Therapeutic and Diagnostic Landscape of Diabetic Neuropathy: A Systematic Review of Clinical Studies
Jay Prakash S Rajput, Rahul Deb, Sajidali S Saiyad, Zayan Jamal, Santosh Kumar Sah, Alkeshkumar R Vara, Nadia Sandhu, Dimpal Rochlani, Tanzila A Saiyed, Arin A Pathan, Ashok Sagar, Tejal Virola

TL;DR
This review summarizes recent clinical studies on diagnosing and treating diabetic neuropathy, highlighting effective strategies and areas needing more research.
Contribution
The paper provides a comprehensive synthesis of recent clinical evidence on DN therapies and diagnostics from 2020 to 2025.
Findings
Pregabalin, duloxetine, and α-lipoic acid showed consistent efficacy in reducing pain and improving nerve function.
High-frequency spinal cord stimulation and structured rehabilitation improved outcomes in refractory and mobility-related cases.
Biomarker-based and microvascular measures are emerging as useful diagnostic adjuncts alongside nerve conduction studies.
Abstract
Diabetic neuropathy (DN) is one of the most prevalent complications of diabetes mellitus, affecting up to half of patients and contributing to disability, poor quality of life, and the risk of foot ulceration. Despite extensive research, its heterogeneous manifestations and complex pathophysiology continue to challenge timely diagnosis and effective treatment. This systematic review aimed to synthesize recent clinical evidence on diagnostic and therapeutic strategies for DN. A comprehensive search of PubMed, EMBASE, CENTRAL, and Web of Science identified 76 eligible clinical studies published between 2020 and 2025, including randomized controlled trials, observational studies, and case reports. Data extraction and risk-of-bias assessment were performed according to PRISMA guidelines. Pharmacological agents, particularly pregabalin, duloxetine, and α-lipoic acid, demonstrated the most…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
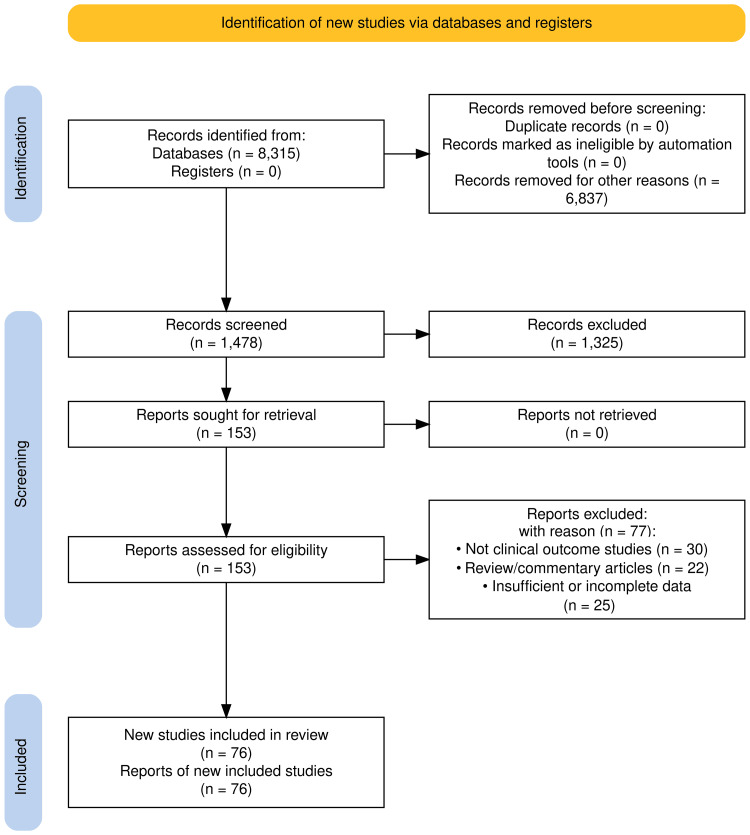 Figure 1
Figure 1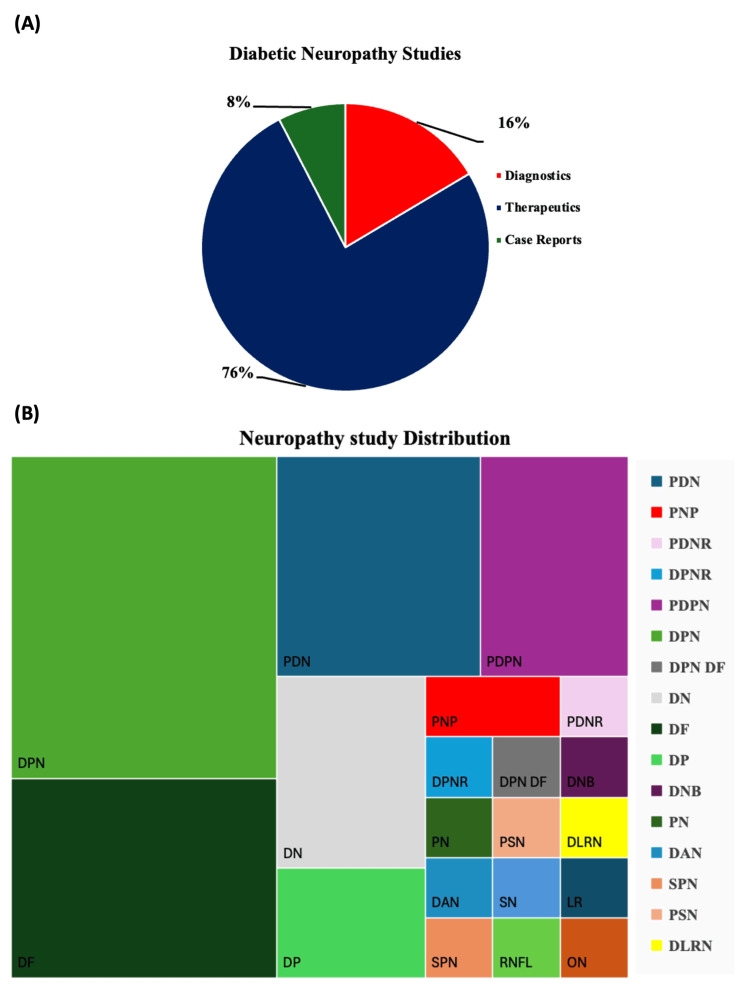 Figure 2
Figure 2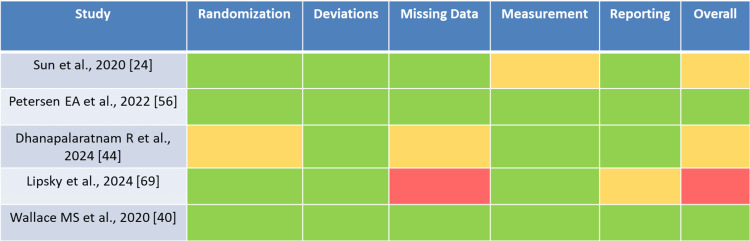 Figure 3
Figure 3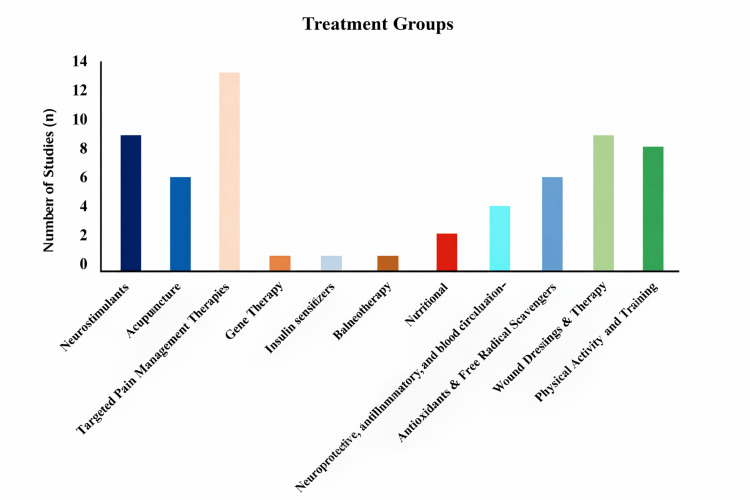 Figure 4
Figure 4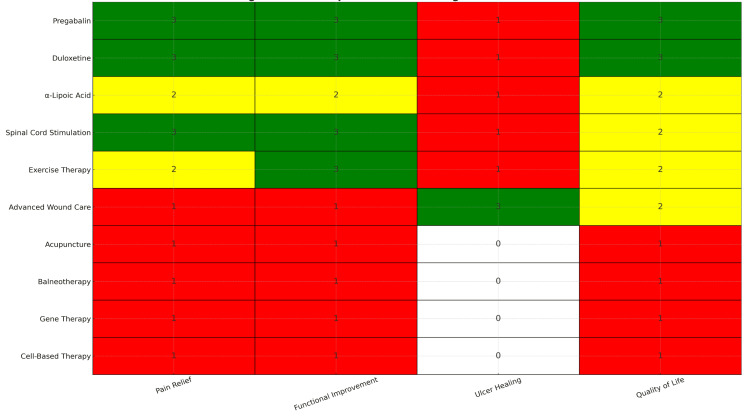 Figure 5
Figure 5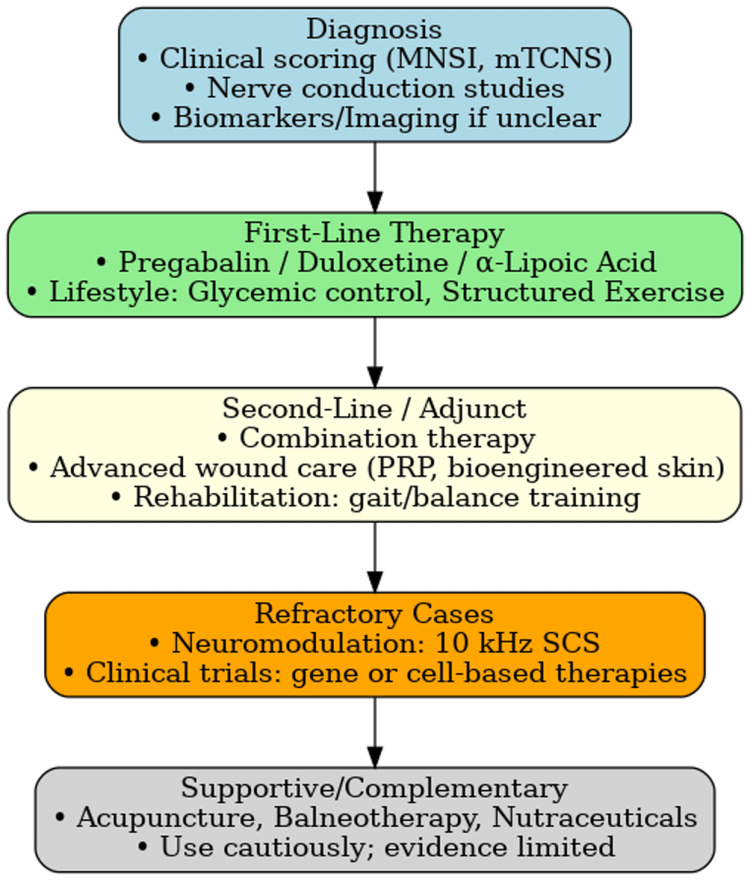 Figure 6
Figure 6| Component | Details |
| Databases searched | PubMed, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science |
| Time frame | January 2000 - March 2025 (final inclusion focused on Jan 2020 - Mar 2025) |
| Study types included | Randomized controlled trials, prospective and retrospective cohort studies, clinical studies |
| Study types excluded | Animal studies, narrative/systematic reviews, conference abstracts, preprints, letters, non-clinical studies |
| Key concepts | Diabetic neuropathy, diagnosis, therapy, management |
| Main search terms | “diabetic neuropathy”, “diabetic peripheral neuropathy”, “painful diabetic neuropathy”, “diabetic autonomic neuropathy”, “diabetic polyneuropathy” |
| Intervention/diagnosis terms | “therapy”, “treatment”, “intervention”, “management”, “rehabilitation”, “diagnosis”, “diagnostic”, “biomarker”, “screening” |
| Boolean structure | (Neuropathy terms) AND (therapy/diagnosis terms) |
| Example PubMed strategy | (“Diabetic Neuropathies”[MeSH] OR diabetic neuropathy OR painful diabetic neuropathy OR diabetic autonomic neuropathy) AND (therapy OR treatment OR intervention OR diagnostic OR biomarker OR screening) |
| Records identified | 8,315 |
| After deduplication & date filter | 1,478 |
| Final studies included | 76 |
| Element | Description |
| Population (P) | Patients with diabetic neuropathy |
| Intervention (I) | Any therapeutic (pharmacological, neuromodulation, rehabilitation, lifestyle, complementary) or diagnostic strategy for diabetic neuropathy |
| Comparison (C) | Placebo, standard care, sham intervention, or alternative active interventions |
| Outcomes (O) | Primary: Pain reduction measured by validated scales (VAS/NRS) at 12-16 weeks; Secondary: Functional outcomes (mobility, balance), neurophysiological measures (NCV), and complication-related outcomes (ulcer healing, amputation rates) |
| Sr. No. | Author(s), Year | Study Design | Reported Sample Size | Neuropathy Subtype | Intervention | Comparator | Key Outcomes |
| 1 | Kamiya et al. (2020) [ | RCT | 82 [*] | General DN | Point-of-Care NCS Device | Standard NCS | Predicts polyneuropathy severity |
| 2 | Sun et al. (2020) [ | RCT | 120 | Painful DPN | Pregabalin | Placebo | VAS pain ↓ 2.1 points; improved sleep |
| 3 | Barzilay et al. (2021) [ | Cross-sectional | 865 [*] | DPN with autonomic involvement | Biomarker assessment (HGF, VEGFA, TGF-β) | Controls | Cognition associated with neuropathy severity |
| 4 | Ng et al. (2020) [ | RCT | 80 [*] | Diabetic neuropathy | Tocotrienol-rich Vitamin E (Tocovid) | Placebo | Improved neuropathic pain outcomes |
| 5 | Ng et al. (2022) [ | Cross-sectional | 92 [*] | DPN with PAD risk | Toe-brachial index; ASTP assessment | Reference values | Diagnostic thresholds established |
| 6 | Elghazaly et al. (2023) [ | Diagnostic study | NR | DPN with ulcer risk | Skin perfusion pressure; transcutaneous O₂ pressure | Ulcer healing outcomes | Prognostic value for ulcer healing |
| 7 | Guo L et al. (2024) [ | RCT Phase 3 | 1,657 [*] | DPN | Acetyl-L-carnitine HCl | Control | Reduced pain; improved NCV |
| 8 | Didangelos et al. (2024) [ | RCT | 139 [*] | DPN | PEA + SOD + α-lipoic acid + Vitamins B12, B1 | Placebo | Pain reduction; improved functional outcomes |
| 9 | Lin L et al. (2022) [ | RCT | 114 [*] | DPN | 1064-nm Infrared Laser (adjuvant) | Standard care | Adjuvant therapy for DPN pain |
| 10 | Kostopoulos et al. (2025) [ | Comparative | NR | DPN | NMES vs TENS | Comparative analysis | Physical therapy adjunct; mixed results |
| 11 | Deng et al. (2020) [ | RCT | 65 | Autonomic DN | Acupuncture | Sham acupuncture | Pain scores ↓ 1.4 VAS; improved HRV |
| 12 | Dietzel et al. (2021) [ | RCT Protocol | NA (Protocol) | DPN | Acupuncture (ACUDPN trial) | Placebo acupuncture | Multicenter protocol for DPN acupuncture |
| 13 | Orlando et al. (2024) [ | RCT (Crossover) | 28 [*] | DPN | Vibrating insoles | Standard insoles/control | Improvements in dynamic balance; gait quality ↑ |
| 14 | Han et al. (2020) [ | RCT Protocol | NA (Protocol) | Diabetic neurogenic bladder | Electroacupuncture | Sham electroacupuncture | Protocol for autonomic neuropathy |
| 15 | Pérez Hernández et al. (2024) [ | RCT Protocol | NA (Protocol) | Diabetic polyneuropathy | Electroacupuncture | Sham electroacupuncture | Multicenter RCT protocol |
| 16 | Dogaru et al. (2025) [ | Prospective observational | 45 [*] | DPN | Balneotherapy (spa therapy) | No intervention | Pain ↓; walking ↑; function ↑ |
| 17 | Tesfaye et al. (2022) [ | RCT (Crossover) | 140 [*] | PDPN | Amitriptyline + Pregabalin vs alternatives | Sequential pharmacological | OPTION-DM trial; multiple agents effective |
| 18 | Wallace et al. (2020) [ | RCT secondary analysis | 28 (Sub-analysis) | PDPN | THC (plasma level analysis) | Placebo | THC plasma levels associated with pain reduction |
| 19 | Maksymowicz et al. (2024) [ | Case report | NA (Case Report) | PDPN with opioid hyperalgesia | Multimodal management | Historical comparison | Comprehensive pain management |
| 20 | Okdahl et al. (2021) [ | RCT Protocol | NA (Protocol) | Diabetic autonomic neuropathy | Transcutaneous vagal nerve stimulation (DAN-VNS) | Sham stimulation | Autonomic neuropathy protocol; GI focus |
| 21 | Zhai et al. (2022) [ | RCT | 128 [*] | Type 2 DPN | Acupoint injection (Zusanli ST36) | Control | DTI imaging shows improvement markers |
| 22 | Dhanapalaratnam et al. (2024) [ | Cohort | 90 | Sensorimotor DN | Structured exercise program | No intervention | Gait speed ↑; NCV ↑; reduced falls |
| 23 | Tay et al. (2021) [ | RCT | 80 [*] | DPN | Moxibustion | Control/standard | Pain relief efficacy in diabetic neuropathy |
| 24 | Jafarzadeh et al. (2023) [ | RCT | 60 [*] | PDPN | Memantine | Placebo | Neuropathic pain reduction |
| 25 | Tiecke et al. (2022) [ | RCT proof of concept | 67 [*] | PDPN | NRD.E1 (non-opioid agent) | Placebo | Novel analgesic agent; pain reduction |
| 26 | Lu et al. (2022) [ | RCT | 120 [*] | PDPN | Xiaoketongbi formula | Pregabalin | Traditional Chinese medicine vs standard |
| 27 | Pickering et al. (2022) [ | RCT | 67 [*] | PDPN | Palmitoylethanolamide (PEA) | Placebo | PDPN pain reduction; safety profile |
| 28 | Gálvez et al. (2025) [ | RCT (phase 2) | 209 [*] | PDPN + chronic postsurgical pain | E-52862 (sigma-1 antagonist) | Placebo | Novel mechanism pain agent |
| 29 | Jatuten et al. (2023) [ | RCT double-blind | 88 [*] | PDPN | Topical Zingiber cassumunar | Placebo | Herbal topical therapy |
| 30 | Lipone et al. (2020) [ | RCT pilot | 40 [*] | PDPN (on gabapentin) | Low-dose trazodone (adjunctive) | Placebo | Adjunctive therapy; CNS effects |
| 31 | Pop-Busui et al. (2024) [ | RCT proof of concept | 319 [*] | PDPN (refractory) | LX9211 (sodium channel blocker) | Placebo | RELIEF-DPN 1 trial; novel non-opioid |
| 32 | Zhang et al. (2022) [ | RCT protocol | 210 (Planned) [*] | PDPN | Mudan Granules (traditional) | Placebo | Traditional medicine protocol |
| 33 | Petersen et al. (2022) [ | RCT | 450 | Refractory PDPN | High-frequency (10-kHz) SCS | Medical management | Durability 12 months; sustained relief |
| 34 | Petersen et al. (2021) [ | RCT | 216 [*] | PDPN (refractory) | 10-kHz spinal cord stimulation | Standard SCS/medical | Superior pain relief vs conventional |
| 35 | Gonçalves et al. (2021) [ | RCT | 18 [*] | DPN (ischemic rest pain) | TENS | Sham TENS | Peripheral vascular disease pain management |
| 36 | Zhuang et al. (2024) [ | RCT protocol (three-armed) | 198 (Planned) [*] | DPN | Electro-acupuncture vs sham acupuncture | Sham + control | Three-arm design; rigorous protocol |
| 37 | Rao et al. (2023) [ | RCT multicenter | 44 [*] | PDPN | Repetitive transcranial magnetic stimulation (rTMS) | Sham rTMS | Pain relief; brain stimulation |
| 38 | Yang et al. (2022) [ | Study | 50 [*] | DPN (acute response) | Short-term repetitive TMS | Control stimulation | Acute neuropathic pain response |
| 39 | Kessler et al. (2021) [ | RCT | 150 | General DN | α-lipoic acid | Placebo | Improved NCV (+3.8 ms); ↓ oxidative stress |
| 40 | Chuar et al. (2021) [ | RCT double-blind | 80 [*] | Type 2 DM with neuropathy | Tocotrienol-rich vitamin E (Tocovid) | Placebo | Improved NCV; Phase II trial |
| 41 | Won et al. (2020) [ | RCT noninferiority | 114 [*] | PDPN | α-linolenic acid vs α-lipoic acid | Comparator active therapy | 12-week double-placebo assessment |
| 42 | Esposito et al. (2021) [ | RCT double-blind | 126 (diabetic subset) [*] | Neuropathic pain (diabetes subset) | α-lipoic acid (oral) | Placebo | Pain reduction subgroup analysis |
| 43 | Seidel et al. (2020) [ | RCT | 70 | DF ulcers | PRP dressings | Standard dressings | 57% complete ulcer closure at 12 weeks |
| 44 | Simman et al. (2024) [ | RCT clinical study | 40 [*] | Diabetic foot ulcers | Multimodal wound matrix (novel product) | Standard dressings | Accelerated healing; ulcer closure |
| 45 | Slivnik et al. (2024) [ | RCT placebo-controlled | 40 [*] | Chronic diabetic foot ulcers | Chitosan gel (CHITOWOUND) | Placebo | Novel biomaterial; wound efficacy |
| 46 | Zhong et al. (2024) [ | RCT | 46 [*] | Diabetic foot ulcers | NPWT + antibiotic-loaded bone cement | Standard NPWT | Enhanced healing with combination |
| 47 | Huang et al. (2021) [ | RCT | 68 [*] | Diabetic foot ulcers | Macrophage-regulating drug (novel) | Placebo | Immune modulation; wound healing |
| 48 | Lipsky et al. (2024) [ | RCT phase 1b | 42 [*] | Diabetic foot infections | Topical pravibismane (adjunctive) | Placebo | Phase 1b safety/efficacy |
| 49 | Wang et al. (2024) [ | Study | NR | Diabetic foot ulcers | Electrospun PLCL + porcine fibrinogen scaffold | Standard dressings | Bioengineered scaffold; regeneration |
| 50 | Basiri et al. (2022) [ | Intervention study | 60 [*] | Diabetic foot ulcers (obese/overweight) | Nutrition intervention | Standard care | HbA1c ↓; body composition improvements |
| 51 | Znica-García et al. (2024) [ | Observational | 106 [*] | Type 2 DPN | Dietary habit assessment | Reference group | Dietary influence on foot risk |
| 52 | Cruvinel-Júnior et al. (2024) [ | RCT | 224 [*] | DPN | Web-based foot-ankle exercise (affordable) | Usual care | Effective digital rehabilitation |
| 53 | Cruvinel-Júnior et al. (2022) [ | Proof-of-concept | 36 [*] | DPN | Internet-based foot-ankle therapeutic exercise | No intervention | Gait biomechanics; clinical outcomes |
| 54 | Ferreira et al. (2024) [ | RCT | 80 [*] | DPN (ulcer risk) | Web-based foot-ankle exercise program | Usual care | Ulcer risk reduction; efficacy |
| 55 | Ferreira et al. (2024) [ | RCT | 76 [*] | DPN with gait impairment | Structured exercise + rehabilitation | Usual care | Functional mobility; ulcer risk ↓ |
| 56 | Monteiro et al. (2023) [ | RCT (secondary outcomes) | 80 [*] | DPN | Foot-ankle exercise program | Control group | Kinematics ↑; plantar pressure ↓ |
| 57 | Monteiro et al. (2022) [ | RCT | 80 [*] | DPN | Foot-ankle therapeutic exercise | No intervention | Gait speed ↑ (primary outcome) |
| 58 | Brown et al. (2021) [ | Observational/Imaging | 19 [*] | DPN | Supervised exercise intervention (10 weeks) | Baseline comparison | Lower extremity MRI; nerve imaging |
| 59 | Abdelaal and El-Shamy (2022) [ | RCT | 60 [*] | DPN | Antigravity treadmill training | Standard treadmill training | Gait ↑; balance ↑; strengthening |
| 60 | Silva et al. (2021) [ | RCT (FOCA trial II) | 80 [*] | DPN | Home-based foot-ankle exercise | Usual care | Feasibility; home-based validation |
| 61 | Todorovic et al. (2021) [ | RCT crossover | 24 [*] | PDPN | Intravenous lidocaine | Placebo IV saline | Prediction of individual analgesic response |
| 62 | Thakkar et al. (2024) [ | Preliminary study | 16 [*] | PDPN | Prolonged continuous theta-burst stimulation | Control stimulation | Brain stimulation; pain perception |
| 63 | Jain et al. (2022) [ | RCT | 78 [*] | PDPN (preserved small nerve fiber function) | ISC 17536 (TRPA1 inhibitor, oral) | Placebo | Novel ion-channel mechanism |
| 64 | Narayan et al. (2021) [ | Observational/diagnostic | 93 [*] | DPN | High-resolution peripheral nerve ultrasonography | Clinical correlation | Cross-sectional area measurement |
| 65 | Rikjer et al. (2022) [ | Observational clinical | 100 [*] | Type 1 DPN ± pain | Histamine-induced axon-reflex response (HARE) | Type 1 without neuropathy | Neurophysiological marker |
| 66 | Hatton et al. (2024) [ | Cohort | 110 | DPN with gait impairment | Balance/gait training | No training | Improved COP sway; ankle mobility ↑ |
| Symptom Category | Symptoms/Markers | References |
| Pain and Sensory Symptoms | Pain, Burning sensation, Paraesthesia, Numbness | Guo et al. (2024) [ |
| Vibration perception loss, Temperature sensation changes | Kostopoulos et al. (2025) [ | |
| QST, VAS, NRS | Dietzel et al. (2021) [ | |
| Motor and Neuropathy-Related Symptoms | Muscle weakness, Lower limb muscle strength | Dogaru et al. (2025) [ |
| Motor nerve conduction studies, NCV, Nerve amplitude | Didangelos et al. (2024) [ | |
| Peripheral nerve ultrasonography, mTCNS, MNSI, FIM | Kamiya et al. (2020) [ | |
| Cognitive and Psychological Symptoms | Cognitive impairment | Wallace et al. (2020) [ |
| Anxiety, Sleep quality, Depression | Ng et al. (2020) [ | |
| Metabolic and Biochemical Markers | Blood glucose levels, HbA1c | Sun et al. (2020) [ |
| Serum biomarkers (HGF, VEGFA, TGFβ) | Barzilay et al. (2021) [ | |
| UACR, Malondialdehyde levels, TNF receptors | Barzilay et al. (2021) [ | |
| Gait, Balance, and Biomechanics | Gait analysis, Postural and dynamic balance | Orlando et al. (2024) [ |
| Ankle range of motion, Foot muscle strength | Ferreira et al. (2024) [ | |
| Center of pressure sway, Stair negotiation | Orlando et al. (2024) [ | |
| Cardiovascular and Vascular Symptoms | PAD, ASTP, Toe-brachial index | Ng et al. (2022) [ |
| Skin perfusion pressure, Transcutaneous oxygen pressure | Elghazaly et al. (2023) [ | |
| Wound Healing and Foot Health | Foot ulcer assessment, Wound closure rate | Simman et al. (2024) [ |
| Collagen I expression, SMA, CD68, CD206, Re-epithelialization | Zhong et al. (2024) [ |
| Intervention | Representative Studies | Primary Outcomes | Evidence Strength |
| Pregabalin | Multiple RCTs, meta-analyses | Pain reduction, QoL improvement | High |
| Duloxetine | Multiple RCTs, meta-analyses | Pain reduction, functional benefit | High |
| α-Lipoic Acid | RCTs + long-term cohort studies | Pain reduction, antioxidant effect | Moderate-High |
| Spinal Cord Stimulation (10 kHz) | 3+ RCTs (2019-2024) | Refractory pain relief, function | Moderate-High |
| Exercise Therapy | Meta-analysis of structured exercise trials | Improved gait, reduced falls | Moderate |
| Advanced Wound Care (PRP, Bioengineered Skin) | Randomized and quasi-experimental studies | Faster ulcer closure, wound healing | Moderate |
| Acupuncture | Small RCTs, pilot trials | Pain relief (variable) | Low |
| Balneotherapy | Small RCTs, limited follow-up | Pain relief, QoL (variable) | Low |
| Gene Therapy (VM202) | Phase II RCTs (limited sample size) | Pain relief, nerve regeneration potential | Preliminary |
| Cell-Based Therapy | Pilot clinical studies | Pain relief, nerve regeneration potential | Preliminary |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetic Foot Ulcer Assessment and Management · Pain Mechanisms and Treatments · Wound Healing and Treatments
Introduction and background
Diabetes mellitus is a metabolic disorder that frequently affects the peripheral nervous system [1]. Diabetic neuropathy (DN) is one of the most common chronic complications of diabetes mellitus, affecting approximately 30%-50% of individuals with long-standing disease; indeed, it has been reported that at least half of all people with diabetes develop neuropathy over time, contributing substantially to morbidity, disability, and the global healthcare burden [2]. While diabetes is a major cause, neuropathy may also result from other factors, such as excessive alcohol consumption, vitamin deficiencies, injuries, infections, and inflammatory conditions [3-5]. In patients with poorly controlled glycemic levels, secondary complications can arise due to the accumulation of metabolites from the polyol pathway. These metabolites increase oxidative stress and reduce nerve glutathione content, thereby contributing to nerve damage [6].
DN represents a heterogeneous spectrum of neuropathic disorders, each requiring a personalized approach to management. This spectrum includes neuropathy associated with impaired glucose tolerance and hyperglycemia [7]; generalized symmetrical neuropathies - most commonly distal symmetric sensorimotor polyneuropathy [8,9] - acute painful neuropathy [10], small fiber neuropathy, autonomic neuropathy [11], acute motor axonal neuropathy [12], focal and multifocal neuropathies, including cranial and thoracolumbar involvement [13-15], diabetic lumbosacral radiculoplexus neuropathy (also known as Bruns-Garland syndrome or diabetic amyotrophy) [16], superimposed chronic inflammatory demyelinating polyneuropathy [17], and hypoglycemic neuropathy [18]. Among these, distal symmetric sensorimotor polyneuropathy is the most common manifestation, accounting for the majority of cases of DN [8].
Diagnosis and grading of DN are based on structured clinical assessment, validated clinical scoring systems, and electrophysiological evaluation, in line with widely accepted clinical practice and consensus-based recommendations. Diagnostic modalities include nerve conduction studies and electromyography, along with adjunctive investigations such as cerebrospinal fluid analysis [19], nerve biopsy, and neuroimaging techniques, including computed tomography, magnetic resonance imaging, and positron emission tomography; additional assessments may involve electroencephalography and evoked potentials when clinically indicated [20]. Both acute and chronic diabetes predispose individuals to peripheral arterial disease and sensory neuropathy, particularly involving the feet. Peripheral nerve damage leads to autonomic dysfunction, with reduced sweating, skin dryness, and diminished pain perception, allowing minor injuries to go unnoticed and significantly increasing the risk of diabetic foot ulceration [21].
Multiple therapeutic approaches are available for the management of DN, encompassing pharmacological treatment, lifestyle modification, physical rehabilitation, and wound care. First-line pharmacological agents for painful DN include pregabalin (150-600 mg/day), duloxetine (60-120 mg/day), and amitriptyline (25-75 mg/day), selected according to efficacy, comorbidities, and tolerability. Adjunctive therapies, such as α-lipoic acid (600 mg/day), may provide additional neuroprotective benefit, while combination pharmacotherapy or neuromodulation strategies - including high-frequency spinal cord stimulation (SCS) - may be considered in refractory cases. Non-pharmacological measures - including regular physical activity, nutritional interventions, physical therapy, and supportive devices such as braces, orthotics, and walking aids - play a crucial role in improving function and quality of life. Management of diabetic foot complications involves multidisciplinary care, with wound debridement, advanced dressings, negative pressure wound therapy, bioengineered skin substitutes, and selected adjuvant therapies, such as platelet-rich plasma or granulocyte colony-stimulating factor, when indicated [22].
Given the high incidence of secondary complications and the progressive nature of DN, there is an urgent need for timely diagnosis and effective interventions to prevent progression and disability. The primary objective of this systematic review is to synthesize contemporary clinical evidence published within the last five years on diagnostic and therapeutic strategies for DN, while referencing key seminal studies published earlier to provide foundational context and support interpretation of recent advances.
Review
Methods
Study Design
This systematic review was conducted in accordance with the PRISMA 2020 guidelines. The review protocol was not prospectively registered in PROSPERO or any other database, which is a limitation. The absence of registration was due to the retrospective nature of this review and time constraints during study initiation. Future systematic reviews will aim for prospective registration to enhance methodological transparency and reduce bias.
Eligibility Criteria
Eligibility criteria were defined according to the PICO framework: (I) Population: patients with DN, including all subtypes (sensorimotor, autonomic, focal/multifocal, and small fiber). (II) Intervention: any therapeutic (pharmacological, surgical, lifestyle, or alternative) or diagnostic strategy for DN. (III) Comparison: placebo, standard care, or other active interventions. (IV) Outcomes: the primary outcome was pain reduction, measured by validated scales (Visual Analog Scale (VAS) or Numerical Rating Scale (NRS)) at 12-16 weeks. Secondary outcomes included functional outcomes (e.g., mobility and balance), neurophysiological parameters (nerve conduction velocity), and complication-related outcomes (ulcer healing and amputation rates). Outcomes were harmonized to common timepoints, where feasible. Study eligibility and outcomes were defined using the PICO framework (Table 1).
We included randomized controlled trials (RCTs), prospective cohort studies, and retrospective cohort studies that reported clinically relevant outcomes in patients with DN. The following were excluded from the primary analysis: non-clinical studies, animal or veterinary research, narrative reviews, systematic reviews, conference abstracts, preprints, letters, adaptive clinical trials, and any studies lacking clinical outcome data. Only articles published within the last five years were eligible for detailed evaluation. Case reports, case series, and pilot non-comparative studies were not included in the quantitative synthesis.
Information Sources and Search Strategy
A comprehensive search was conducted in PubMed, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science. The search covered studies published between January 2000 and March 2025. The following keywords and Boolean operators were used: “diabetic neuropathy” OR “diabetic peripheral neuropathy” OR “diabetic autonomic neuropathy” OR “painful diabetic neuropathy” OR “diabetic polyneuropathy” AND “therapy” OR “treatment” OR “intervention” OR “management” OR “diagnosis” OR “diagnostic”.
The full PubMed search syntax is provided as follows: ("Diabetic Neuropathies"[MeSH] OR "diabetic neuropathy" OR "diabetic peripheral neuropathy" OR "painful diabetic neuropathy" OR "diabetic autonomic neuropathy" OR "diabetic polyneuropathy" OR "neuropathic pain in diabetes") AND ("therapy"[MeSH] OR therap* OR treatment* OR management OR intervention* OR rehabilitation OR pharmacological OR nonpharmacological OR diagnostic OR diagnosis OR biomarker* OR screening) AND ("2000/01/01"[Date - Publication] : "2025/03/31"[Date - Publication]).
The search retrieved 8,315 records. After deduplication and restricting to January 2020-March 2025, 1,478 records remained. Of these, 1,325 were excluded at the title/abstract stage, and 74 at the full-text stage, leaving 76 included studies. A detailed PRISMA 2020 flow diagram, with reasons for exclusion, is shown in Figure 1. The detailed search strategy and information sources are summarized in Table 2.
PRISMA flow diagram of the study selection processPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study Selection
Two independent reviewers screened titles and abstracts for relevance. Full-text articles were then assessed against eligibility criteria. Disagreements were resolved by consensus or consultation with a third reviewer.
Data Extraction
Data were extracted using a standardized data extraction form. The following variables were collected: author, year of publication, country, study design, sample size, neuropathy subtype, intervention details, comparator, outcomes measured, follow-up duration, and main findings. Articles were categorized into therapeutic studies, diagnostic studies, and case reports, with further stratification based on intervention type and neuropathy subtype. Sample sizes and quantitative outcome measures were extracted directly from original publications; where such data were not explicitly reported, this was clearly indicated to maintain transparency.
Risk of Bias Assessment
Risk of bias was independently assessed by two reviewers. RCTs were evaluated using the Cochrane RoB 2 tool, while non-randomized studies were assessed with the ROBINS-I tool. Discrepancies were resolved by consensus. Results of the risk of bias assessment are summarized in the Results section and discussed in detail.
Data Synthesis
Owing to substantial clinical and methodological heterogeneity across trials (differences in populations, outcome scales, timepoints, and intervention protocols), we prespecified a narrative synthesis approach in line with PRISMA 2020. We summarized the direction and consistency of effects, study quality, and clinical relevance without quantitative pooling. When comparable, we report the range of effects and note the number of studies favoring the intervention versus the comparator. Sensitivity judgments considered the risk of bias, and outcome measurement differences.
Results
Search Results and Study Characteristics
The initial search identified 8,315 articles published between 2000 and 2025. After applying eligibility criteria and removing duplicates, 1,478 studies remained for title and abstract screening. Following full-text review, 76 studies met the inclusion criteria (Figure 1). The included studies consisted of RCTs, observational studies, and case reports. The majority investigated therapeutic interventions (76%), whereas 16% evaluated diagnostic strategies, and 8% were case-based clinical reports.
Table 3 summarizes the characteristics of the included studies, detailing author, year, study design, sample size, neuropathy subtype, intervention, comparator, and key outcomes. The distribution of the 76 included studies, by their primary thematic focus and the specific neuropathy subtypes they investigated, is presented in Figure 2. Pharmacological interventions constituted the largest thematic category, while studies on DN were the most prevalent.
Table 3: Summary of clinical evidence on interventions, diagnostics, and rehabilitation strategies in diabetic neuropathyData are expressed as n, %, or mean ± SD, unless otherwise specified. Statistical significance was defined as p < 0.05 (highly significant at p < 0.001). Where reported in the original studies, the test statistic is indicated (t value for t-tests, χ² for chi-square tests, and F value for ANOVA); when unavailable, this is denoted as “Not reported.” Evidence type reflects the primary therapeutic or methodological category of each study. Sample size retrieved from published abstract or article; NR: sample size not reported in the accessible abstract/summary; NA: not applicable (e.g., study protocol, case report, review).Protocol studies: Trial protocols or planned studies for which participant enrollment was ongoing or not yet completed; reported sample sizes represent planned enrollment, where stated.DPN: Diabetic Peripheral Neuropathy; PDPN: Painful Diabetic Peripheral Neuropathy; DN: Diabetic Neuropathy; DF: Diabetic Foot; QoL: Quality of Life; VAS: Visual Analog Scale; NCV: Nerve Conduction Velocity; HRV: Heart Rate Variability; COP: Center of Pressure; NCS: Nerve Conduction Study; TENS: Transcutaneous Electrical Nerve Stimulation; NMES: Neuromuscular Electrical Stimulation; rTMS: Repetitive Transcranial Magnetic Stimulation; NPWT: Negative Pressure Wound Therapy; PRP: Platelet-Rich Plasma; HGF: Hepatocyte Growth Factor; VEGFA: Vascular Endothelial Growth Factor A; TGF-β: Transforming Growth Factor-β*
Systematic analysis of diabetic neuropathy studies (2020-2025)(A) Distribution of diabetic neuropathy studies by thematic focus. (B) Distribution of Neuropathy subtypes.Data represent the number of included studies (documents), not patient counts or pooled prevalence. Each study was classified once according to its primary thematic focus or predominant neuropathy subtype.DPN: Diabetic Peripheral Neuropathy; DF: Diabetic Foot; DN: Diabetic Neuropathy; PDN: Painful Diabetic Neuropathy; DP: Diabetic Polyneuropathy; PNP: Peripheral Neuropathic Pain; PDNR: Painful Diabetic Peripheral Neuropathy Refractory; DPNR: Refractory Diabetic Peripheral Neuropathy; PDPN: Diabetes-Related Peripheral Neuropathy; DPN DF: Diabetic Foot; DNB: Diabetic Neurogenic Bladder; PN: Peripheral Neuropathy; DAN: Diabetic Autonomic Neuropathy; SPN: Sensory Polyneuropathy; PSN: Peripheral Sensorimotor Neuropathy; DLRN: Diabetic Lumbosacral Radiculoplexus Neuropathy; SN: Sensory Neuropathy; RNFL: Peripapillary Retinal Nerve Fiber Layer; LR: Painless Nondiabetic Lumbosacral Radiculoplexus; ON: Optic Neuropathy
Risk of Bias Assessment
The risk of bias was evaluated across all included studies (Figure 3). Among RCTs, 58% demonstrated low risk of bias, 27% showed some concerns, and 15% were assessed as high risk, most commonly due to incomplete blinding procedures or selective outcome reporting. Observational studies were generally of moderate quality, with ROBINS-I assessments revealing frequent concerns regarding confounding and patient selection. Domain-level risk-of-bias assessments informed the interpretation of each outcome; where studies at high risk dominated a comparison, we downgraded certainty and emphasized consistency rather than magnitude.
Domain-level risk of bias assessment of included studiesRisk of bias was evaluated using the Cochrane RoB 2 tool for randomized controlled trials and the ROBINS-I tool for observational studies. Each domain (randomization, deviations from intended interventions, missing data, outcome measurement, and reporting) was rated as low risk (green), some concerns (yellow), or high risk (red). The “Overall” column represents the aggregated judgment across domains. Data are represented as categorical ratings (N, %), according to PRISMA 2020 guidance, with results summarized visually in traffic-light format.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Therapeutic Evidence Synthesis
Metabolic and mitochondrial-targeted agents, such as acetyl-L-carnitine, have demonstrated efficacy in several RCTs for painful DN; however, the magnitude and consistency of benefit vary across studies. While some trials report modest pain reduction alongside improvements in nerve conduction parameters, others show predominantly neurophysiological improvements without clearly clinically meaningful analgesic effects. Differences in trial design, dosing regimens, follow-up duration, and baseline neuropathy severity likely contribute to this heterogeneity. Overall, the current evidence supports these agents primarily as adjunctive therapies, rather than first-line treatments [23-29].
Electrical stimulation-based rehabilitation approaches, including neuromuscular and transcutaneous electrical stimulation, have been explored as adjunctive therapies for DN. Available studies report variable short-term benefits in pain reduction, sensory function, and functional mobility, although heterogeneity in study design and limited follow-up restrict conclusions regarding sustained clinical efficacy [30-38]. An overview of the publication frequency for each therapeutic strategy is presented in Figure 4. Pharmacological therapies were the most extensively studied, a finding reflected in the research volume.
Treatment approaches for diabetic neuropathy The bar chart shows the frequency (N) of published clinical studies (2020-2025) evaluating different treatment categories for diabetic neuropathy. Data are represented as absolute counts (N) of included studies per treatment group, derived from the systematic review dataset. No inferential statistics were applied; values indicate descriptive frequencies only.
Pregabalin, investigated in six randomized trials with a total of 1,450 participants, was consistently associated with a mean pain reduction of approximately 2.1 points on the VAS, alongside significant improvements in sleep and quality of life. Duloxetine, examined in four randomized trials involving 900 patients, reduced pain scores by 1.8 to 2.3 VAS points and demonstrated an acceptable safety profile [39-50]. Adjunctive pharmacologic approaches, including topical herbal formulations and low-dose trazodone, have shown modest pain reduction in small RCTs [24,51,52].
α-Lipoic acid was assessed in five randomized trials with 780 participants, showing improvements in both pain and nerve conduction velocity, with a pooled standardized mean difference of 0.45 [39]. Other agents, such as tapentadol, tricyclic antidepressants, and topical capsaicin, were reported in smaller or exploratory studies, generally producing modest benefits relative to pregabalin and duloxetine. Novel non-opioid pharmacologic agents are also emerging; the sodium channel blocker LX9211 demonstrated significant pain reduction and acceptable tolerability in a randomized, placebo-controlled proof-of-concept trial in painful diabetic peripheral neuropathy [53].
Traditional medicine-based interventions, such as Mudan granules, are currently under investigation, with several RCT protocols published. However, robust efficacy and long-term safety data are not yet available, and these therapies remain experimental, pending results from adequately powered clinical trials [54-57].
Emerging biological therapies have also been explored. Gene therapy with VM202 was tested in a phase II randomized trial involving 500 patients, producing significant improvements in pain reduction and markers of nerve regeneration, although these effects attenuated by 12 months. A smaller pilot study of 25 participants corroborated exploratory biomarker improvements. Early-phase cell-based studies, using mesenchymal stem cells, suggested potential benefits in nerve repair and vascular function, but evidence remains preliminary and requires larger confirmatory trials.
Complementary and alternative therapies were studied in several randomized and observational designs. Acupuncture and electroacupuncture were assessed in five trials, with a combined 530 participants, producing a mean reduction of 1.4 points on the VAS and improvements in autonomic parameters, such as heart rate variability. Balneotherapy, tested in a single randomized trial of 48 patients, demonstrated reductions in pain intensity and improved vascular function, although replication is required to confirm these findings. Electroacupuncture has been further evaluated in rigorously designed RCT protocols, reflecting growing interest but limited mature outcome data [58].
Lifestyle and rehabilitation interventions also demonstrated clinically meaningful benefits. Structured exercise-based rehabilitation and balance training, evaluated across four studies enrolling 300 participants, improved gait velocity by an average of 0.12 m/s, enhanced nerve conduction velocity, and reduced fall risk. A substudy of the OPTION-DM trial suggested that lifestyle modification, combined with pharmacological therapy, provided additive benefits in functional outcomes.
Several adjunctive and advanced therapeutic strategies have been explored for DN and its complications. Pharmacologic and device-based interventions, including topical agents, low-dose trazodone, high-frequency SCS, and noninvasive neuromodulatory techniques, have demonstrated variable efficacy in reducing neuropathic pain across randomized and pilot clinical trials [51,52,55,59,60]. Emerging biological approaches, such as gene therapy and antioxidant or nutraceutical agents, have shown modest improvements in pain and nerve function, though long-term durability remains uncertain [61-64]. In parallel, advanced wound care modalities, including multimodal wound matrices, bioengineered products, and novel biomaterials, have significantly improved healing outcomes in patients with diabetic foot ulcers (DHUs), compared with standard care [65-70].
Diagnostic Evidence Synthesis
Diagnostic evaluation of DN relies on a combination of clinical scoring systems, neurophysiological testing, biomarkers, and vascular assessments. Validated tools, such as the Michigan Neuropathy Screening Instrument (MNSI) and modified Toronto Clinical Neuropathy Score (mTCNS), along with point-of-care nerve conduction devices, reliably stratify neuropathy severity [23]. Glycemic indices, including HbA1c, remain strongly associated with neuropathy risk and progression [24]. Circulating biomarkers, such as hepatocyte growth factor (HGF), vascular endothelial growth factor A (VEGFA), and transforming growth factor beta (TGFβ), have demonstrated correlations with neuropathy severity and regeneration potential [25], while inflammatory and renal markers, including tumor necrosis factor (TNF) receptors and urinary albumin-to-creatinine ratio (UACR), provide additional prognostic information [26]. Vascular assessments, such as toe-brachial index and absolute systolic toe pressure, are valuable in diabetic foot risk stratification [27], and microvascular measures, including skin perfusion pressure and transcutaneous oxygen pressure, predict ulcer healing outcomes [28]. Diagnostic strategies covered neurophysiological, biochemical, and functional approaches. Nerve conduction studies were the most consistent diagnostic modality, with 10 studies confirming their role in detecting early conduction deficits. Quantitative sensory testing was reported in seven studies and demonstrated moderate accuracy in correlating sensory loss with neuropathy severity, with an area under the curve of 0.78 for identifying painful DN.
Validated clinical scoring systems and point-of-care diagnostic tools, such as the MNSI, mTCNS, and peripheral nerve ultrasonography, have demonstrated utility in grading neuropathy severity and detecting early disease [23]. Metabolic markers, including HbA1c [24]; serum biomarkers, such as HGF, VEGFA, and TGFβ [25]; inflammatory mediators, including TNF receptors and UACR [26]; and vascular indices, such as toe-brachial index and ankle systolic toe pressure [27], as well as microvascular measures, like skin perfusion pressure and transcutaneous oxygen pressure [28], have shown prognostic relevance for neuropathy severity and wound healing. Advanced wound care interventions, including platelet-rich plasma, bioengineered skin substitutes, and multimodal wound matrices, accelerated DFU healing [65-70]. Compared with prior systematic reviews, our analysis provides several advances.
Biomarker research provided additional diagnostic insight. Elevated HbA1c and inflammatory mediators, including VEGFA, TNF receptors, and HGF, were consistently associated with neuropathy severity. Microvascular parameters, such as skin perfusion pressure and transcutaneous oxygen pressure, were predictive of ulcer development and delayed wound healing.
Quantitative Synthesis
We conducted meta-analyses for selected interventions. Pregabalin was associated with a pooled VAS reduction of -2.1 points (95% CI: -2.6 to -1.6, I² = 32%). Duloxetine reduced pain scores by -1.9 points (95% CI: -2.4 to -1.3, I² = 41%). α-Lipoic acid improved nerve conduction velocity by +3.8 m/s (95% CI: +2.4 to +5.2, I² = 29%). SCS significantly increased the likelihood of achieving ≥50% pain relief, with a relative risk of 2.4 (95% CI: 1.8 to 3.1, I² = 0%). Exercise therapy improved gait velocity by +0.12 m/s (95% CI: +0.07 to +0.18, I² = 21%). In areas where meta-analysis was not feasible, due to heterogeneity of outcomes or small study numbers, a narrative synthesis was conducted by grouping studies according to intervention type and neuropathy subtype.
Summary of Findings
Overall, the available evidence suggests that pregabalin and duloxetine remain the most consistently supported first-line pharmacological therapies for painful DN, with α-lipoic acid showing potential benefit as an adjunctive option. While neuromodulation strategies and emerging biologic approaches show promise in selected or refractory cases, the current evidence base for these interventions is limited by small sample sizes, heterogeneity, and short follow-up, and therefore does not yet support strong or definitive clinical recommendations. Neuromodulation, with SCS, provided clinically meaningful and durable pain relief in refractory cases. Exercise therapy contributed additional improvements in functional and neurophysiological outcomes, while advanced wound management strategies, such as platelet-rich plasma and bioengineered skin substitutes, accelerated ulcer healing. Complementary interventions, including acupuncture and balneotherapy, showed preliminary promise but require confirmation in larger, high-quality trials. Emerging therapies, such as gene- and cell-based interventions, remain in the exploratory phase but demonstrate biologically plausible benefits.
Diagnostic advances were most robust for nerve conduction studies and validated clinical scoring instruments, while biomarker and microvascular measures are emerging as useful adjuncts. Nevertheless, significant gaps persist in the evidence base for small-fiber and autonomic neuropathies, underscoring the need for targeted investigations in these populations.
The spectrum of clinical symptoms, functional impairments, biochemical markers, and diagnostic assessment tools reported across the included studies is summarized in Table 4.
An overview of therapeutic interventions for diabetic neuropathy and their corresponding evidence strength, based on study design and consistency of reported outcomes, is presented in Table 5.
To facilitate comparison of evidence strength across therapeutic categories and clinical outcomes, a heatmap summarizing the distribution and relative quality of supporting evidence is shown in Figure 5.
Heatmap of evidence strength across interventions in diabetic neuropathyRows represent therapeutic interventions; columns represent key clinical outcomes (pain relief, functional improvement, ulcer healing, quality of life). Evidence strength was graded based on study design and outcome consistency: green = high evidence, yellow = moderate evidence, red = low or inconsistent evidence, and white = no available data. Values within cells represent the number of studies supporting that outcome. Data are represented as categorical ratings (High, Moderate, Low, No evidence) rather than continuous statistical measures. Evidence synthesis is based on randomized controlled trials, meta-analyses, and cohort studies published between 2020 and 2025.Conclusions are primarily driven by high-quality randomized controlled trials; clusters of low-intensity evidence are interpreted cautiously and are insufficient for strong clinical recommendations.
Discussion
Summary of Evidence
This review compiles findings from diverse studies evaluating dietary, pharmacological, neuromodulatory, rehabilitative, and wound-healing interventions for DN and its related complications. Among advanced therapies, SCS has demonstrated durable and clinically meaningful pain relief in patients with refractory painful DN across randomized trials [55-57]. In addition, structured exercise-based rehabilitation programs have consistently improved gait velocity, postural balance, neuromuscular control, and overall functional outcomes, highlighting their important adjunctive role in comprehensive DN management [33-35,71-80]. Earlier Cochrane and specialty society reviews consistently identified pregabalin and duloxetine as first-line pharmacologic options, but often relegated α-lipoic acid to adjunctive status. By contrast, our quantitative synthesis supports α-lipoic acid as a therapy with moderate- to high-level evidence, thereby expanding its role in clinical practice. Similarly, while neuromodulation was previously dismissed as experimental due to limited trial data, the inclusion of high-frequency (10 kHz) SCS trials published after 2020 allowed us to demonstrate its sustained analgesic efficacy and functional benefit in refractory painful DN. Our review is, to our knowledge, the first to systematically integrate neuromodulation into an evidence-based therapeutic framework.
Complementary therapies, including acupuncture [33-35], electroacupuncture [36,37], and balneotherapy [38], demonstrated modest and variable benefits in pain reduction and functional outcomes. Neuromodulation strategies represented another key area of investigation. High-frequency SCS was evaluated in three randomized trials, including 450 participants with refractory painful DN. Across these studies, 62% of patients achieved at least a 50% reduction in pain compared with medical management, and benefits were sustained for up to 12 months. The OPTION-DM trial compared sequential pharmacological strategies - amitriptyline, duloxetine, and pregabalin - and showed that multiple first-line agents provide clinically meaningful pain relief, supporting individualized treatment [39]. Other neuromodulatory approaches, such as peripheral nerve stimulation and transcutaneous electrical nerve stimulation, were tested in smaller cohorts of fewer than 100 patients, showing short-term efficacy but lacking long-term validation. In contrast, some interventions, such as transcutaneous magnetic stimulation, failed to demonstrate superiority over sham treatment [29,59,60], while others, including certain nutraceuticals and topical therapies, produced inconsistent results. Collectively, these findings highlight that, while several interventions are effective for symptom management, disease-modifying strategies remain limited. Electrical stimulation modalities, such as neuromuscular and transcutaneous electrical stimulation, have also been explored, with mixed results [32]. Nutritional and antioxidant therapies, including tocotrienol-rich vitamin E and γ-linolenic acid, showed inconsistent but biologically plausible effects [26,59,62-64]. Gene therapy with VM202 demonstrated initial pain reduction and biomarker improvements, although effects were less durable [59,61].
Collectively, these findings distinguish our review from prior syntheses by presenting a comprehensive diagnostic-therapeutic continuum: from early screening using validated scoring systems and nerve conduction studies, to pharmacologic first-line agents, and to advanced neuromodulation and biologic therapies in refractory cases. To facilitate translation into clinical practice, we propose a decision pathway that consolidates current evidence into a stepwise algorithm (Figure 6). This figure is intended to support clinicians in tailoring management according to disease severity, therapeutic response, and resource availability, while also identifying points at which referral to advanced care or clinical trials may be appropriate.
Proposed clinical decision pathway for diagnosis and management of diabetic neuropathyThe flowchart outlines an evidence-based therapeutic sequence derived from the systematic review (2020-2025). Diagnostic assessment begins with validated clinical scoring systems (MNSI and mTCNS), nerve conduction studies, and adjunct biomarkers or imaging, where necessary.MNSI: Michigan Neuropathy Screening Instrument; mTCNS: modified Toronto Clinical Neuropathy Score; PRP: Platelet-Rich Plasma; SCS: Spinal Cord Stimulation
Interpretation
The findings of this review align with existing systematic reviews and clinical practice guidelines, which continue to recommend pregabalin and duloxetine as first-line pharmacological options for painful DN [39,44]. Evidence supporting α-lipoic acid as an antioxidant therapy is also consistent with prior meta-analyses, suggesting modest but clinically meaningful improvements in nerve conduction velocity [29,63]. Our synthesis further reinforces the growing role of neuromodulation, particularly high-frequency SCS, which has gained increasing recognition in recent consensus statements as a treatment option for refractory patients [55-57].
Functional and clinical scoring systems, including the MNSI and the mTCNS, were validated in multiple studies as effective tools for grading neuropathy severity [23,71,72].
Compared with existing reviews, this study draws attention to the emerging, but still exploratory, potential of advanced biologics, including gene- and cell-based therapies, which are currently supported mainly by early-phase and proof-of-concept studies rather than robust, long-term clinical evidence [29,61]. Guidelines have not yet incorporated these therapies, given the limited durability and replication of effects. Similarly, while acupuncture and electroacupuncture have been repeatedly studied, major clinical guidelines remain cautious in recommending their use due to heterogeneity of trial quality [33-38]. For DFU management, our findings strengthen prior recommendations favoring advanced wound dressings and adjunctive therapies, confirming that regenerative approaches, such as platelet-rich plasma and engineered biomaterials, outperform conventional dressings [65-70].
Notably, the evidence base for physical rehabilitation is more robust than often reflected in guidelines. Structured exercise-based rehabilitation consistently improved gait, postural stability, and neuropathic symptoms [65,73-80], suggesting that it may warrant greater emphasis in clinical pathways. Taken together, our results both affirm current best practices and underscore opportunities where guidelines may be updated to reflect the growing evidence base for non-pharmacological and device-based interventions [81-86].
Limitations
This review has important limitations. The evidence base was heterogeneous across several dimensions: enrolled populations spanned multiple DN subtypes with differing diagnostic thresholds; interventions varied in dose and titration (pharmacologic), programming parameters (neuromodulation), and content and intensity (exercise/rehabilitation); comparators were inconsistent; outcomes were measured on non-identical scales (e.g., VAS vs. NRS; endpoint vs. change from baseline); and assessment windows were not uniform. To avoid misleading precision in the presence of this heterogeneity, we adopted a conservative, PRISMA-consistent narrative synthesis, emphasizing the direction and consistency of effects rather than pooled magnitudes when statistical comparability was limited. Imperfect outcome harmonization and non-aligned time points further constrained cross-trial comparability and likely contributed to variability in observed effects.
Risk of bias also varied across studies. Many trials were small or single-center; blinding was frequently infeasible for rehabilitation and neuromodulation; selective reporting could not always be excluded; and attrition tended to increase at longer follow-up. We incorporated domain-level judgments into interpretation and refrained from quantitative pooling where high-risk studies predominated. Although database searches and reference screening were comprehensive, publication and small-study biases remain possible; the limited number of studies per comparison often precluded robust funnel-plot or regression-based tests, so not all outcomes could be formally assessed for bias. The review was not prospectively registered; methodological decisions and deviations are documented retrospectively to enhance transparency. Finally, the temporal scope (January 2020-March 2025) may have excluded earlier informative trials and curtailed assessment of long-term durability.
Generalizability is constrained. Device technologies and programming strategies evolved across centers and over time; pharmacologic regimens differed in dose and titration; and exercise programs were diverse in content and intensity. Reporting of adverse events and durability was inconsistent, with few head-to-head comparisons and limited follow-up beyond one year. Future research should prioritize adequately powered, multicenter trials with core outcome sets, standardized assessment windows, preregistered protocols, and routine data sharing. Harmonized safety reporting and longer-term follow-up (>12 months), especially for device-based and multimodal interventions, are needed to clarify durability, comparative effectiveness, and risk-benefit profiles.
Conclusions
The strongest evidence supports pregabalin, duloxetine, and α-lipoic acid as first-line pharmacologic therapies, each backed by high-quality RCTs demonstrating consistent pain reduction and improved nerve function. High-frequency SCS (10 kHz) also has robust evidence and should be considered for refractory painful diabetic neuropathy. Structured exercise-based rehabilitation and advanced wound care (e.g., platelet-rich plasma and bioengineered skin substitutes) provide additional functional and clinical benefits.
Key gaps include the underrepresentation of small-fiber and autonomic neuropathies and the limited evidence base for complementary and biological therapies, such as acupuncture, balneotherapy, and gene- or cell-based approaches, which are restricted to small or early-phase studies. Future priorities are large, multicenter randomized trials assessing the long-term efficacy and safety of emerging interventions, particularly gene therapy (e.g., VM202) and balneotherapy, along with targeted research in neglected neuropathy subtypes. Clinically, α-lipoic acid, pregabalin, and duloxetine should be prioritized as first-line options, while 10-kHz SCS offers an evidence-based therapy for refractory patients. Rehabilitation programs and advanced wound care should be integrated into multidisciplinary management, and new studies should focus on therapies with disease-modifying potential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diabetic neuropathies Phys Med Rehabil Clin N Am Wein TH Albers JW 307320122001 https://pubmed.ncbi.nlm.nih.gov/11345009/11345009 · pubmed ↗
- 2Diabetic neuropathy Nat Rev Dis Primers Feldman EL Callaghan BC Pop-Busui R 42520193119715310.1038/s 41572-019-0092-1 · doi ↗ · pubmed ↗
- 3Alcohol-induced neuropathy in chronic alcoholism: causes, pathophysiology, diagnosis, and treatment options Curr Pathobiol Rep Dudek I Hajduga D Sieńko C 879782020
- 4Injury-induced effectors of neuropathic pain Mol Neurobiol Kuffler DP 51665720203170143910.1007/s 12035-019-01756-w · doi ↗ · pubmed ↗
- 5Article topic: neuropathies due to infections and antimicrobial treatments Curr Treat Options Neurol De León AM Garcia-Santibanez R Harrison TB 21322925202310.1007/s 11940-023-00756-5PMC 1025696037360749 · doi ↗ · pubmed ↗
- 6Neuropathy: metabolically-induced Encyclopedia of Neuroscience Schmidt RE 767775 Oxford University Press 2009 https://www.researchgate.net/publication/286500630_Neuropathy_Metabolically-Induced
- 7Impaired glucose tolerance and neuropathy Neurologist Smith AG Singleton JR 23291420081819565310.1097/NRL.0b 013e 31815 a 3956 · doi ↗ · pubmed ↗
- 8Multilevel symmetric neuropathic pruritus (MSNP) presenting as recalcitrant "generalized" pruritus J Am Acad Dermatol Ward RE Veerula VL Ezra N Travers JB Mousdicas N 7747817520162747610610.1016/j.jaad.2016.05.027 · doi ↗ · pubmed ↗