI, -1.26; -76 | Not assessed | MD -1.6, 95% CI, -2.83;-3.6 | Not assessed | MD -0.19; 95% CI, -3.9;- 3.52 | OR 2.03; 95% CI, 1.16 to 3.54 |
| Study | Overall AMSTAR-2 confidence | Journal/year | Studies included | Participants age | Patients number | Morbidities |
|---|---|---|---|---|---|---|
| Chadda et al., 2021 ( | Moderate | Obes Rev 2021 | 9 trials | < 18 | 286 | DM/obesity |
| Cornejo-Estrada et al., 2023 ( | Low | Children 2023 | 3 trials | 5-< 18 | 296 | Obesity |
| Dai et al., 2024 ( | Low | J Clin Res Pediatr Endocrinol 2024 | 14 trials | < 18 | 1262 | DM/obesity |
| Gou et al., 2023 ( | Low–Moderate | Eur J Pediatr 2023 | 7 studies | Not stated | 547 | Obesity |
| Katole et al., 2024 ( | Critically low | Cureus 2024 | 7 trials | < 18 | 567 | Obesity |
| Kotecha et al., 2025 ( | High | JAMA Pediatr 2025 | 18 trials | 6 to17 | 1402 | DM/obesity |
| Romariz et al., 2025 ( | High | Pediatr Res 2025 | 11 trials | 6 to 16 | 1024 | Obesity |
| Ryan et al., 2021 ( | Moderate | J Pediatr 2021 | 9 studies | Not stated | 474 | Obesity |
| Sedenho-Prado et al., 2025 ( | High | Int J Obes 2025 | 8 studies | ≤ 18 | 715 | Obesity |
| Wang et al., 2024 ( | High | Obes Rev 2024 | 15 trial | Not stated | 1286 y | DM/obesity |
| Yugar et al., 2024 ( | High | Diabetol Metab Syndr 2024 | 5 studies | 10-18 | 415 | Diabetes |
| Outcome | Studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Certainty of evidence |
|---|---|---|---|---|---|---|---|---|
| Body weight | 11 | Trials=11 | serious | Serious ( | Not serious | Not serious | None | ⨁⨁◯◯ LOW |
| HbA1c | 6 | Trials=6 | Serious | Not serious ( | Not serious | Not serious | None | ⨁⨁◯◯ LOW |
| BMI z | 5 | Trials=3 | serious | Very serious ( | Not serious | Not serious | None | ⨁⨁◯◯ LOW |
| GIT adverse events | 6 | Trials=3 | Serious | Not serious ( | Not serious | Not serious | None | ⨁⨁◯◯ LOW |
| Systolic blood pressure | 5 | Trials=3 | serious | Serious ( | Not serious | Not serious | None | ⨁⨁◯◯ LOW |
| Hypoglycemia | 3 | Trials=2 | Serious | Not serious ( | Not serious | Not serious | None | ⨁⨁◯◯ LOW |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Diabetes Management and Research · Pancreatic function and diabetes
Introduction
Diabetes and obesity are major health concerns, with diabetes mellitus affecting 10.5% globally. The prevalence is expected to increase in 2045 by 21.1% in middle-income countries, and 12.1% in high-income countries (1). Recent data from the International Diabetes Federation indicate that the Middle East and North Africa region (MENA) currently bears the world’s highest age-adjusted prevalence of diabetes among adults at 12.2%. This burden is expected to rise to 13.3% by 2030, and projections suggest that by 2045, approximately one in eight individuals in the region will be living with diabetes (2). In some countries in this diabetes super-region, type 2 DM affected more than a quarter of the adult population in Saudi Arabia, with an overall prevalence of about 28% according to 2016 and 2022 data. Adults older than 40 years showed a substantially higher likelihood of having T2DM, with nearly double the risk compared with those under 40 years of age, indicating age as a strong determinant of disease burden in the general population (3). Obesity affects 20% of children and adolescents, with a parallel increase in type 2 DM in the young age group (2). A systematic review and meta-analysis reported that the pooled prevalence of obesity among children and adolescents was 8.5% (95% CI 8.2–8.8), highlighting a substantial public health burden. Despite the ongoing rise in diabetes and obesity rates. Nonetheless, significant challenges hinder the translation of existing evidence into routine clinical practice. These barriers include poor integration of obesity and diabetes services across different levels of care within healthcare systems, inadequate training of healthcare professionals, and limited affordability and accessibility of prevention and treatment services (4). The increasing rate of type 2 DM in children and adolescents is mainly due to the increasing obesity from an unhealthy diet and lack of physical activity in genetically predisposed people (5–7). The number of newly diagnosed type 2 diabetes cases in children and adolescents was 41,600 in 2017 worldwide (8). Genome-wide association studies have revealed multiple genetic regions linked to the risk of type 2 DM, with variants in transcription factor 7-like 2, peroxisome proliferator-activated receptor gamma, and fat mass and obesity–associated genes influencing insulin secretion and sensitivity, thereby highlighting the genetic basis of disease susceptibility (9). Children and adolescents with type 2 DM have poor glycemic control and are more prone to diabetes microvascular complications (10). In addition, type 2 DM in the pediatric age group is associated with several cardiovascular risk factors, including hypertension, dyslipidemia, and metabolic-associated liver disease (11). Because of the above, the use of GLP-1 agonists is on the rise worldwide.
GLP-1 agonists use among patients with type 2 DM started with the approval of the twice/daily exenatide in 2005. Many classes were developed in the following years. Liraglutide injection once daily and semaglutide once/week subcutaneous injection were approved in 2017 for glycemic control, and in 2021 for the treatment of obesity (12–14). Liraglutide is currently approved for use in pediatrics, with some concerns regarding treatment adherence. Although semaglutide was approved and showed better glycemic and weight control. However, the recruitment of children for controlled trials is challenging (15–17). Other GLP-1 agonists that received approval for use in the pediatric age group are exanetide slow-release and dulaglutide. GLP-1 agonists were shown to reduce glycemic parameters, reduce weight, and improve obesity associated comorbidities (18). The use of GLP-1 agonists was shown to reduce weight and improve glycemic control in children through appetite reduction and slowing gastric emptying. GLP-1 agonists act on the brain by stimulating specific receptors in central nervous system regions such as the hypothalamus, leading to enhanced feelings of fullness. They also influence gastrointestinal function by slowing gastric emptying, which helps blunt post-meal rises in lipids and carbohydrates. This gastric effect is partly regulated through neural signaling pathways involving the vagal afferent nerves, brainstem nuclei such as the nucleus of the solitary tract, and vagal efferent fibers (19). In addition, they increase insulin secretion and decrease glucagon secretion. In large single trials, such as SCALE Teens (liraglutide) and STEP TEENS (semaglutide), reductions of 4–16% in BMI were observed over 56–68 weeks. However, because of ongoing growth and pubertal development, extrapolation from adult data must be cautious (20–22). The findings from earlier meta-analyses, demonstrated a consistent reduction in body weight. However, evidence related to glycemic control remains inconsistent across studies, and several meta-analyses did not evaluate key clinical outcomes such as body mass index z score, systolic blood pressure, overall adverse events, and hypoglycemia, which are critical in managing pediatric obesity and diabetes. Consequently, synthesizing all available evidence through a comprehensive umbrella review is highly warranted. This umbrella review aimed to assess the role of GLP-1 agonists on body weight, HbA1c, waist circumference, BMI z, and systolic blood pressure in children and adolescents.
Methods
This umbrella review was conducted according to the PRISMA guidelines with additional methodological considerations specific to umbrella reviews. This umbrella review aimed to study the effects of GLP-1 agonists on pediatric body weight, HbA1c, BMI z, SBP, gastrointestinal adverse events, and hypoglycemia in children with obesity/type 2 DM.
Inclusion criteria
We included systematic reviews and meta-analyses assessing the role of GLP-1 agonists on weight, HbA1c, BMI z, SBP, gastrointestinal adverse events, and hypoglycemia in children with obesity/type 2 DM. The studies must report the mean difference, standard mean difference, odds ratios, hazard ratios, and risk ratios or equivalent with corresponding 95% confidence intervals for the outcomes.
Exclusion criteria
Observational studies, trials, cross-sectional studies, case-control studies, opinion, editorials, letters to the editors, and narrative reviews were not included. In addition, studies not reporting the mean difference, standard mean difference, odds ratios, hazard ratios, and risk ratios for the outcomes were not included.
Outcome measures
The outcomes measures were the effects of GLP-1 agonists on pediatric body weight, HbA1c, BMI z, SBP, gastrointestinal adverse events, and hypoglycemia in children with obesity/type 2 DM.
Literature search
We reviewed the literature in PubMed/MEDLINE, Web of Science, and Cochrane Library from inception up to December 2025 using the following terms: GLP-1 agonists, semaglutide, tirzepatide, liraglutide, exenatide, children, obesity, adolescents, BMI z, blood pressure, gastrointestinal, adverse events, hypoglycemia, and HbA1c. We retrieved 1600 articles (1312 articles in PubMed, 227 in the Web of Science, and 61 in Cochrane Library), of which 1402 remained after the removal of duplications, and 44 reviews and meta-analyses full texts were reviewed. Out of the 44 reviews found, only 11 meta-analyses were included in the final results Figure 1.
Studies evaluating the role of GLP-1 agonists in children with obesity/type 2 diabetes. The PRISMA Chart.
Data extraction
The data from 11 systematic reviews were reported in Table 1. The author’s name, year of publication, weight reduction, BMI z, SBP, HbA1c, gastrointestinal adverse events, and hypoglycemia were reported Tables 1, 2.
The quality assessment of the included meta-analyses
The quality of the included meta-analyses was assessed by the Measurement Tool to Assess Systematic Reviews, version 2 (34) Table 3.
Overlap determination
The Overlap of primary studies across meta-analyses was evaluated by identifying shared cohorts and calculating the Corrected Covered Area (CCA) (35). There were 11 meta-analyses with 78 trials included; the duplicates were 66, with only 12 unique trials. Therefore, the Corrected Covered Area (55% (very high overlap).
Statistical analysis
We used the RevMan System from Cochrane (version 5.4, Oxford) for data analysis. The retrieved mean differences (MD) for weight, HbA1c, SBP, and BMI z, odds ratios, and hazard ratios for gastrointestinal side effects and hypoglycemia were converted to Log ratios and standard errors (SE). MD, Log ratios, and SE were entered using the random effect to generate the forest plots at 95% CI, and a standard error of 5%. A funnel plot was generated for the weight and HbA1c due to the significant heterogeneity observed. A heterogeneity of 25% was considered mild, and heterogeneity of ≥ 50% was considered significant. A subgroup analysis was conducted for the HbA1c outcome to locate the source of heterogeneity. A P-value of < 0.05 was considered significant.
Results
A meta-analysis of eleven studies demonstrated a statistically significant reduction in body weight in the GLP-1 agonists compared with controls. Using a random-effect model, the pooled mean difference (MD)=0.11, 95% CI 0.05–0.25; Z = 5.30, P < 0.00001. There was evidence of between-study heterogeneity (χ^2^ = 42.38, df = 10, P < 0.001; I^2^ = 076%). A fixed-effects model produced identical results, indicating robust findings independent of the analytical approach. Weight reduction was significant after removing studies with a significant contribution to heterogeneity, MD = 0.17, 95% CI 0.09–0.34; Z = 5.07, P < 0.00001. There was no evidence of between-study heterogeneity (χ^2^ = 1.63, df = 4, P = 0.80; I^2^ = 0%) (Figures 2A–C).
(A) The effect of GLP-1 agonists on body weight in children (forest plot). (B) The effect of GLP-1 agonists on body weight in children (funnel plot). (C) The effect of GLP-1 agonists on weight in children (forest plot, no heterogeneity).
Regarding the HbA1c, GLP-1 agonists reduced it with a significant statistical difference, MD = 0.65, 95% CI 0.53–0.80; P< 0.001, and Z = 4.09. A significant heterogeneity was found (χ^2^ = 26.60, df = 5, P < 0.001; I^2^ = 81%). A subgroup analysis showed a significant HbA1c reduction, MD = 0.71, 95% CI 0.62–0.81; P < 0.001, and Z = 5.00. No significant heterogeneity was found (χ^2^ = 2.66, df = 3, P = 0.45; I^2^ = 0%) (Figures 3A–C).
(A) The effect of GLP-1 agonists on HbA1c in children. (B) The effect of GLP-1 agonists on HbA1c in children (funnel plot). (C) The effect of GLP-1 agonists on HbA1c in children (Forest Plot, no heterogeneity).
Only 6 studies assessed the BMI z; there was a significant statistical reduction in GLP-1 agonists compared to controls, MD = 0.85, 95% CI 0.81–0.90; P < 0.001, and Z = 5.55). No significant heterogeneity was found (χ^2^ = 4.02, df = 4, P = 0.40; I^2^ = 1%) Figure 4.
The effect of GLP-1 agonists on BMI z in children.
The SBP was significantly reduced by GLP-1 agonists, MD = 0.19, 95% CI 0.04–83; P, 0.03, and Z = 2.22. A significant heterogeneity was found (χ^2^ = 55.88, df = 4, P < 0.001; I^2^ = 93%). (Figures 5A, B). The systolic reduction of blood pressure remained significant in a subgroup analysis removing studies with high heterogeneity, MD = 0.10, 95% CI 0.06–17; P <0.001, and Z = 8.38. No significant heterogeneity was found (χ^2^ = 1.64, df = 3, P = 0.65; I^2^ = 0%) (Figures 5A, B).
(A) The effect of GLP-1 agonists on systolic blood pressure in children. (B) The effect of GLP-1 agonists on systolic blood pressure in children (no heterogeneity).
The total adverse events were not different between GLP-1 agonists and controls (log ratios=1.29, 95% CI 0.80–2.09; P = 0.03, and Z = 1.03). A significant heterogeneity was found (χ^2^ = 33.58, df = 5, P < 0.001; I^2^ = 85%). However, the total side effects were higher in GLP-1 agonists after removing studies with high heterogeneity (log ratios=1.45, 95% CI 1.12–1.87; P = 0.005, and Z = 2.82). No significant heterogeneity was found (χ^2^ = 1.32, df = 2, P = 0.52; I^2^ = 0%) (Figures 6A, B).
(A) The effect of GLP-1 agonists on total adverse events in children. (B) The effect of GLP-1 agonists on total adverse events in children (no heterogeneity).
Hypoglycemia was not increased in GLP-1 agonists compared to controls (log ratios=1.26, 95% CI 0.59–2.70; P = 0.56, and Z = 0.59). No significant heterogeneity was found (χ^2^ = 3.81, df = 2, P = 0.15; I^2^ = 48%). The results remained insignificant after the elimination of the study with high contribution to heterogeneity (log ratios=0.81, 95% CI 0.35–1.89; P = 0.63, and Z = 0.48). No significant heterogeneity was found (χ^2^ = 0.71, df = 1, P = 0.63; I^2^ = 48%) (Figures 7A, B).
(A) The effect of GLP-1 agonists on hypoglycemia in children. (B) The effect of GLP-1 agonists on hypoglycemia in children.
Discussion
In this umbrella review, GLP-1 agonists were more effective than control in reducing body weight, HbA1c, BMI z, and SBP, MD = 0.11, 95% CI 0.05–0.25, MD = 0.65, 95% CI 0.53–0.80, MD = 0.85, 95% CI 0.81–0.90, and MD = 0.19, 95% CI 0.04–83, respectively. The total adverse events and hypoglycemia were not different, log ratios=1.29, 95% CI 0.80–2.09, and log ratios=1.26, 95% CI 0.59–2.70, respectively.
Evidence from systematic reviews and meta-analyses
Previous meta-analyses have demonstrated significant reductions in body weight (23–27, 29–33, 36). However, findings related to glycemic control remain inconsistent across studies. Moreover, several meta-analyses have not comprehensively evaluated other clinically relevant outcomes, including BMI z score, SBP, total adverse events, and hypoglycemia—parameters that are critical for the optimal management of pediatric obesity and type 2 DM. Consequently, an umbrella review synthesizing all available evidence across these outcomes is both timely and highly warranted.
Regarding the comparative effectiveness of GLP-1 agonists, semaglutide currently has the strongest evidence supporting its efficacy in weight reduction, whereas liraglutide has demonstrated more modest effects, and data on tirzepatide remain preliminary (37). In the context of type 2 DM, liraglutide is the most well-established agent, evidence for tirzepatide is steadily emerging, and data on semaglutide are still limited (38).
Obesity is a chronic inflammatory disease and a biological disease of energy regulation. The pathophysiology is complex and includes genetic, societal, and neuroendocrine interplay. Therefore, the use of GLP-1 agonists is acknowledged because they act in the gastrointestinal tract (39, 40). The use of GLP-1 agonists in children with obesity and type 2 DM is justifiable due to the current evidence.
There is a marked and continuing rise in childhood and adolescent obesity. Currently, hundreds of millions worldwide are either overweight or obese. The prevalence jumped from 8% in 1990 to 20% in 2022, together with parallel increases in youth-onset type 2 DM (8, 41, 42). This trend creates a strong clinical and public-health rationale for considering evidence-based pharmacologic options such as GLP-1 agonists as adjuncts to lifestyle and prevention strategies.
Although lifestyle interventions can result in modest weight reduction, their long-term sustainability remains limited at both individual and population levels. By contrast, randomized controlled trials in adolescents have consistently shown that GLP-1 agonists achieve substantially greater and clinically meaningful reductions in BMI, accompanied by significant improvements in cardiometabolic risk markers, compared with placebo combined with lifestyle modification. The adverse effects associated with GLP-1 agonists are generally acceptable and predominantly gastrointestinal in nature. Accordingly, GLP-1 agonists may be considered for selected adolescents and young individuals with severe obesity or obesity accompanied by comorbidities, with the potential to reduce short-term cardiometabolic risk and to prevent or delay progression to type 2 DM and its related complications (21, 43). The rapidly rising incidence and poorer prognosis of youth-onset Type 2DM mean therapies that safely improve weight and glycemic risk factors could alter lifetime risk trajectories when used under specialist supervision alongside comprehensive care (21, 43, 44).
Evidence from this umbrella review confirmed the benefits of GLP-1 agonists in obesity and diabetes in the short term. In addition, GLP-1 agonists showed benefits in MBMI z and SBP. Moreover, GLP-1 agonists were tolerable, and the total adverse events and hypoglycemia were similar to those of the control. However, there is an increasing concern about medium and long-term safety data, including the effects on growth, pubertal timing, and bone outcomes (12, 45). Importantly, most randomized trials on GLP-1 agonists used in children have a short duration (56–68 weeks), and therefore, they could not assess the effects of puberty timing, final adult height, and bone outcomes that require long-term data. Hypoglycemia with GLP-1 agonist use is rare and mild (5% and 15-20% when combined with insulin and sulphonylurea); no severe hypoglycemia requiring assistance was reported (11, 46). Another major issue is the rising concerns about the association of GLP-1 agonists, depression, and suicidal ideation. Evidence from randomized trials and observational studies showed no association and a possible reduction in the short term. However, long-term results are lacking (47). Potential nutritional deficiencies and effects on peak bone mass are biologically plausible (reduced intake, GI losses, reduced mechanical loading), so active monitoring of growth, diet, and bone-health risk factors is recommended (48). Long-term studies (years to final adult height and bone mass) are needed (49, 50).
Overall, the glycemic efficacy of GLP-1 agonists in children and adolescents with type 2 DM is well established. Consequently, GLP-1 agonists represent a valuable adjunctive therapy for youth with Type 2 DM who exhibit suboptimal glycemic control with metformin or insulin alone. GLP-1agonists (liraglutide, semaglutide, exenatide) are effective adjuncts for pediatric obesity and Type 2 DM, improving weight, glycemic control, and BMI z with modest SBP lowering. Long-term safety regarding growth, puberty, and bone development requires further study. Use should remain individualized and integrated with behavioral therapy, nutrition, and physical activity programs.
The strength of this umbrella review is that it is the first to combine the evidence from 11 meta-analyses (5 were high quality, and three moderate quality). We assessed 4 important morbidities in children with obesity/type 2 DM, including body weight, HbA1c, BMI z, and SBP. In addition, we gave an insight into the total side effects and hypoglycemia.
Limitations
Most pediatric trials last <1 year, and some of the studies (3) showed low quality. The significant overlap (68 out of 78 trials) significantly limited this umbrella review.
Conclusion
Based on the low certainty evidence, GLP-1 agonists may improve weight, HbA1c, BMI z-score, and SBP in adolescents with obesity and youth with type 2 DM. Short-term safety outcomes appear acceptable, with no consistent signals of increased adverse events or hypoglycemia compared with standard care. However, the certainty of evidence is limited by study heterogeneity, imprecision, and the lack of long-term pediatric safety data. While semaglutide demonstrates potential comparative advantages in weight-related outcomes, confidence in this finding remains restricted. Consequently, additional well-designed, adequately powered, and long-duration trials are essential before drawing definitive conclusions or informing long-term clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Audrain-Mc Govern J Benowitz NL . Cigarette smoking, nicotine, and body weight. Clin Pharmacol Ther. (2011) 90:164–8. doi: 10.1038/clpt.2011.105, PMID: 21633341 PMC 3195407 · doi ↗ · pubmed ↗
- 2International Diabetes Federation . IDF diabetes atlas. 9th ed. Brussels, Belgium: International Diabetes Federation (2019). Available online at: https://www.diabetesatlas.org (Accessed December 25, 2025).
- 3Alwadeai KS Alhammad SA . Prevalence of type 2 diabetes mellitus and related factors among the general adult population in Saudi Arabia between 2016-2022: A systematic review and meta-analysis of the cross-sectional studies. Med (Baltimore). (2023) 102:e 34021. doi: 10.1097/MD.0000000000034021, PMID: 37327272 PMC 10270537 · doi ↗ · pubmed ↗
- 4Hamman RF Bell RA Dabelea D D’Agostino RB Jr Dolan L Imperatore G . The SEARCH for Diabetes in Youth study: rationale, findings, and future directions. Diabetes Care. (2014) 37:3336–44. doi: 10.2337/dc 14-0574, PMID: 25414389 PMC 4237981 · doi ↗ · pubmed ↗
- 5Amutha A Mohan V . Diabetes complications in childhood and adolescent onset type 2 diabetes-a review. J Diabetes Complications. (2016) 30:951–7. doi: 10.1016/j.jdiacomp.2016.02.009, PMID: 26970673 · doi ↗ · pubmed ↗
- 6Kumar A Gangwar R Zargar AA Kumar R Sharma A . Prevalence of diabetes in India: A review of IDF diabetes atlas 10th edition. Curr Diabetes Rev. (2024) 20:e 130423215752. doi: 10.2174/1573399819666230413094200, PMID: 37069712 · doi ↗ · pubmed ↗
- 7GBD 2021 Adolescent BMI Collaborators . Global, regional, and national prevalence of child and adolescent overweight and obesity 1990-2021, with forecasts to 2050: a forecasting study for the Global Burden of Disease Study 2021. Lancet. (2025) 405:785–812. doi: 10.1016/S 0140-6736(25)00397-6, PMID: 40049185 PMC 11920006 · doi ↗ · pubmed ↗
- 8Wu H Patterson CC Zhang X Ghani RBA Magliano DJ Boyko EJ . Worldwide estimates of incidence of type 2 diabetes in children and adolescents in 2021. Diabetes Res Clin Pract. (2022) 185:109785. doi: 10.1016/j.diabres.2022.109785, PMID: 35189261 · doi ↗ · pubmed ↗