The effect of nitrates in patients with coronary artery disease across different left ventricular ejection fractions
Hui Liu, Wei Liu, Yalin Cao, Zongzhuang Li, Piao Zheng

TL;DR
This study finds that nitrates may increase risk of death and heart events in patients with coronary artery disease and low heart function.
Contribution
The study reveals that nitrates are linked to worse outcomes specifically in patients with reduced left ventricular ejection fraction.
Findings
Nitrates at discharge were associated with higher death and MACE rates in patients with LVEF <45%.
No significant associations were found in patients with LVEF 45%–55% or >55%.
The study suggests cautious use of nitrates in patients with reduced LVEF.
Abstract
Long-acting nitrates are widely prescribed in coronary artery disease (CAD), yet their association with long-term outcomes remains controversial. Whether left ventricular ejection fraction (LVEF) modifies this relationship has not been well characterized. We conducted a single-center retrospective cohort study using the Guizhou Provincial People's Hospital CAD database. Adults (≥18 years) who underwent coronary angiography between July 2012 and September 2016 and met angiographic criteria for CAD (≥50% stenosis in ≥1 proximal epicardial coronary artery) were eligible if LVEF and discharge medications were available. Patients were stratified by LVEF (<45%, 45%–55%, >55%) and by discharge prescription of any nitrate (mononitrate or dinitrate). The primary endpoint was all-cause death. The secondary endpoint was major adverse cardiovascular events (MACE), defined as a composite of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
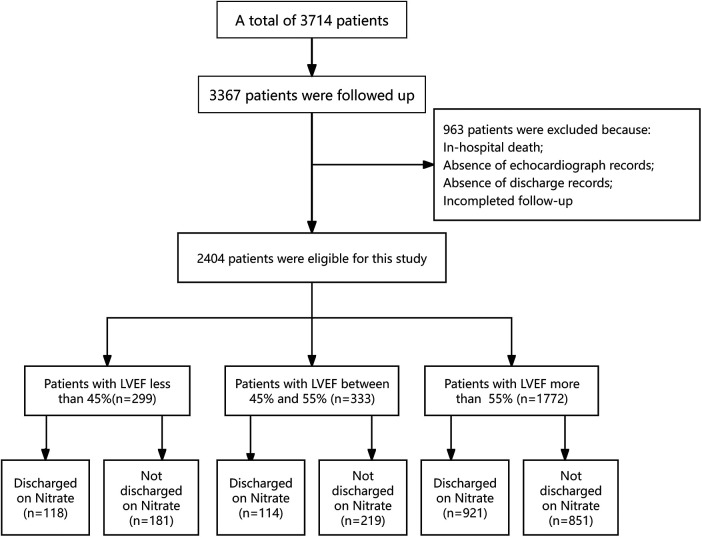 Figure 1
Figure 1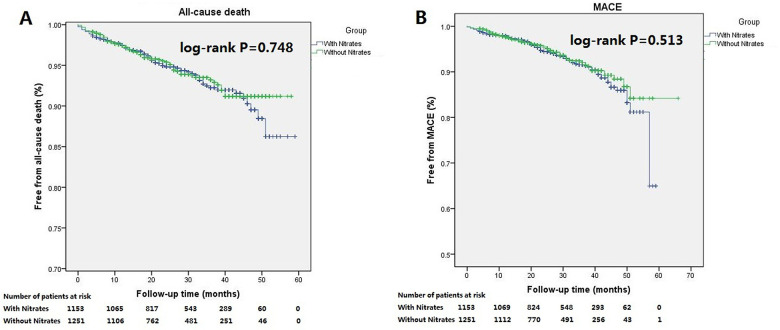 Figure 2
Figure 2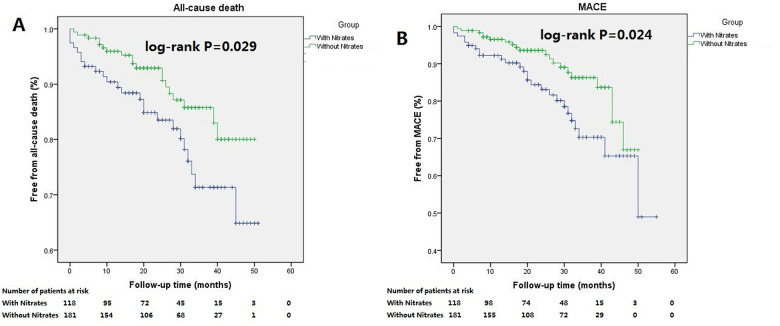 Figure 3
Figure 3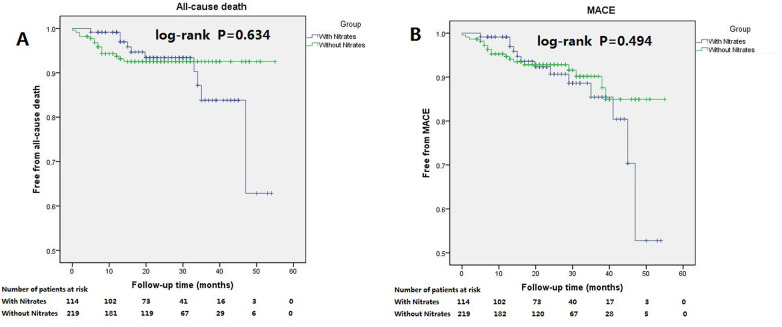 Figure 4
Figure 4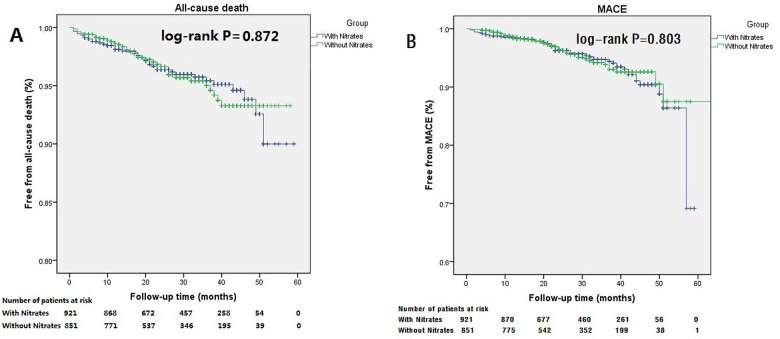 Figure 5
Figure 5| Variables | Total ( |
| LVEF < 45% ( |
| 45% ≤ LVEF ≤ 55% ( |
| LVEF > 55% ( |
| ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| With nitrates | Without nitrates | With nitrates | Without nitrates | With nitrates | Without nitrates | With nitrates | Without nitrates | |||||
| No. of patients | 1,153 (48.0) | 1,251 (52.0) | 118 (39.5) | 181 (60.5) | 114 (34.2) | 219 (65.8) | 921 (52.0) | 851 (48.0) | ||||
| Male, | 905 (78.5) | 1,007 (80.5) | 0.224 | 97 (82.2) | 159 (87.8) | 0.174 | 92 (80.7) | 186 (84.9) | 0.324 | 71.6 (77.7) | 662 (77.8) | 0.980 |
| Age, years | 65.3 (10.1) | 63.8 (10.7) | 0.000 | 65.4 (10.0) | 64.8 (10.8) | 0.630 | 63.2 (11.7) | 62.1 (11.1) | 0.392 | 65.5 (9.8) | 64.0 (10.6) | 0.002 |
| ACS, | 829 (71.9) | 862 (69.0) | 0.118 | 82 (69.5) | 129 (71.3) | 0.741 | 85 (74.6) | 157 (71.7) | 0.577 | 662 (71.9) | 577 (67.8) | 0.062 |
| History of MI, | 266 (23.1) | 404 (32.3) | 0.000 | 55 (46.6) | 92 (50.8) | 0.476 | 41 (36.0) | 100 (45.7) | 0.089 | 170 (18.5) | 212 (24.9) | 0.001 |
| History of PCI, | 139 (12.1) | 147 (11.8) | 0.818 | 15 (12.7) | 22 (12.2) | 0.886 | 12 (10.5) | 20 (9.1) | 0.682 | 112 (12.2) | 105 (12.3) | 0.909 |
| Hypertension, | 684 (59.3) | 656 (52.4) | 0.001 | 68 (57.6) | 73 (40.3) | 0.003 | 59 (51.8) | 101 (46.1) | 0.329 | 557 (60.5) | 482 (56.6) | 0.101 |
| Diabetes milletus, | 257 (22.3) | 278 (22.2) | 0.968 | 32 (27.1) | 38 (21.0) | 0.222 | 31 (27.2) | 50 (22.8) | 0.379 | 194 (21.1) | 190 (22.3) | 0.519 |
| Current Smoker, | 300 (26.0) | 397 (31.7) | 0.002 | 33 (28.0) | 64 (35.4) | 0.182 | 33 (28.9) | 80 (36.5) | 0.166 | 234 (25.4) | 253 (29.7) | 0.042 |
| BMI, kg/m2 | 24.3 (3.3) | 24.1 (3.0) | 0.088 | 23.9 (3.3) | 23.8 (2.7) | 0.728 | 24.6 (3.9) | 24.1 (2.7) | 0.203 | 24.4 (3.2) | 24.2 (3.1) | 0.275 |
| Waist-Hip ratio | 0.96 (0.66) | 0.96 (0.69) | 0.533 | 0.96 (0.53) | 0.95 (0.49) | 0.167 | 0.96 (0.48) | 0.96 (0.52) | 0.336 | 0.96 (0.69) | 0.96 (0.76) | 0.986 |
| LVEF, % | 61.7 (11.1) | 58.8 (11.8) | 0.000 | 36.6 (6.2) | 36.7 (6.1) | 0.890 | 50.1 (3.2) | 50.3 (3.1) | 0.717 | 66.3 (5.4) | 65.6 (5.1) | 0.009 |
| Serum creatinine, µmol/L | 96.5 (62.3) | 91.9 (41.5) | 0.030 | 98.8 (32.4) | 98.6 (43.1) | 0.956 | 99.6 (81.6) | 97.0 (66.3) | 0.752 | 95.9 (62.5) | 89.1 (31.5) | 0.004 |
| Glucose, mmol/L | 6.7 (2.9) | 7.2 (3.5) | 0.000 | 7.4 (3.9) | 7.4 (3.6) | 0.947 | 7.6 (3.6) | 8.3 (4.2) | 0.126 | 6.5 (2.6) | 6.9 (3.3) | 0.007 |
| Total cholesterol, mmol/L | 4.1 (1.1) | 4.1 (1.1) | 0.539 | 4.0 (1.0) | 4.1 (1.1) | 0.672 | 4.1 (1.2) | 4.2 (1.4) | 0.288 | 4.1 (1.1) | 4.1 (1.0) | 0.904 |
| Triglyceride, mmol/L | 1.8 (1.1) | 1.7 (1.2) | 0.462 | 1.6 (0.8) | 1.6 (1.0) | 0.674 | 1.7 (0.9) | 1.9 (1.6) | 0.235 | 1.8 (1.1) | 1.7 (1.1) | 0.131 |
| HDL-C, mmol/L | 1.1 (0.4) | 1.2 (0.4) | 0.458 | 1.1 (0.3) | 1.1 (0.3) | 0.824 | 1.1 (0.3) | 1.1 (0.3) | 0.358 | 1.2 (0.4) | 1.2 (0.4) | 0.349 |
| LDL-C, mmol/L | 2.4 (0.9) | 2.4 (0.9) | 0.314 | 2.4 (0.9) | 2.4 (0.9) | 0.952 | 2.4 (1.1) | 2.5 (1.0) | 0.624 | 2.3 (0.9) | 2.4 (0.9) | 0.545 |
| Systolic blood pressure on admission, mmHg | 133.0 (20.5) | 128.8 (21.5) | 0.000 | 127.1 (20.1) | 121.3 (21.4) | 0.020 | 129.7 (20.6) | 124.5 (21.5) | 0.036 | 134.2 (20.3) | 131.5 (20.9) | 0.006 |
| Diastolic blood pressure on admission, mmHg | 77.2 (11.9) | 75.9 (12.5) | 0.009 | 76.7 (11.5) | 75.4 (14.1) | 0.400 | 76.7 (12.2) | 75.5 (13.1) | 0.457 | 77.3 (12.0) | 76.1 (12.0) | 0.029 |
| Patients with stent implantation, | 702 (60.9) | 906 (72.4) | 0.000 | 64 (55.1) | 126 (69.6) | 0.011 | 63 (55.3) | 171 (78.1) | 0.000 | 571 (62.0) | 600 (70.5) | 0.000 |
| Number of stents | 1.2 (1.3) | 1.3 (1.2) | 0.139 | 1.13 (1.32) | 1.30 (1.30) | 0.253 | 1.2 (1.4) | 1.3 (1.1) | 0.334 | 1.2 (1.3) | 1.3 (1.2) | 0.489 |
| Number of lesions | ||||||||||||
| One vessel, | 481 (41.8) | 580 (46.4) | 0.021 | 36 (30.5) | 70 (38.7) | 0.149 | 41 (36.0) | 101 (46.1) | 0.075 | 404 (43.9) | 409 (48.2) | 0.072 |
| Two vessels, | 276 (24.0) | 329 (26.3) | 0.179 | 31 (26.3) | 46 (25.4) | 0.868 | 26 (22.8) | 59 (26.9) | 0.412 | 219 (23.8) | 224 (26.4) | 0.211 |
| Three vessels, | 273 (23.7) | 243 (19.5) | 0.011 | 40 (33.9) | 46 (25.4) | 0.113 | 37 (32.5) | 39 (17.8) | 0.003 | 196 (21.3) | 158 (18.6) | 0.157 |
| Left main artery, | 122 (10.6) | 97 (7.8) | 0.016 | 11 (9.3) | 19 (10.5) | 0.741 | 10 (8.8) | 20 (9.1) | 0.913 | 101 (11.0) | 58 (6.8) | 0.002 |
| Medicines before admission | ||||||||||||
| Aspirin, | 493 (42.8) | 439 (35.1) | 0.000 | 49 (41.5) | 56 (30.9) | 0.061 | 39 (34.2) | 54 (24.7) | 0.065 | 405 (44.0) | 329 (38.7) | 0.023 |
| Clopedogrel, | 254 (22.0) | 260 (20.8) | 0.457 | 25 (21.2) | 37 (20.4) | 0.877 | 18 (15.8) | 33 (15.1) | 0.862 | 211 (22.9) | 190 (22.3) | 0.769 |
| β-Blockers, | 344 (29.8) | 325 (26.0) | 0.035 | 31 (26.3) | 42 (23.2) | 0.546 | 22 (19.3) | 26 (11.9) | 0.067 | 291 (31.6) | 257 (30.2) | 0.525 |
| Statin, | 320 (27.8) | 293 (23.4) | 0.015 | 32 (27.1) | 37 (20.4) | 0.180 | 22 (19.3) | 25 (11.4) | 0.050 | 266 (28.9) | 231 (27.1) | 0.416 |
| ACEI/ARB, | 285 (24.7) | 252 (20.1) | 0.007 | 23 (19.5) | 29 (16.0) | 0.439 | 26 (22.8) | 25 (11.4) | 0.006 | 236 (25.6) | 198 (23.3) | 0.249 |
| CCB, | 325 (28.2) | 249 (19.9) | 0.000 | 20 (16.9) | 23 (12.7) | 0.307 | 24 (21.1) | 21 (9.6) | 0.004 | 281 (30.5) | 205 (24.1) | 0.002 |
| Medicines at discharge | ||||||||||||
| Aspirin, | 1,097 (95.1) | 1,187 (94.9) | 0.771 | 107 (90.7) | 172 (95.0) | 0.141 | 108 (94.7) | 209 (95.4) | 0.778 | 882 (95.8) | 806 (94.7) | 0.297 |
| Clopedogrel, | 1,065 (92.4) | 1,146 (91.6) | 0.493 | 108 (91.5) | 167 (92.3) | 0.818 | 105 (92.1) | 204 (93.2) | 0.726 | 852 (92.5) | 775 (91.1) | 0.270 |
| Statin, | 1,029 (89.2) | 1,190 (95.1) | 0.000 | 109 (92.4) | 174 (96.1) | 0.158 | 99 (86.8) | 206 (94.1) | 0.024 | 821 (89.1) | 810 (95.2) | 0.000 |
| CCB, | 375 (32.5) | 305 (24.4) | 0.000 | 20 (16.9) | 19 (10.5) | 0.105 | 26 (22.8) | 28 (12.8) | 0.019 | 329 (35.7) | 258 (30.3) | 0.016 |
| ACEI/ARB, | 675 (58.5) | 749 (59.9) | 0.508 | 73 (61.9) | 97 (53.6) | 0.158 | 67 (58.8) | 134 (61.2) | 0.669 | 535 (58.1) | 518 (60.9) | 0.234 |
| β-Blocker, | 821 (71.2) | 838 (67.0) | 0.025 | 85 (72) | 115 (63.5) | 0.127 | 75 (65.8) | 152 (69.4) | 0.501 | 661 (71.8) | 571 (67.1) | 0.033 |
| Variates | All-cause death | MACE | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI |
| HR | 95% CI |
| |
| Discharged on nitrates | 1.08 | 0.75–1.54 | 0.695 | 1.20 | 0.87–1.66 | 0.269 |
| Age | 1.07 | 1.05–1.10 | 0.000 | 1.02 | 1.00–1.03 | 0.114 |
| LVEF | 0.96 | 0.95–0.98 | 0.000 | 0.96 | 0.95–0.98 | 0.000 |
| Serum creatinine | 1.00 | 1.00–1.01 | 0.000 | 1.00 | 1.00–1.00 | 0.090 |
| White blood cell | 1.09 | 1.03–1.15 | 0.005 | 1.05 | 0.99–1.10 | 0.098 |
| Stent implantation | 0.56 | 0.38–0.81 | 0.002 | 0.59 | 0.42–0.82 | 0.002 |
| Left main artery disease | 1.48 | 0.80–2.74 | 0.220 | 1.87 | 1.12–3.14 | 0.017 |
| Medicines before admission | ||||||
| β-Blocker | 0.59 | 0.36–0.97 | 0.036 | 0.61 | 0.39–0.95 | 0.029 |
| Medicines at discharge | ||||||
| Aspirin | 0.43 | 0.25–0.74 | 0.002 | 0.54 | 0.29–0.98 | 0.043 |
| All-cause death | MACE | ||||||
|---|---|---|---|---|---|---|---|
| Variates | HR | 95% CI |
| Variates | HR | 95% CI |
|
| Discharged on nitrates | 2.14 | 1.15–3.96 | 0.016 | Discharged on nitrates | 1.91 | 1.07–3.43 | 0.03 |
| Age | 1.06 | 1.02–1.10 | 0.001 | ||||
| Current smoking | 2.37 | 1.16–4.83 | 0.018 | ||||
| Serum Creatinine | 1.01 | 1.01–1.02 | 0.000 | ||||
| Variates | All-cause death | MACE | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI |
| HR | 95% CI |
| |
| Discharged on nitrates | 0.63 | 0.20–1.96 | 0.426 | 1.10 | 0.42–2.88 | 0.853 |
| Age | 1.11 | 1.02–1.20 | 0.017 | 1.07 | 1.01–1.14 | 0.025 |
| Serum creatinine | 1.01 | 1.00–1.01 | 0.003 | 1.00 | 1.00–1.01 | 0.034 |
| Medicines at discharge | ||||||
| Aspirin | 0.04 | 0.01–0.22 | 0.000 | 0.16 | 0.03–0.80 | 0.026 |
| Variate | All-cause death | MACE | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI |
| HR | 95% CI |
| |
| Discharged on nitrates | 0.83 | 0.49–1.41 | 0.495 | 0.97 | 0.60–1.56 | 0.891 |
| Age | 1.09 | 1.05–1.13 | 0.000 | 1.00 | 0.97–1.02 | 0.790 |
| Serum creatinine | 1.00 | 1.00–1.01 | 0.002 | 1.00 | 1.00–1.01 | 0.166 |
| White blood cell | 1.15 | 1.06–1.25 | 0.001 | 1.06 | 0.97–1.15 | 0.193 |
| Stent implantation | 0.50 | 0.28–0.88 | 0.015 | 0.53 | 0.32–0.88 | 0.014 |
| Left main artery disease | 2.25 | 0.96–5.27 | 0.063 | 3.07 | 1.51–6.23 | 0.002 |
| Medicines at discharge | ||||||
| Statin | 0.79 | 0.35–1.75 | 0.559 | 4.20 | 1.25–14.16 | 0.02 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNitric Oxide and Endothelin Effects · Cardiovascular Function and Risk Factors · Electron Spin Resonance Studies
Introduction
1
Despite more than 140 years of clinical use, the long-term prognostic impact of nitrates remains uncertain (1). Nitrates continue to be among the most commonly prescribed medications for patients with coronary artery disease (CAD). According to current guidelines, long-acting nitrates may be used for angina prevention or symptom relief in patients who remain symptomatic despite treatment with aspirin, statins, β-blockers, or calcium channel blockers (2). In addition CAD, nitrates also have been recommended in the treatment of congestive heart failure (3). However, controversy surrounding nitrate use has persisted.
Several studies have suggested that long-term nitrate therapy may be associated with increased adverse clinical events in patients with CAD. Nevertheless, few studies have explicitly examined whether baseline left ventricular ejection fraction (LVEF) modifies this association (4–6). In some studies involving patients with reduced LVEF, nitrate treatment has demonstrated convincing benefits in terms of remodeling and exercise tolerance. In the case of African-American patients with LVEF ≤ 45%, nitrate treatment was even associated with reduced mortality (7, 8). However, approximately half of the patients enrolled in these studies did not have CAD. Therefore, evidence regarding the impact of nitrate therapy on patients with CAD across different levels of LVEF remains limited.
Discharge medications, as a critical component of the discharge summary, play a very important role in patient safety and continuity of care (9). The purpose of this study was therefore to analyze and compare if CAD patients discharged on nitrates experienced different prognoses across different levels of LVEF.
Methods
2
Data collection
2.1
We retrospectively selected patients diagnosed with coronary heart disease from the Department of Cardiology at Guizhou Provincial People's Hospital between July 2012 and August 2016. Eligible patients were aged 18 years or older and had undergone coronary angiography. CAD was defined as angiographic evidence of ≥50% diameter stenosis in at least one major epicardial coronary artery (left main, LAD, LCx, or RCA), regardless of segment location (proximal, mid, or distal) (10, 11). Detail definitions of acute coronary syndrome and stable angina have been previously described (12). The hospital database collects information about medical history, cardiovascular risk factor, previous medication, clinical characteristics, laboratory variables, echocardiographic results, angiographic findings, revascularization procedures, medication on discharge, and follow-up data.
Study population
2.2
A total of 3,714 patients diagnosed with coronary heart disease in the cardiology department at Guizhou Provincial People's Hospital between July 2012 and August 2016 were retrospectively selected. Eligible patients had ≥50% stenosis in at least one major epicardial vessel, irrespective of lesion segment. The analyses in this study were restricted to patients with detailed discharge medication records and documented LVEF. Patients discharged on nitrates were defined as those prescribed any formulation of nitrates (i.e., mononitrate or dinitrate) at discharge. Typically, patients are discharged with a 2-week supply or more in this hospital. The following groups of patients were excluded from this study: patients who died during hospitalization; patients lost to follow-up; patients with incomplete follow-ups; patients who did not undergo at least one echocardiographic examination; and patients with missing data on discharged medicines. Guideline-directed medicine treatment was defined a priori as evidence-based pharmacologic therapy recommended for chronic coronary disease, including antiplatelet therapy and statins for secondary prevention, as well as beta-blockers and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers when clinically indicated (13). Antianginal agents, including calcium channel blockers and long-acting nitrates, were prescribed for symptom control at the treating physicians’ discretion, consistent with contemporary guideline recommendations (13).
Follow-up
2.3
Follow-up was completed primarily through telephone interviews. All interviewers were trained professionally prior to conducting interviews. A predefined questionnaire was used to collect the follow-up information. If patients could not be contacted or declined telephone follow-up, alternative methods—including chart review, clinical attendance records, or letter correspondence—were used.
Endpoints and definitions
2.4
The primary endpoint of this study was all-cause death. The secondary endpoint was major adverse cardiovascular events (MACE) [defined as the composite of cardiovascular death (CV death), non-fatal myocardial infarction (MI), and non-fatal stroke]. All events were adjudicated by two independent members.
Statistical analysis
2.5
Patients were divided into three groups according to LVEF status. Group 1 was LVEF less than 45%, group 2 was LVEF between 45% and 55%, and group 3 was LVEF more than 55% (14). This categorization was selected a priori to reflect commonly used echocardiographic grading of systolic function, in which LVEF >55% is generally considered normal, 45%–54% is considered mildly reduced, and values below this range indicate at least moderate systolic dysfunction. In addition, contemporary evidence in coronary artery disease supports 55% as a clinically relevant prognostic threshold, with higher mortality observed below an LVEF of approximately 55% in a large CAD cohort (15). To facilitate comparison with ESC heart failure nomenclature, we performed a sensitivity analysis using ESC LVEF categories [Heart failure with reduced ejection fraction(HFrEF) ≤ 40%, Heart failure with mildly reduced ejection fraction (HFmrEF) 41%–49%, and Heart failure with preserved ejection fraction (HFpEF) ≥ 50%]. In each group, patients were further stratified into two subgroups based on whether they were discharged with or without nitrates. The prescription of nitrates was at the discretion of the doctor. Data were compared between patients discharged with and without nitrates in each group. Continuous variables are expressed as mean ± standard deviation (SD), and categorical variables are reported as absolute value [percentages (%)]. Continuous and categorical variables were compared using analysis of variance and chi-square tests, respectively. Kaplan–Meier analyses were performed to estimate the cumulative incidences of primary and secondary outcomes, stratified by discharged with or without nitrates. Cox proportional hazards regression analysis was performed to examine factors associated with outcomes. The effect size was hazard ratios (HRs) and its corresponding 95% confidence intervals (95% CI). In multivariate Cox proportional hazards regression analysis, clinical risk factors included age, gender, diabetes, hypertension, and smoking. Additional covariates were selected based upon univariate analyses or baseline comparisons. Variables entered the analyses if the univariate analysis showed p ≤ 0.2 or if baseline comparisons suggested significant differences between subgroups. All tests were two-sided, and p ≤ 0.05 was considered statistically significant. All analyses were performed using SPSS software (Version 19.0). Given the retrospective nature of the study, the sample size was determined by the available data in the database. A post-hoc power analysis was performed to estimate the statistical power of the LVEF subgroups. We calculated the power to detect a clinically meaningful HR of 1.5–2.0 for all-cause death, assuming a two-sided alpha of 0.05 and using observed event rates in the control groups (PASS 15.0, NCSS, LLC).
Results
3
A total of 3,714 patients diagnosed with coronary heart disease by coronary angiography in the cardiology department at Guizhou Provincial People's Hospital between July 2012 and August 2016 were retrospectively selected. Of these, 3,367 patients (90.7%) completed follow-up, while 347 patients (9.3%) were lost to follow-up. The mean duration of follow-up was 27.2 ± 13.5 months. The follow-up flowchart is presented in Figure 1. Among the 3,367 patients, another 963 patients were excluded from this study because of in-hospital death, incomplete follow-up, absent echocardiograph records, or missing discharge records. Finally, 2,404 patients were eligible for this study. Of these, 1,153 patients (48%) were discharged on nitrates and 1,251 patients (52%) were not discharged on nitrates. Classifying these patients into three groups based upon LVEF, 299 patients had LVEF < 45%, 333 LVEF between 45% to 55%, and 1,772 LVEF > 55%.
Patient screening and disposition.
The detailed baseline characteristics of the study population are shown in Table 1. Based on these sample sizes, a post-hoc power analysis indicated that the statistical power was sufficient (>80%) to detect clinically relevant hazard ratios in the LVEF < 45% and >55% subgroups, which comprised the majority of the study population. Compared with patients not discharged on nitrates, patients discharged on nitrates had similar distributions of sex, acute coronary syndrome, diabetes, body mass index, and LDL-C. However, patients with nitrates at discharge were older, appeared to have more hypertension, were less likely to have a history of myocardial infarction, and had fewer current smokers. Moreover, these patients seemed to have higher LVEF and serum creatinine, and fewer implanted stents during the index procedures. Importantly, patients discharged on nitrates seemed to take aspirin, statin, angiotensin-converting enzyme inhibitor (ACEI)/angiotensin receptor blocker (ARB), β-blockers, and calcium channel blocker (CCB) before admission. However, patients discharged on nitrates received comparable rates of aspirin, clopidogrel, and ACEI/ARB, but were prescribed fewer statin and more CCB and β-blockers.
Endpoints
3.1
Total patients
3.1.1
Among patients with nitrates at discharge, 72 patients (6.2%) died during follow-up, compared with 67 (5.4%) deaths among patients without nitrates. The cumulative incidence for all-cause death was insignificant between patients with nitrates and without nitrates at discharge (log-rank P = 0.748; Figure 2A). Similarly, no difference in cumulative incidence for MACE was observed (log-rank p = 0.513; Figure 2B). Multivariate Cox regression analysis showed that discharged on nitrates was not associated with the occurrence of all-cause death or MACE among the overall cohort (Table 2). Age, LVEF, serum creatinine, white blood cell, taking β-blocker before admission, prescribed aspirin at discharge, and stent implantation were independent predictors of all-cause death. LVEF, β-blocker use before admission, aspirin prescription at discharge, stent implantation, and left main artery disease were independently associated with MACE in these patients (Table 2).
Kaplan–Meier curves for the all-cause death and MACE in the total patient population stratified according to discharged or not discharged on nitrates. There were no statistically significant difference in cumulative incidences of all-cause death (A, log-rank P = 0.748) and MACE (B, log-rank P = 0.513) between patients discharged on nitrates and not discharged on nitrates.
Patients with LVEF < 45%
3.1.2
Discharge on nitrates and all-cause death
3.1.2.1
During the follow-up, 43 patients (14.3%) died. Of these, 24 deaths occurred among patients with nitrates at discharge, and 19 deaths were among those without nitrates. The cumulative incidence of all-cause death was higher in patients with nitrates at discharge (log-rank P = 0.029; Figure 3A). Multivariate Cox regression analysis identified discharged on nitrates, age, current smoking, and serum creatinine as independent predictors of all-cause death. Discharge on nitrates was associated with an HR of 2.14 (95% CI, 1.15–3.96) after adjusting for confounding factors (Table 3).
Kaplan–Meier curves for the all-cause death and MACE in patients with LVEF less than 45% stratified according to discharged or not discharged on nitrates. Patients discharged on nitrates had statistically significant worse outcomes with higher cumulative incidence of all-cause death (A, log-rank P = 0.029), and MACE (B, log-rank P = 0.024).
Discharge on nitrates and MACE
3.1.2.2
MACE was reached in 44 patients (14.7%). Increased cumulative incidence of MACE was observed in patients with nitrates at discharge (log-rank p = 0.024, Figure 3B). However, after adjusting for confounding factors, the Multivariate Cox regression analysis showed that discharge on nitrates was the only independent predictor of MACE, with an HR of 1.91 (95% CI, 1.07–3.43) (Table 3).
Patients with LVEF between 45% and 55%
3.1.3
Among patients with LVEF between 45% and 55%, discharge on nitrates was not associated with all-cause death or MACE. Compared with patients not discharged on nitrates, those with discharged on nitrates had similar cumulative incidences of all-cause death and MACE (Figure 4. A: all-cause death, log-rank P = 0.634; B: MACE, log-rank P = 0.494). Multivariate Cox regression analysis also showed that discharge on nitrates was not an independent predictor of all-cause death or MACE (Table 4). Age, serum creatinine, and aspirin prescription at discharge were independent predictors of all-cause death. Body mass index and serum creatinine predicted MACE independently in patients with LVEF between 45% and 55%.
Kaplan–Meier curves for the all-cause death and MACE in patients with LVEF between 45% and 55% stratified according to discharged or not discharged on nitrates. Patients discharged or not discharged on nitrates had similar long-term outcome showing insignificantly difference in cumulative incidences of all-cause death (A, log-rank P = 0.634), and MACE (B, log-rank P = 0.494).
Patients with LVEF more than 55%
3.1.4
There were 38 all-cause deaths and 49 MACEs among patients with nitrates at discharge. For patients without nitrates at discharge, 33 died and 38 reached MACE. The differences of cumulative incidence for all-cause death and MACE between patients with nitrates and without nitrates at discharge were both insignificant (Figure 5A: all-cause death, log-rank P = 0.872; Figure 5B: MACE, log-rank P = 0.803). Similarly, multivariable Cox regression analysis also showed that discharge on nitrates was not an independent predictor of all-cause death or MACE. Age, LDL-C, and white blood cell were independently associated with all-cause death. Left main artery disease, number of stents, stent implantation, and statin prescription at discharge were independent predictors of MACE (Table 5).
Kaplan–Meier curves for the all-cause death and MACE in patients with LVEF more than 55% stratified according to discharged or not discharged on nitrates. Patients discharged or not discharged on nitrates had similar long-term outcome showing insignificantly difference in cumulative incidences of all-cause death (A, log-rank P = 0.872), and MACE (B, log-rank P = 0.803).
Reclassified groups
3.2
Reclassification followed the ESC heart failure nomenclature (≤40%, 41%–49%, and ≥50%) (16) to ensure comparability with current guideline categories. Considering that some guidelines and studies classify LVEF into normal, mildly abnormal, and moderately and severely abnormal with LVEF ≥ 50%, 40%–50%, and ≤40%, respectively (3), we reclassified patients into the following three groups: LVEF ≥ 50%, 40%–50%, and ≤40%. There were 206 patients with LVEF ≤ 40%, 234 with LVEF between 40% and 50%, and 1964 with LVEF ≥ 50%. The baseline differences between patients discharged on nitrates and those not on nitrates were comparable in each subgroup compared with the former grouping strategy. Similarly, the reclassified strategy also noted that discharge on nitrates was an independent predictor factor of MACE and all-cause death in patients with LVEF ≤ 40%, but had no association with MACE or all-cause death in patients with LVEF between 40% and 50% or LVEF ≥ 50% (data not shown).
Discussion
4
Chronic nitrate therapy remains widely used for symptom control in CAD, yet its long-term prognostic impact has not been established in contemporary practice. Moreover, whether baseline left ventricular systolic function modifies any association between nitrates and clinical outcomes has been insufficiently characterized. In our angiography-confirmed CAD cohort, nearly half of the patients were discharged on long-acting nitrates. In the overall population, nitrate prescription at discharge was not associated with all-cause mortality or MACE. However, after stratification by LVEF, an adverse association was confined to patients with LVEF < 45%, in whom discharge on nitrates was independently associated with higher risks of all-cause death and MACE; no significant associations were observed in patients with LVEF 45%–55% or >55%.
These findings are clinically relevant because long-acting nitrates continue to be prescribed frequently in coronary artery disease, despite limited evidence for sustained prognostic benefit. Current guidelines recommend long-acting nitrates primarily for angina prevention and symptom relief, particularly when symptoms persist despite first-line antianginal therapy (13). In contrast, several observational studies have raised concerns about chronic nitrate exposure in ischemic heart disease. Using databases from two large postinfarction studies, Nakamura and colleagues reported an association between long-term nitrate use and higher mortality (17, 18). Similarly, Ishikawa et al. found that long-term oral nitrate therapy was associated with more cardiac events in a cohort of patients with healed myocardial infarction (4), and Kanamasa et al. reported higher event rates during follow-up among patients treated continuously with oral and transdermal nitrates (6). More contemporary registry data have extended these observations to other clinical contexts. For example, among higher-risk stable coronary disease populations—including patients with diabetes undergoing elective percutaneous coronary intervention—chronic oral nitrate therapy has been linked to increased major adverse cardiovascular events in observational analyses (19). In addition, in cohorts of vasospastic angina, long-acting nitrates have not demonstrated prognostic benefit, and certain nitrate-based regimens have been associated with higher rates of adverse events (20–22). Taken together, although these data are subject to confounding by indication, the consistency of signals across diverse cohorts supports the possibility that chronic nitrate therapy may be prognostically non-neutral in selected subgroups, which provides clinical context for our finding of an adverse association primarily in patients with reduced LVEF.
However, most prior studies have not evaluated whether baseline LVEF modifies the association between chronic nitrate therapy and clinical outcomes in coronary artery disease. To address this gap, we assessed discharge prescriptions for long-acting nitrates across prespecified LVEF strata in an angiographically confirmed CAD cohort. The primary finding was that an adverse association with both all-cause mortality and major adverse cardiovascular events was observed among patients with LVEF < 45%, whereas no significant associations were detected among those with LVEF ≥ 45%. Although the observational design precludes causal inference and residual confounding remains possible, these data suggest that the clinical risk profile associated with chronic nitrate therapy may differ according to baseline systolic function.
Although these results may appear to conflict with heart failure trials that evaluated nitrate-based regimens, several distinctions are important. First, the trials most often cited in support of nitrate therapy in HFrEF evaluated hydralazine plus isosorbide dinitrate rather than nitrate monotherapy, and they were conducted in therapeutic eras that differed substantially from contemporary guideline-directed medical therapy (8, 23). In our cohort, most patients received background neurohormonal therapies, including an ACEI or ARB and a beta blocker, which may influence both symptoms and prognosis and may also modify the net effect of vasodilator therapy. In A HeFT, which enrolled African American patients with heart failure, hydralazine plus isosorbide dinitrate was associated with reduced mortality; however, the restriction to a single racial group and early trial termination limit generalizability, particularly to non-Black populations (8). Consistently, a large observational cohort study including 76,828 patients with heart failure did not show an apparent benefit of hydralazine plus nitrate therapy overall or within major racial or ethnic subgroups (24). Furthermore, contemporary guidance positions hydralazine plus isosorbide dinitrate as a therapy for selected patients with HFrEF rather than a broadly applicable nitrate strategy to improve prognosis (25). Finally, more recent randomized data in HFpEF have not supported benefit from nitrate-based approaches. Extended release isosorbide mononitrate reduced daily activity without improving exercise capacity or quality of life in NEAT HFpEF (26), and inhaled inorganic nitrite did not improve peak oxygen consumption in INDIE HFpEF (27). Taken together, the broader contemporary literature suggests that nitrate-related strategies are not uniformly beneficial across heart failure phenotypes, which is compatible with our observation that adverse associations were confined to CAD patients with reduced LVEF.
Nitrate tolerance, the potential role of intermittent nitrate therapy, neurohumoral effects, aggravation of myocardial ischemia, and hypervascular responses in coronary arteries may contribute to the adverse outcomes associated with chronic nitrate therapy (28, 29). In the setting of prior myocardial infarction, the ischemic myocardial microenvironment is often characterized by persistent oxidative stress, inflammation, and microvascular dysfunction, which may further impair myocardial and vascular homeostasis (30). In addition, the thrombotic microenvironment in postmyocardial infarction patients can exacerbate endothelial dysfunction, further compromising vascular integrity and increasing the risk of adverse cardiovascular events (31, 32). These factors may contribute to the impaired endothelial function observed in patients with reduced LVEF, which could amplify their vulnerability to additional endothelial or hemodynamic stress. As a result, this adverse ischemic milieu may potentially contribute to the unfavorable associations observed with chronic nitrate therapy in these patients. In addition, both experimental and human studies have suggested that sustained exposure to organic nitrates may impair endothelial function through oxidative stress-related pathways (33, 34). In a well-characterized animal model, short-term treatment with isosorbide 5 mononitrate was associated with endothelial dysfunction and increased oxidative stress even in the absence of clear hemodynamic tolerance, which supports the possibility that vascular dysfunction may occur independently of classic tolerance (33). Consistently, once-daily isosorbide 5 mononitrate therapy impaired endothelial-dependent vasomotor function in humans, and this effect was reversed by antioxidant supplementation, further implicating reactive oxygen species in this process (34). Because hydralazine has been reported to exert antioxidant-related effects, it is possible that concomitant hydralazine could attenuate nitrate-associated oxidative stress, thereby influencing the net clinical effects of combination therapy; however, this remains a mechanistic hypothesis rather than a definitive explanation for trial outcomes (35). Endothelial dysfunction is an established marker of worse long-term prognosis in patients with coronary artery disease and heart failure (36–38). Moreover, patients with reduced systolic function may have less physiologic reserve and could be more vulnerable to additional vascular dysfunction, which may help explain why adverse associations with nitrates were observed in patients with LVEF < 45% but not in those with preserved systolic function (37–39).
In addition to the primary exposure of interest, several established clinical and treatment-related factors were independently associated with outcomes, supporting the overall clinical plausibility of our models. In the Cox regression analyses, preadmission beta blocker use, higher LVEF, discharge aspirin prescription, and stent implantation were associated with lower risks of all-cause mortality and major adverse cardiovascular events, whereas older age, higher serum creatinine and white blood cell count, left main coronary artery disease, and current smoking were associated with higher risks of these outcomes. These associations are consistent with prior reports in patients with coronary artery disease and heart failure (40–44). By contrast, the direction of the association between discharge statin therapy and outcomes in the subgroup with LVEF greater than 55% did not align with the broader literature supporting statins for secondary prevention (13, 45). This finding should be interpreted cautiously because only a small proportion of patients were not discharged on statins, which may have limited statistical power and increased susceptibility to imbalance and model instability. In addition, residual confounding and treatment selection related to disease severity or comorbidity could have influenced this estimate. Accordingly, while these covariate associations provide clinical context for our main findings, the statin signal in this subgroup should be viewed as exploratory and is further addressed in the limitations.
Limitations
5
This study has several limitations. First, its retrospective, single-center observational design precludes causal inference and leaves the possibility of residual confounding despite multivariable adjustment. Second, nitrate exposure was defined according to discharge prescription, and detailed information on postdischarge adherence, treatment duration, or dose changes was not available, which may have resulted in exposure misclassification. Third, coronary artery disease was defined using angiographic criteria without routine physiological assessment, and anatomical stenosis severity may not always reflect functional ischemic significance. Fourth, echocardiographic data were not available for all patients undergoing coronary angiography, potentially introducing selection bias. Finally, as the cohort was derived from a single center, the generalizability of these findings to other populations requires external validation.
Conclusion
6
Our study suggests that nearly half of patients with coronary artery disease are discharged on nitrates. The impact of prescribed nitrates at discharge on prognosis is diverse across LVEF. Being discharged on nitrates was not a predictor of MACE or all-cause death in patients with normal or mildly reduced LVEF, but it was a strong predictor among those with moderately or severely reduced LVEF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nossaman VE Nossaman BD Kadowitz PJ. Nitrates and nitrites in the treatment of ischemic cardiac disease. Cardiol Rev. (2010) 18(4):190–7. 10.1097/CRD.0b 013e 3181 c 8e 14a 20539102 PMC 2885014 · doi ↗ · pubmed ↗
- 2Knuuti J Wijns W Saraste A Capodanno D Barbato E Funck-Brentano C 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. (2020) 41(3):407–77. 10.1093/eurheartj/ehz 42531504439 · doi ↗ · pubmed ↗
- 3Mc Donagh TA Metra M Adamo M Gardner RS Baumbach A Böhm M 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42(36):3599–726. 10.1093/eurheartj/ehab 36834447992 · doi ↗ · pubmed ↗
- 4Ishikawa K Kanamasa K Ogawa I Takenaka T Naito T Kamata N Long-term nitrate treatment increases cardiac events in patients with healed myocardial infarction. Secondary prevention group. Jpn Circ J. (1996) 60(10):779–88. 10.1253/jcj.60.7798933241 · doi ↗ · pubmed ↗
- 5Nakamura Y Moss AJ Brown MW Kinoshita M Kawai C. Long-term nitrate use may be deleterious in ischemic heart disease: a study using the databases from two large-scale postinfarction studies. Multicenter myocardial ischemia research group. Am Heart J. (1999) 138(3 Pt 1):577–85. 10.1016/S 0002-8703(99)70163-810467211 · doi ↗ · pubmed ↗
- 6Kanamasa K Hayashi T Kimura A Ikeda A Ishikawa K. Long-term, continuous treatment with both oral and transdermal nitrates increases cardiac events in healed myocardial infarction patients. Angiology. (2002) 53(4):399–408. 10.1177/00033197020530040512143944 · doi ↗ · pubmed ↗
- 7Cohn JN Johnson G Ziesche S Cobb F Francis G Tristani F. A comparison of enalapril with hydralazine-isosorbide dinitrate in the treatment of chronic congestive heart failure. N Engl J Med. (1991) 325(5):303–10. 10.1056/NEJM 199108013250502057035 · doi ↗ · pubmed ↗
- 8Taylor AL Ziesche S Yancy C Carson P D'Agostino R Jr Ferdinand K. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. (2004) 351(20):2049–57. 10.1056/NEJ Moa 04293415533851 · doi ↗ · pubmed ↗