Obturator Foramen Bypass With Fluoroscopic Guidance for Recurrent Femoral Prosthetic Bypass Occlusions: A Case Report
Hiroto Yasumura, Kenichi Arata, Ryo Imada, Hideyuki Satozono, Koichiro Shimoishi, Yoshihiro Fukumoto, Goichi Yotsumoto, Yuki Ogata, Tomoyuki Matsuba, Yoshiharu Soga

TL;DR
This case report describes a successful surgical bypass through the obturator foramen to treat a patient with multiple blocked femoral bypasses and chronic limb-threatening ischemia.
Contribution
The paper presents a novel application of obturator foramen bypass using fluoroscopic guidance to address femoral crowding and hip flexion-induced compression.
Findings
Obturator foramen bypass was successfully performed under live fluoroscopic guidance using Artis zeego.
The graft remained patent for 12 months post-surgery, with no complications.
The procedure avoided the risks of groin infection and femoral compression during hip flexion.
Abstract
Repeated and additional prosthetic bypass to the femoral artery causes femoral crowding and adhesion and increases the risk of bypass infection. The femoral crowding may cause the stenosis of native and prosthetic bypass during hip flexion. An obturator foramen bypass is a bypass from a particular branch of the abdominal aorta to the lower limb artery to circumvent groin infection. This procedure is particularly effective in treating infected femoral prosthetic bypasses and mycotic femoral artery aneurysms; however, the bypass is routed through a narrow obturator foramen, which requires advanced technical skills. A 57-year-old Japanese man with a history of a coronary stent occlusion and a terminal aorta-left common femoral artery (CFA) prosthetic bypass occlusion underwent a right external iliac artery (EIA)-left superficial femoral artery (SFA) crossover prosthetic bypass. At the age…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
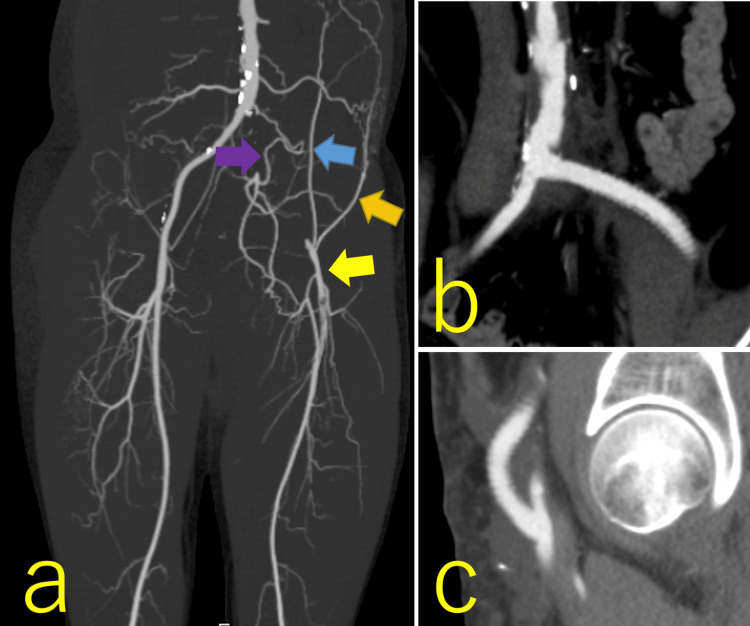 Figure 1
Figure 1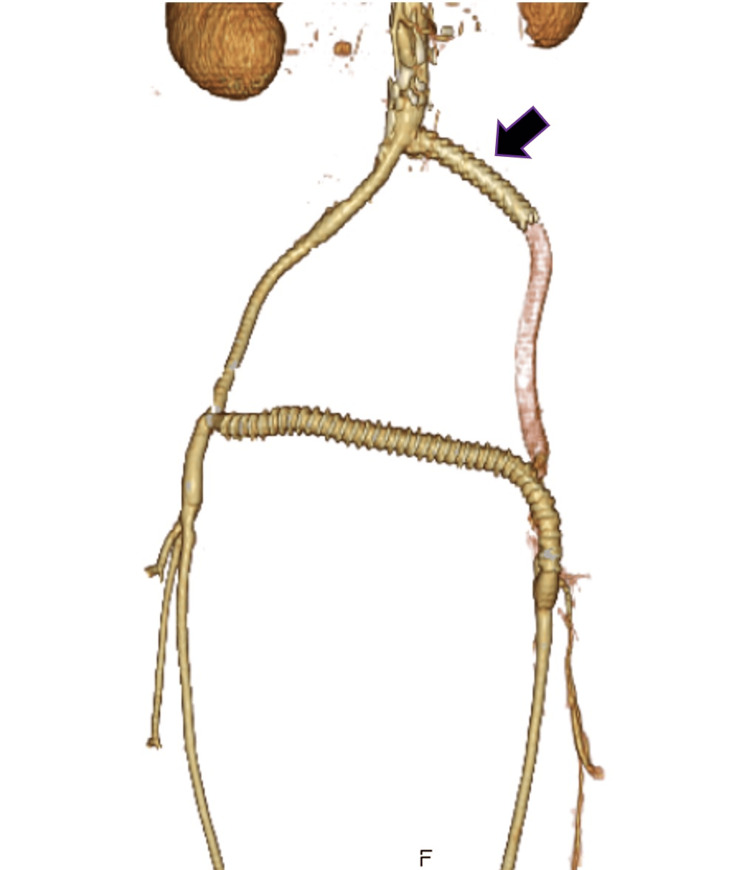 Figure 2
Figure 2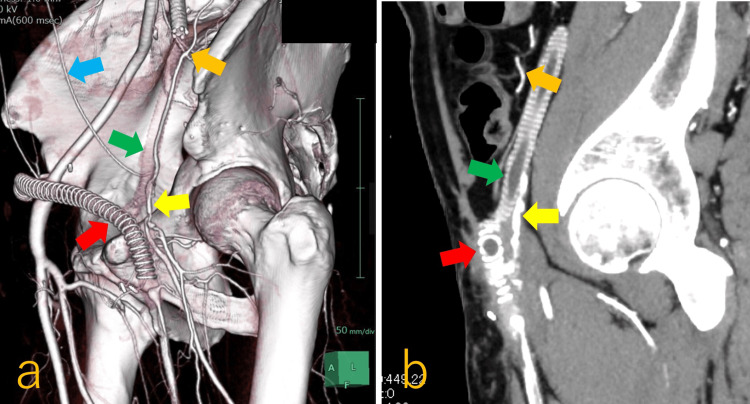 Figure 3
Figure 3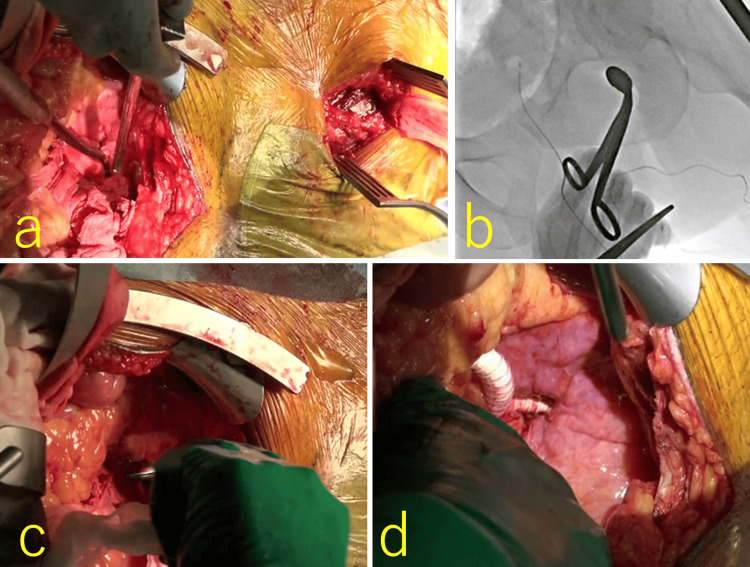 Figure 4
Figure 4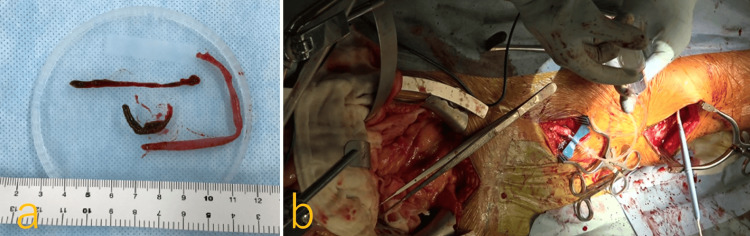 Figure 5
Figure 5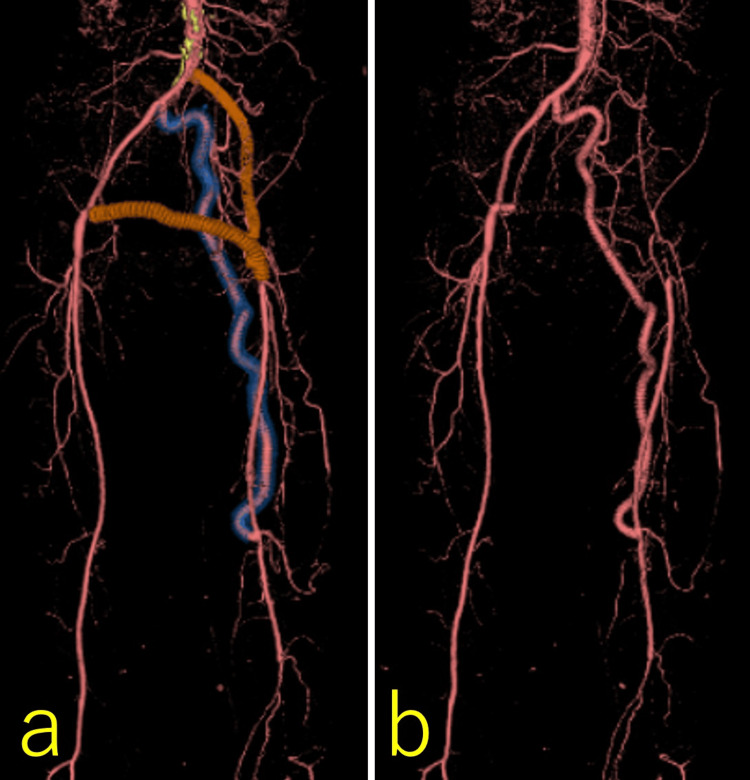 Figure 6
Figure 6| Data | Preoperative findings | Intraoperative findings | Postoperative findings | |||
| One week later | 6 months later | 12 months later | ||||
| Age (years) | 61 | 62 | ||||
| Limb symptoms | Pain in the left first toe, which turned purple during soaking in the bathtub | None | None | None | ||
| Blood flow measurement using the Doppler method | Left CFA | D-2, 49 cm/sec | ||||
| Left SFA | D-3 | 50 cm/sec | 44 cm/sec | 40 cm/sec | ||
| Left Pop. A | D-3, 13 cm/sec | D-2, 43 cm/sec | ||||
| Obturator foramen bypass | 220 mL/min PI 0.9 (TTFM) | Patent 50-119 cm/sec | Patent 32-160 cm/sec | Patent 39-150 cm/sec | ||
| ABI | Left | Unmeasurable | 0.84 | 0.78 | 0.84 | |
| Right | 1.17 | 1.1 | 1.12 | 1.1 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Peripheral Artery Disease Management · Vascular Procedures and Complications
Introduction
The common femoral artery (CFA) is located as shallow as 2-4 cm below the skin of the inguinal site. Repeated and additional prosthetic bypass to the femoral artery causes femoral crowding and adhesion and increases the risk of bypass infection. Prosthetic graft infections occur in 3.8% of bypass procedures involving the femoral artery during a mean follow-up period of 27 months [1].
Hip flexion can cause a CFA stenosis of more than 50% in patients with non-atheromatous disease [2]. The femoral crowding due to repeated prosthetic bypass procedures may cause the stenosis of native and prosthetic bypass during hip flexion.
An obturator foramen bypass is usually a bypass from a particular branch of the abdominal aorta to the lower limb artery to circumvent groin infection. This procedure is particularly effective in treating infected femoral prosthetic bypasses [3] and mycotic femoral artery aneurysms [4]; however, the bypass is routed through a narrow obturator foramen, which requires advanced technical skills. We describe a rare case of obturator foramen bypass for chronic limb-threatening ischemia (CLTI) induced by femoral crowding due to multiple prosthetic bypasses and hip flexion, using fluoroscopic guidance.
Case presentation
A 57-year-old Japanese man with hyperglycemia and hypertension underwent emergency percutaneous coronary intervention (PCI) for acute myocardial infarction of the right coronary artery. He had a 37-year smoking history of 20-40 cigarettes per day, and his father had a history of stroke. After the PCI, he was prescribed aspirin (100 mg) and prasugrel (3.75 mg); however, the drug-eluting stent was occluded four days later, necessitating another emergency PCI. During the hospitalization, the patient complained of three-year-longstanding intermittent claudication after walking 100 meters (Fontaine classification Stage Ⅱ b) [5]. Fontaine classification is staged from I to Ⅳ. Stage I is asymptomatic, meaning there are no symptoms despite the presence of arterial disease. Stage II is characterized by intermittent claudication and is divided into two subgroups: Stage IIa, where walking distance is greater than 200 meters (mild claudication), and Stage IIb, where walking distance is 200 meters or less (moderate to severe claudication). Stage III involves ischemic rest pain, indicating more advanced circulatory compromise. Stage IV represents the most severe stage and includes ulceration or gangrene, consistent with CLTI.
A contrast-enhanced CT scan revealed chronic total occlusion from the left common iliac artery (CIA) to CFA (Trans-Atlantic Inter-Society Consensus Class Ⅱ: D lesion). The CT also showed that collateral arteries that had developed on the left, including the lumbar arteries, inferior epigastric artery, and iliac circumflex artery, drained into the left CFA (Figure 1a). His left ankle brachial index (ABI: ankle systolic blood pressure/highest brachial systolic blood pressure [6]) was 0.52. There were no specific findings on blood thrombotic factors. Trousseau’s syndrome was suspected, and examinations of tumor markers, positron emission tomography, CT, and endoscopy were performed. However, no malignancies were observed.
Pre- and postoperative computed tomography (CT) findings of the prosthetic bypass between the terminal aorta and left common femoral artery (CFA)a: occlusion from the left common iliac artery to the CFA, and developed collateral arteries, including the left lumbar artery (purple arrow), inferior epigastric artery (blue arrow), and circumflex artery (orange arrow), which drained into the left CFA (yellow arrow); b: proximal anastomosis site of the prosthetic bypass between the terminal aorta and left CFA; c: distal anastomosis site of the prosthetic bypass between the terminal aorta and left CFA.
Four months after discharge, the patient (168.4 cm, 68.4 kg) was referred to our hospital for revascularization. The therapeutic lesion was as long as 32 cm, and the surgical procedure was preferable to endovascular therapy (EVT). Thrombectomy was performed from the left CFA to the superficial femoral artery (SFA), and prosthetic bypass grafting was performed between the terminal aorta (Figure 1b) and left CFA (Figure 1c) using an 8 mm Advanta VXT (Getinge, Gothenburg, Sweden) through the retroperitoneal space. On postoperative day (POD) 1, clopidogrel sulfate (75 mg), aspirin, and prasugrel were prescribed. The patient was discharged on POD 10. However, the CFA prosthetic bypass was occluded within two months postoperatively. We performed thrombectomy for the occluded bypass and EVT for the proximal anastomotic mild stenosis using an 8 mm Epic Vascular Stent (Boston Scientific, Massachusetts, USA); however, two hours after the procedure, the patient complained of sudden numbness and pain in the left leg, and echography revealed that the bypass was occluded again. Therefore, we performed emergent crossover prosthetic bypass grafting between the right external iliac artery (EIA) and left SFA using an 8 mm Fusion (Getinge, Gothenburg, Sweden) through the prevesical space (Figure 2).
Postoperative CT finding of an emergent crossover prosthetic bypassAn emergent crossover prosthetic bypass between the right EIA and left SFA was performed through the prevesical space. The black arrow is the previous 8 mm Epic Vascular Stent.EIA: external iliac artery; SFA: superficial femoral artery
Postoperative blood tests for thrombophilia indicated negative heparin-induced thrombocytopenia antibody and low plasminogen activity (43% (reference value, 71-128%)), which was considered complicated serological and vascular coagulopathy due to smoking and hyperglycemia. Hence, edoxaban tosilate hydrate (60 mg) was added to the patient’s medication regimen. The patient was discharged on POD 11.
Three years after the crossover bypass, at the age of 61 years, the patient experienced pain in the left first toe with purulent discharge (Fontaine classification Stage Ⅲ) and noticed that the toe turned purple when his left hip joint was flexed during soaking in the bathtub. The patient visited our hospital again. We could not palpate the left dorsalis pedis or the posterior tibial arteries. The left ABI of the patient could not be measured (Table 1).
Contrast-enhanced CT revealed that the crossover bypass was occluded, the left CFA and SFA appeared narrow and shaggy (Figures 3a, 3b), and the deep femoral artery (DFA) was patent. He was diagnosed with CLTI. Compression of the left CFA between the two occluded prosthetic bypasses and the caput femoris during hip flexion was considered to limit the blood flow to the lower limb. We were concerned that a new subcutaneous femoral bypass to the left CFA would be compromised by the dynamic femoral compression due to graft crowding during hip flexion. Therefore, we opted for obturator foramen crossover bypass grafting between the right CIA and left SFA. Preoperative blood examination revealed no specific abnormality.
Preoperative CT finding of obturator foramen crossover bypass graftinga: three-dimensional CT showing the two occluded prosthetic bypasses: the green arrow indicates a terminal aorta–left CFA bypass, whose distal anastomosis was detached, and the red arrow indicates a right EIA–left SFA crossover bypass, the blue arrow marks the inferior epigastric artery, the orange arrow indicates the iliac circumflex artery, and the yellow arrow identifies the CFA; b: the left CFA (yellow arrow) and SFA were narrow and shaggy, the CFA was suspected to be compressed between the two prosthetic bypasses (green and red arrows), the caput femoris when the hip joint was flexed, and the orange arrow indicates the iliac circumflex artery.EIA: external iliac artery; SFA: superficial femoral artery; CFA: common femoral artery
We performed an abdominal median incision, incised the retroperitoneum from the terminal aortic bifurcation to the outside of the sigmoid colon, and tunneled the sigmoid colon mesenterium. After identifying the bilateral obturator foramina lateral to the bladder, we incised the left middle thigh, released the Hunter canal, and exposed the narrow SFA. However, the tunneler could not communicate between the trans-abdominal retroperitoneal and post-adductor longus muscle pathways. Therefore, a left inguinal incision was made (Figure 4a) to obtain the post-sartorius muscle pathway. Although we could not initially pull through the obturator foramen, fluoroscopic guidance using Artis zeego (Siemens Healthineers, Erlangen, Germany) (Figure 4b) enabled us to obtain safe and successful tunneling through the obturator foramen from the inguinal site (Figure 4c). We then anastomosed an 8 mm PROPATEN (Gore, New Jersey, USA) 80 cm to the right CIA and tunneled it through the left obturator foramen via the retroperitoneal pathway (Figure 4d).
Intraoperative findings of obturator foramen crossover bypass grafting and thrombectomya: the tunneller could not communicate between the transabdominal retroperitoneal pathway and the post-adductor longus muscle pathway; therefore, we added a left inguinal incision; b: we could not pull through the obturator foramen and used live fluoroscopic guidance; c: fluoroscopic guidance enabled us to obtain safe and successful tunneling through the obturator foramen from the inguinal site; d: we anastomosed an 8-mm PROPATEN graft to the right common iliac artery and tunneled it through the left obturator foramen via the retroperitoneal pathway.
Additionally, we performed a thrombectomy for a 25-cm massive red thrombus that extended from the left CFA to the SFA (Figure 5a) to ensure as much blood flow as possible to the DFA and anastomosed the PROPATEN graft to the left SFA. Transit time flow measurements at the distal SFA (Figure 5b) indicated a flow rate of 220 mL/min (SFA reference value, 226.2 ± 82.1 mL/min [7], 93.6 ± 14.1 cm/sec [8]) and a pulsatile index of 0.9 (Table 1).
Intraoperative findings of obturator foramen crossover bypass grafting and thrombectomya: 25-centimeter massive thrombus was removed from the left CFA to SFA; b: prostaglandin was injected from the prosthetic bypass graft, and blood flow measured at the distal SFA was 220 mL/min with a PI of 0.9.CFA: common femoral artery; SFA: superficial femoral artery
The patient’s postoperative course was uneventful, and contrast-enhanced CT on POD 6 confirmed good patency of the obturator foramen crossover bypass (Figure 6). His left ABI improved to 0.84. He was discharged on POD 15. The graft surveillance was performed every six months by ultrasonography. The graft remained patent over 12 months postoperatively (Table 1).
Postoperative findings of obturator foramen crossover bypass grafting and thrombectomya: contrast-enhanced three-dimensional CT showing the previously implanted grafts, demonstrating good patency of the obturator foramen crossover bypass; b: contrast-enhanced three-dimensional CT without visualization of the previously implanted grafts.
Discussion
Shaw and Baue first reported the obturator foramen bypass in 1963 [9]. Although this technique is considered "extra-anatomical," it offers a shorter and straighter route compared to the subcutaneous pathway, which contributes to longer-term graft patency. Sautner reported that the primary patency rate of obturator foramen prosthetic bypass was 75% at one year and 54% at five years [10]. Similarly, Masaki noted patency rates of 69% at three years and 43% at five years for prosthetic bypasses [11]. Although an autologous vein graft provides longer patency, the saphenous veins were as narrow as 1 mm at the knees, and they were not suitable as a bypass graft in our case.
Obturator foramen bypass performed to avoid physical compression is rare, and this is the first such report to our knowledge. We also considered a redo femoral-femoral crossover bypass and left axillofemoral bypass; however, these options require a bypass to route the subcutaneous pathway and cross the hip joint. As such, they would be more susceptible to surgical site infections and compression during hip flexion, which is why they were discontinued. Surgical removal of the previously implanted grafts was not a therapeutic consideration due to the strong adhesion of the bypass graft, either.
Obturator foramen bypass requires surgeons to work in a confined space within the pelvic floor. Therefore, care must be taken not to injure the bladder, ureter, obturator artery, or vein during tunneling. Magishi reported a case in which an obturator foramen crossover prosthetic bypass penetrated the bladder [12]. In our case, we were able to identify both obturator foramina on the pelvic floor; however, we could not clearly locate the obturator artery and vein. Passing the graft through the narrow obturator foramen is technically challenging [13]. We initially advanced a tunneler bluntly, but the tip veered off course beneath the ischium and strayed under the adductor magnus, which is why the transabdominal and inguinal pathways did not communicate. Live fluoroscopic guidance using Artis zeego from multiple angles is helpful for confirming the correct passage of the tunnel through the obturator foramen [13]. The most important consideration when passing through the obturator foramen is bleeding due to vascular injury. The obturator artery and vein route at the upper medial position of the obturator foramen [14], and penetrating the obturator foramen should be performed at the center or lower position. Preoperative vascular assessment of the foramen ovale on CT is also important.
Conclusions
Obturator foramen bypass may be considered an option not only in avoiding inguinal infections but also in addressing femoral crowding and compression caused by hip flexion. Penetrating the obturator foramen should be performed at the center or lower position. Preoperative vascular assessment of the foramen ovale on CT is also important. The procedure can be safely performed under live fluoroscopic guidance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prosthetic graft infections involving the femoral artery J Vasc Surg Siracuse JJ Nandivada P Giles KA 700705572013 http://Siracuse JJ, Nandivada P, Giles KA, Hamdan AD, Wyers MC, Chaikof EL, Pomposelli FB, Schermerhorn ML. Prosthetic graft infections involving the femoral artery. J Vasc Surg. 2013 Mar;57(3):700-5.2331294010.1016/j.jvs.2012.09.049PMC 3587316 · doi ↗ · pubmed ↗
- 2Common femoral artery curvature during hip flexion Cardiovasc Intervent Radiol Tresson P Hublet A Holdner A Bordet M Millon A Papillard M Rouviere O 8448514620233731184310.1007/s 00270-023-03479-x · doi ↗ · pubmed ↗
- 3Obturator bypass in the treatment of prosthetic graft infection: classic but still effective Turk Gogus Kalp Damar Cerrahisi Derg Altun G Pulathan Z Hemsinli D 4804832620183208278410.5606/tgkdc.dergisi.2018.15744 PMC 7018284 · doi ↗ · pubmed ↗
- 4Obturator bypass for mycotic aneurysm in the drug addict Arch Surg Fromm SH Lucas CE 82831001970546689810.1001/archsurg.1970.01340190084019 · doi ↗ · pubmed ↗
- 5Surgical treatment of peripheral circulation disorders (Article in German)Helv Chir Acta Fontaine R Kim M Kieny R 499533211954 https://pubmed.ncbi.nlm.nih.gov/14366554/14366554 · pubmed ↗
- 6Critical review of the ankle brachial index Curr Cardiol Rev Khan TH Farooqui FA Niazi K 101106420081993628410.2174/157340308784245810 PMC 2779349 · doi ↗ · pubmed ↗
- 7Doppler ultrasound measurement of blood circulation in the lower extremity of man. I. Normal values at rest and changes in trauma and vascular diseases (Article in German)Langenbecks Arch Chir Nutz V Peschen M 3683713771992147986110.1007/BF 00574776 · doi ↗ · pubmed ↗
- 8Duplex Scanning for the Evaluation of Lower Limb Arterial Disease: Noninvasive Diagnostic Techniques in Vascular Disease Jager KA Ricketts HJ Strandness DE Jr. St. Louis Mosby 1985