Shifting from an expected to an opportunistic pathogen: Comparison of cases of infant late and very late onset group B streptococcal (GBS) infection in a Canadian city over a 27-year period
Isoken Isah, Sneha Suresh, Gregory J. Tyrrell, Manoj Kumar, Joan L. Robinson, Yung-Fu Chang, Yung-Fu Chang, Yung-Fu Chang, Yung-Fu Chang

TL;DR
This study compares late and very late onset GBS infections in infants, finding that VLOD cases are more complex and may involve GBS acting as an opportunistic pathogen.
Contribution
The study provides new insights into the clinical and epidemiological differences between late and very late onset GBS infections in infants.
Findings
VLOD infants were more likely to be preterm and have complex medical histories compared to LOD infants.
GBS VLOD cases showed higher rates of mechanical ventilation and co-infections with other pathogens.
Serotype III was the most common in both LOD and VLOD cases, but VLOD had a lower proportion.
Abstract
Despite decades of study, the characteristics of infants with invasive group B streptococcus (GBS) late onset disease (LOD) (onset day 7–89 of life) and in particular very late onset disease (VLOD) (after day 89 of life) are not well described. This was a retrospective cohort study of infants hospitalized in four Edmonton hospitals April 1, 1994 through June 30, 2022 with LOD or VLOD GBS invasive disease. Data were collected on demographics, day of onset of infection, clinical manifestations and outcomes. There were 115 episodes of LOD in 111 infants of which 50 infants (45%) were preterm. Onset of initial LOD infection was on median day 27 (IQR 19–40.5) of life. All but one infant was bacteremic while 38/111 (34%) had proven and 17/111 (15%) had possible GBS meningitis. Five of 111 (5%) died before hospital discharge with all deaths probably due to GBS. There were 11 episodes of VLOD…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
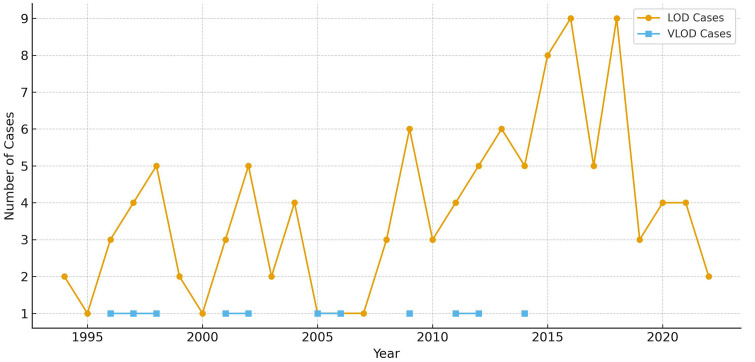 Fig 1
Fig 1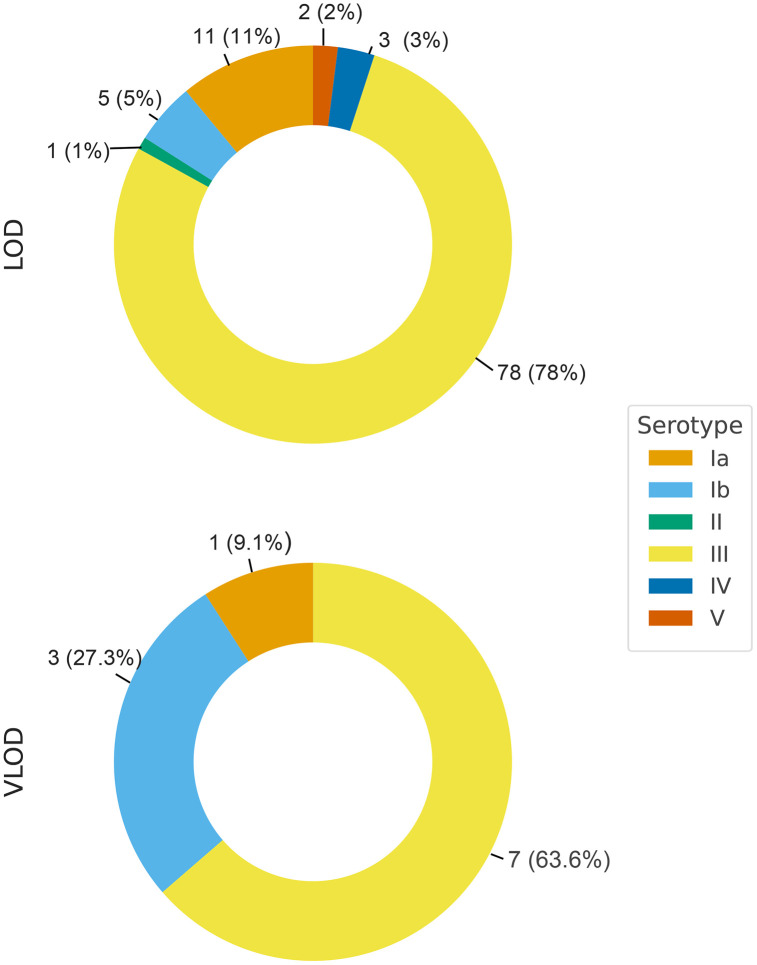 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Preterm Birth and Chorioamnionitis · Streptococcal Infections and Treatments
Introduction
Streptococcal agalactiae, or group B streptococcus (GBS) is part of rectovaginal flora for approximately 10–35% of women [1]. Carriage in pregnancy can lead to neonatal invasive GBS disease; this was a rare entity until the 1970’s when GBS became the leading cause of neonatal sepsis. The reasons for this epidemiologic shift are not clear.
GBS early onset disease (EOD) is transmitted from rectovaginal colonization during labor or at delivery and presents in the first 6 days of life. About 90% of infants present in the first 24 hours of life [2], often with bacteremia and pneumonia. Risk factors for EOD include maternal GBS bacteriuria (an indicator of heavy colonization), chorioamnionitis (as the uterus may contain a high concentration of GBS), prolonged rupture of membranes, preterm delivery (which can be due to symptomatic or subclinical GBS chorioamnionitis) and birth of a previous infant with GBS infection (presumably because the mother does not produce effective GBS antibodies) [1]. Intrapartum antibiotic prophylaxis (IAP) markedly decreases the incidence of EOD [1].
GBS late-onset disease (LOD) occurs day 7–89 and very late onset disease (VLOD) after day 89 of life. Infants with VLOD or LOD typically present with bacteremia with or without a focus [2]. The pathogenesis of GBS acquisition and infection in LOD and VLOD are not established with potential sources being intrapartum transmission [3], the hands of the mother or of other people, breastmilk [1,4], and nosocomial transmission [5] IAP does not change the incidence of LOD [1] so has not been studied for prevention of VLOD.
The objective of this study was to describe and compare the incidence and characteristics of LOD and VLOD in a cohort of neonates in a Canadian city over a prolonged period.
Materials and methods
This was a retrospective study of a cohort of infants born in Edmonton or St. Albert and hospitalized in one of four Edmonton hospitals April 1, 1994 through June 30, 2022 that had GBS isolated from a sterile site (excluding urine) after day 6 of life. LOD was defined as presentation on day 7–89 while VLOD as presentation on day 90–364 of life. In 1997, the initial Society of Obstetricians and Gynecologists of Canada GBS guideline recommended either rectovaginal screening at 35–37 weeks gestation with intrapartum antibiotics for all who screened positive or no screening with intrapartum antibiotics for those with risk factors [6]. In 2004 their guideline was revised to recommend only the former approach [7].
Cases were selected via health records search of inpatients discharges up to 12 months of age with discharge ICD9 CM/ICD10CA diagnostic codes that would capture GBS sepsis (S1 Table). Eligibility was confirmed by chart review. Cross referencing of LOD cases was done through a provincial microbiological database of all infants with GBS isolated from a sterile site up to day 89 of life. Cross referencing was not possible for VLOD cases.
Charts were reviewed and data collected on demographics, day of onset of GBS infection, clinical manifestations and outcomes (S2 Table). Serious bacterial infections (defined as bacteriologically proven infections other than skin or mucous membrane infections) with other pathogens that occurred during the GBS admission were recorded data were accessed from 01/07/2016 to 05/08/2025.
Confirmed meningitis was defined as detection of GBS in cerebrospinal fluid (CSF). Possible meningitis was defined as pleocytosis in culture-negative CSF obtained after minimum one dose of antibiotics. CSF pleocytosis was defined as > 20 X 10^6^/L WBCs up to 28 days of age, > , 10 X 10^6^/L WBCs at days 29–56 [8] and > 5 X 10^6^/L WBCs after 56 days of age. For traumatic lumbar punctures, a ratio of 1000 RBCs:1WBC was applied.
For the 2003–2020 cases, microbiologic data but no clinical data were reported in two previous provincial studies [9,10].
Ethics approval was obtained from the University of Alberta Health Research Ethics Board (Pro00059616) who waived the need for parental consent. They approved entry of anonymized data and date of birth into REDCap.
Data analysis
The data for the characteristics of LOD and VLOD cases was compared to identify any differentiating features among these groups. Chi-square tests were used to compare dichotomous variables, with the use of Fisher’s exact test to estimate statistical significance if the expected cell frequency were <5 for any of the cells in 2x2 tables. Data were analyzed using OpenEpi, an open-source software (Available at www.openepi.com). Data on continuous variables are provided as means with standard deviation (SD) or medians with inter-quartile range, depending on the characteristics of the data distribution. Figures were created with the assistance of ChatGPT (OpenAI, San Francisco, CA).
Capsular polysaccharide (CPS) typing
Neonatal invasive GBS disease is a notifiable disease in Alberta, requiring GBS isolates to be submitted to the Alberta Public Health Laboratory for CPS typing [9]. Prior to January 2017, CPS typing was performed using a double immunodiffusion method with CPS-specific antisera [11]. From 2017 on, a real-time PCR assay was used [12].
Results
Screening of discharge codes yielded 842 infants of which 122 had confirmed LOD or VLOD.
Late onset disease (day 7–89 of life)
There were 111 infants with 115 episodes of culture-confirmed GBS LOD (37 with positive blood and CSF cultures, 1 with positive CSF cultures only and 77 with positive blood cultures). Onset of the initial episode of LOD was on median day 27 (IQR 19–40.5) of life; 47 (42%) were male and 50 (45%) were preterm (data on birth gestation missing for 3 cases) (Table 1). At the time of GBS infection, 69 (62%) were receiving breast milk (66 mother’s own milk and 3 donor human milk) while 5 (5%) required parenteral nutrition.
Table 1: Comparison of LOD and VLOD cases.
At least one CSF was obtained from 108 of the 115 episodes (94%); 38 (35%) were culture-positive (19 obtained prior to antibiotics, 19 after at least one dose antibiotics) and 70 (65%) were culture-negative (22 obtained prior to antibiotics, 42 after at least one dose antibiotics and 6 with unknown timing). For 17 of the CSFs obtained after antibiotics or with unknown timing, there was CSF pleocytosis so the total number of episodes with confirmed (N = 38) or possible (N = 17) meningitis was 55 (48%). Eight cases had more than one positive CSF culture with these occurring day 1 (N = 1), day 2 (N = 2), day 3 (N = 2) day 4 (N = 2) and day 13 (N = 1) after the initial positive culture.
In addition to bacteremia and/ or meningitis, local sites of infection included adenitis (N = 2), omphalitis (N = 1), cellulitis (N = 3), adenitis and cellulitis (N = 1), and omphalitis and cellulitis (N = 1). Another 7 infants had positive urine cultures for GBS in addition to positive blood or CSF cultures. There were no musculoskeletal infections.
Three of the 111 infants had EOD before the episode of LOD including one infant who went on to have two episodes of LOD. That infant was born at 36 weeks gestation and had GBS bacteremia without a focus on days 6, 19 and 45 of life. No explanation was established but breastfeeding was stopped after the second recurrence as breast milk and infant throat culture grew GBS. Another three infants had two episodes of LOD. A 28-week GA infant had meningitis on day 13 and bacteremia with no focus on day 43 of life (5 days after a 25-day course of antibiotics ended). A 29-week GA infant had bacteremia with no focus on day 39 and day 56 of life (7 days after a 10-day course of antibiotics ended). The third infant born at 27 weeks GA had LOD days 19 and day 36 of life (4 days after a 13-day course of antibiotics for bacteremia ended) with possible meningitis in the second episode (CSF pleocytosis in a culture-negative bloody tap obtained after antibiotics were given).
Fourteen of the 111 infants (13%) were discharged on anticonvulsants; 11 of these had confirmed and 2 had possible meningitis. Four infants had documented hearing loss, of whom 2 had meningitis. Three infants required ventriculoperitoneal shunts.
Five of 111 infants (5%) died before hospital discharge; 4 died on day 0–5 of treatment for GBS and one had withdrawal of care after GBS treatment was completed.
The number of cases over time is shown in Fig 1.
Number of cases of GBS LOD and VLOD over time.
Serotypes from 100 of the 111 infants are shown in Fig 2 with 78 (78%) being serotype III (For the four infants with two episodes of LOD, serotypes were identified only on the initial isolate). Data were omitted from one infant as serotype III was identified in blood and serotype V in CSF; it seems likely that one of these results was incorrect, but specimens are no longer available for retesting.
GBS serotypes from LOD and VLOD cases N (%).
Very late onset disease (day 90–364)
There were 11 VLOD cases presenting on median day 116 (IQR 103–138) (range 93–207) of life (Table 1) (2 with positive blood and CSF cultures, 1 with positive CSF cultures only and 8 with positive blood and negative CSF cultures). Three infants were male (27%) and 8 (73%) were preterm. None had been diagnosed with chronic medical conditions at the time of GBS onset. Nine were bacteremic and two had only positive CSF cultures.
CSF was obtained from all 11 cases. Three (27%) were culture-positive (2 obtained prior to antibiotics and 1 after at least one dose antibiotics) and 8 (73%) were culture-negative (3 obtained prior to antibiotics, 5 after at least one dose antibiotics). None of the 5 with negative cultures obtained after antibiotics had CSF pleocytosis.
Local sites of infection included 3 cases (27%) with cellulitis, none of whom had meningitis.
One of the 11 VLOD cases (9%) (with meningitis) was discharged on anticonvulsants. Six (55%) had normal hearing when tested while the other 5 (45%) were not tested. None had prior or subsequent GBS infections. All survived to discharge. Serotypes were Ia (N = 1; 9%)), Ib (N = 3; 27%), and III (N = 7; 64%) (Fig 2).
The number of cases overtime is shown in Fig 1 with there never being more than one VLOD case per year.
Comparison of LOD to VLOD cases
As compared with infants with LOD, those with VLOD were less likely to be born vaginally (n = 3/11 [27%] versus n = 72/111 [65%] p = 0.036), more likely to be mechanically ventilated during their birth hospitalization (n = 5/11 [45%] versus n = 17/111 [15%]; p = 0.039); and more likely to have serious bacterial infections with other pathogens during their GBS admission (n = 3/11 [27%] versus n = 4/111 [4%]); p = 0.032) (Table 1). The proportion of isolates that were serotype III did not differ between LOD and VLOD cases (P = 0.51).
Discussion
Over a 27-year period in Edmonton hospitals, there was a mean of 4.3 infants per year with GBS invasive disease with onset after day 6 of life (range 1–10 infants). Approximately 10% had VLOD (11 of 122). Statistically significant differences between LOD and VLOD were a higher incidence of vaginal delivery with LOD, and a higher incidence of mechanical ventilation during birth hospitalization and serious bacterial infection with pathogens other than GBS noted with VLOD. This suggests that a risk factor for VLOD is having a complicated neonatal course.
From provincial data, the incidence of LOD in Alberta increased from 0.15 to 0.41 per 1000 live births from 2003 to 2020 for unclear reasons [9,10]. Data from the current study cannot be used to look at the incidence of LOD or VLOD as the proportion of infants with these conditions admitted to Edmonton hospitals is not known.
EOD always arises from intrapartum transmission due to high-grade GBS colonization. For LOD and VLOD, it is not clear when transmission of GBS most commonly occurs, i.e., intrapartum, from the mother after delivery (from GBS on her hands or from breastmilk), from nosocomial transmission, or from the community.
A 2022 systematic review of LOD reported an odds ratio (OR) of 2.67 (95% confidence interval (CI): 2.07–3.45) for maternal GBS colonization [13]. Furthermore, a prospective cohort of 100 infants with LOD reported that 30 of 47 mothers (64%) had GBS colonization [3]. In the current study, almost half of all infants with LOD where colonization status was known were born to those with colonization and almost half were preterm. In one study, IAP was associated with later presentation of LOD and milder disease [3]. This all suggests that intrapartum transmission accounts for some LOD.
Even less is known about the source of GBS or the characteristics of VLOD. Because of this, we completed a narrative review of the literature for VLOD case series. This identified 352 cases in 13 studies dating back to 1995 (Table 2) [14–26]. Three were population based studies that reported the incidence per 1000 live births: LOD 0.36 (95% CI: 0.31–0.42) and VLOD 0.03 (95% CI: 0.01–0.04) in New Zealand 2012–2021 [14], LOD 0.20 (95% CI: 0.17–0.23) and VLOD 0.012 (95% CI: 0.007–0.021) in Norway 1996–2012 [15], and LOD 0.12 (95% CI 0.11–0.14), and VLOD 0.01 (95% CI 0.01–0.02) in Japan 2011–2015 [16]. The upper age limit for VLOD was 6 months in the New Zealand study and 12 months in the other two studies. Combining data from the 7 studies that included cases up to 1 year of age [15–20. 22], there were 2242 cases of EOD, 2668 of LOD and 265 of VLOD – again indicating that as in our study, VLOD cases account for about 10% of GBS cases after 6 days of age. For the 10 studies that reported GA [14,17–26], 82 of 208 infants (39%) were preterm (versus 73% on the current study). Seven studies reported clinical presentation [15,17,18,22–24,26] with 64 of 187 infants (34%) having meningitis (versus 27% in the current study), 94 (54%) having bacteremia with no focus mentioned in the manuscript (versus 45% in the current study) and 20 (11%) having bacteremia with a likely focus: urinary tract infection (N = 7); cellulitis (n = 4); septic arthritis (N = 3); central line associated blood stream infection (N = 2); infective endocarditis (N = 2) and a bullous rash (N = 1).
Table 2: Literature review of case series of VLOD due to GBS.
In the literature review, a risk factor for VLOD as compared to LOD + /- EOD included prematurity in 4 studies [17,22,24,25] and male gender in 3 studies [17,20,22] (Table 2). However, combining data from the 6 studies that reported gender with our study [17,19,21–24,26], 95 of 176 VLOD cases were male (54%), so it seems unlikely that there is a true gender predominance. Another risk factor for VLOD in one study was the presence of underlying disorders (not further defined) [17]. A major limitation is that underlying disorders would often not yet be diagnosed at the time of LOD or VLOD presentation so are not reliably mentioned in published studies. Immune deficiency is thought to lead to some cases of VLOD. In the review of the literature, at least 2 of the 352 VLOD cases had human immunodeficiency virus and one study reported that 3 of 28 cases had “immunodeficiency”. There is a case report of a child with IRAK-4 deficiency who presented with GBS meningitis at 5 months of age [28]. A recurrent case of VLOD has also been reported in a child with thoracic congenital lymphatic dysplasia (which is associated with CD4 lymphopenia and hypogammaglobulinemia) with two episodes of bacteremia 5 months apart starting at 2 years of age [29]. In our cohort, VLOD infants were more likely to have serious bacterial infections with pathogens other than GBS, which could signal a defect in host defense. However immune deficiency was not limited to VLOD cases, as one of our infants with LOD (GBS meningitis at 15 days of age) went on to be diagnosed with an Nf kappa B pathway immune deficiency that also affected toll-like receptor (TLR) function similar to IRAK-4 deficiency. The correlation between inborn errors of immunity that affect TLR function and VLOD/LOD GBS disease needs further study.
In the literature review, in terms of severity of illness, one study reported at least a trend towards a higher risk of neurodevelopmental disorders (NDD) and of death with VLOD than with EOD or LOD (P value not provided) [15] while another study reported the opposite – a decreased risk of NDD or death with VLOD than with LOD [23] (Table 2). In the current study, there were no deaths in 11 VLOD cases versus 5 deaths in 111 infants with LOD; neurodevelopmental outcomes were not captured. One previous study reported a lower risk of ICU admission with VLOD than with LOD and EOD combined [21].
It is possible that the pathogenicity of certain serotypes of GBS predisposes to later onset disease. Serotype III is the most common cause of both EOD and LOD infant invasive GBS in the literature [30] and in the current study. Sequence type 17 and its associated virulence factor HvGA are associated with infant invasive GBS, with the majority of these cases being serotype III [30]; unfortunately, such testing was not available for the isolates from the current study.
Serotyping was reported for 180 of the 352 VLOD cases in the literature review [16,17,19,20,25,26] including 87 (48%) serotype III, 44 (24%) serotype Ia, 17 (9%) serotype Ib, 13 (7%) serotype V, 10 (6%) serotype II, 5 (3%) serotype VI, 3 (2%) serotype IV and 1 (1%) serotype IX. In in our cohort, serotype III was also the most common accounting for 64% of VLOD cases ((Fig 2). In the literature review, some VLOD cases were with uncommon serotypes (VI: N = 5; XI: N = 1) and there is a case report of VLOD meningitis due to serotype IX presenting at 120 days of age [31]. This may further support the hypothesis that a defect in host defense is sometimes the culprit in VLOD, as less pathogenic serotypes of GBS are sometimes responsible for VLOD cases.
It has been postulated that VLOD has the same origins and clinical course as LOD, occurring in infants who were typically more preterm so present at an older chronological age [24]. However, this does not explain VLOD cases in term babies, which accounted for 61% of cases in the literature review (Table 2) and about one-third of cases in the current study. Our review of the VLOD literature suggests that the risk factors, clinical course, serotypes and outcomes are broadly similar to those of LOD.
Limitations of the study are all those typical of a retrospective chart review. Serotyping data was incomplete.
In conclusion, our study shows that VLOD accounts for about 10% of GBS disease after 6 days of age, but there are only relatively small studies looking at this important cause of morbidity and mortality. While prematurity is a risk factor in previous studies, further exploration into defects in infant microbial defense, particularly innate immune defects, is warranted. It seems possible that infant GBS shifts from being an expected pathogen to an opportunistic one with maturity and that an immune disorder should be considered in infants with VLOD.
Supporting information
S1 TableDischarge screening codes.ICD9 CM and ICD19 CA Discharge Codes used for health records retrieval.(DOCX)
S2 TableCase report form.REDCap form used for data collection.(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coggins SA, Puopolo KM. Neonatal Group B Streptococcus Disease. Pediatr Rev. 2024;45(2):63–73.38296778 10.1542/pir.2023-006154 PMC 10919294 · doi ↗ · pubmed ↗
- 2Manuel G, Twentyman J, Noble K, Eastman AJ, Aronoff DM, Seepersaud R, et al. Group B streptococcal infections in pregnancy and early life. Clin Microbiol Rev. 2025;38(1):e 0015422. doi: 10.1128/cmr.00154-22 39584819 PMC 11905376 · doi ↗ · pubmed ↗
- 3Berardi A, Rossi C, Creti R, China M, Gherardi G, Venturelli C, et al. Group B streptococcal colonization in 160 mother-baby pairs: a prospective cohort study. J Pediatr. 2013;163(4):1099-104.e 1. doi: 10.1016/j.jpeds.2013.05.064 23866714 · doi ↗ · pubmed ↗
- 4Ching NS, Buttery JP, Lai E, Steer AC, Standish J, Ziffer J, et al. Breastfeeding and Risk of Late-Onset Group B Streptococcal Disease. Pediatrics. 2021;148(3):e 2020049561. doi: 10.1542/peds.2020-049561 34385351 · doi ↗ · pubmed ↗
- 5Collin SM, Lamb P, Jauneikaite E, Le Doare K, Creti R, Berardi A, et al. Hospital clusters of invasive Group B Streptococcal disease: A systematic review. J Infect. 2019;79(6):521–7. doi: 10.1016/j.jinf.2019.11.008 31733233 · doi ↗ · pubmed ↗
- 6Society of Obstetricians and Gynaecologists of Canada. Statement on the prevention of early-onset group B streptococcal infections in the newborn. J SOGC. 1997;19:751–8.
- 7Money DM, Dobson S, Canadian Paediatric Society, Infectious Diseases Commitee. RETIRED: The prevention of early-onset neonatal group B streptococcal disease. J Obstet Gynaecol Can. 2004;26(9):826–40. doi: 10.1016/s 1701-2163(16)30157-8 15361281 · doi ↗ · pubmed ↗
- 8Kestenbaum LA, Ebberson J, Zorc JJ, Hodinka RL, Shah SS. Defining cerebrospinal fluid white blood cell count reference values in neonates and young infants. Pediatrics. 2010;125(2):257–64. doi: 10.1542/peds.2009-1181 20064869 PMC 3033868 · doi ↗ · pubmed ↗