Implementation of a decision aid to promote shared decision-making on mode of birth in low-risk pregnant women: a cross-sectional study within the QUALI-DEC hybrid trial
Truc Phuong Nguyen, Ana Pilar Betran, Guillermo Carroli, Charles Kaboré, Pisake Lumbiganon, Quoc Nhu Hung Mac, Celina Gialdini, Camille Etcheverry, Barbara Vololonarivelo, Kristi Sidney Annerstedt, Ramón Escuriet, Claudia Hanson, Allison Shorten, Alexandre Dumont

TL;DR
A decision aid tool helped low-risk pregnant women make informed choices about their mode of birth, improving communication and satisfaction in four low- and middle-income countries.
Contribution
Demonstrates the effectiveness of a decision aid in promoting shared decision-making in maternity care in low- and middle-income settings.
Findings
DAT users were more likely to identify risks/benefits of each mode of birth and communicate their preferences.
DAT users were less likely to prefer caesarean section and reported higher satisfaction with their birth experience.
Use of the DAT was associated with improved knowledge and no adverse outcomes.
Abstract
Implementing shared decision-making (SDM) in maternity care remains challenging in low-income and middle-income countries (LMICs). Decision aids can support SDM, but evidence on their effectiveness in such settings is limited. We assessed the impact of a decision analysis tool (DAT) for pregnant women on mode of birth (MOB) within the QUALIty DECision-making project, a multisite, multicountry pragmatic trial to reduce unnecessary caesarean sections. We conducted a cross-sectional survey among postpartum women considered at low risk for caesarean section in early pregnancy and who delivered in 32 hospitals across Argentina, Burkina Faso, Thailand and Viet Nam. Associations between DAT exposure and selected outcomes were analysed using multilevel, multivariate regression models adjusting for confounders and cluster effects. Of 2368 women included, 249 (11%) had used it outside antenatal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
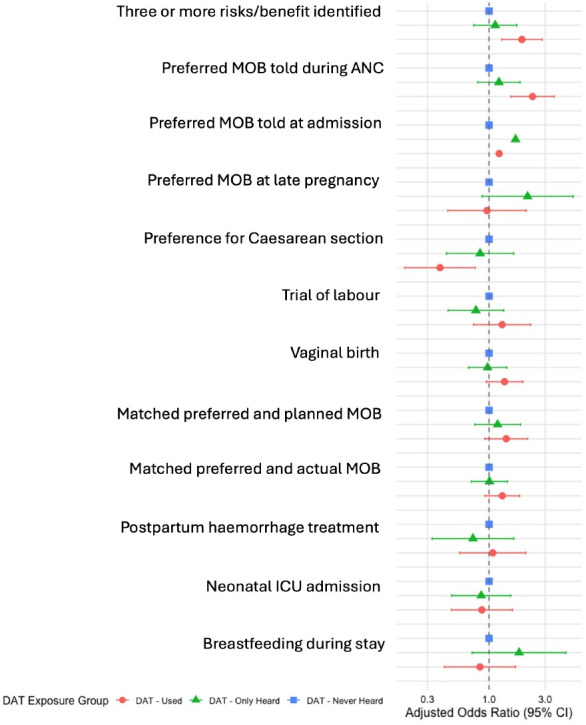 Figure 1
Figure 1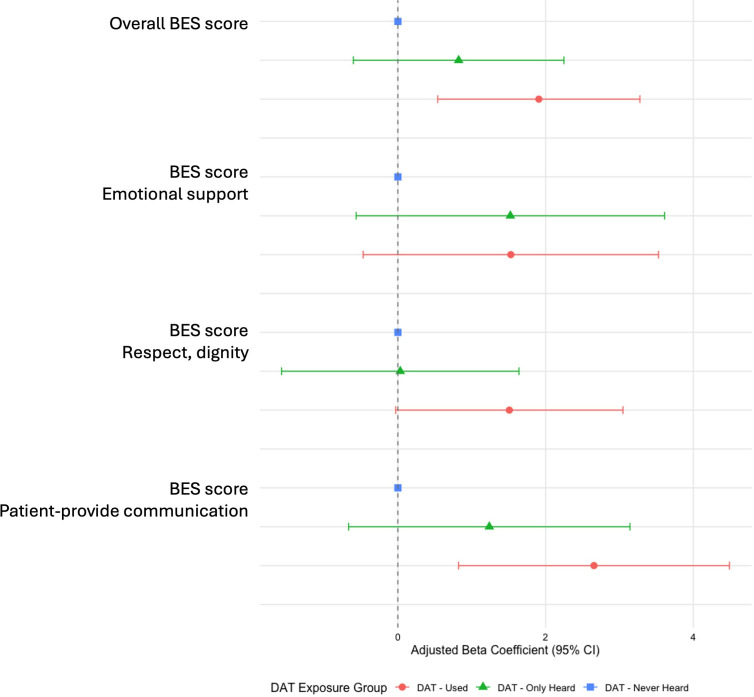 Figure 2
Figure 2| Characteristic | Used | Only heard | Never Heard | P value |
|---|---|---|---|---|
| Country of residence | <0.001 | |||
| Argentina | 111 (45) | 53 (25) | 310 (16) | |
| Burkina Faso | 7 (2.8) | 21 (9.9) | 721 (38) | |
| Thailand | 38 (15) | 36 (17) | 461 (24) | |
| Viet Nam | 93 (37) | 102 (48) | 415 (22) | |
| Marital status | 0.2 | |||
| Married/living with a partner | 243 (98) | 206 (98) | 1752 (96) | |
| Separated/single/widow | 5 (2) | 4 (1.9) | 65 (3.6) | |
| Maternal age | 0.036 | |||
| <25 | 83 (33) | 60 (28) | 719 (38) | |
| 25–34 | 123 (49) | 122 (58) | 912 (48) | |
| ≥35 | 43 (17) | 30 (14) | 276 (14) | |
| Education level | 0.041 | |||
| Secondary or lower | 167 (67) | 154 (73) | 1421 (75) | |
| Tertiary education | 82 (33) | 58 (27) | 486 (25) | |
| Geographic context | <0.001 | |||
| Rural | 64 (26) | 71 (33) | 411 (22) | |
| Urban | 185 (74) | 141 (67) | 1496 (78) | |
| Maternal occupation | <0.001 | |||
| Employed formal sector | 76 (31) | 61 (29) | 371 (19) | |
| Employed informal sector | 75 (30) | 81 (38) | 721 (38) | |
| Unemployed/housewife | 98 (39) | 70 (33) | 814 (43) | |
| Partner’s occupation | 0.013 | |||
| Employed formal sector | 91 (40) | 66 (33) | 578 (32) | |
| Employed informal sector | 128 (57) | 122 (60) | 1148 (64) | |
| Unemployed/homemaker | 7 (3) | 14 (7) | 59 (4) | |
| Wealth index | <0.001 | |||
| Higher | 99 (40) | 77 (36) | 611 (32) | |
| Intermediate | 30 (12) | 37 (17) | 437 (23) | |
| Lower | 120 (48) | 98 (46) | 858 (45) | |
| Having a smartphone | 246 (99) | 207 (98) | 1861 (98) | 0.6 |
| Characteristic | Used | Only heard | Never heard | P value |
|---|---|---|---|---|
| Parity | 0.2 | |||
| Nulliparous | 145 (58) | 106 (50) | 1008 (53) | |
| Multiparous | 104 (42) | 106 (50) | 896 (47) | |
| Preference at early pregnancy | 0.004 | |||
| Caesarean section | 14 (6) | 9 (4) | 92 (5) | |
| Vaginal birth | 209 (84) | 180 (85) | 1471 (77) | |
| No preference | 26 (10) | 23 (11) | 343 (18) | |
| Having complication during pregnancy | 0.14 | |||
| Yes | 92 (37) | 75 (36) | 785 (41) | |
| No | 157 (63) | 136 (64) | 1116 (59) | |
| Referred from another hospital | <0.001 | |||
| Yes | 10 (4) | 20 (9) | 600 (31) | |
| No | 239 (96) | 192 (91) | 1307 (69) | |
| Number of antenatal care visits | <0.001 | |||
| 4 visits or more | 236 (97) | 191 (93) | 1582 (86) | |
| Less than 4 visits | 7 (3) | 14 (6.8) | 264 (14) | |
| Antenatal care visit in participating hospital | <0.001 | |||
| Yes | 184 (74) | 134 (63) | 731 (38) | |
| No | 65 (26) | 78 (37) | 1176 (62) | |
| Antenatal care visit in another private facility, outside participating hospital | 0.035 | |||
| Yes | 76 (31) | 87 (41) | 627 (33) | |
| No | 173 (69) | 125 (59) | 1280 (67) | |
| Time to get to hospital | <0.001 | |||
| Less than 30 min | 167 (67) | 122 (58) | 914 (49) | |
| 30 min or more | 82 (33) | 89 (42) | 948 (51) | |
| Referral level | 0.8 | |||
| Tertiary | 146 (59) | 123 (58) | 1142 (60) | |
| Primary–secondary | 103 (41) | 89 (42) | 765 (40) | |
| Teaching facility | 0.004 | |||
| Yes | 187 (75) | 133 (63) | 1790 (73) | |
| No | 62 (25) | 79 (37) | 517 (27) | |
| Any private practice in the maternity unit | <0.001 | |||
| Completely (private hospital) | 11 (4) | 26 (13) | 82 (4) | |
| Partially (for some providers) | 106 (43) | 94 (44) | 873 (46) | |
| No | 132 (53) | 92 (43) | 952 (50) | |
| Level of implementation of the paper-based decision aid | <0.001 | |||
| High | 229 (92) | 170 (80) | 1563 (82) | |
| Low | 20 (8) | 42 (20) | 344 (18) |
| Categorical variable outcome | Never heard | Only heard | Multivariate analysis | P value | Used | Multivariate analysis | P value |
|---|---|---|---|---|---|---|---|
| Three or more risks/benefits identified | 359 (18.8) | 44 (20.8) | 1.1 (0.7 to 1.7) | 0.578 | 61 (24.5) | 1.9 (1.3 to 2.8) | 0.001 |
| Preferred MOB told during ANC | 815 (47.4) | 111 (57.2) | 1.2 (0.8 to 1.8) | 0.365 | 169 (76.8) | 2.3 (1.5 to 3.6) | <0.001 |
| Preferred MOB told at admission | 364 (19.2) | 91 (43.1) | 1.7 (1.7 to 1.7) | <0.001 | 84 (33.7) | 1.2 (1.2 to 1.2) | <0.001 |
| Preferred MOB at late pregnancy | 1552 (84.1) | 192 (93.7) | 2.1 (0.9 to 5.2) | 0.098 | 224 (92.2) | 1 (0.4 to 2.1) | 0.915 |
| Preference for CS | 166 (9) | 16 (7.8) | 0.8 (0.4 to 1.6) | 0.6 | 16 (6.6) | 0.4 (0.2 to 0.8) | 0.006 |
| Trial of labour | 1727 (91) | 191 (90.5) | 0.8 (0.4 to 1.3) | 0.352 | 229 (92) | 1.3 (0.7 to 2.3) | 0.37 |
| Vaginal birth | 1282 (69.8) | 142 (69.6) | 1 (0.7 to 1.4) | 0.878 | 169 (69.5) | 1.4 (0.9 to 1.9) | 0.098 |
| Matched preferred and planned MOB | 1380 (75.1) | 170 (83.3) | 1.2 (0.8 to 1.8) | 0.465 | 204 (84) | 1.4 (0.9 to 2.1) | 0.118 |
| Matched preferred and actual MOB | 1174 (61.9) | 142 (67.3) | 1 (0.7 to 1.4) | 0.973 | 172 (69.1) | 1.3 (0.9 to 1.8) | 0.134 |
| PPH treatment | 99 (5.2) | 8 (3.8) | 0.7 (0.3 to 1.6) | 0.439 | 14 (5.6) | 1.1 (0.6 to 2.1) | 0.827 |
| Neonatal ICU admission | 261 (14.7) | 17 (8.5) | 0.9 (0.5 to 1.5) | 0.601 | 16 (7.1) | 0.9 (0.5 to 1.6) | 0.645 |
| Breastfeeding during stay | 1822 (96) | 205 (97.2) | 1.8 (0.7 to 4.5) | 0.21 | 236 (94.8) | 0.8 (0.4 to 1.7) | 0.614 |
- —European Union’s Horizon 2020 research and innovation programme
- —French Gorvenment - MINISTERE AFFAIRES ETRANGERES
- —IdEx Université Paris Cité
- —UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Maternal and Perinatal Health Interventions · Patient-Provider Communication in Healthcare
Introduction
Patient-centred care is widely recognised as a cornerstone of high-quality healthcare, emphasising respect for patients’ values, preferences and needs—particularly through shared decision-making1 (SDM). Research has shown that patients who actively participate in their care decisions are more likely to experience better health outcomes and greater satisfaction.2 3 In maternity care, empowering women to engage in decision-making is increasingly recognised as a fundamental component of respectful and high-quality care.4 However, many women lack adequate support and resources to make informed, value-based decisions about their childbirth options.5
Patient decision aids are evidence-based tools designed to help patients make specific and deliberated choices among healthcare options.6 They include at least information about options and outcomes and also provide guidance in the decision-making steps or explicit methods to clarify values.7 Studies from high-income countries indicate that decision aids for pregnant women around childbirth can enhance their knowledge and autonomy, reduce decisional conflict, promote physiological birth preferences and improve childbirth experiences and health outcomes.5810
However, evidence on their effectiveness remains limited in low-income and middle-income countries (LMICs),10 where processes of SDM need to be strengthened.11 Previous studies have shown that pregnant women are not sufficiently involved in decision-making, even when they have clear preferences.12 13 In the context of increasing use of caesarean sections (CSs) rates, substantial gaps exist between women’s preferences and actual delivery modes. This mismatch raises questions about women’s involvement in the decision-making processes surrounding the mode of birth (MOB). Moreover, the majority of women prefer vaginal delivery and rising CS rates in LMICs are unlikely to be mainly driven by women’s demand for CS.14
QUALIty DECision-making project
In 2020, we started the Appropriate use of CS through QUALIty DECision-making by women and providers (QUALI-DEC) project to implement an evidence-based multifaceted non-clinical intervention in four LMICs: Argentina, Burkina Faso, Thailand and Viet Nam. This intervention simultaneously targeted pregnant women and healthcare providers (HCPs) to improve decision-making on MOB and combined four components: (1) opinion leaders to improve evidence-based clinical practices; (2) audits and feedback to help HCPs identify unnecessary CS; (3) implementation of companionship during labour and childbirth to support labouring women and (4) a decision-analysis tool (DAT) to help women make an informed decision on MOB.15
The DAT
The DAT was designed for low-risk pregnant women and provides information about risks and benefits of both MOB, as well as facilitating the clarification of their personal values. The DAT was available to women either as a printed booklet or as a mobile application developed for the QUALI-DEC project; its full content and development process are described in detail elsewhere.16 Low-risk women are those who are pregnant with a single fetus and no previous CS. This tool was adapted from the decision aid ‘Birth Choices. What is best for you… Vaginal or Caesarean Birth?’17 and meets the criteria of the International Patient Decision Aid Standards.7 The DAT has two sections: the first provides evidence-based information on the risks and benefits of each MOB in an engaging, appropriate plain language for women; the second guides women to reflect on what matters most to them, thereby preparing them for meaningful discussions with HCPs. We hypothesised that the DAT would benefit low-risk women regardless of whether they preferred a vaginal birth or a CS, as it promotes meaningful dialogue with HCPs. Such conversations may help address factors influencing caesarean preferences while also supporting women who prefer vaginal birth in realising their desired mode of delivery. This study is nested within a pragmatic hybrid effectiveness-implementation type III trial, which includes an effectiveness and a process evaluation of the multi-faceted intervention in Argentina, Burkina Faso, Thailand and Viet Nam.18 The aim of this study is to evaluate the impact of the DAT on the SDM process and outcomes regarding the MOB for low-risk pregnant women.
Methods
Study design and setting
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research. The protocol for the QUALI-DEC project has been published elsewhere.15 Briefly, 32 hospitals (eight in each country) were selected for the intervention implementation, based on policymakers’ concerns and commitment to reducing unnecessary CS rates in their context. Two cross-sectional postpartum surveys were conducted in each country to assess differences between before and after the intervention. This study is an ancillary analysis of the second cross-sectional postpartum survey which was conducted from 16 October–31 October 2023 in Burkina Faso, 18 March–14 July 2024 in Thailand, 22 April–14 May 2024 in Viet Nam and 24 June–16 September 2024 in Argentina.
Participants and sample size
The detailed description of the QUALI-DEC cross-sectional survey has been published elsewhere19 (see description in online supplemental information text S1). Briefly, postpartum women were eligible for the interview if they had given birth to a live-born child beyond 22 weeks of gestation (28 weeks in Burkina Faso). Women were excluded if they had a major health problem following childbirth, according to the judgement of HCPs, gave birth to a stillborn child, experienced neonatal death, or if their newborns presented severe morbidity. Women who delivered at home or in another health facility (postnatal transfer) were also excluded. The survey included all eligible women in hospitals with fewer than ten deliveries per day, while a random sample of women was used in facilities with 10 or more deliveries per day.
The sample size estimate was not calculated specifically for this ancillary study but for the trial effectiveness evaluation. The calculation was based on the expected before-after difference in women’s birth experience and satisfaction (BES) scores, that is, 470 women per country.15 The minimum number of women to approach during recruitment was 564 women in each country (71 women per hospital), assuming a 10% non-response rate and 10% ineligible women.
Outcomes
Proxy indicators for SDM were defined according to the four objectives of a DAT, according to the Ottawa Decision Support Framework20: (1) quality of decision (three or more evidence-based risks and benefits identified of any MOB), (2) quality of decision-making process (preferred MOB told during antenatal care or at admission), (3) care behaviours (having a preferred MOB at late pregnancy, preference for CS, trial of labour, vaginal birth, matched preferred and planned MOB, matched preferred and actual MOB) and (4) health outcomes (postpartum haemorrhage treatment, neonatal intensive care unit admission, breastfeeding during hospital stay, BES score with intrapartum care) (detail outcomes description in online supplemental table S1 and S2).
Information on sociodemographic characteristics, preferred MOB, identified evidence-based risks and benefits of each MOB and BES score was collected during the postpartum period, before hospital discharge, by a trained social scientist. Clinical information on pregnancy, labour and delivery management, maternal and child health outcomes was extracted from medical records by trained clinical data collectors. Both pieces of information were collected via standardised forms.
Exposure
Participants’ exposure to the DAT was determined based on their answers to two consecutive interview questions. While asking these questions during the interview, the data collectors showed the women both versions of the tool (the printed booklet and the app on a smartphone) to help them recognise it: (1) ‘Have you heard or seen this booklet or App?’ and (2) ‘Have you ever used this tool outside of your antenatal consultation?’. The exposures were categorised into three groups: (1) ‘Used’ when a woman reported using the DAT outside of her antenatal care visit, regardless of the format; (2) ‘Only heard’ when she heard about the DAT but never used it; and (3) ‘Never heard’ when she had neither heard nor seen the DAT during pregnancy.
Two formats of the DAT were made available to women in each participating country: a booklet and a mobile application (App). The printed booklet was given to women at the discretion of HCPs during antenatal care visits or was made freely accessible in hospital waiting areas. Its content was culturally adapted for each participating country, resulting in variations in presentation: 16 pages in Argentina, 18 pages in both Burkina Faso and Thailand, and a more concise 4–6 pages in Viet Nam. The App could be accessed by scanning a QR code displayed on posters promoting the QUALI-DEC project, placed prominently in hospital lobbies. To ensure accessibility, the App was developed in six languages: Burmese, English, French, Spanish, Thai and Vietnamese, matching the linguistic needs of the participating countries. Furthermore, multimedia formats of the DAT, including videos and podcasts, were displayed on screens in antenatal clinic waiting rooms to ensure that pregnant women were aware of the DAT. The availability of these materials varied depending on the resources and infrastructure of each participating hospital. In addition, short promotional videos (reels) were disseminated through social media platforms such as Instagram, TikTok and YouTube to further expand awareness and encourage the uptake of the DAT, particularly in Argentina, Thailand and Viet Nam.
Potential confounders
Sociodemographic, pregnancy-related and organisational factors were selected based on existing literature and contextual relevance. Sociodemographic factors included country of residence, marital status, maternal age, level of education, maternal occupation, partner’s occupation, having a smartphone and household wealth index. The wealth index is a context-specific composite index, developed through variable selection and component analysis carried out in collaboration with local investigators. Pregnancy-related factors include any preference for MOB at early pregnancy; frequency and place of antenatal care visits; referral from another hospital; any complications during pregnancy including pre-labour rupture of membrane, gestational hypertension, chronic hypertension, pre-eclampsia, eclampsia, cardiac/renal disease, chronic respiratory conditions, suspected foetal growth impairment, diabetes, vaginal bleeding during second Half of pregnancy, condyloma acuminatum, confirmed HIV/AIDS, cholestasis; and other obstetric or medical conditions that could be an indication for a CS. Organisational factors include women’s accessibility to healthcare services which was estimated by the time to get to the hospital (in minutes), status of the maternity unit where the woman delivered (academic or not, reference level, totally public or private practice for all/some doctors) and the implementation score of the paper-based DAT at hospital level. This score was calculated based on two items: (a) whether the booklet was available in waiting areas, antenatal clinics, doctors’, nurses’ stations or other locations; and (b) whether the booklet was administered to eligible pregnant participants. Each item was scored as either 1 or 0 (1: yes; 0: no). The information on the implementation score was collected during regular monitoring visits and consultations with implementing partners.18
Quantitative variables
Age, parity, antenatal care attendance, hospital accessibility, wealth index and DAT implementation score at hospital level were treated as categorical variables, based on distribution and theoretical relevance (eg, age grouping as <25, 25–35, >35; parity as nulliparous versus multiparous, wealth index as higher, intermediate, lower; time to reach the hospital as less than 30 min vs 30 min and more). Healthcare facilities were categorised as having a high level of implementation if the score was higher than 75%. BES scores were treated as continuous variables.
Analysis
While the QUALI-DEC trial evaluates the strategy as a whole, the present analysis focuses specifically on exploring the associations between DAT exposure and selected outcomes. The analysis was restricted to low-risk women who were eligible for the use of DAT16: women with a singleton pregnancy and having never given birth by CS in a previous pregnancy. In this study, ‘low-risk women’ refers to those classified as having a low baseline probability of caesarean delivery early in pregnancy. Since the DAT was integrated into routine antenatal care and could be administered from the first visit, before later-pregnancy clinical information (such as foetal presentation) was available. We restricted eligibility to criteria measurable during early pregnancy. This approach ensured alignment to the population for whom reducing unnecessary primary CS is most relevant.
All variables described in the outcomes, potential confounders and quantitative variables subsections were included in our analysis to build up multilevel multivariate regression models.
Descriptive statistics were used to summarise participant characteristics and key variables. Categorical variables are presented as frequencies and percentages, while continuous variables are summarised as medians and IQRs. Women’s characteristics were initially compared between exposure groups via χ² tests and crude associations between DAT exposure and each of the 16 outcomes were tested using χ^2^ tests for categorical variables and the Kruskal-Wallis test for continuous variables.
To control for confounders, we used multivariable logistic and linear mixed-effects regression models, as appropriate. A stepwise model selection procedure based on the Akaike Information Criterion was employed to identify the most parsimonious models. To account for clustering at the facility level, a random intercept for the variable hospital (n=32) was included, capturing site-specific differences in implementation and clinical practices.
During data collection, some responses were classified as 'unknown’ when the information provided was unclear. These were later treated as missing data during analysis. No data imputation was performed. The dataset had less than 3.5% missing values, except for the partner occupation, which had 6.5% of missing values.
A sensitivity analysis was conducted to evaluate the robustness of the findings by excluding women giving birth in Burkina Faso where the number of DAT users was low (n=8).
The datasets analysed during the current study are publicly available in Zenodo.2124
All statistical analyses were performed using R software (V.4.4.2) in RStudio (V.2024.12.1+563).
Results
From a total of 5830 women who gave birth during the study period, 3545 were randomly selected and 3071 of whom provided consent (online supplemental figure S1). As per the analysis plan, we further excluded 703 women due to multiple pregnancies and prior CS. We then analysed 2368 women who were eligible for the DAT.
Exposure and women’s acceptability
Among them, 1907 (80%) women had never heard of the DAT, 212 (9%) had heard of the DAT but never used it, and 249 (11%) women had used the DAT outside antenatal care visits. Among the 461 women who either used or only heard about the DAT, 370 (80%) reported receiving it from their HCPs. Among all 461 women, 94 (20%) received the DAT in the first trimester, 79 (17%) in the second trimester and 202 (44%) in the third trimester of pregnancy. The remaining 86 women (19%) included 12 who were unsure of the timing and 74 who reported awareness of the DAT but did not receive a personal introduction to the tool. Among the 249 women who reported using the DAT, 209 (84%) used the paper-based format, while 13 (5%) used the App, and 28 (11%) used both formats. Among users, 122 (49%) used the DAT once, 69 (28%) used it twice, and 58 (23%) used it three times or more, and 72 (29%) reported writing their motivation into the tool. A total of 245 (98%) users found the DAT easy to use, 228 (92%) users agreed that the DAT facilitated communication with HCPs, and 233 (94%) users agreed that it helped them clarify their birth preference. A total of 242 (97%) users agreed or strongly agreed that they would recommend the DAT to other pregnant women.
Participant characteristics
The distribution of sociodemographic characteristics varied across the three exposure groups (table 1). Women aged ≥35 years were more likely to be DAT users, whereas women aged 25–34 years were more represented in the Only-heard group. While most women lived in urban areas, rural women were proportionally more represented among those who had only heard about the DAT. Women with secondary education were the majority across groups, but the proportion of women with tertiary education was highest among DAT users, suggesting a gradient favouring DAT use with increasing education. Regarding socioeconomic status, both women in the lowest and highest wealth index categories seem more likely to use the DAT, while those in the middle category were less likely to do so. Most pregnancy-related and organisational factors were also associated with exposure (table 2), particularly attending ANC in participating hospitals and giving birth in facilities with higher levels of DAT implementation.
Outcomes
Adjusted associations are presented numerically in table 3 and graphically in figures12 for binary and continuous outcomes, respectively. Bivariate analysis results are provided in online supplemental table S3.
Associations between exposure and binary variable outcomes: adjusted ORs using logistic mixed models. ANC, antenatal care; DAT, decision analysis tool; ICU, intensive care unit; MOB, mode of birth.
Associations between exposure and continuous variable outcomes: adjusted coefficients of linear mixed models. BES, birth experience and satisfaction; DAT, decision analysis tool.
Compared with women who had never heard about the DAT, those who used the tool were significantly more likely to identify three or more evidence-based risks and benefits for each MOB (adjusted OR, aOR 1.9; 95% CI 1.3 to 2.8; p=0.001), to express their preferred MOB during antenatal care (aOR 2.3; 95% CI 1.5 to 3.6; p<0.001) and at admission (aOR 1.2; 95% CI 1.2 to 1.2; p<0.001). DAT use was also associated with lower odds of preferring a CS in late pregnancy (aOR 0.4; 95% CI 0.2 to 0.8; p=0.006).
Regarding birth experience, adjusted linear regression models showed that overall BES scores were significantly higher among DAT users compared with the Never-heard group (β=1.9; 95% CI 0.5 to 3.3; p=0.006). The largest improvement was observed in the communication dimension (β=2.7; 95% CI 0.8 to 4.5; p=0.004).
Multilevel modelling showed that overall satisfaction scores were significantly influenced by the hospital where women gave birth, with intraclass correlation coefficients equal to 0.32. The between-hospital variance was 35.96% for BES scores indicating substantial facility-level effects on women’s experiences and perceptions of care. Full adjusted multivariate models are provided in online supplemental figure S2–S17.
Excluding women from Burkina Faso did not change the overall trends observed across outcome dimensions.
Discussion
This multicountry, cross-sectional study revealed that among low-risk pregnant women, the use of the DAT was significantly associated with greater awareness of the risks and benefits of each MOB, with increased discussion with HCPs about women’s preference, a greater preference for vaginal birth, a more positive birth experience and greater satisfaction with care. The findings are consistent with what women said about the DAT. Most of them agreed that it was easy to use and said that it helped them talk to HCPs and clarify their birth preference. However, no significant differences were observed in other outcomes such as trial of labour, actual MOB or maternal and newborn health, among the exposure groups. Significant behavioural changes would have been needed from HCPs, in response to women’s use of the DAT, to have resulted in changes to birth outcomes. In contexts where caesareans occur without clear medical indication, ensuring that women can articulate their preferences, particularly their preference for vaginal birth, supports better alignment with respected maternal care.19 25 26 Facilitating informed discussions is consistent with women-centred care and does not conflict with clinicians’ responsibility to recommend vaginal birth when medically safest.27 In line with expert recommendations to reduce unnecessary CSs,28 29 our findings reinforce the need for multidimensional strategies that address both clinical and psychosocial determinants of MOB. Evidence from a recent scoping review indicates that women’s requests for planned caesarean without clinical indication are primarily motivated by fear of labour and a desire for control over the birth experience.30 Similar patterns emerged in our study settings, where women reported fear of labour pain, often exacerbated by limited access to epidural analgesia, and a wish to schedule the birth at an auspicious time.19 31 However, preferences for CS accounted for only a small proportion of caesarean births,14 suggesting that addressing women’s requests alone is insufficient. While it was not feasible within the QUALI-DEC trial to co-design additional interventions targeting women’s fear and difficult access to epidural, the DAT may help providers identify the reason for CS preference, explore fears and offer reassurance or mitigation strategies, as recommended by WHO guidance on respectful maternity care.9 The QUALI-DEC theory of change shows that birth outcomes and impact on CS use are linked to the implementation of all four components of the intervention.18 A scoping review of the effects of decision aids around childbirth supported the idea that these tools combined with other interventions seem to be important factors in improving care behaviour and health outcomes.10 The results of the QUALI-DEC trial’s process and effectiveness evaluation will reveal whether the multifaceted intervention produced the intended long-term outcomes. Importantly, our findings show that the use of the DAT was not associated with any harm to maternal or neonatal outcomes, which is consistent with evidence from studies conducted in high-income countries.10
Our study has several strengths. This study is the first to evaluate the impact of the DAT on the decision-making process for choosing the MOB for low-risk pregnant women in LMICs. Second, we address all four main objectives of the decision aids to perform a comprehensive evaluation of SDM regarding MOB in this context. While the study was observational and hospital-based, we controlled for confounding biases and cluster effect using appropriate statistical methods.
However, several limitations should be considered when interpreting these findings. First, the cross-sectional design limits causal inference. However, by adjusting for potential confounders, the analysis provides a more accurate estimate of the associations observed. Second, the number of women who used the DAT was relatively small compared with those who did not hear about it, limiting the subgroup analysis per country. Third, the level of DAT implementation varied across facilities. This could have diluted the observed associations, especially for care behaviour-related outcomes that require strong provider involvement. Fourth, women with major maternal health complications or perinatal death were excluded from the survey, preventing us from assessing the association of the DAT with severe morbidity. Fifth, other relevant outcomes such as women’s values about MOB, decisional conflict, decisional satisfaction and decisional regret were not measured. Sixth, the DAT was only available in formats that required women to read, which may have limited accessibility for women with low literacy. Seventh, the question of whether women told their care provider their preferred MOB reflects one-way communication of preference and does not necessarily capture whether a two-way discussion or SDM occurred. Finally, as data on women’s knowledge and preferences were collected after childbirth, recall and social desirability biases cannot be ruled out.
To maximise decision aid impacts for pregnant women, decision aids should be made available in multiple formats to accommodate different literacy levels, and efforts should be made to ensure a wide outreach. Future research should focus on why women do not use the DAT. Ideally, support from policymakers should be provided to ensure sustainability and broader uptake. When used effectively (not only heard about it), the DAT can help women prepare for SDM with their HCPs. At the same time, providers must have an honest and unbiased discussion with them and create space for women to express their values and preferences. This joint effort is essential to ensure that women in LMICs receive the care that is aligned with their preferences.
Conclusions
Among low-risk pregnant women in Argentina, Burkina Faso, Thailand and Viet Nam, the use of the DAT was associated with significant differences in knowledge, value-based communication with HCPs, greater preference for vaginal birth and improved childbirth experience and satisfaction. These findings suggest that the DAT may have helped foster more respectful and women-centred care. Future research will assess the effects of the combination of the DAT with other interventions targeting HCPs on medical practice and perinatal outcomes.
Supplementary material
10.1136/bmjgh-2025-022365online supplemental file 1
10.1136/bmjgh-2025-022365online supplemental appendix 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barry MJ Edgman-Levitan S Shared Decision Making — The Pinnacle of Patient-Centered Care N Engl J Med 2012366780110.1056/NEJ Mp 110928322375967 · doi ↗ · pubmed ↗
- 2Hibbard JH Greene J What The Evidence Shows About Patient Activation: Better Health Outcomes And Care Experiences; Fewer Data On Costs Health Aff (Millwood)2013322071410.1377/hlthaff.2012.106123381511 · doi ↗ · pubmed ↗
- 3Kiesler DJ Auerbach SM Optimal matches of patient preferences for information, decision-making and interpersonal behavior: evidence, models and interventions Patient Educ Couns 2006613194110.1016/j.pec.2005.08.00216368220 · doi ↗ · pubmed ↗
- 4Shakibazadeh E Namadian M Bohren M et al Respectful care during childbirth in health facilities globally: a qualitative evidence synthesis BJOG 20181259324210.1111/1471-0528.1501529117644 PMC 6033006 · doi ↗ · pubmed ↗
- 5Kloester J Willey S Hall H et al Midwives’ experiences of facilitating informed decision-making – a narrative literature review Midwifery 202210910332210.1016/j.midw.2022.10332235358936 · doi ↗ · pubmed ↗
- 6Stacey D LégaréF Lewis K et al Decision aids for people facing health treatment or screening decisions Cochrane Database Syst Rev 20174 CD 00143110.1002/14651858.CD 001431.pub 528402085 PMC 6478132 · doi ↗ · pubmed ↗
- 7International patient decision aids standards (ipdas) collaboration [internet]2023 Availablehttp://www.ipdas.ohri.ca/using.html
- 8López-Toribio M Bravo P LlupiàA Exploring women’s experiences of participation in shared decision-making during childbirth: a qualitative study at a reference hospital in Spain BMC Pregnancy Childbirth 20212163110.1186/s 12884-021-04070-334535117 PMC 8447503 · doi ↗ · pubmed ↗