Optimizing Benefits‐Harms of H. pylori Screen‐and‐Treat Programs Tailored to the Regional Settings
Duco T. Mülder, Yi‐Chia Lee, Mario Dinis‐Ribeiro, Melissa McLeod, Jin Young Park, Iris Lansdorp‐Vogelaar

TL;DR
This paper explains how decision modeling can help create cost-effective H. pylori screening and treatment programs that are tailored to specific regions.
Contribution
The paper introduces a framework for using decision modeling to optimize H. pylori screen-and-treat programs based on regional needs.
Findings
Modeling studies show H. pylori screen-and-treat is cost-effective in diverse populations.
Decision modeling can improve resource allocation and health equity in these programs.
Integrating H. pylori screening with other preventive programs may enhance efficiency.
Abstract
This article outlines how decision modeling can be used to optimize the cost‐effectiveness of H. pylori screen‐and‐treat programs. Decision models enable the translation of data from pilot studies into locally tailored strategies by adapting test modalities, treatment options, and the need to retest specific to the local setting. We summarize existing evidence from modeling studies, which consistently demonstrate that H. pylori screen‐and‐treat is cost‐effective across diverse populations. In addition, we discuss how decision modeling can support resource allocation, promote health equity, and guide implementation planning. Integrating H. pylori screen‐and‐treat into established preventive programs, such as colorectal cancer screening, may further increase efficiency and feasibility. The article concludes with a proposed research agenda to advance efficient H. pylori…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
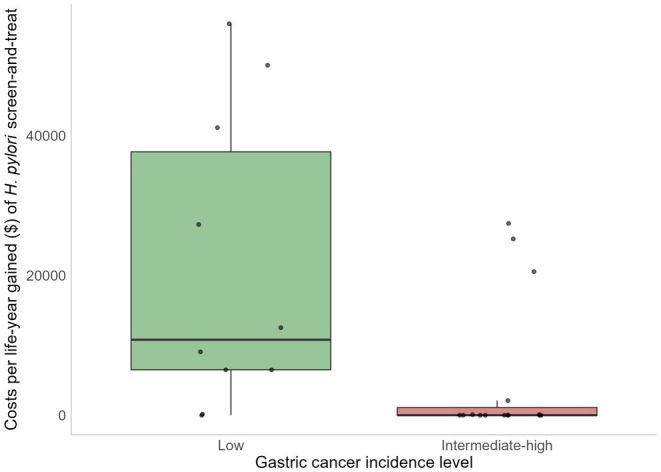 FIGURE 1
FIGURE 1| Demographic | Disease and testing | Outcome |
|---|---|---|
| Birth tables |
| Costs of and associated to the test and procedure |
| Life‐tables (life‐expectancy) | Gastric cancer incidence by localization (cardia vs. non‐cardia) and histology (Lauren‐classification) by age | Treatment costs (stage specific, ideally split by phase of care) |
| Observed cancer stage distribution | Estimates of disutility per test procedure | |
| Stage‐specific cancer survival | Stage‐specific estimates of disutility to gastric cancer | |
| Test participation in pilot studies (initial participation and treatment adherence) |
| Author, year | Country | Population simulated | Strategies evaluated | Test characteristics | Test costs | Costs per QALY/LY |
|---|---|---|---|---|---|---|
| Nakatani, 2023 [ | Japan | 40 and 50‐year old employees | Adding HPA test to UGI |
HPA sensitivity: 93% HPA specificity: 79% | HPA: $9.1 | cost‐saving |
| Zheng, 2023 [ | Hypothetical high‐risk country | > 40 years old | 14C UBT and NGCS risk‐based screening | 14C UBT sensitivity: 96% 14C UBT specificity: 93% | UBT: $25.56 |
$76.17 UBT compared to no‐screen $5492.84 UBT compared to NGCS |
| Kowada, 2024 [ | Japan | 15‐year old cohort | HPA. If positive, UBT. At ages 15, 18, 20, 30, …, 80 |
HPA sensitivity: 93% HPA specificity: 99% UBT sensitivity: 96% UBT specificity: 93% |
HPA: $16.27 UBT: $36.90 | Cost‐saving at ages 15–40 and age 80. At ages 50–70: $2476–2479 |
| Ma, 2025 [ | China | Families ≥ 2 people |
Random testing and if positive, test family members vs. Random testing. All 13C‐UBT |
UBT sensitivity: 95.5% UBT specificity: 94.7% | UBT: $24.28 | Family‐based: cost‐saving |
| Li, 2025 [ | China | Cohort of 20‐year olds | UBT at ages 20, 30, 40. One‐time test + every 2/3/5 years until age 50 |
UBT sensitivity: 87.6% UBT specificity: 84.8% | UBT: $11.63 |
All one‐time tests cost‐saving. Costs compared to no‐screen of repeat tests every 2/3/5 years: At age 20: $215/$122/$47 At age 30: $201/$81/$15 At age 40: $98/cost‐saving/cost‐saving |
| Eligibility | The eligibility criteria for FIT are shifting towards younger ages, at which |
|---|---|
| Invitation | Stool sample‐based tests are more acceptable and accessible for people compared to invasive procedures like endoscopies |
| Participation | The participation rate of FIT may be increased by adding |
| Testing | Both tests use stool samples, making it easy to distribute them together |
| Management | The management of |
| Cost‐effectiveness | The direct and indirect cost of |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Microscopic Colitis · Clostridium difficile and Clostridium perfringens research
Introduction
1
The articles in this special issue highlight the variety of gastric cancer prevention strategies implemented worldwide, with a strong emphasis on population‐based * Helicobacter pylori (H. pylori)* screen‐and‐treat programs. Collectively, these articles demonstrate the potential of an H. pylori screen‐and‐treat approach to reduce the burden of gastric cancer. However, translating success strategies to other settings can be challenging, as the optimal strategy depends on local circumstances, such as the disease burden, resource availability, and the structure of the healthcare system.
This paper aims to support health policymakers in designing efficient H. pylori screen‐and‐treat programs tailored to their context. The article starts by delving into the role of decision modeling in the optimal implementation of H. pylori screen‐and‐treat and what information needs to be collected to allow effective decision modeling for the local context. Notwithstanding the need for local evidence, we then discuss currently available international evidence with respect to the cost‐effectiveness of H. pylori screen‐and‐treat, and optimal strategies for implementation (e.g., which test, what age, etc.). Furthermore, we explain the potential synergy when combining H. pylori screen‐and‐treat with existing preventive interventions.
The content of this article provides an update of the findings in chapter 9 of the working group report on population‐based H. pylori screen‐and‐treat strategies for gastric cancer prevention [1]. This report, written by an international interdisciplinary panel convened by the International Agency for Research on Cancer (IARC), aims to provide guidance on program implementation. The authors of this article were part of the working group and participated in the expert meeting in February 2025. Since the publication of the original report, new evidence and modeling studies have emerged warranting an updated synthesis of the literature. We therefore updated the literature search to include all published articles until December 2025. Furthermore, this article extends the original report by exploring how decision modeling can inform H. pylori screen‐and‐treat programs beyond cost‐effectiveness, such as applications in healthcare resource planning and addressing health disparities.
Decision Modeling for Regional
H. pylori Screen‐And‐Treat Optimization
2
Although the optimal strategy for H. pylori screen‐and‐treat depends on local conditions, it is not feasible to perform local clinical studies addressing all variables and dimensions of the program. Alternatively, decision modeling can translate findings of clinical studies to the local settings in a different way to estimate whether H. pylori screen‐and‐treat provides good value for money in the local setting and under what conditions.
Decision modeling is a structured process that predicts the outcomes of certain scenarios, offering valuable insights to policy makers and stakeholders. This may help in both the implementation and evaluation phase of preventive interventions.
Similarly, decision modeling should be used in the decision‐making phase of H. pylori screen‐and‐treat programs to establish for the local setting whether its benefits outweigh its harms and whether the required resources are economically balanced with the net benefits. If a positive decision on implementation has been made, decision models can next be used in the preparatory phase before implementation to estimate annual resource requirements for laboratory testing, drug availability, endoscopic follow‐up capacity, etc. to help planning of the H. pylori screen‐and‐treat program. Different roll‐out schedules can be compared to best accommodate resource constraints, and potential bottlenecks in implementation can be identified and tackled where necessary. After that, during implementation, decision modeling can be used to compare program outcomes (and their distribution over population subgroups) with expectations based on prior modeling and/or pilot studies. Moreover, decision modeling can evaluate how best to adjust the program if it does not perform according to expectations. Finally, modeling can be used to make predictions of the long‐term benefits of the program. This is especially important in the light of the long lag time between the implementation of an H. pylori screen‐and‐treat strategy and its actual reduction in gastric cancer incidence and mortality.
Data Requirements for Regional Modeling
3
The aim of decision modeling is to extrapolate findings of clinical studies to different settings and strategies. However, for valid extrapolation to the local setting, two requirements need to be met: (1) evidence for the effectiveness of screening is available for settings comparable to the local situation; and (2) good‐quality data is available to inform model parameters to the local setting. Currently, most trial evidence relies on the long‐term benefits of H. pylori screen‐and‐treat, which comes from studies in Asia; long‐term model results for the non‐Asian context should, therefore, be interpreted with caution.
With respect to data availability, access to more elaborate and detailed data enables more precise estimations. Data requirements can generally be categorized into three main groups: demographic data, disease & testing data and outcome data (Table 1).
Developing and calibrating decision models is a complex and time‐consuming task that requires specialized expertise in statistical modeling and epidemiology. Instead of developing independent decision models, health policymakers may choose to collaborate with established modeling consortia such as the Cancer Intervention Screening Network (CISNET) [3] or Decision Analysis in R for Technologies in Health (DARTH) group [4].
Current Evidence from Decision Modeling on
H. pylori Screen‐And‐Treat Strategies
4
Decision models should always reflect the local demographic and epidemiological data to inform health policy. While such context‐specific studies are needed to maximize the benefits of H. pylori screen‐and‐treat, some lessons can be learnt from existing decision modeling studies. Especially when results are found to be robust across different H. pylori prevalence and gastric cancer risk settings, it is likely that these results are generalizable to the local setting. Even though decision models can serve multiple purposes, such as evaluating the impact of interventions on healthcare resources or equity, most applications of H. pylori screen‐and‐treat modeling have focused on cost‐effectiveness. The discussion of current evidence will therefore center on that aspect.
Evidence for the Cost‐Effectiveness of
H. pylori Screen‐And‐Treat
5
Four reviews have assessed the cost‐effectiveness of H. pylori screen‐and‐treat [5, 6, 7, 8]. Three reviews included studies from countries all over the world, with different levels of H. pylori prevalence and gastric cancer burden [6, 7, 8]. One review specifically focused on cost‐effectiveness in Western countries, with a lower burden of H. pylori and gastric cancer [5]. All four reviews concluded that a strategy of H. pylori screen‐and‐treat is cost‐effective in reducing gastric cancer incidence and mortality. Of all 18 studies included in the reviews, only two found H. pylori screen‐and‐treat to result in net cost‐savings compared to a situation without testing. In these studies, cost‐savings from preventing dyspepsia were also considered in addition to those of gastric cancer prevention.
The literature was again reviewed for the IARC working group report, finding an additional five studies [1]. Interestingly, four of these studies found that H. pylori screen‐and‐treat not only gained life years (LY) by preventing gastric cancer but was also cost‐saving to the health system (compared to no testing) [9, 10, 11, 12]. In the fifth study, H. pylori screen‐and‐treat was not found to save costs, but still resulted in a favorable balance between the additional costs and benefits compared to no testing [13].
The search query (Supporting Information) was again updated for this study, yielding an additional five studies all conducted in Asian countries with a high gastric cancer risk (Table 2). Four out of the five studies found H. pylori screen‐and‐treat to be cost‐saving [11, 14, 16, 17]. The fifth study found H. pylori screen‐and‐treat to be efficient, yet concluded that risk‐based endoscopy screening was the optimal strategy [15].
TABLE 2: Overview of studies on the cost‐effectiveness of H. pylori screen‐and‐treat published between 2023 and 2025.
Gastric cancer burden has an important influence on the cost‐effectiveness of H. pylori screen‐and‐treat programs. With a higher burden of disease, more deaths can be prevented with the same number of tests, resulting in a more favorable balance between benefits and resources required than in lower incidence settings. Although H. pylori screen‐and‐treat was found to be cost‐effective across all settings, the costs per life‐year gained were therefore typically lower in studies performed in high‐risk areas (Figure 1). One study explicitly studied the impact of H. pylori prevalence and gastric cancer burden on the cost‐effectiveness of H. pylori screen‐and‐treat [18]. This study concluded that in countries with intermediate to high (in this study ASR ≥ 17 per 100,000 person‐years) gastric cancer incidence, H. pylori screen‐and‐treat would be cost‐saving. However, the study also showed that even in low‐incidence countries (in this study: ASR 6 per 100,000 person‐years) H. pylori screen‐and‐treat resulted in a favorable balance between costs and health benefits.
Costs per life‐year gained for H. pylori screen‐and‐treat as observed in reviewed cost‐effectiveness analyses, stratified by gastric cancer incidence level. Boxes show the interquartile range, horizontal lines indicate the median, and points represent individual studies. Costs per life‐year gained have been standardized to present value. Studies demonstrating cost savings are set at 0. As willingness‐to‐pay thresholds and price levels differ across settings, the interpretation of costs per life year gained may differ among studies and settings. Data based on Lansdorp‐Vogelaar et al. [1] combined with the extra studies extracted in this study (Table 2).
It is important to note that a formal quality assessment of the included decision modeling studies has not been performed in any of the reviews, nor have we engaged in such an endeavor ourselves. Nevertheless, the consistency of the finding that H. pylori screen‐and‐treat is cost‐effective across studies provides additional confidence in the validity and robustness of this finding.
Optimizing the Cost‐Effectiveness of
H. pylori Screen‐And‐Treat Strategies for Gastric Cancer Prevention
6
When H. pylori screen‐and‐treat is implemented, decisions need to be made on the test modality, screening age (s), which drugs to use for eradication, whether to perform confirmation of eradication testing, and whether to perform resistance testing prior to eradication. In this paragraph, we summarize the current available evidence on which strategies provide most value for money.
Test Modality
6.1
Only three studies directly compared Carbon Urea Breath Test (^13^C‐UBT) with serology testing, with two of them additionally considering Stool Antigen Test (SAT) [9, 19, 20]. In these three studies, a strategy based on ^13^C‐UBT testing was associated with higher costs than serology testing. However, ^13^C‐UBT was also more effective in preventing gastric cancer incidence and mortality and thus gaining more LY. In the study by Yousefi et al. these extra benefits weighed favorably against the extra costs [9]. In the other two studies, the incremental costs per QALY exceeded the considered willingness‐to‐pay threshold, implying that ^13^C‐UBT did not provide good value for money compared to serology in these settings [19, 20]. Two studies comparing SAT to serology and ^13^C‐UBT concluded that SAT was more effective than serology. One of the studies also found SAT to be less expensive than the other test modalities [9] while the other found it to be highly cost‐effective [20].
Another study compared ^13^C‐UBT with polymerase chain reaction (PCR) testing of gastric biopsies and concluded that PCR testing is cost‐effective for gastric cancer prevention [13]. However, testing of gastric biopsies is an invasive strategy and may therefore be less acceptable and scalable than other testing modalities. Moreover, serology and SAT were not considered in this analysis. Consideration of these strategies may have resulted in a less favorable balance between costs and benefits (QALY gained) of PCR testing compared to these strategies.
In conclusion, there is limited evidence on the optimal test for H. pylori screen‐and‐treat for gastric cancer prevention with only four decision modeling studies performing direct comparisons between tests. These studies suggest that SAT may be more cost‐effective than serology. However, in general, all tests were found to be cost‐effective for gastric cancer prevention compared to no testing, and none of the tests was consistently dominated in all of the analyses. This finding suggests that the choice of the test may be based on local setting and resource considerations rather than cost‐effectiveness.
Test Age
6.2
Eight studies compared the cost‐effectiveness of different ages for H. pylori screen‐and‐treat [11, 17, 18, 19, 21, 22, 23, 24]. Three studies concluded that it was optimal to test for H. pylori infection at a young age (20 or 30 years), because H. pylori testing in cohorts older than that was both less effective and less cost‐effective.^10,2018^ These studies were performed in high‐incidence settings (ASR ≥ 20 per 100,000 person‐years). Another study found that one‐time testing was cost‐effective at all ages 20–40, but that retesting was only cost‐effective at age 40 [17]. The other studies, mostly based in low‐incidence settings (ASR < 10 per 100,000 person‐years) also found H. pylori testing to be more effective at these younger ages, but this effectiveness was accompanied by higher costs per life‐year gained. They therefore suggested ages for H. pylori testing centered around 40–50 years. These findings suggest that in low‐incidence settings, H. pylori screen‐and‐treat might not be cost‐effective before age 40, whereas it may be in high‐incidence settings. However, an important caveat with these findings is that many studies compared different screening ages across different birth cohorts. Given the high correlation between birth cohort and gastric cancer risk, this may indicate that it is more cost‐effective to screen older birth cohorts, rather than older individuals. Although not a cost‐effectiveness study, a model‐analysis within one birth cohort in the United States demonstrated that H. pylori screen‐and‐treat had a substantial larger benefit before age 40, reflected by the number‐needed‐to‐treat to prevent one cancer case [25]. Conversely, screening at younger age poses challenges to cost‐effectiveness, as the benefits of cancer prevention will only become apparent further in the future and therefore have a lower present value due to discounting. More studies looking at the optimal age of screening within the same birth cohort are therefore needed to demonstrate whether the increase in efficacy compensates the lack of cost‐effectiveness due to discounting.
Repeat Testing for
H. pylori
6.3
Evidence was limited with respect to repeat H. pylori screen‐and‐treat strategies. The purpose of repeated testing might be to account for (re‐)infection or failed eradication therapy. Three studies evaluated repetition of H. pylori screen‐and‐treat [17, 18, 22]. The studies considered different intervals (varying from 1 to 10 years) and frequencies (one repeat versus multiple) for repeated testing. Two out of three concluded that the extra benefits of repeat testing did not outweigh the extra resources. A third study suggested that repeat testing could be beneficial in China, although cost per life year gained was higher than for a one‐time test [17]. It is important to point out that evidence on re‐infection rates is scarce, although the rates are estimated to be less than 1% [26]. In the absence of strong evidence, policy makers can best implement a once‐only H. pylori screen‐and‐treat strategy. However, pilot studies within these programs, in which a subset of individuals is rescreened after 5–10 years, should be considered to fill this important gap in knowledge and inform future modeling.
Management of
H. pylori Infection
6.4
None of the cost‐effectiveness analyses on H. pylori screen‐and‐treat compared different eradication therapy regimens, or the benefit of resistance testing prior to initiating treatment. However, one study each addressed the incremental cost‐effectiveness of confirmation testing of successful eradication [27] and restricting treatment to only those that tested CagA‐positive [28]. Fendrick et al. explicitly compared serological testing with and without confirmatory testing 6 weeks after eradication therapy [27]. Assuming 80% effectiveness of initial eradication therapy, the scenario with the confirmatory test resulted in more life years gained than the strategy without confirmatory testing, but was substantially more costly. This finding suggests that in settings where the eradication rate of initial therapy exceeds 80%, confirmatory testing is not cost‐effective. However, without confirmatory testing in at least a sample of the population it is not possible to establish the H. pylori eradication rate.
Harris et al. evaluated the cost‐effectiveness of screening and treating either all H. pylori strains or CagA‐positive strains only [28]. Testing and treating only CagA‐positive infection reduced the number treated, the number of cases of anaphylaxis and overall costs of screen‐and‐treat, but it also reduced the number of cancers prevented and life years gained. In all countries for which it was evaluated, the incremental cost‐effectiveness ratio (ICER) for treating all H. pylori compared to CagA‐positive strains only was less than $25,100 per life year gained. These results suggest that it is better to screen‐and‐treat for all H. pylori rather than CagA‐positive alone.
Family‐Based Testing
6.5
A novel screening strategy for H. pylori is through family‐based testing, in which family members of positively tested individuals are also tested and treated for infection. This strategy started with a Chinese consensus report [29] and has now been adopted by several clinical guidelines [30, 31, 32]. From a cost‐effectiveness perspective, Ma et al. demonstrated that family‐based H. pylori screen‐and‐treat is a cost‐saving strategy and provides better value for money than traditional screen‐and‐treat in China. Further studies on family‐based testing are needed to confirm its effectiveness in different settings.
Decision Modeling for Resource Planning
7
In addition to cost‐effectiveness, feasibility and successful implementation depend on access to healthcare facilities, availability of trained personnel, and follow‐up care. Decision analysis not only measures costs and benefits, but also the intermediate aspects of the screening process, such as the number H. pylori tests needed, the number of antibiotic treatments needed, hospital visits, etc. This information helps policymakers prepare to ensure availability of resources and health professionals that are adequately trained to perform their role in the H. pylori screen‐and‐treat program. Such information is especially important in light of recent shortages of healthcare personnel and antibiotics [33].
Decision modeling can be used to project the required resources to implement a strategy. An illustrative example is how the MISCAN‐Colon model affected resource planning during the roll‐out of the successful Dutch colorectal cancer (CRC) screening program. In the implementation phase, the chosen FIT resulted in longer waiting lists for colonoscopy than expected. MISCAN‐Colon was considered to address the capacity constraints while maximizing screening benefits. The model analysis demonstrated that adjusting the cut‐off, rather than prolonging test intervals or changing eligible screening ages, was the most effective way to ease colonoscopy demand [34, 35].
The availability of resources and needs for H. pylori screen‐and‐treat programs may differ substantially between low‐and‐middle‐income countries (LMICs) and high‐income countries (HICs). While LMICs may face a higher disease burden and H. pylori prevalence, the lower level of available resources is often reflected in a lower willingness‐to‐pay threshold in CEA. This implies that the costs per life‐year gained need to be lower for the intervention to be considered cost‐effective. In addition to financial constraints, access to tests and antibiotic treatments may be limited in LMICs. Consequently, recommendations developed for HICs may not be feasible in LMICs. Decision modeling can help bridge this gap by integrating evidence with local data to identify the most efficient use of available resources. For instance, in breast cancer screening, modeling demonstrated that starting screening at later ages in LMICs may maximize benefits if screening resources are scarcer than in HICs [36].
Addressing Health Disparities
8
Decision modeling can also be applied to address health disparities. While traditional CEA often focuses on cost‐effectiveness as the primary output, there is a growing body of literature on CEA methods that can additionally consider the distributional and equity impacts of interventions [37, 38]. Two key examples of methods are the distributional cost effectiveness analysis (DCEA) and the extended cost effectiveness (ECEA) analysis. DCEA involves modeling an intervention by population subgroup, incorporating a measure of opportunity cost and then using relative and absolute measures of inequality to identify the service configuration that maximizes health while also minimizing ‘unfair’ health inequality [39]. ECEA is an approach that has been developed to address equity concerns relating to medical impoverishment in low‐ and middle‐income countries, where the majority of health care is funded through out‐of‐pocket payments [40, 41].
One study based in New Zealand examined a screen and treat program targeted by age, sex and ethnicity. This study found that while a population‐wide program would not be cost‐effective, targeting the program to Indigenous Māori (who have a higher burden of H. pylori and gastric cancer) would be cost‐effective [42].
Combinations with Colorectal Cancer Screening Programs to Create Synergy
9
A ‘one‐stop‐shop’ approach combining H. pylori screen‐and‐treat with other healthcare interventions may provide synergistic benefits.
One potential synergistic approach for H. pylori screen‐and‐treat is the combination with CRC screening. Many CRC screening programs across the world are based on non‐invasive collection of feces, which would combine well with SAT. The feasibility of a combined approach has been established both in Asia [43] and Europe [44]. Nieuwenburg et al. demonstrated that H. pylori antigen measurement can be performed in FIT stool samples with similar test performance compared to standard SAT [44]. Since the FIT is widely used in clinical practice, this approach may conveniently enable dual prevention of cancer in both the upper and lower gastrointestinal tracts.
Lee et al. combined the SAT with FIT in the screening of both upper and lower gastrointestinal lesions in a population with high prevalence of digestive tract diseases [43]. They compared three scenarios in a hospital cohort: the usage of SAT in all individuals; only among those with negative FIT; or only among those with negative colonoscopy. The SAT and FIT were therefore used as primary tests for the presence of upper and lower gastrointestinal lesions. The sensitivity of SAT for detecting gastric cancer did not differ and was approximately 50%. Importantly, three‐quarters of gastric cancers were diagnosed as stage I‐II disease. In the same study, but within a validation community cohort, the positive predictive value for upper gastrointestinal lesions using SAT was approximately 32%.\n.
Moreover, a randomized clinical trial inviting approximately 150,000 people to participate in either SAT plus FIT or FIT alone demonstrated an increased participation rate of about 14% of FIT combined with SAT compared with FIT alone [45]. This implies that combined screening attracts a larger proportion of individuals to engage in the screening program. Therefore, utilizing the existing FIT screening framework may be advantageous as outlined in Table 3.
TABLE 3: Potential advantages of using the FIT program as the foundation for offering screening and treatment for H. pylori infection for gastric cancer prevention.
The effectiveness of using the FIT program to offer H. pylori screen‐and‐treat depends on the screening age. While most CRC screening programs begin at age 50 [46], the best age to apply H. pylori screen‐and‐treat is uncertain. Some studies have suggested that H. pylori has most impact before the onset of precursor lesions or in less severe precursor lesions [47]. In that case, it seems likely that the optimal screening age is lower than the start age of CRC screening. Continuation of the current trend towards starting CRC earlier could lead to more potential for synergistic effects in future screening programs. Nevertheless, an intervention at the age of 50 may still be reasonable to achieve meaningful reductions in gastric cancer risk. A randomized clinical trial evaluating the addition of SAT to FIT included participants with a mean age of 58 years [45]. In this trial, an invitation to H. pylori screen‐and‐treat reduced gastric cancer incidence by 14% among invited individuals, although the reduction was not statistically significant. However, in post hoc analyses adjusted for non‐adherence to the invitation, a significant 21% reduction in gastric cancer incidence was observed [48]. These analyses should be considered exploratory because of the potential healthy‐screenee bias.
Pragmatic Trials
10
The potential benefits of adding H. pylori screen‐and‐treat to existing health interventions highlight the need for pragmatic trials and pilot studies, similar to those conducted in Taiwan [48]. Findings from such studies could inform policy decisions and provide key inputs for decision‐analytic models assessing whether H. pylori screen‐and‐treat should be implemented as a stand‐alone strategy or integrated within existing infrastructure. Such cost‐effectiveness analysis requires robust evidence on the magnitude of the effectiveness of H. pylori eradication at older ages, as well as data on potential cost reductions when tests and treatments are combined with existing screening programs.
Discussion
11
This article describes how to optimize the balance between harms and benefits of H. pylori screen‐and‐treat. Using decision models, factors such as the choice of test modality, target age and the need for repeat testing, can be tailored to context‐specific factors such as the local disease burden and the available resources. Current evidence from modeling studies was summarized, demonstrating that H. pylori screen‐and‐treat was cost‐effective at all investigated levels of gastric cancer incidence. However, the optimal approach differed per setting. We therefore outline practical recommendations for policymakers on the data required to adapt decision models for local use and explore how H. pylori screen‐and‐treat can be integrated with colorectal cancer screening.
H. pylori infection is known to be the major contributor to gastric cancer [49]. Efforts to combat H. pylori should replicate the success seen in other primary prevention programs targeting the elimination of well‐known risk factors, such as human papillomavirus, hepatitis B virus, and hepatitis C virus [50]. Further pilot studies and pragmatic trials are needed to guide the implementation and to inform decision models, such that the optimal strategy can be tailored to the population.
Although more than 23 cost‐effectiveness analyses have been performed on the topic of H. pylori screen‐and‐treat, considerable gaps in knowledge and limitations still exist. First, none of the cost‐effectiveness analyses considered the impact of widespread H. pylori screen‐and‐treat on antimicrobial resistance (AMR). This has been challenging given that explicit modeling of AMR requires accounting for biological evolution, human behavior and transmission. As standard Markov‐based and microsimulation models are generally unable to capture interaction, integration of cancer natural history models with infectious disease models is needed, similar to approaches adopted for cervical cancer and human papillomavirus (HPV) [51]. Alternatively, the impact of screen‐and‐treat on AMR rates could be estimated indirectly by modeling the projected increases in antibiotic consumption attributable to screen‐and‐treat, and linking these increases to changes in AMR rates. This approach is similar to that presented in the IARC working group report [52]. Second, few cost‐effectiveness studies considered important side benefits of mass H. pylori eradication. Such side benefits may include the prevention of peptic ulcer disease, dyspepsia and gastric lymphoma [53]. Associations between H. pylori and colorectal cancer have also been established [54, 55]. However, modeling multiple diseases has remained challenging due to the need for separate natural‐history structures, limited data on symptom trajectories and inconsistent definitions across studies. As a result, only two cost‐effectiveness studies considered additional benefits of H. pylori screen‐and‐treat related to the prevention of PUD and dyspepsia [56, 57]. The impact of these ancillary benefits and harms on the cost‐effectiveness of H. pylori screen‐and‐treat could be considerable. Third, many of the evaluated model analyses rely on literature‐based assumptions regarding disease progression and treatment efficacies. As these factors may evolve over time, ongoing model validation and timely updates are warranted. Finally, few cost‐effectiveness analyses have examined the impact of H. pylori screen‐and‐treat programs on health inequalities between subgroups of the target population, such as racial or ethnic minorities or those with lower socioeconomic position.
Most studies included in this article only estimated cost‐effectiveness of one particular strategy for H. pylori screen‐and‐treat. The maximum number of strategies considered did not exceed five. However, many questions remain on the most cost‐effective approach to implementing H. pylori screen‐and‐treat. This includes questions on which test to use, at what age range to screen, with what frequency, with what treatment regimen to eradicate, and whether to test for resistance prior to treatment or successful eradication after treatment.
Cost‐effectiveness is only one part of the financial question of a screening program, budget impact of the strategy being at least as important. An intervention can be highly cost‐effective or even cost‐saving (better health outcome at lower costs), yet the savings occur later in time and investments are needed now before the start of the program. To date, no studies have been performed to help policy makers gain insight into the annual resource requirements of H. pylori screen‐and‐treat. Such decision model studies based on real‐world data from pilot studies are needed for implementation.
New observational evidence and comprehensive decision modeling analyses help address the knowledge gaps identified here. These studies, that capture both the negative and positive side effects of H. pylori screen‐and‐treat, can provide a final verdict on the balance between benefits, harms and resources of this strategy, evaluate the optimal way to implement and provide policy makers with estimates on what resources are needed now for successful implementation of the program. In Europe, the first step in this direction is being made with the TOGAS project and the Joint Action EUCancScreen. Both projects combine local pilot studies with decision modeling to provide policy makers throughout Europe with the essential information to make informed decisions about H. pylori screen‐and‐treat.
Author Contributions
All authors contributed to the study conceptualization and interpretation of the results. Duco T. Mülder and Iris Lansdorp‐Vogelaar performed the data analysis. Duco T. Mülder drafted the manuscript. All authors critically reviewed the manuscript and approved the final version.
Funding
The authors have nothing to report.
Disclosure
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy, or views of the International Agency for Research on Cancer/World Health Organization.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1: Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1I. Lansdorp‐Vogelaar , D. T. Mülder , M. Dinis‐Ribeiro , M. Mc Leod , J. Y. Park , and Y.‐C. Lee , “How to Optimize Cost‐Benefits of H. Pylori Screen‐And‐Treat Programs for Gastric Cancer Prevention,” in Population‐Based Helicobacter Pylori Screen‐And‐Treat Strategies for Gastric Cancer Prevention: Guidance on Implementation (IARC Working Group Reports no 12), ed. J. Y. Park (International Agency for Research on Cancer, 2025).40601795 · pubmed ↗
- 2L. Li , J. L. H. Severens , and O. Mandrik , “Disutility Associated With Cancer Screening Programs: A Systematic Review,” P Lo S One 14, no. 7 (2019): e 0220148.31339958 10.1371/journal.pone.0220148 PMC 6655768 · doi ↗ · pubmed ↗
- 3Y. Sereda , F. Alarid‐Escudero , N. A. Bickell , et al., “Approaches to Developing De Novo Cancer Population Models to Examine Questions About Cancer and Race in Bladder, Gastric, and Endometrial Cancer and Multiple Myeloma: The Cancer Intervention and Surveillance Modeling Network Incubator Program,” JNCI Monographs 2023, no. 62 (2023): 219–230.10.1093/jncimonographs/lgad 021PMC 1100951037947329 · doi ↗ · pubmed ↗
- 4F. Alarid‐Escudero , E. M. Krijkamp , P. Pechlivanoglou , et al., “A Need for Change! A Coding Framework for Improving Transparency in Decision Modeling,” Pharmaco Economics 37, no. 11 (2019): 1329–1339.31549359 10.1007/s 40273-019-00837-x PMC 6871515 · doi ↗ · pubmed ↗
- 5I. Lansdorp‐Vogelaar , R. G. S. Meester , M. Laszkowska , F. A. Escudero , Z. J. Ward , and J. M. Yeh , “Cost‐Effectiveness of Prevention and Early Detection of Gastric Cancer in Western Countries,” Best Practice & Research Clinical Gastroenterology 50 (2021): 101735.33975689 10.1016/j.bpg.2021.101735 · doi ↗ · pubmed ↗
- 6I. Lansdorp‐Vogelaar and L. Sharp , “Cost‐Effectiveness of Screening and Treating Helicobacter pylori for Gastric Cancer Prevention,” Best Practice & Research Clinical Gastroenterology 27, no. 6 (2013): 933–947.24182612 10.1016/j.bpg.2013.09.005PMC 3880867 · doi ↗ · pubmed ↗
- 7M. Areia , R. Carvalho , A. T. Cadime , F. Rocha Gonçalves , and M. Dinis‐Ribeiro , “Screening for Gastric Cancer and Surveillance of Premalignant Lesions: A Systematic Review of Cost‐Effectiveness Studies,” Helicobacter 18, no. 5 (2013): 325–337, 10.1111/hel.12050.23566268 · doi ↗ · pubmed ↗
- 8M. Sarmasti , M. Khoshbaten , F. Khalili , and M. Yousefi , “Cost‐Effectiveness of Screening Helicobacter Pylori for Gastric Cancer Prevention: A Systematic Review,” Journal of Gastrointestinal Cancer 53 (2022): 1–11.34694594 10.1007/s 12029-021-00726-7 · doi ↗ · pubmed ↗