Osteoporosis: a missed link in fall prevention - a retrospective cohort study
Nadja Fries, Agathi Constantinou, Therése Wretborn, Anna Spångeus

TL;DR
This study finds that many elderly patients who fall in hospitals are not treated for osteoporosis, leading to fractures.
Contribution
The study highlights the underutilization of anti-osteoporotic treatment in high-risk fallers and its link to fracture incidence.
Findings
9% of patients who fell sustained fractures, mostly hip and vertebral.
None of the fracture patients were on anti-osteoporotic treatment.
High fall risk and prior fractures did not correlate with treatment initiation.
Abstract
Falls and osteoporotic fractures are common in the geriatric population. Although falls increase the risk of osteoporotic fractures, many patients with recurrent falls are untreated for osteoporosis. In our study, we aimed to; (1) assess the incidence of fractures among patients who experience falls during inpatient care in a geriatric ward; (2) investigate the risk factors associated with fractures in this cohort; and (3) investigate whether patients on anti-osteoporotic treatment differed from and had better fall-related clinical outcomes compared to those without anti-osteoporotic treatment. This study involved a retrospective cohort analysis of inpatient falls in the Geriatric ward between 2018 and 2020. Patients who experienced a fall during this period were identified through the hospital’s adverse event tracking system. Demographic and clinical data, fall-related information,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
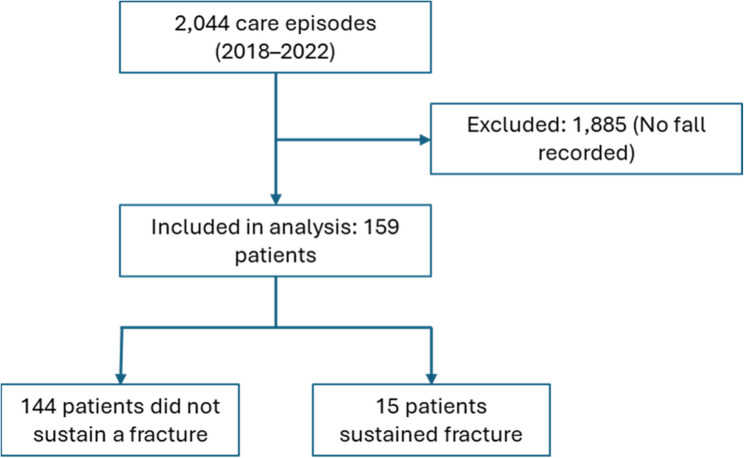 Figure 1
Figure 1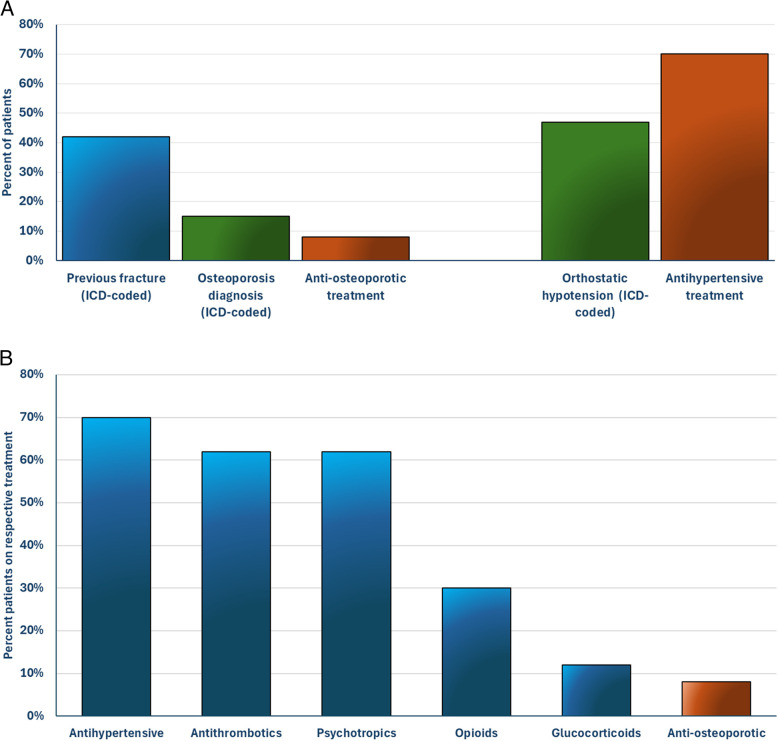 Figure 2
Figure 2 Figure 3
Figure 3- —Linköping University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Bone health and osteoporosis research · Hip and Femur Fractures
Why does this paper matter?
This study highlights a critical gap in osteoporosis management among high-risk geriatric inpatients, emphasizing the need for improved treatment strategies to prevent fall-related fractures and enhance patient outcomes.
Background
Osteoporosis is a common skeletal disease characterized by reduced bone mass and deterioration of bone microarchitecture, resulting in diminished bone strength and an increased risk of fragility fractures. This condition is particularly common in the aging population, as bone mineral density (BMD) declines with age [1]. With rising life expectancy, the prevalence of fragility fractures is expected to rise [2]. These fractures are associated with substantial morbidity, including persistent disability and impaired quality of life, as well as considerable health care costs (such as hospitalization), and increased mortality rates [3–6]. Importantly, the risk of sustaining a subsequent fracture is significantly higher in the years following an initial fracture [7] underscoring the importance of preventive strategies.
Falls are frequent among older hospitalized individuals and represent a major risk factor for fracture [6, 8]. Multiple comorbidities, polypharmacy and the use of certain medications, such as sedatives and antihypertensives, further increase fall risk in older adults [9]. However, the clinical need for these treatments often escalates with age, highlighting the necessity of individualized, carefully balanced risk–benefit assessments.
To mitigate hospital falls, multifactorial interventions are recommended, including patient and staff education, systematic use of fall-risk assessment tools, regular medication reviews, tailored physical exercise programs, and environmental modification [9–11].
Despite the strong link between falls and fractures, and the availability of well-documented and effective fracture prevention treatments [12–15], only a minority of patients with osteoporosis are identified and treated [2, 16]. Therefore, integrating osteoporosis assessment into fall and fall-injury prevention strategies is essential [9]. Many clinical guidelines emphasize fall prevention rather than fall-injury prevention, the latter encompassing measures to enhance endogenous resistance to fall injuries such as optimizing skeletal health, despite a clear treatment gap among high-risk fallers.
In the present study, we aimed to; (1) assess the incidence of fractures among patients who experience falls during inpatient care in a geriatric ward; (2) investigate the risk factors associated with fractures in this cohort; and (3) investigate whether patients on anti-osteoporotic treatment differed from and had better fall-related clinical outcomes compared to those without anti-osteoporotic treatment.
Methods
Study cohort and variables
In this retrospective study, patients who experienced a fall during inpatient care in the geriatric ward at Linköping University Hospital in Sweden over a three-year period (January 1, 2018, to December 31, 2020) were included. Information regarding the falls, associated risk factors, and outcomes was extracted from the hospital’s electronic medical records. Fall incidents were identified by the hospital’s adverse event tracking system (Synergi) and were defined in accordance with the definition outlined by the World Health Organization as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level [17]. Exclusion criteria included fall incidents secondary to clinical events (e.g., stroke, seizure, arrhythmia). A fall was considered severe if it resulted in a fracture, the need for opioid prescription, major head injury, internal bleeding, or death.
Different risk assessments were routinely evaluated for all patients upon admission to the ward and were documented in the medical records. These included Elderly Mobility Scale (M-EMS), Downton Fall Risk Index (DFRI), nutrition status (Short Form Mini Nutritional Assessment, SF-MNA), and risk of developing pressure sore (Risk Assessment Pressure Sore, RAPS) [18–21].
Current medications were reviewed from the medical records and defined as those prescribed (i.e. listed on medication chart) to patients within 24 h prior the fall, except for Zoledronic acid, which was included if administered up to one year prior to the fall and denosumab if administered up to 6 months prior to the fall. For analysis purposes medications were divided into sub-groups i.e.; (1) psychotropics including sedatives-hypnotics and antipsychotic medications; (2) antihypertensives including diuretics, beta-blockers, renin-angiotensin system (RAS) agents, alpha-1 antagonists, and calcium channel blockers; and (3) antithrombotics, including anticoagulants and platelet inhibitors. In addition, a variable containing the number of medications classified as fall risk increasing drugs (FRIDs) was included [22].
Previous fractures were identified in two ways; (1) if ICD-coded (International Statistical Classification of Diseases and Related Health Problems) in the medical record; or (2) if ICD-coded and/or identified having a previously undiagnosed vertebral fractures in opportunistic screening from CT scans performed in near time from fall (data from a sub-study [23]). ICD codes were available in the medical records from 2008.
Statistical analysis
Continuous variables were presented as mean and standard deviation (SD) or median and 25–75 percentile, depending on their normality. Categorical variables were expressed as frequencies. Group comparisons for continuous data were performed using either the T-test or the Mann-Whitney U test, based on normality, while the Chi-square test was used for categorical data. Data analysis was conducted using IBM SPSS (version 29.0.2.0, IBM Corp., Armonk, NY, USA). A p-value of < 0.05 was considered statistically significant.
Ethics
The study protocol was reviewed and approved by the Swedish Ethical Review Authority (2021 − 01425, with an amendment 2022-02053-02). Informed consent was not required for this retrospective cohort study design.
Results
Study population and incidence of fractures
Descriptive statistics are summarized in Table 1. Throughout the 3-year study period, the care unit had 2,044 care episodes. A total of 159 patients (mean age 84 years, 45% females) experienced a documented fall incident during their inpatient stay, thus falls occurred in 8% of all care episodes at the ward. Of the 159 patients with a fall, 23 falls were classified as severe and included 15 patients who sustained fractures (Fig. 1). The most common type of fracture was hip fractures (n = 5) followed by vertebral fractures (n = 4). Other types of fractures included rib, clavicle, facial, and humerus fractures. Among the 159 patients, 42% had a history of at least one ICD-coded fracture (Fig. 2a). When including non-ICD-coded vertebral fractures identified through opportunistic CT screening, the percentage increased to 52%. Despite the high prevalence of previous fractures in this cohort, only a small proportion of patients (15%) were diagnosed with osteoporosis.
Table 1. Demographic and clinical characteristics of patientsVariableAll (n = 159)MissingDemographicsAge84 ± 70Sex, female45%0BMI24 [21–27]12Assessment ScoreDFRI5 [4–6]24DFRI ≥ 397%M-EMS10 [6–14]10SF-MNA8 [6–10]25SF-MNA ≤ 1193%RAPS30 [28–32]26RAPS < 2931%Previous fall (≥ 1) last year84%1MedicationTotal number of medications9 ± 40Total number of FRID-classified medication3 [2–5]0Any FRID-classified medication91%0Medical History*Osteoporosis15%0Previous fracture42%0Orthostatic hypotension47%0Cognitive disease34%0Parkinson disease14%0Fall incidentFall-related fracture9%0Severe fall15%0Length of stay16 [10–27]030-day mortality16%0One year mortality45%0Values presented as mean ± SD, median [25 - 75 percentile] or percent. *ICD-coded. BMI Body Mass Index, FRID Fall-Risk Increasing Drugs, DFRI Downton Fall Risk Index, M-EMS Modified Elderly Mobility Scale, SF-MNA Short form Mini Nutrition Assessment, RAPS Risk Assessment Pressure Sore scale
Fig. 1. Flow chart describing the study cohort
Nearly all participants were considered as high risk of falling according to the DFRI, with moderate mobility limitations, averaging 10 points on the M-EMS. This aligns with the fact that 84% of participants were recurrent fallers (≥ 1 fall in the past year). As a result of high DFRI scores, fall prevention measures were implemented and documented in the medical records in 69% of patients during their inpatient care. Orthostatic blood pressure was evaluated in 73 participants during their inpatient stay, with 64% showing a pathological reaction (orthostatic hypotension). Additionally, 47% of all patients had ICD-coded orthostatic hypotension prior to admission (Fig. 2a).
As shown in Fig. 2b, over half of the participants were receiving antihypertensives, antithrombotics, and/or psychotropics (70%, 62%, and 62%, respectively). Nearly one-third of the participants were receiving opioids (30%), and 12% glucocorticoids. In contrast, only 8% were receiving anti-osteoporotic treatment. On average, patients were prescribed 9 medications and a total of 91% of the patients were prescribed at least one FRID-classified medication.
Fig. 2(a) The proportion of patients diagnosed with prior fractures, osteoporosis, and/or orthostatic hypotension, compared to the proportion of patients receiving anti-osteoporotic and/or antihypertensive treatment. (b) Patients on respective treatment prior to the fall. Antihypertensives: diuretics, beta-blockers, renin-angiotensin system (RAS) agents, alpha-1 antagonists, or calcium channel blockers; Antithrombotics: anticoagulants and platelet inhibitors; Psychotropics: sedatives-hypnotics and antipsychotic medications
Fracture vs. no fracture related to the fall
Risk factors for patients who sustained a fracture compared to those who did not are summarized in Table 2. Most fractures occurred in males, i.e. 11 males compared to 4 females. No significant age difference was observed between patients with or without fractures. There was a trend towards lower BMI in patients who sustained a fracture during the fall (BMI 22 [21–24] vs. 24 [20–27] kg/m², p = 0.177). Significantly fewer patients with a high BMI (≥ 25 kg/m²) sustained a fracture after the fall falls (2%) than patients with normal weight (15%, p = 0.015). No statistically significant difference was seen between patients with underweight (< 18.5 kg/m²) and normal weight (6% vs. 15%, p = 0.453).
The prevalence of previous fractures was high in both groups (42–47%). Despite this, only a minority of the patients had an osteoporosis diagnosis (7–15%). Though non-significant, the diagnosis of osteoporosis was twice as common in the non-fracture group compared to the fracture group (15% vs. 7%). Similarly, 8% of the patients in the non-fracture group were prescribed anti-osteoporotic treatment prior to the fall, in comparison to none of the patients in the fracture group. Conversely, glucocorticoid treatment was nearly twice as common in the fracture group compared to the non-fracture group (20% vs. 11%). The length of hospitalization was longer, though statistically non-significant, in the fracture-group compared to the non-fracture group (median 19 days and 16 days respectively). No statistical difference was observed between the groups regarding risk scores or fall preventive measures.
Table 2. Comparison between the fracture vs. non-fracture patient groups related to the fallVariableFracture (n = 15)No fracture (n = 144)p-valueDemographicsAge86 ± 684 ± 70.479Sex, female27%47%0.141BMI (kg/m^2^)22 [21–24]24 [20–27]0.177Assessment ScoreDFRI5 [4–6]5 [4–6]0.531DFRI ≥ 3100%98%0.524M-EMS9 [6–14]10 [6–14]0.907SF-MNA7 [4–8]8 [6–10]0.128SF-MNA ≤ 11100%92%0.326RAPS29 [25–31]31 [28–32]0.181RAPS < 2936%30%0.678Previous fall (≥ 1) last year93%83%0.307MedicationOpioids27%30%0.796Psychotropics60%62%0.891Antithrombotics87%60%0.040Antihypertensives73%69%0.755Glucocorticoids20%11%0.312Anti-osteoporotic0%8%0.245FRID-classified medication100%90%0.189Total number of FRID-classified medication3 [2–5]3 [2–5]0.510Total number of medications9 ± 39 ± 40.841Medical History*Osteoporosis7%15%0.367Previous fracture47%42%0.709Orthostatic hypotension33%48%0.281Cognitive disease47%33%0.275Parkinson disease27%13%0.133Fall incidentLength of stay19 [12–26]16 [10–27]0.70430-day mortality20%15%0.633One year mortality40%46%0.666Values presented as mean ± SD, median [25 - 75 percentile] or percent. *ICD-coded. BMI Body Mass Index, FRID Fall-Risk Increasing Drugs, DFRI Downton Fall Risk Index, M-EMS Modified Elderly Mobility Scale, SF-MNA Short form Mini Nutrition Assessment, *RAPS *Risk Assessment Pressure Sore scale
Anti-osteoporotic treatment vs. no anti-osteoporotic treatment
A summary of patients with anti-osteoporotic treatment vs. no anti-osteoporotic treatment is shown in Table 3. Overall, the proportion of patients receiving treatment for osteoporosis was low, i.e. 8%. There was no significant difference regarding age and sex between patients treated or not treated with anti-osteoporotic drugs.
Patients with ongoing anti-osteoporotic treatment were more frequently diagnosed with osteoporosis and had a higher total number of medications prescribed. Furthermore, the patients with anti-osteoporotic treatment showed a trend (p = 0.074) towards having experienced a previous fracture more frequently.
Table 3. Comparison of patients with anti-osteoporotic treatment vs. no anti-osteoporotic treatmentVariableAnti-osteoporotic treatment (n = 12)No anti-osteoporotic treatment (n = 147)p-valueDemographicsAge86 ± 684 ± 70.430Sex, female58%42%0.322BMI (kg/m^2^)24 [20–27]24 [21–27]0.914Assessment ScoreDFRI5 [3–7]5 [4–6]0.442DFRI ≥ 3100%97%0.586M-EMS7 [6–10]10 [6–14]0.384SF-MNA8 [4–10]8 [6–10]0.792SF-MNA ≤ 11100%92%0.351RAPS31 [25–32]30 [28–32]0.770RAPS < 2933%31%0.866Previous fall (≥ 1) last year91%84%0.526MedicationOpioids17%31%0.309Psychotropics67%61%0.709Antithrombotics83%61%0.117Antihypertensives83%69%0.289Glucocorticoid25%11%0.147FRID-classified medication100%90%0.245Total number of FRID-classified medication5 [4–6]3 [2–4]0.009Total number of medications13 ± 29 ± 4< 0.001Medical History*Osteoporosis83%9%< 0.001Previous fracture67%40%0.074Orthostatic hypotension58%46%0.394Cognitive disease42%33%0.558Parkinson disease25%13%0.220Fall incidentLength of stay21 [11–27]16 [10–27]0.39630-day mortality8%16%0.465One year mortality67%44%0.122Values presented as mean ± SD, median [25 - 75 percentile] or percent. *ICD-coded. BMI Body Mass Index, FRID Fall-Risk Increasing Drugs, DFRI Downton Fall Risk Index, M-EMS Modified Elderly Mobility Scale, SF-MNA Short form Mini Nutrition Assessment, *RAPS *Risk Assessment Pressure Sore scale
Discussion
In the present study we show that the incidence of fractures was high during geriatric inpatient care with nearly one in ten patients that had a documented fall during their hospital stay sustaining a fracture related to the fall. Most of these were hip or vertebral fractures. Only 8% of the patients had ongoing anti-osteoporotic treatment; despite half of the patients having had a previous fragility fracture, nearly all (97%) being considered as high-risk for fall (DFRI assessed), and 84% being recurrent fallers (≥ 1 fall recent year). None of the patients that fractured during the fall on the ward were on anti-osteoporotic treatment prior to the fall.
Fractures related to fall incidents during hospital care have previously been reported from other inpatient settings such as in Australia (3.8%) and Brazil (< 2.1%) [24, 25]. The latter study also included younger patients (average age 65 years) but concluded that fractures were more common after falls in the oldest patients, thus in the age group most similar to our study. If a patient had fallen multiple times our study included the most severe fall, this may thereby partly explain our higher frequency of fractures. Another factor that may explain the higher fracture incidence in our study is a higher mean age in our cohort. Furthermore, the definition of fall incidence differs between studies. Thus, in our study, a fall-incidence was strictly defined as incidents where patients actually fell to ground level or a lower level. In contrast, other studies also included fall incidents where the actual fall was prevented by healthcare professionals assisting the patient to an armchair or the floor [25].
The patients in our study exhibited several strong risk factors for osteoporosis, including advanced age (mean 84 years), high prevalence of previous fractures, glucocorticoid treatment, recurrent falls, high fall risk, and risk of malnutrition. Despite these risk factors, only a minority of patients, i.e. 15%, were diagnosed with osteoporosis, and even fewer (8%) received anti-osteoporotic treatment. These findings indicate that osteoporosis remains significantly underdiagnosed and undertreated in this patient population, underscoring the need to prioritize osteoporosis assessment and management alongside fall prevention strategies in geriatric care. In our cohort, 8% of patients in the non-fracture group had received anti-osteoporotic treatment prior to the fall, whereas none (0%) in the fracture group had been treated. Although this difference appears clinically relevant, it did not reach statistical significance, most likely due to insufficient statistical power. Based on our calculations, approximately twice the number of observations would have been required to detect such a difference with adequate power.
As previously mentioned, it is, however, important to value each patients’ current risk versus benefit when prescribing additional medications, particularly in this fragile patient group. On the other hand, other medical treatments, including FRID medications, were frequently prescribed, i.e. 91% of patients had at least one, and the mean number of medications was considerable. i.e. mean number 9, indicating that this patient group was considered to benefit from active treatments. Thus, it seems unlikely that the non-treatment for osteoporosis was an active decision.
A cohort study conducted in Canada examined anti-osteoporotic treatment in patients (≥ 65 years) who previously sustained a hip fracture [26]. Similarly to our findings, only 38 of 449 patients (8%) were receiving anti-osteoporotic treatment prior to fracture and 23% were receiving it post-fracture. Mortality post-fracture was significantly lower in the group receiving anti-osteoporotic treatment. In general, osteoporosis treatment rates remain low after fractures, despite clear guidelines and efforts to develop fracture liaison services (FLS) [2]. While a history of previous fracture was similarly high in both the fracture and non-fracture group in our study, osteoporosis diagnoses (M80.x and M81.x) were twice as common in the non-fracture group. Additionally, glucocorticoid use, a well-known risk factor for osteoporosis [27], was nearly twice as common in the fracture group. These findings might suggest a higher degree of underdiagnosis and undertreatment in the fracture group.
Although the overall treatment rate with anti-osteoporotic medications in our study was low, both a prior diagnosis of osteoporosis and a history of previous fragility fractures were associated with a higher likelihood of receiving treatment. The proportion of treated patients was lower than national data on secondary fracture prevention, including younger patients as well (12%) [28]. This is despite previous studies indicating comparable efficacy of anti-osteoporotic treatments in ageing patients as in the younger [29]. In a study by Ek et al., the rate of secondary fracture prevention with anti-osteoporotic therapy was two to three times lower in patients aged 90 years and above compared to those aged 70–89 years [16].
Regarding previous fractures, 42% of the patients had sustained one or more previous fractures, according to ICD coding. In the present fall cohort, radiological examinations of available CT scans were performed in another sub-study, revealing a considerable number of undiagnosed vertebral fractures (i.e. an additional 10% points in the previous fracture sub-group) [23]. The underdiagnosing of vertebral fractures is well known and today less than one-third are diagnosed [30–32]. Including these non-ICD-coded fractures, a total of 52% of patients in our cohort were found to have had a previous fracture. This suggests that fractures in the geriatric population are very common and that vertebral fractures are often missed or overlooked. Given that previous fractures and specifically vertebral fractures, are strong risk factors for osteoporosis and future osteoporotic fractures, it is crucial to improve the diagnosis and treatment rates after these fractures [33].
In our cohort, fall risk and mobility assessments were typically conducted prior to the fall. The results of these assessments correlated well with the clinical outcomes, as 97% of all the patients who fell at our ward were classified as at risk of falling (DFRI ≥ 3). Nevertheless, DFRI was not associated with the severity of the fall, including fractures which seems logical as DFRI aims to identify individuals at high risk of fall, not the outcome of the fall (severity). As a result of the generally high-risk scores of falls in our cohort, a total of 69% of the patients had documented fall-preventive measures in place prior to their fall. However, despite preventive efforts, many of these vulnerable patients continue to fall, as in our cohort, and thus are at risk of sustaining severe injuries, such as fractures or hemorrhages. Therefore, it seems prudent to complement fall prevention measures with strategies to enhance internal resistance to injuries from falls. One approach is to focus on anti-osteoporotic treatment to fortify patients who are likely to fall again despite fall preventive interventions. This is highlighted in several fall-prevention guidelines, but can still be missed in the clinical setting [11].
Our study has several limitations. Firstly, the sample size is relatively small (n = 159), which diminishes the statistical power and increases the risk of clinically significant differences being statistically non-significant. Additionally, the retrospective observational study design may introduce research biases, such as inaccuracies in the documentation of falls and their consequences, as well as in the assessment of risk scores. Furthermore, the study was conducted in a single ward, which may limit the generalizability of the findings. However, our study also has notable strengths. The access to a unified electronic medical record system allowed for the identification of ICD-codes and prescriptions registered across all the hospitals and primary health care centers, thereby enhancing the comprehensiveness of the data. Furthermore, there were well-implemented routines for fall risk assessment, ensuring that assessments were systematically conducted in most patients by experienced personnel.
In conclusion, although risk assessments and interventions are conducted to prevent injurious falls, a significant proportion of patients continue to experience falls. Despite being classified as high-risk fallers and having a history of recent fractures, only a minority of risk-patients received anti-osteoporotic treatment. This shortfall could potentially contribute to the high incidence of fractures resulting from falls observed in this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Willers C, Norton N, Harvey NC, et al. Osteoporosis in europe: a compendium of country-specific reports. Arch Osteoporos. 2022;17(1). 10.1007/s 11657-021-00969-8.10.1007/s 11657-021-00969-8PMC 878973635079919 · doi ↗ · pubmed ↗
- 2Kanis JA, Norton N, Harvey NC, et al. SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos. 2021;16(1). 10.1007/s 11657-020-00871-9.10.1007/s 11657-020-00871-9PMC 817240834080059 · doi ↗ · pubmed ↗
- 3Veronese N, Kolk H, Maggi S. Epidemiology of fragility fractures and social impact. In: Falaschi P, Marsh D, editors. Orthogeriatrics. Practical issues in geriatrics. Springer; 2021. 10.1007/978-3-030-48126-1_1.33347224 · pubmed ↗
- 4Coussement J, Paepe L, De, Schwendimann R, Denhaerynck K, Dejaeger E, Milisen K. Interventions for preventing falls in Acute- and Chronic-Care. Published Online 2008:29–36. 10.1111/j.1532-5415.2007.01508.x 10.1111/j.1532-5415.2007.01508.x 18031484 · doi ↗ · pubmed ↗
- 5van der Velde N, Seppala LJ, Herrero AC et al. Falls prevention in community-dwelling older adults and implementation of world falls guidelines: a call for action across Europe by the European Geriatric Medicine Society Special Interest Group on Falls and Fractures. Eur Geriatr Med. Published online June 12, 2025. 10.1007/s 41999-025-01206-y 10.1007/s 41999-025-01206-y PMC 1237877340506658 · doi ↗ · pubmed ↗
- 6Montero-odasso MM, Kamkar N, Pieruccini-faria F, Osman A, Sarquis-adamson Y. Evaluation of clinical practice guidelines on fall prevention and management for older adults A systematic review. 2021;4(12):1–15. 10.1001/jamanetworkopen.2021.3891110.1001/jamanetworkopen.2021.38911 PMC 867474734910151 · doi ↗ · pubmed ↗
- 7Black DM, Delmas PD, Eastell R et al. Once-Yearly Zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007;35618.10.1056/NEJ Moa 06731217476007 · doi ↗ · pubmed ↗
- 8Ek S, Meyer AC, Sääf M, Hedström M, Modig K. Secondary fracture prevention with osteoporosis medication after a fragility fracture in Sweden remains low despite new guidelines. Arch Osteoporos. 2023;18(1). 10.1007/s 11657-023-01312-z.10.1007/s 11657-023-01312-z PMC 1038695737516714 · doi ↗ · pubmed ↗