Case report of extensive embolic complications in culture-negative mitral valve endocarditis due to Rothia dentocariosa
Hing Yin Wilson Lam

TL;DR
A man with culture-negative mitral valve endocarditis caused by Rothia dentocariosa had severe embolic complications and was successfully treated with valve replacement after molecular diagnosis.
Contribution
This case highlights the use of next-generation sequencing to identify a rare pathogen in culture-negative endocarditis and the importance of multidisciplinary care.
Findings
NGS identified Rothia dentocariosa from a calf abscess in a case of culture-negative endocarditis.
Multidisciplinary care and timely valve replacement improved outcomes despite neurological complications.
Persistent vegetations and embolic risk necessitated surgical intervention after medical stabilization.
Abstract
Culture-negative infective endocarditis presents significant diagnostic and therapeutic challenges, especially in patients with systemic embolic complications. A middle-aged man with a history of intravenous drug use presented with fever, new apical systolic murmur, and widespread embolic phenomena affecting the brain, spleen, kidneys, and lower limb. Transthoracic echocardiography revealed a large posterior mitral leaflet vegetation with moderate–severe mitral regurgitation. Blood and tissue cultures were negative. Next-generation sequencing (NGS) of an aspirated calf muscle abscess identified Rothia dentocariosa. Despite prolonged antimicrobial therapy and multidisciplinary care, persistent vegetations and high embolic risk prompted mitral valve replacement after interval stabilization of intracranial haemorrhages. He recovered without recurrent emboli and with stable prosthetic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
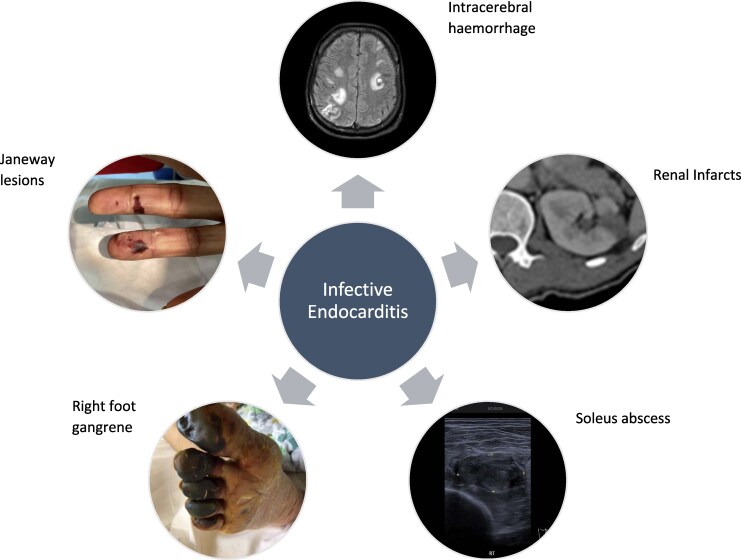 Figure 1
Figure 1 Figure 1
Figure 1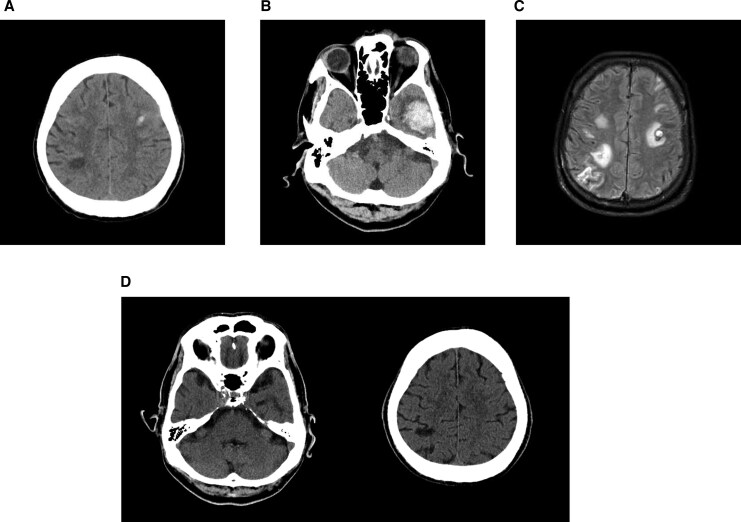 Figure 2
Figure 2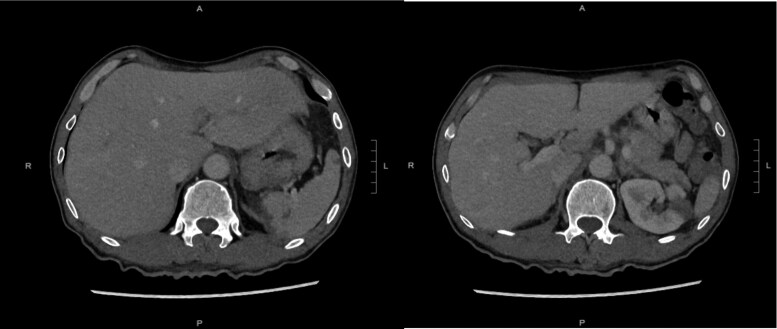 Figure 3
Figure 3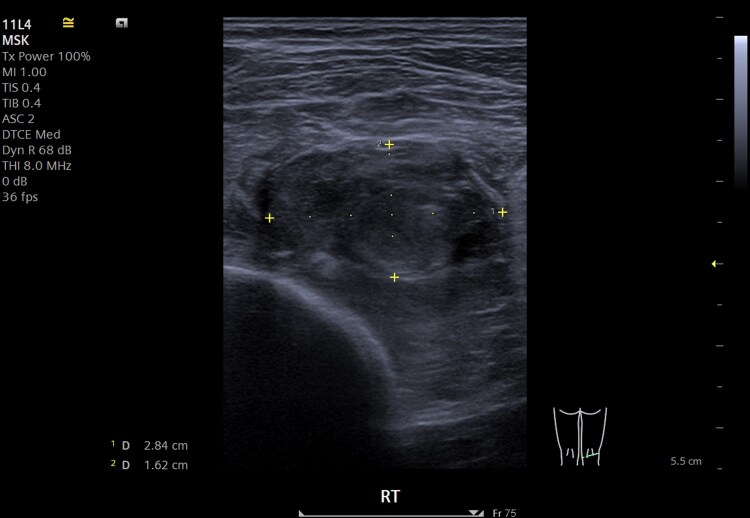 Figure 4
Figure 4| Hospital day/event | WBC (×10⁹/L) (3.7–9.2) | Hb (g/dL) (13.4–17.0) | Plt (×10⁹/L) (145–370) | Creatinine (µmol/L) (65–109) | Urea (mmol/L) (3.1–7.8) | ALT (U/L) (<53) | ALP (U/L) (43–105) | Total bilirubin (µmol/L) (<22) | C-reactive protein (mg/L) (<5.0) | ESR (mm/h) (<32) | Antibiotic regimen |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Day 0 (admission) | 25.4 | 12.5 | 235 | 96 | 7.5 | 114 | 200 | 32 | Day 0–1: piperacillin–tazobactam | ||
| Day 1 | 208 | – | |||||||||
| Day 2 | – | ||||||||||
| Day 4 | 253 | 57 | Day 4–6: ceftriaxone + ampicillin | ||||||||
| Day 6 | 153 | – | |||||||||
| Day 13 | 120 | – | |||||||||
| Day 17 | 109 | – | Day 18–82: ceftriaxone | ||||||||
| Day 18 | – | ||||||||||
| Day 35 | 38 | – | |||||||||
| Day 38 | 28 | – | |||||||||
| Day 54 | 26 | 76 | |||||||||
| Day 60 | 123 | 89 | |||||||||
| Day 62 | 67 | 87 | |||||||||
| Day 63 | 51 | 79 | |||||||||
| Day 67 | 41 | 63 | |||||||||
| Day 74 | 153 | 101 | |||||||||
| Day 76 | 86 | 64 | |||||||||
| Day 81 | 34 | 102 | |||||||||
| Day 82 | From Day 82: antibiotics stopped | ||||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiphtheria, Corynebacterium, and Tetanus · Infective Endocarditis Diagnosis and Management · Infections and bacterial resistance
Introduction
Blood culture-negative infective endocarditis (BCNIE) accounts for up to 20% of infective endocarditis (IE) cases and is associated with delayed diagnosis and high mortality.^1^ Rothia dentocariosa, a Gram-positive coccobacillus, is a rare cause of IE, most often linked to dental disease or intravenous drug use (IVDU). Next-generation sequencing (NGS) can assist diagnosis when conventional microbiology is unrevealing.
We report a case of BCNIE with extensive embolic complications in which R. dentocariosa was identified by NGS from a peripheral abscess. This case illustrates the diagnostic value of molecular techniques in BCNIE and the complexity of surgical timing in a patient with large vegetations, multisystem embolization and intracerebral haemorrhage.
Summary figure
Blood culture-negative infective endocarditis (mitral valve) with extensive embolic complications
Case presentation
A 58-year-old male smoker with previous IVDU was found on the floor at home and brought to the hospital with fever and altered mental state. He had no known chronic illness or cardiac disease. His history was limited, and he denied chest pain or dyspnoea.
On admission (Day 0), his temperature was 38°C; blood pressure 116/66 mmHg, pulse 97/min, and oxygen saturation 97% on room air. He required no vasopressors or respiratory support. Examination revealed poor oral hygiene, a new apical systolic murmur, and peripheral stigmata of IE (Osler’s nodes and Janeway lesions).
Initial investigations (Table 1) showed leucocytosis and elevated high-sensitivity troponin I (peak 7750 ng/L). A 12-lead electrocardiogram showed sinus tachycardia without ischaemic changes. Chest radiography was unremarkable. Urine toxicology was positive for methamphetamine.
Transthoracic echocardiography (TTE) on Day 6 (Figure 1A; Supplementary material online, Video S1A/B) showed a mildly enlarged left atrium, preserved biventricular systolic function, and a 2.3 × 1.0 cm mobile vegetation on the posterior mitral leaflet with moderate–severe mitral regurgitation (MR). Right ventricular systolic pressure was 26 mmHg. No pericardial effusion was present.
(A) Baseline transthoracic echocardiography showed posterior mitral valve leaflet vegetation 2.3 × 1.0 cm. (B) Transthoracic echocardiography after complete 11-week ceftriaxone showed persistent infective endocarditis over mitral valve > 1 cm. (C) Transthoracic echocardiography of post-mitral valve (MV) replacement showed MV prosthesis in situ, and there is no obvious leakage seen. The mean pressure gradient across MV prosthesis is 5 mmHg.
Multiple blood and fungal cultures were negative. Serology for atypical pathogens (including Bartonella spp., Brucella spp., Coxiella burnetii, Chlamydia spp., and Mycoplasma pneumoniae) was negative. Autoimmune screening, complement levels, and serum protein electrophoresis were unremarkable. Dental assessment found no active source, and there had been no recent dental procedure.
Empirical antibiotics were commenced on Day 0 and adjusted following infectious diseases review (Table 1). Therapy was consolidated to ceftriaxone monotherapy for a total of 11 weeks. He remained afebrile and the leucocytosis resolved, but C-reactive protein fluctuated between 26 and 153 mg/L (normal < 5 mg/L).
The hospital course was complicated by multifocal embolic events.
Neurological: Within 24 h, he developed dysarthria and facial asymmetry. Computer tomography (CT) of brain on Day 1 (Figure 2A) showed right parietal hypodensities and a small left frontoparietal intracerebral haemorrhage (ICH). Repeat CT on Day 3 (Figure 2B) showed a new large left temporal ICH with additional small bilateral frontal haemorrhages. Magnetic resonance imaging (MRI) on Day 14 (Figure 2C) demonstrated multiple rim-enhancing lesions, including one with acute haemorrhage, consistent with septic emboli and haemorrhagic transformation. Follow-up CT on Day 84 (Figure 2D) confirmed resolution of haemorrhage and maturation of infarcts. His neurological deficits resolved to baseline. CT angiography showed no mycotic aneurysm, and neurosurgical intervention was not required.
(A) Brain CT showed right parietal hypodensity and a small left frontoparietal intracerebral haemorrhage. (B) Repeat CT on follow-up revealed a new large left temporal lobe haemorrhage. (C) MRI (T2 fluid-attenuated inversion recovery (FLAIR)) demonstrated multiple rim-enhancing lesions. (D) Subsequent brain CT showed resolution of intracerebral haemorrhage.
Systemic: Contrast-enhanced CT of the abdomen and pelvis demonstrated multiple splenic and renal infarcts without abscess formation (Figure 3), consistent with systemic embolization.
CT of the abdomen and pelvis showed splenic and renal infarcts.
Musculoskeletal and vascular: By Week 3, he developed right foot gangrene. Lower limb CT angiography showed rim-enhancing abscesses in the right flexor hallucis longus and soleus muscles (largest 2.2 cm) and a tibioperoneal trunk pseudoaneurysm (3.4 × 2.9 × 5.5 cm). The posterior tibial artery reconstituted distally via collateral vessels. Ultrasound-guided aspiration and drainage of the calf abscess were performed on Day 19 (Figure 4). Conventional cultures were negative, but NGS of the aspirate identified R. dentocariosa 16S rRNA gene. As limb perfusion was stable, vascular and orthopaedic teams advised conservative management of the pseudoaneurysm and dry gangrene with close follow-up.
Ultrasound-guided drainage of right soleus muscle abscess.
Despite prolonged antibiotics, repeat TTE on Day 79 showed a persistent mobile vegetation > 1 cm and ongoing moderate–severe MR (Figure 1B; Supplementary material online, Video S2). After multidisciplinary review, and once interval neuroimaging confirmed ICH resolution, surgical mitral valve replacement with a 29 mm bioprosthesis was performed ∼3 months after admission. Preoperative transoesophageal echocardiography (TEE) confirmed a 1.4 cm mobile vegetation on P2 with a flail segment and severe eccentric MR. Intraoperatively, two ∼1 cm vegetations were found on P2 with ruptured chordae at A1, precluding valve repair. The excised valve was culture negative. Postoperative TTE (Figure 1C; Supplementary material online, Video S3) showed a well-seated prosthesis with no paravalvular leak.
Recovery was uneventful, and at 1-month follow-up, he was asymptomatic with normalized inflammatory markers.
Discussion
This case highlights challenges in BCNIE, including diagnostic uncertainty despite extensive investigations, the value of molecular diagnostics, the high embolic risk of large mobile mitral vegetations, and the need to individualize surgical timing after ICH.
The 2023 European Society of Cardiology (ESC) guidelines recommend a structured BCNIE pathway incorporating repeat blood cultures, targeted serology, pathogen-specific polymerase chain reaction (PCR), and consideration of non-bacterial thrombotic endocarditis.^2^ Despite broad testing, conventional microbiology and serology were unrevealing in our patient.
Rothia dentocariosa is a rare cause of IE with few cases reported.^3^ Risk factors include periodontal disease, recent dental manipulation, and IVDU.^4^ In this case, NGS of a drained calf abscess identified R. dentocariosa, providing a plausible aetiology when standard cultures were negative. A limitation is the absence of molecular testing on the excised valve, which would have strengthened causal attribution.
There are no guideline-specific antibiotic recommendations for R. dentocariosa endocarditis, and treatment is informed by case reports and susceptibility patterns. Reported regimens include penicillin for 4–6 weeks with or without gentamicin, and ceftriaxone monotherapy has also been described.^5^ In this patient, the NGS result supported prolonged ceftriaxone in the context of persistent vegetation, extensive embolization, and fluctuating inflammatory markers.
The extent of embolization to the brain, abdominal organs, and peripheral vasculature is consistent with the recognized embolic risk associated with large, mobile left-sided vegetations. This reinforces the importance of early multimodality imaging and coordinated multidisciplinary care.
The major management dilemma was surgical timing. The ESC guidelines recommend urgent surgery (within 3–5 days) for patients with vegetations ≥ 1 cm following an embolic event to reduce the risk of further embolization.^2^ In the presence of ICH, however, they give a Class IIa recommendation to defer surgery for >1 month where possible, with frequent clinical and imaging reassessment to minimize neurological risk. In our patient, persistent large vegetation and ongoing inflammatory activity suggested medical therapy alone was insufficient, yet early cardiopulmonary bypass carried substantial neurological risk. Delayed surgery with prolonged antimicrobial therapy and serial neuroimaging enabled mitral valve replacement once ICH had resolved.
Percutaneous vegetation aspiration has emerged as a potential bridge to surgery in selected high-risk patients,^6^ but experience is predominantly in right-sided or device-related infection. Evidence for left-sided disease remains limited, and it is not standard care. Potential risks include systemic embolization, valve or chordal injury, and intraprocedural anticoagulation-related bleeding, with uncertain long-term outcomes. Given severe MR, persistent large vegetation, and intraoperative evidence of extensive leaflet and chordal destruction, definitive surgical valve replacement rather than repair was the most appropriate strategy in this patient.
Conclusion
Blood culture-negative infective endocarditis due to rare organisms may require molecular diagnostics such as NGS when conventional testing is unrevealing. In patients with large mitral vegetations complicated by intracranial haemorrhage, surgical timing should be individualized through multidisciplinary assessment balancing embolic and neurological risks.
Lead author biography
Hing Yin Wilson Lam graduated from the University of Hong Kong. He is currently working in the Department of Medicine, Yan Chai Hospital. He is interested in interventional cardiology and percutaneous coronary intervention.
Supplementary Material
ytag097_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin KP, Yeh TK, Chuang YC, Wang LA, Fu YC, Liu PY. Blood culture negative endocarditis: a review of laboratory diagnostic approaches. Int J Gen Med 2023;16:317–327.36718144 10.2147/IJGM.S 393329 PMC 9884005 · doi ↗ · pubmed ↗
- 2Delgado V, Marsan NA, de Waha S, Bonaros N, Brida M, Burri H et al ESC Guidelines for the management of endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). Eur Heart J 2023;44:3948–4042. https://doi.org/10.1093/eurheartj/ehad 19337738322 10.1093/eurheartj/ehad 625 · doi ↗ · pubmed ↗
- 3Elkattawy S, Alyacoub R, Younes I, Mowafy A, Noori M, Mirza M. A rare report of Rothia dentocariosa endocarditis. J Community Hosp Intern Med Perspect 2021;11:413–415.34234918 10.1080/20009666.2021.1880539 PMC 8118413 · doi ↗ · pubmed ↗
- 4Franconieri F, Join-Lambert O, Creveuil C, Auzou M, Labombarda F, Aouba A, et al Rothia spp. Infective endocarditis: a systematic literature review. Infect Dis Now 2021;51:228–235.33164836 10.1016/j.medmal.2020.10.021 · doi ↗ · pubmed ↗
- 5Chowdhary M, Farooqi B, Ponce-Terashima R. Rothia dentocariosa: a rare cause of left-sided endocarditis in an intravenous drug user. Am J Med Sci 2015;350:239–240.26241376 10.1097/MAJ.0000000000000539 · doi ↗ · pubmed ↗
- 6Marinacci LX, Sethi SS, Paras ML, El Sabbagh A, Secemsky EA, Sohail MR, et al Percutaneous mechanical aspiration for infective endocarditis: proceedings from an inaugural multidisciplinary summit and comprehensive review. J Soc Cardiovasc Angiogr Interv 2024;3:102283.39807229 10.1016/j.jscai.2024.102283 PMC 11725074 · doi ↗ · pubmed ↗