Clinical outcomes and safety of eravacycline in hematology: a multicenter, real-world study
Jun Wang, Jun Zhu, Wen Wu, Rongmu Luo, Zhengyin Liu, Zhaohui Tong, Tongwen Sun, Yingchun Xu, Depei Wu

TL;DR
This study shows eravacycline is effective and safe for treating infections in hematology patients, especially against drug-resistant bacteria.
Contribution
The study provides real-world evidence of eravacycline's clinical effectiveness and safety in hematology patients with multidrug-resistant infections.
Findings
Eravacycline showed an 88.8% overall clinical response rate in hematology patients.
The antibiotic was highly effective against Klebsiella pneumoniae and Acinetobacter baumannii.
Only 2.5% of patients experienced adverse events, indicating good safety.
Abstract
Hematology patients are highly susceptible to severe bacterial infections, particularly those caused by multidrug-resistant (MDR) gram-negative pathogens, which are associated with significant morbidity and mortality. Eravacycline, a novel fluorocycline antibiotic, demonstrates broad-spectrum activity against MDR bacteria. This real-world study aimed to evaluate the effectiveness and safety of eravacycline in Chinese hematology patients. In this multicenter, retrospective study, hematology patients receiving ≥3 days of eravacycline between September 2023 and September 2024 were included. The outcomes included clinical response rate, microbiological response rate, and safety. Of 796 patients included, most had hematological diseases (94.6%) and recent chemotherapy or radiotherapy (80.2%). The most common infection was pneumonia (57.4%), and sputum (47.2%) was the most frequent specimen…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
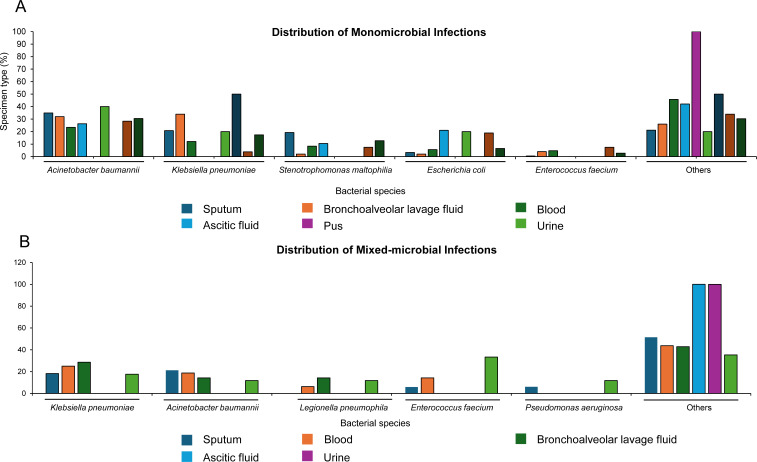 Fig 1
Fig 1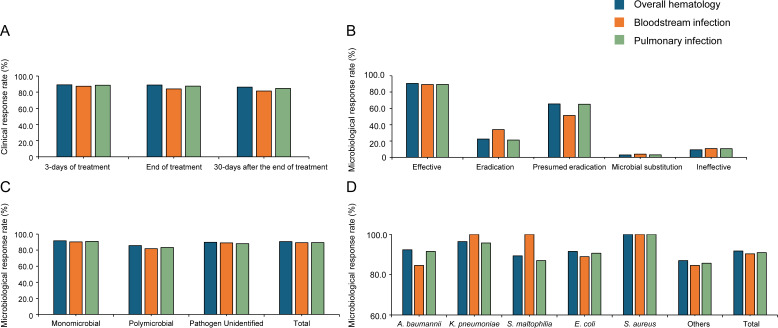 Fig 2
Fig 2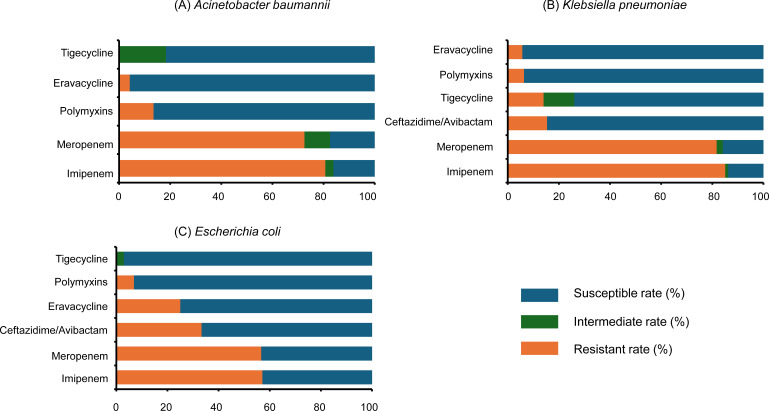 Fig 3
Fig 3| Characteristic | Patients, |
|---|---|
| Age (years), median (range) | 49.0 (18.0–89.0) |
| Male | 469 (58.9) |
| Comorbidities | |
| Hematological diseases | 753 (94.6) |
| Acute myeloid leukemia | 345 (43.3) |
| Acute lymphoblastic leukemia | 79 (9.9) |
| Others | 372 (46.7) |
| Pulmonary diseases | 455 (57.2) |
| Cardiovascular diseases | 114 (14.3) |
| Hypertension | 67 (8.4) |
| Cardiac insufficiency | 13 (1.6) |
| Others | 34 (4.3) |
| Neutropenia | 594 (74.6) |
| Sepsis | 101 (12.7) |
| Diabetes | 80 (10.1) |
| Kidney disease | 59 (7.4) |
| Nervous system disease | 21 (2.6) |
| Rheumatic immune diseases | 20 (2.5) |
| Other underlying diseases and comorbidities | 110 (13.8) |
| High risk factor associated with immunosuppression | |
| Chemotherapy/radiotherapy within 1 month | 638 (80.2) |
| Long-term use of corticosteroids/immunosuppressants | 460 (57.8) |
| Transplantation | 260 (32.7) |
| AIDS | 5 (0.6) |
| Splenectomy | 6 (0.8) |
| Infection sites | |
| Pneumonia | 457 (57.4) |
| Abdominal infection | 48 (6.0) |
| Bloodstream infections | 58 (7.3) |
| Pneumonia + bloodstream infections | 71 (8.9) |
| Pneumonia + abdominal infection | 30 (3.8) |
| Abdominal infection + bloodstream infection | 5 (0.6) |
| Pneumonia + abdominal infection + bloodstream infection | 8 (1.0) |
| Others | 119 (14.9) |
| Laboratory tests, median (IQR) | |
| White blood cell count (×109/L) | 2.0 (0.4–5.8) |
| Outlier | 640 (80.4) |
| Neutrophil count (×109/L) | 1.0 (0.1–3.5) |
| Outlier | 578 (72.6) |
| Neutrophil ratio (%) | 53.7 (20.0–79.6) |
| Outlier | 544 (68.3) |
| C-reactive protein (mg/L) | 54.7 (19.5–111.6) |
| Outlier | 676 (84.9) |
| Procalcitonin (ng/mL) | 0.7 (0.2–2.6) |
| Outlier | 787 (98.9) |
| SOFA score, median (IQR) | 2.5 (2.0–4.0) |
| Eravacycline-based regimen | |
| Monotherapy | 402 (50.5) |
| Combination | 394 (49.5) |
| Eravacycline + polymyxins | 70 (8.8) |
| Eravacycline + carbapenems | 15 (1.9) |
| Eravacycline + aminoglycosides | 8 (1.0) |
| Eravacycline + ceftazidime-avibactam | 2 (0.3) |
| Other | 65 (8.2) |
| Unknown | 234 (29.4) |
| Dosage of eravacycline | |
| 1 mg/kg q12h | 778 (97.7) |
| ≤7 days | 370 (46.5) |
| 7–14 days | 287 (36.1) |
| >14 days | 121 (15.2) |
| 50 mg q12h | 15 (1.9) |
| ≤7 days | 8 (1.0) |
| 7–14 days | 6 (0.8) |
| >14 days | 1 (0.1) |
| Other | 3 (0.4) |
| Factor | After 3 days | End of treatment | |||
|---|---|---|---|---|---|
| Clinical response rate (%) | Clinical response rate (%) | ||||
| Sex | 0.527 | 88.8 | 0.432 | ||
| Male | 469 (58.9) | 88.5 | 89.6 | ||
| Female | 327 (41.1) | 89.9 | 87.8 | ||
| Comorbidities | |||||
| Hematological diseases | 753 (94.6) | 89.2 | 0.513 | 88.8 | 0.924 |
| Pulmonary diseases | 455 (57.2) | 86.4 | 0.005 | 86.2 | 0.006 |
| Sepsis | 101 (12.7) | 86.1 | 0.312 | 80.2 | 0.003 |
| Other underlying diseases and comorbidities | 110 (13.8) | 81.8 | 0.009 | 88.2 | 0.819 |
| Infection sites | |||||
| Pneumonia | 457 (57.4) | 88.4 | 0.483 | 88.8 | 0.982 |
| Abdominal infection | 48 (6.0) | 87.5 | 0.719 | 91.7 | 0.518 |
| Bloodstream infections | 58 (7.3) | 87.9 | 0.773 | 91.4 | 0.52 |
| Laboratory tests | |||||
| White blood cell count | 640 (80.4) | 88.6 | 0.383 | 88.9 | 0.874 |
| Neutrophil count | 578 (72.6) | 88.8 | 0.642 | 89.1 | 0.682 |
| Neutrophil ratio | 544 (68.3) | 87.9 | 0.11 | 87.9 | 0.211 |
| C-reactive protein | 677 (85.1) | 88.9 | 0.698 | 88.2 | 0.156 |
| Procalcitonin | 787 (98.9) | 89.1 | 0.986 | 88.7 | 0.284 |
| SOFA score | 426 (53.5) | 86.9 | 0.032 | 88.5 | 0.757 |
| <Median | 213 (50.0) | 89.2 | 0.013 | 91.1 | 0.116 |
| ≥Median | 213 (50.0) | 84.5 | 0.013 | 85.9 | 0.116 |
| Eravacycline-based regimen | |||||
| Monotherapy | 402 (50.5) | 92.0 | 0.007 | 90.8 | 0.074 |
| Combination | 394 (49.5) | 86.0 | 0.007 | 86.8 | 0.074 |
| Dosage of eravacycline | |||||
| 1 mg/kg q12h | 778 (97.7) | 88.8 | 0.133 | 88.8 | 0.992 |
| ≤7 days | 370 (46.5) | 83.0 | <0.001 | 82.2 | < 0.001 |
| 7–14 days | 287 (36.1) | 96.9 | <0.001 | 95.5 | < 0.001 |
| >14 days | 121 (15.2) | 87.6 | 0.574 | 93.4 | 0.083 |
| 50 mg q12h | 15 (1.9) | 100.0 | 0.171 | 86.7 | 0.789 |
| ≤7 days | 8 (1.0) | 100.0 | 0.319 | 75.0 | 0.213 |
| 7–14 days | 6 (0.8) | 100.0 | 0.389 | 100.0 | 0.383 |
| >14 days | 1 (0.1) | 100.0 | 0.726 | 100.0 | 0.723 |
| Adverse event | Any grade, |
|---|---|
| Any adverse event | 20 (2.5) |
| Nausea | 12 (1.5) |
| Vomiting | 12 (1.5) |
| Hepatic enzyme increased | 7 (0.9) |
| Infusion reaction | 5 (0.6) |
| Rash | 2 (0.3) |
| Hypocalcemia | 1 (0.1) |
| Dizziness | 1 (0.1) |
| Amylase increased | 1 (0.1) |
| Lipase increased | 1 (0.1) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Neutropenia and Cancer Infections · Infections and bacterial resistance
INTRODUCTION
Hematology patients are more susceptible to serious infection, of which bacterial infections—especially gram-negative—were the most clinically relevant issue, carrying increased morbidity and mortality (1, 2). Despite preferred antibiotics recommended in the clinical practice, the emergence of multidrug-resistant (MDR) gram-negative bacilli, such as Escherichia coli and Klebsiella pneumoniae, has complicated the optimal treatment option and posed a significant challenge to clinicians and public health (1, 3, 4). In the context of the urgent global crisis of antimicrobial-resistant infections, new antibiotic therapy with a wider range of activity is needed.
Eravacycline is the first fully synthetic fluorocycline and exerts broad-spectrum activity against anaerobes, gram-negative bacteria, and gram-positive bacteria, such as extended-spectrum β-lactamase (ESBL)-producing Enterobacterales, carbapenem-resistant Enterobacterales (CRE), methicillin-resistant Staphylococcus aureus (MRSA), and vancomycin-resistant enterococci (5, 6). Based on the non-inferiority from the IGNITE 1 and IGNITE 4 trials, eravacycline has received approval for the treatment of complicated intra-abdominal infections (cIAIs) (7, 8). Although several retrospective studies provided valuable evidence for clinical practice of eravacycline outside the prospective trial settings, real-world evidence remains limited, with the small sample size and the absence of Asian experience and data on clinically relevant infections in hematology (9–12). In the present study, we retrospectively evaluated the effectiveness and safety of eravacycline in hematology patients with multidrug-resistant infections across China.
MATERIALS AND METHODS
Study design and sample
This retrospective, multicenter, real-world study included patients from the department of hematology between September 2023 and September 2024 at 71 centers across China. Eligible patients received eravacycline for at least 3 days. Patients who participated concurrently in clinical trials or received eravacycline prophylactically only were excluded from this study.
Data collection and outcomes
We retrospectively collected the patient data from electronic medical records, including baseline characteristics (underlying diseases and infection sites), microbiological data (pathogen identification and antimicrobial susceptibility results), details of treatment regimens (including dosage, treatment duration, and combination therapies), infection-related symptoms, signs, auxiliary examinations, and any adverse events (AEs). Patients’ records were manually reviewed to confirm drug administration and documentation of adverse events. Data were then pooled into a single secure database.
The outcomes included clinical response rate (defined as complete resolution of infection-related symptoms, signs, and ancillary tests, with confirmed or presumed pathogen eradication, or as significant improvement in these parameters with at least one not fully normalized), microbiological response rate (defined as pathogen eradication, presumed eradication, or microbial substitution [replacement by non-primitive pathogens]), and safety. Normal body temperature was defined as a temperature of <37.3°C maintained for at least 24 h, based on both Chinese and international infectious disease criteria. Mixed-microbiological infection was defined as the isolation of two or more different pathogenic microorganisms from the same infection site or specimen.
For minimum inhibitory concentrations (MICs), all cultures, bacterial identifications, and antibiotic susceptibilities were conducted according to local procedures at each center. Clinical Laboratory Standards Institute (CLSI)/European Committee on Antimicrobial Susceptibility Testing (EUCAST)/Food and Drug Administration (FDA)/China Antimicrobial Susceptibility Testing (ChinaCAST) breakpoints were used to interpret MIC results, where applicable. AEs were monitored and recorded by the investigators, and the severity was graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.0.
Statistical analysis
Descriptive statistics were employed to evaluate baseline characteristics. Frequencies and percentages were used to report categorical variables, while continuous data were described using median and interquartile range (IQR) or mean and standard deviation, depending on the normality of the distribution. Statistical comparisons of clinical response rates according to baseline characteristics were performed using the chi-squared test. All statistical tests were two-sided, with significance set at P values of <0.05. IBM SPSS Statistics version 29 (IBM Corp., Armonk, NY) was used to carry out the analysis.
RESULTS
Baseline characteristics
From September 2023 to September 2024, 796 patients receiving ≥3 days of eravacycline in the department of hematology were included. Baseline characteristics are summarized in Table 1. The median age was 49.0 (range, 18–89) years, and the majority of the patients were male (58.9%). Hematological diseases (94.6%, mainly including acute myeloid leukemia and acute lymphoblastic leukemia), pulmonary diseases (57.2%), and cardiovascular diseases (14.3%, mainly including hypertension and cardiac insufficiency) were the most common comorbidities. Almost all the patients had high risk factors associated with the immunosuppression, the most common being chemotherapy/radiotherapy within 1 month (80.2%). Over half of the patients were diagnosed with pneumonia (57.4%). Half of the patients (50.5%) underwent eravacycline monotherapy, and the rest (49.5%) underwent eravacycline-based combination therapies. The median scores of sequential organ failure assessment (SOFA) were 2.5 (IQR, 2.0–4.0). Almost all (97.7%) patients received the standard dose of 1 mg/kg/12 h. The average administration period of eracycline was 8.9 (range, 3–52) days.
Microbiological characteristics
Among the 481 patients with microbiological examination results, 446 (92.7%) were infected by a single pathogen, and 35 (7.3%) were infected by mixed pathogens. Among single-pathogen infections, Acinetobacter baumannii was the most common (30.5%), followed by K. pneumoniae (17.4%), Stenotrophomonas maltophilia (12.7%), E. coli (6.5%), and Enterococcus faecium (2.7%). The predominant source of A. baumannii was sputum (n = 74), followed by blood (n = 25) and bronchoalveolar lavage fluid (n = 16). K. pneumoniae spp. were mainly derived from sputum (n = 44) and bronchoalveolar lavage fluid (n = 17, Fig. 1A and Table S1). Of 76 mixed-pathogen infections, the most common pathogens were K. pneumoniae (19.7%), A. baumannii (17.1%), E. faecium (11.1%), Legionella pneumophila (5.3%), and Pseudomonas aeruginosa (5.3%), with the predominant source of sputum (n = 33, Fig. 1B and Table S2).
Distribution of monomicrobial infections (A) and mixed-microbial infections (B).
Clinical and microbiological effectiveness
A total of 732 patients had available data on defervescence. The mean time to return to normal body temperature was 3.2 ± 2.1 days, with no significant difference observed in patients receiving eravacycline combination. Laboratory test indicators, including C-reactive protein, procalcitonin, and SOFA score, were decreased both at 3 days and at the end of treatment (Fig. S1).
The clinical response rates at 3 days, the end, and 30 days after the end of eravacycline treatment were 89.1%, 88.8%, and 86.2%, respectively. At 3 days, 79 patients (9.9%) showed no clinical response, and 8 (1.0%) had died. At the end of treatment, 59 (7.4%) were non-responsive and 30 (3.8%) had died. Within 30 days after the end of eravacycline treatment, 33 (4.1%) remained non-responsive and 75 (9.4%) deaths occurred. Patients with bloodstream infections achieved clinical response rates of 87.3% at 3 days, 84.0% at the end of treatment, and 81.4% at 30 days after the end of treatment. In patients with pulmonary infections, the clinical response rates were 88.6%, 87.5%, and 84.6% at the corresponding time points, respectively (Fig. 2A). At the end of treatment, the overall microbiological response rate was 90.7%, with a pathogen eradication rate of 22.4% and a presumed eradication rate of 65.5% (Fig. 2B). When stratified by infection site, patients achieved microbiological response rates of 91.7% in monomicrobial infections and 85.7% in polymicrobial infections (Fig. 2C). Eravacycline demonstrated both clinical and microbiological response rates of A. baumannii and K. pneumoniae (Fig. 2D; Fig. S2).
Clinical and microbiological response rates in patients with different infection sites. (A) Clinical response rates at different time points. (B) Microbiological response rates in patients with different infection sites. (C) Microbiological response rates in monomicrobial and polymicrobial pathogen infections. (D) Microbiological response rates in different pathogen species. Abbreviations: A. baumannii, Acinetobacter baumannii; K. pneumoniae, Klebsiella pneumoniae; S. maltophilia, Stenotrophomonas maltophilia; E. coli, Escherichia coli; S. aureus, Staphylococcus aureus.
Subgroup analysis showed that pulmonary diseases (P = 0.005), other underlying diseases and comorbidities (P = 0.009), monotherapy (P = 0.007), combination (P = 0.007), eravacycline treatment at a dosage of 1 mg/kg/12 h for ≤7 days (P < 0.001) and 7–14 days (P < 0.001) were significantly associated with clinical response rate after 3 days, and pulmonary diseases (P = 0.006), sepsis (P = 0.003), duration ≤7 days (P < 0.001) and between 7–14 days (P < 0.001) of 1 mg/kg/12 h eravacycline treatment showed significant associations for clinical response rate at the end of treatment (Table 2). At the eravacycline dosage of 1 mg/kg/12 h, clinical response rate was significantly higher with a treatment duration of 7–14 days than with <7 days, both at 3 days and at the end of treatment.
Antimicrobial susceptibility test results
The susceptibility rates of A. baumannii to eravacycline, tigecycline, and polymyxins were 94.3%, 81.7%, and 93.7%. The resistant rates of A. baumannii to imipenem and meropenem were 80.6% and 72.5% (Fig. 3A). K. pneumoniae showed susceptibility to eravacycline and tigecycline of 94.3% and 74.0%, with similar resistance to both imipenem (85.1%) and meropenem (81.7%; Fig. 3B). Eravacycline and tigecycline showed strong activity against E. coli, with susceptibility rates of 75.0% and 97.1%, respectively. E. coli displayed resistance to carbapenems, with 57.1% resistant to imipenem and 56.7% to meropenem (Fig. 3C). S. aureus demonstrated full susceptibility to both eravacycline and tigecycline (Fig. 3). S. maltophilia susceptibility to eravacycline could not be formally interpreted due to limited data and absence of established criteria. However, its MIC values were low overall, with a median MIC of 0.13 μg/mL, MIC_50_ of 0.5 μg/mL, MIC_90_ of 0.75 μg/mL, and inhibition zone diameters ranging from 6 to 30 mm.
Susceptibility rates of pathogens to antimicrobial agents. (A) Acinetobacter baumannii. (B) Klebsiella pneumoniae. (C) Escherichia coli.
Safety
Detailed AEs are summarized in Table 3. Among the 796 patients included in this study, 20 patients (2.5%) reported AEs, of whom 13 (65%) had received an eravacycline-based combination. The most frequent AEs were nausea (1.5%), vomiting (1.5%), increased hepatic enzyme (0.9%), infusion reaction (0.9%), and rash (0.6%). After eravacycline treatment, 69 (8.7%) patients underwent rescue therapy with other antibiotics. Thirteen patients (1.6%) experienced organ failure. Seventy-seven patients (9.7%) were admitted to the intensive care unit due to infection or infection-related complications, with a median length of stay of 7 (range, 1–134) days. A total of 84 patients (10.6%) died, including 30 (3.8%) due to infections and 54 (6.8%) due to non-infectious causes.
DISCUSSION
This study provides the first antibacterial profile evidence supporting the clinical and microbiological effectiveness and safety of eravacycline, particularly in hematology patients with infections. Our study has demonstrated that eravacycline showed clinically promising effectiveness and safety, with the clinical response rate and microbiological response rate at 88.8% and 90.7%, respectively. Eravacycline showed high susceptibility rates against MDR pathogens, such as A. baumannii and K. pneumoniae. Infrequent AEs and no new safety signals were observed, indicating that eravacycline was administered safely in hematology patients. To our knowledge, it represents the largest real-world observational investigation of eravacycline conducted in China to date. It is expected that the accumulation of clinical experience and data from China will contribute to the global evidence on eravacycline for clinical application and informing antimicrobial stewardship worldwide, ultimately benefiting patients.
Among the 796 patients from the hematology department, eravacycline, administered either as monotherapy or in combination, demonstrated an overall clinical response rate of 88.8%, which was comparable to the reported effectiveness of conventional carbapenems (7, 8, 13, 14). To further evaluate its pathogen-specific effectiveness beyond general clinical outcomes, we analyzed the microbiological response rates. Microbiological effectiveness analysis showed overall response rates of 90.7%, with 91.7% for monomicrobial infections and 85.7% for polymicrobial infections, indicating that eravacycline is effective both as monotherapy and in combination regimens against a broad range of pathogens. For patients in critical condition, combination regimens are recommended. Given that patients in this study presented with multiple concurrent infections and resistance to various gram-negative pathogens, the observed clinical effectiveness of eravacycline is especially meaningful—particularly in the context of patients with multiple underlying comorbidities. The majority of patients (83.9%) were eventually discharged with clinical improvement, with a small proportion of deaths due to infections (30/796, 3.8%). Additionally, the IGNITE1 and IGNITE4 trials were limited to a specific infection site (i.e., cIAI) rather than other sites with more common A. baumannii infections, such as pulmonary, blood, and urine (9). In comparison, our study enriches the limited real-world data in Asian populations with clinical response rates of 84.0% and 87.5% in patients with bloodstream and pulmonary infections, respectively, supporting the potential of eravacycline as a treatment option for challenging infections such as CRE, ESBL, MRSA, and S. maltophilia.
Early defervescence is frequently regarded as a surrogate marker of treatment effectiveness (15). The mean time to return to normal body temperature was 3.2 ± 2.1 days in our study, indicating a relatively rapid response to eravacycline. The observed result supports the clinical utility of eravacycline in hematology patients who are often immunocompromised and at elevated risk of infection-related complications (15–17). Subgroup analysis further revealed that the duration of eravacycline therapy had a significant impact on clinical outcomes. Specifically, treatment durations of ≤7 days at the standard dose of 1 mg/kg were associated with lower clinical response rates (P < 0.001), while patients receiving eravacycline for 7–14 days exhibited significantly improved clinical response rates (P < 0.001). These results prompt us to consider optimizing treatment duration based on individual patient factors such as infection severity, pathogen resistance profiles, and immunologic status. The findings regarding antibiotic duration should be interpreted with caution due to the retrospective design of the study. Nevertheless, ensuring adequate dosage and a full course of treatment remains essential to achieving optimal therapeutic outcomes.
Clinical guidelines have reported the limited susceptibility of imipenem and meropenem against gram-negative pathogens, particularly K. pneumoniae and A. baumannii (18, 19). Consistently, our study also identified high resistance rates to both carbapenems among clinical isolates. Nevertheless, we also observed favorable clinical effectiveness of eravacycline despite the high prevalence of carbapenem resistance. In contrast, eravacycline demonstrated higher in vitro susceptibility against K. pneumoniae and A. baumannii, surpassing even tigecycline, another commonly used tetracycline antibiotic. Structurally, eravacycline is a synthetic fluorocycline antibacterial agent closely related to tigecycline, with two key modifications on the D-ring of its tetracycline core: a fluorine atom replaces the dimethylamine moiety at C-7, and a pyrrolidinoacetamido group replaces the 2-tertiary-butyl glycylamido at C-9. These structural enhancements confer two- to fourfold greater potency against most aerobic gram-negative pathogens than tigecycline (20). This structural advantage may help explain the higher susceptibility rates and the promising clinical effectiveness observed in our study. In addition, our study observed that E. coli showed higher susceptibility to tigecycline compared to eravacycline (97.1% vs 75.0%). This finding may be attributed to the use of the FDA breakpoints (2, 4, and 8 mg/L) for tigecycline, which could potentially overestimate its susceptibility, as the EUCAST has lowered the clinical susceptibility breakpoint of tigecycline to ≤0.5 mg/L. Thus, susceptibility data should be interpreted with caution, considering the differences in breakpoint standards and their clinical implications.
In terms of safety, 20 out of 796 patients (2.5%) reported any AEs. The most frequently observed AEs included gastrointestinal disorders (nausea [1.5% vs 4.8%−8.1%] and vomiting [1.5% vs 3.6%]), and hepatic enzyme increased (0.9%), lower than the known safety profile reported in the IGNITE 1 and 4 trials, with no new safety signals (7, 8). Compared with previous clinical trials and real-world analysis of other antibiotic and tetracyclines, the incidence of AEs in this study, such as nausea and vomiting, was far lower, even in patients receiving combination regimens, suggesting the favorable tolerability of eravacycline in real-world settings (5, 7, 8, 21–25).
Certain limitations of our study should be acknowledged. First, the selection biases were inevitable due to the non-randomized and retrospective nature of the study. Second, although centralized microbiological testing was not performed, standardized methods for microbiological testing were adopted across all centers. Despite its imperfections, these real-world data may provide complementary references for clinicians in hematology by reflecting the performance of eravacycline in routine clinical practice. Future prospective multicenter studies are warranted to further validate these findings and define the optimal use of eravacycline within antimicrobial stewardship frameworks.
Conclusion
In conclusion, eravacycline demonstrated good effectiveness and safety in treating infections of patients in the hematology department. Given the limited clinical experience with eravacycline in Chinese populations, our study may provide valuable real-world evidence to guide clinical decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. 2024. Infectious Diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis:ciae 403. doi:10.1093/cid/ciae 40339108079 · doi ↗ · pubmed ↗
- 2Fritsche G. 2021. Clinically relevant infections in hematology and oncology: bacterial infections and the role of novel antibiotics in times of multidrug resistance. memo 14:292–297. doi:10.1007/s 12254-021-00702-8 · doi ↗
- 3Moja L, Zanichelli V, Mertz D, Gandra S, Cappello B, Cooke GS, Chuki P, Harbarth S, Pulcini C, Mendelson M, et al.. 2024. WHO’s essential medicines and A Wa Re: recommendations on first- and second-choice antibiotics for empiric treatment of clinical infections. Clin Microbiol Infect 30:S 1–S 51. doi:10.1016/j.cmi.2024.02.00338342438 · doi ↗ · pubmed ↗
- 4Meschiari M, Asquier-Khati A, Tiseo G, Luque-Paz D, Murri R, Boutoille D, Falcone M, Mussini C, Tattevin P, Tropical D, Infectious D. 2024. Treatment of infections caused by multidrug-resistant Gram-negative bacilli: a practical approach by the Italian (SIMIT) and French (SPILF) Societies of Infectious Diseases. Int J Antimicrob Agents 64:107186. doi:10.1016/j.ijantimicag.2024.10718638688353 · doi ↗ · pubmed ↗
- 5Alosaimy S, Abdul-Mutakabbir JC, Kebriaei R, Jorgensen SCJ, Rybak MJ. 2020. Evaluation of eravacycline: a novel fluorocycline. Pharmacotherapy 40:221–238. doi:10.1002/phar.236631944332 · doi ↗ · pubmed ↗
- 6Zhanel GG, Baxter MR, Adam HJ, Sutcliffe J, Karlowsky JA. 2018. In vitro activity of eravacycline against 2213 Gram-negative and 2424 Gram-positive bacterial pathogens isolated in Canadian hospital laboratories: CANWARD surveillance study 2014–2015. Diagn Microbiol Infect Dis 91:55–62. doi:10.1016/j.diagmicrobio.2017.12.01329338931 · doi ↗ · pubmed ↗
- 7Solomkin J, Evans D, Slepavicius A, Lee P, Marsh A, Tsai L, Sutcliffe JA, Horn P. 2017. Assessing the efficacy and safety of eravacycline vs ertapenem in complicated intra-abdominal infections in the investigating gram-negative infections treated with eravacycline (IGNITE 1) trial: a randomized clinical trial. JAMA Surg 152:224–232. doi:10.1001/jamasurg.2016.423727851857 · doi ↗ · pubmed ↗
- 8Solomkin JS, Gardovskis J, Lawrence K, Montravers P, Sway A, Evans D, Tsai L. 2019. IGNITE 4: results of a phase 3, randomized, multicenter, prospective trial of eravacycline vs meropenem in the treatment of complicated intraabdominal infections. Clin Infect Dis 69:921–929. doi:10.1093/cid/ciy 102930561562 PMC 6735687 · doi ↗ · pubmed ↗