Intramyocardial dissecting haematoma with false pseudoaneurysm
Diana Isabel Katekaru-Tokeshi, Moisés Jiménez-Santos, Eric Kimura-Hayama

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
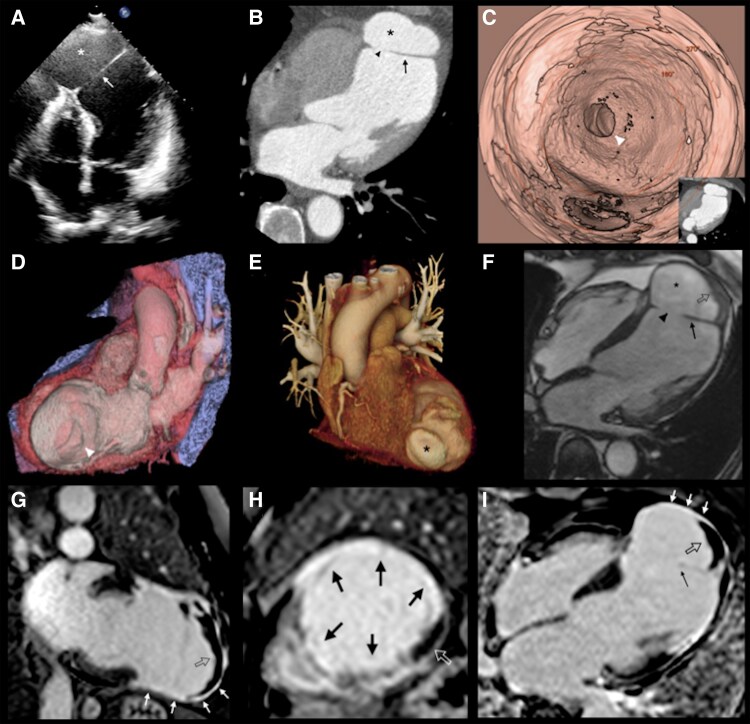 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Trauma Management and Diagnosis · Cardiovascular Issues in Pregnancy
Case description
A 76-year-old man with dyspnoea of moderate efforts. Three months ago he had a myocardial infarction that was thrombolyzed 6 h after the onset of precordial pain at another institution. ECG showed Q waves in II, AVF, and from V_2_ to V_6_ leads.
Transthoracic echocardiography evidenced severe left ventricular (LV) systolic dysfunction (ejection fraction of 25%) with anterior severe hypokinesis and apical akinesia. Also it noted the presence of a thin and mobile rounded cavity at the apical level connecting the LV with a large cavity apparently contained by the pericardium, suggestive of a contained rupture (see Figure 1A, Supplementary material, S1). Coronary angiography reported proximal occlusion of the left anterior descending artery.
(A) Transthoracic echocardiography apical four-chamber (4C) view showing a dissection flap at the apical level (arrow) connecting the left ventricle with a large cavity (). (B) An axial view of cardiac CT confirmed the defect of the myocardial wall (arrowhead) connecting the left ventricle with the cavity () previously described by TTE and apparently contained by the pericardium. A false pseudoaneurysm was considered. (C-D). Virtual CT ventriculoscopy and long axial 3D VR image with lateral cut showing the defect (arrowhead) in the myocardial wall communicating with the abnormal cavity of the false-pseudoaneurysm. (E) Cardiac CT VR reconstruction allowed the visualization of false-pseudoaneurysm from its surface (). (F) CMR apical 4C view with cine showed the presence of thrombus (open arrow) within the false pseudoaneurysm (), and the communication (arrowhead) through the thinned myocardial wall (arrow). (G–I). CMR Phase-Sensitive Inversion Recovery (PSIR) late gadolinium enhancement reconstructions involving the mid-segment of the anterior wall and apical segments (black arrows) and thrombus (open arrow) surrounded by enhancing overlying pericardium (white arrows).
The cardiac CT demonstrated more clearly the defect in the myocardial wall communicating with the abnormal cavity compatible with a false pseudoaneurysm (Figure 1B–E). Cardiovascular MR revealed the presence of a laminar thrombus that was surrounded by enhancing overlying pericardium and a transmural late gadolinium enhancement involving the mid-segment of the anterior wall and apical segments of both the left and right ventricles suggesting non-viable myocardium (Figure 1F–I). The right ventricular function was 56% without regional wall motion abnormality and CMR confirmed the severe decrease in LVEF (see Supplementary material S2).
Intramyocardial dissection (ID) is an extremely rare mechanical complication of myocardial infarction,^1^ due to the rupture of intramyocardial vessels causing infiltration of blood into and through the myocardial wall. ID can be contained within the myocardium, known as a contained myocardial rupture or closed ID, or in late stages, and the ID tears into the LV cavity and may cause an open ID, also known as a false pseudoaneurysm.^2^
The patient is currently undergoing medical treatment with functional class III.
This case demonstrates the importance of multimodality cardiac imaging for assessment post-infarction mechanical complications in its different clinical stages.
Lead author biography
Diana Isabel Katekaru-Tokeshi is a medical doctor graduate from the National Major San Marcos University (Lima, Perú). She got a Cardiology Diploma from the Residency Programme at Hospital Militar Central (Lima, Perú) and fellowship in Cardiac Computed Tomography and Cardiac Magnetic Resonance at “Instituto Nacional de Cardiologia Ignacio Chavez” (Mexico). Now works as attending cardiologist at Hospital Nacional Dos de Mayo (Lima, Perú). Her main fields of interest are congenital heart and ischaemic heart disease.
Supplementary Material
ytag124_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moral S, Martinez-Ballart S, Ballesteros E, Brugada R. Ventricular intramyocardial dissecting hematoma: what is its true clinical evolution and the best treatment? JACC Case Rep 2023;28:102085.38204536 10.1016/j.jaccas.2023.102085 PMC 10774762 · doi ↗ · pubmed ↗
- 2Carrión-Sánchez I, Tejada-González C, Gómez-Delgado J, Párraga R, Cobiella J, De Agustín JA, et al Role of multimodality cardiac imaging for evaluation of intramyocardial dissection, from dissecting haematoma to false-pseudoaneurysm: a case series. European Heart Journal—Case Reports 2024;8:ytae 219.38745731 10.1093/ehjcr/ytae 219PMC 11091479 · doi ↗ · pubmed ↗