Empowering informal caregivers of people living with dementia and enhancing digital health literacy through an extended digital intervention of the WHO iSupport manual: protocol for the project iDEM-Support
Nora Berner, Theresa Sophie Busse, Jan P. Ehlers, Franziska Anushi Jagoda, Amelie Meibeck, Ina Carola Otte, Julia Nitsche

TL;DR
This project adapts the WHO's iSupport platform for German caregivers of dementia patients and adds a module to improve digital health literacy.
Contribution
The study introduces a culturally adapted German version of iSupport with a new digital health literacy module.
Findings
The iDEM-Support project translates and adapts the iSupport platform for the German context.
A DHL module is developed to improve digital health literacy among informal caregivers.
The platform will be evaluated in a randomized controlled study.
Abstract
Informal caregivers of people living with dementia (PlwD) play a central role in home-based care. They are often exposed to emotional, physical, and organizational burdens, which increases their risk of psychological stress. Digital interventions have shown promise in supporting this target group. The WHO’s iSupport program offers a digital training platform for informal caregivers of PlwD; however, it has not yet been translated or adapted for the German healthcare context. Furthermore, deficits in digital health literacy (DHL) present a barrier to the use of digital health services. The iDEM-Support project aims to translate the platform iSupport into German, culturally adapt it, and develop a module to promote DHL. Using a mixed-methods design, informal caregivers and experts are involved in a participatory manner to enable user-centered development of both the platform and the DHL…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
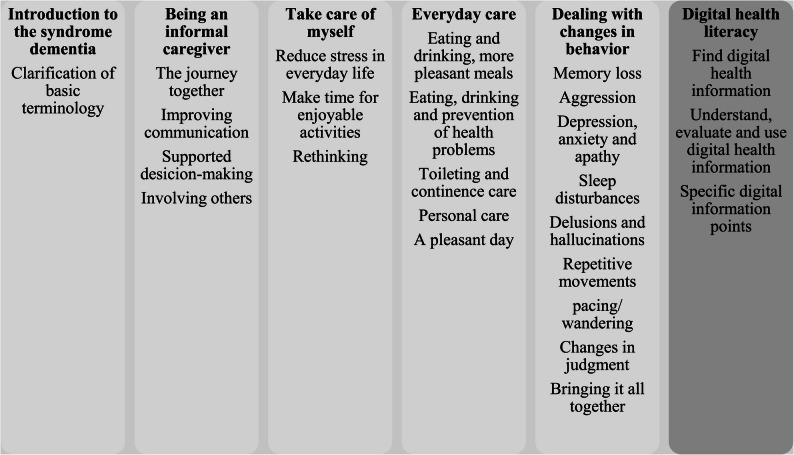 Figure 1
Figure 1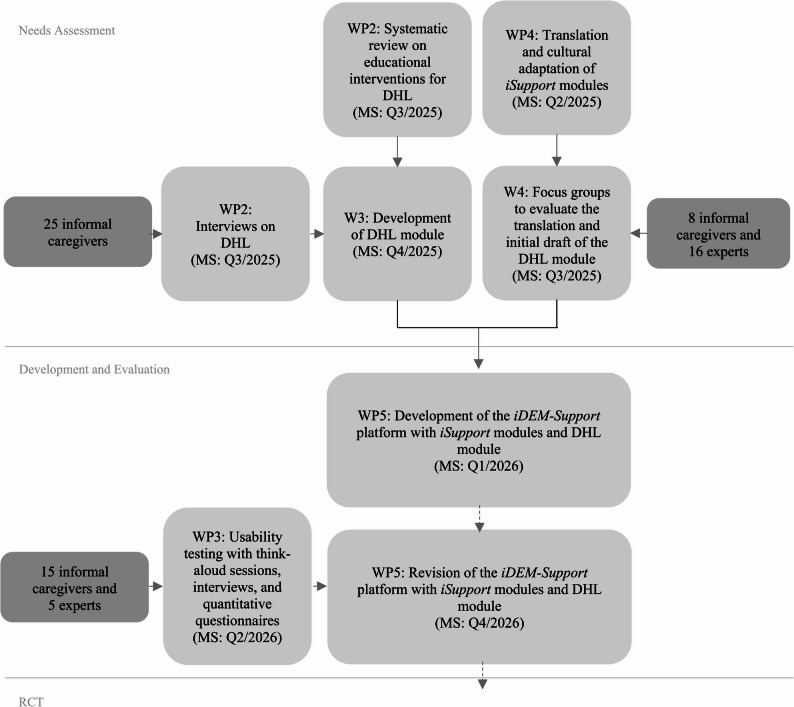 Figure 2
Figure 2- —Private Universität Witten/Herdecke gGmbH (3128)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Literacy and Information Accessibility · Technology Use by Older Adults · Dementia and Cognitive Impairment Research
Background
In light of ongoing demographic shifts, which according to the Federal Statistical Office of Germany is characterized by a continuous rise in the population aged 67 and older [1], the prevalence of age-related illnesses – particularly dementia – is steadily increasing. Dementia currently represents the most common chronic syndrome among older adults: Worldwide, the estimated number of people living with dementia (PlwD) is around 55 million [2, 3]. In Germany, it is estimated that 1.8 million people live with dementia [4, 5]. Globally, approximately 84% of PlwD live at home and depend on support and care by unpaid informal caregivers – typically family members, friends, or other close individuals [6, 7].
At the same time, informal caregivers of PlwD frequently bear the full responsibility for care over extended periods – often spanning several years – while being exposed to a multitude of stressors, including financial difficulties, time pressure, and complex challenges in care management [2]. Empirical studies consistently show that informal caregivers of PlwD experience considerable substantial physical and psychological strain [8–10]. Compared to the general population, they face an elevated risk of developing mental health conditions such as depression and anxiety, as well as somatic illnesses including hypertension, gastrointestinal disturbances, and respiratory problems [11]. Moreover, informal caregivers of PlwD are themselves often of advanced age (frequently spouses) and therefore more likely to experience age-related health problems and multimorbidity [12]. This dual burden of managing their own chronic conditions while providing demanding long-term care further exacerbates psychological and physical strain and increases the risk of care-related overload [13].
When informal caregivers are no longer able to fulfill this role – due to excessive burden, exhaustion/burnout, or caregiving-related mental or physical health problems – the consequences for PlwD are often profound, particularly regarding to autonomy and the ability to remain in their preferred living environment. Chronic stress and burden can undermine the stability of a home care arrangement [14]. When the care situation becomes unsustainable, moving to institutional care is often considered. However, such a decision is not solely a consequence of the behavior of informal caregivers or potential conflicts [15], but rather, it is deeply connected to the overall fragility of the care network [13]. It is important to mention that relocating to a care home can also be distressing for PlwD. This transition, which involves an unfamiliar environment and the loss of familiar routines, can lead to a worsening of dementia-related symptoms such as anxiety, and decline in cognition and psychological well-being. This highlights the need to empower informal caregivers, as they play a central role in shaping both the daily lives and care trajectories of PlwD, and frequently act as their primary decision-makers. Supporting informal caregivers with adequate resources and interventions is essential to maintaining stable home care arrangements, delaying or preventing premature institutionalization, and improving the quality of life for both informal caregivers and PlwD. These findings underscore the urgent need for accessible and effective support interventions tailored to the needs of informal caregivers.
Digital educational interventions and programs [16] offer promising potential to empower informal caregivers: they can be accessed irrespective of location and time, are potentially scalable, and have demonstrated cost-effectiveness [17]. Over the past decade, interest in internet-based information and communication technologies for PlwD and their informal caregivers – including online training and support programs – has grown substantially [18]. National and international studies demonstrate that digital and face-to-face interventions have equivalent effects on informal caregivers’ emotional well-being, stress, and caregiver burden [19], risk of developing mental health disorders, and symptoms of anxiety and depression [20]. Moreover, informal caregivers report a reduction in feelings of being overwhelmed [20] and increased self-efficacy and confidence in caregiving tasks [15]. Digital formats also eliminate barriers such as long travel distances, limited professional resources, and concerns about stigma. In addition, they offer flexible access independent of time and location, allowing users to engage with content at their own pace and convenience. This reduces scheduling pressure, eliminates the need to arrange alternative care, and enables participation in familiar environments.
However, the mere availability of digital offerings does not suffice to engage target populations effectively. In Germany, significant deficits persist in the handling and utilization of digital health information [21]. There remain major societal challenges regarding digital health literacy (DHL): 75.8% of the German population exhibit low DHL (self-evaluation) [18]. DHL is defined as the ability to find, understand, evaluate, and apply relevant health information in digital environments [22] and is composed of traditional literacy, information literacy, scientific literacy and media literacy, computer and health literacy [23, 24].
In Germany individuals with lower DHL use digital health resources significantly less often [18] and are at risk of misinterpreting or being unable to verify the validity of health information obtained online. Previous studies and national health literacy surveys have shown that improving DHL is a significant challenge, and that it contributes to overall health literacy [18, 25, 26]. These findings highlight the need for promotion and training to encourage the competent use of digital health information. Furthermore, recent reviews have shown that informal caregivers, in particular, demonstrate high acceptance of digital interventions [27].
Against this background, the World Health Organization (2019) developed the digital training and support manual iSupport [2]. This generic, English-language intervention provides guided education, skills training, and social support to informal caregivers of PlwD, who experience stress, burden, and mild to moderate symptoms of depression or anxiety. This intervention empowers them to manage the care situation [17]. To ensure worldwide accessibility, iSupport must (1) be translated into the specific national language – given that many informal caregivers are older and may not speak English – and (2) undergo cultural adaptation to the local implementation context – to tailor content, examples, and values to the realities, needs, and expectations of informal caregivers. This process, guided by the WHO’s adaptation framework [2], has been completed and positively evaluated in randomized controlled trials in Portugal [28], India [29], the Netherlands [30], Greece [31], Spain [32], and Australia [33]. Although a German-language platform has already been implemented in Switzerland [34], a corresponding translation and cultural adaptation has not yet been realized in Germany.
While existing implementation research on iSupport has demonstrated positive effects, studies have also identified several barriers for its use, including lack of mobile accessibility, insufficient content personalization, limited moderation, and scarce peer exchange opportunities [28, 30, 33]. Low awareness of digital interventions [29] and low DHL further exacerbate these challenges and require targeted addressing. The project systematically addresses these findings.
Study aim
The iDEM-Support project aims to translate the WHO’s iSupport into German and adapt it to the German healthcare context, implementing it as a digital learning platform – web-based, responsive and user-friendly. The translation is based on the existing German-language version of iSupport, which was developed for Switzerland [34], rather than translating the original English version. Although this version provides a high-quality linguistic foundation, it cannot be transferred unchanged to other German-speaking contexts. Despite the common language, there are relevant differences in terminology and usage, as well as differences in the healthcare system, legal framework, and available support services. Consequently, the Swiss version incorporates context-specific cultural references that may not be comprehensible or relevant to users residing in Germany. To ensure clarity, cultural relevance, and practical applicability for informal caregivers in Germany, the content will be systematically adapted both linguistically and culturally, including specific information and examples related to the healthcare system.
The manual will be expanded to include a module on DHL tailored to the needs of informal caregivers of PlwD, as well as an interactive feature to facilitate interaction among informal caregivers and other users (Fig. 1).
Fig. 1. Content of the iSupport Deutschland platform (own representation). The figure illustrates the structure and thematic modules of the iSupport Deutschland platform. Modules 1–5 correspond to the core content of iSupport, module 6 introduces DHL, aimed at enabling informal caregivers PlwD to find, understand, evaluate, and apply health information digitally. The platform is web-based, responsive, and user-friendly, and includes interactive features, and learning objectives
The module on DHL is developed using a theory- and empirical-informed approach. It is grounded in an established conceptual model by Milanti et al. [35], who conceptualize DHL as a meta-competence that encompasses functional, interactive, and critical competencies required to effectively engage with digital health information and services. This theoretical framework provides a robust foundation for the systematic development, operationalization, and evaluation of learning content within digital health interventions. In addition to this theoretical framework, the development of the DHL module is informed by the findings of a systematic review (carried out during the course of the project) as well as by results from preceding empirical data collection, including qualitative interviews and focus group discussions with relevant stakeholders.
Building on this combined theoretical and empirical foundation, the module on DHL is designed to provide both foundational knowledge and practical guidance for effectively searching, understanding, evaluating, and applying health-related information in digital contexts. Specially, the module seeks to ensure that users know where and how to find reliable health information online, how to assess the quality and trustworthiness of digital health information, and how to use this information to make informed decisions appropriate to their individual life situations or to seek adequate support [23, 36]. The individual DHL components defined by the model of Milanti et al. [35] are systematically linked to specific learning objectives and interactive tasks. Depending on user needs, preferences and current behaviors in searching for health-related information via digital media, the module may include task-based learning activities that require the use of digital tools to promote engagement and competency development.
Furthermore, particular emphasis will be placed on ensuring conceptual alignment with the existing iSupport content whereby interactivity and usability are particularly important. We refer to the resulting platform below as the iSupport Deutschland platform, which can be seen as a further development of iSupport.
The iSupport Deutschland platform is designed to reduce psychological stress among informal caregivers and to improve their quality of life. The development therefore focusses on usability, instructional design, participation, the enhancement of DHL, and social networking, based on findings from previous studies in other countries [28–30, 33]. This will be followed by a proof-of-concept in a randomized controlled trial (RCT). If the proof of concept is successful, the iSupport Deutschland platform will be docked onto existing networks (e.g. Last Aid Germany gGmbH) and made permanently accessible as permanent links and applications on the websites of interest groups (e.g. German Alzheimer Society e.V., We care – Interest group and self-help group for family caregivers e.V. (Wir pflegen NRW e.V.), and Last Aid Germany gGmbH).
This study protocol describes the planned work packages for translation, cultural adaptation, identification of needs and current behavior for searching for information online, development and piloting of the new module on DHL and the platform. The RCT will be reported separately in an independent study protocol.
The project aims to achieve the following specific objectives:
- To identify what needs informal caregivers have when searching for health-related information regarding care for PlwD online.
- To determine how a digital intervention to support informal caregivers of PlwD regarding informal care and DHL should look and function technically so that it is accessible to all users.
- To develop a structured module for improving DHL, guided by the theoretical framework of Milanti et al. [35], including relevant content and instructional design, so that informal caregivers of PlwD can improve their own DHL by working through the module.
Methods
Study design
The research design of iDEM-Support follows a mixed-methods approach that integrates both qualitative and quantitative methods to address the study aims comprehensively. The usability (including accessibility) of both the DHL module and the overall platform will be systematically assessed. Central to the methodological framework is the continuous involvement of prospective users, which ensures that the ongoing development of the platform remains closely aligned with the specific needs and expectations of the target group. The sample size was guided by practical considerations, including expected recruitment feasibility within the study period, resource availability, and alignment with comparable feasibility and pilot studies in the field. However, the respective data collections are always considered in relation to data saturation, and appropriate adjustments are made to the sample size if necessary to ensure data saturation and diversity of perspectives.
The project proceeds in several interrelated steps (Fig. 2):
- A systematic review will be conducted to identify the facilitating and hindering factors of digital educational interventions aimed at improving DHL among informal caregivers aged 18 years (age of majority in Germany) or older and older adults aged 65 years or above. The review question is structured according to the PICO framework, with informal caregivers and older adults as the population, digital educational interventions focusing on the enhancement of DHL as the intervention, no mandatory comparison group, and improvement in DHL as the primary outcome. People aged 65 and older were included because 65 traditionally marks the onset of retirement in Germany and remains a recognized legal and political threshold for older adulthood. Although the statutory retirement age is shifting toward 67, including individuals from age 65 ensures that relevant age-related changes are appropriately represented. Informal caregivers and older adults, often less familiar with digital technologies may also benefit from such interventions, but the primary focus is to understand how to best support informal caregivers and older adults in improving their DHL. Eligible interventions include web-based educational programs and mobile health applications designed to improving DHL. Interventional studies, as well as systematic reviews and meta-analyses, published in peer-reviewed scientific journals will be included. Only studies available in full text and published in German or English will be considered.
- Qualitative semi-structured interviews with informal caregivers of PlwD will explore current behaviors and needs related to searching for health-related information in digital media. Participants’ DHL will also be assessed using the GR-eHEALS [37]. The GR-eHEALS is the validated German version of the eHealth Literacy Scale (eHEALS) [38], a widely used 8-item self-report instrument assessing individuals’ perceived ability to find, understand, evaluate, and apply digital health information. It has been used and validated in German-speaking populations, including older adults. In the iDEM**-**Support project, the GR-eHEALS will initially be used to assess baseline DHL and describe the study population. The measure will be re-administered following the intervention phases (Think-Aloud sessions and RTC), enabling the examination of potential improvements in DHL associated with use of the platform. Its focus on core DHL competencies directly aligns with the aims of the study and the learning objectives of the DHL module.
- The translation and cultural adaptation of the iSupport modules as well as the initial draft of the DHL-module will be evaluated in focus groups with informal caregivers and experts. The aim is to ensure content accuracy, clarity, and usability based on user expectations and preferences.
- The DHL module will be designed regarding content and functionality, based on the insights from the systematic review as well as findings from the semi-structured interviews and focus group discussions. These preparatory studies identified key challenges, needs, and contextual factors in the use of digital health information, ensuring that the module is evidence-based and closely aligned with the experiences and informational needs of the target population. Its instructional design is informed by the theoretical framework of Milanti et al. [35], current scientific evidence on effective didactical strategies, usability research, and content-specific findings in the field of DHL.
- Think-aloud sessions with informal caregivers of PlwD and experts will assess usability-related challenges and inform participatory design. These includes (1) cognitive walkthroughs to document user interactions and thought processes, (2) post-session interviews for user reflection, and (3) standardized questionnaires – including the System Usability Scale (SUS) [39], the short version of the User Experience Questionnaire (UEQ-S) [40], and the GR-eHEALS [37] – to evaluate accessibility, usability, user experience, and DHL quantitatively.
Fig. 2. Applied steps in the iDEM-Support project (own representation). The figure shows the sequential work packages (WPs) and milestones (MSs) of the iDEM-Support project across the phases of needs assessment, development and evaluation, and preparation for a RCT. This process includes a systematic review, qualitative interviews and focus groups, development and cultural adaptation of the iSupport modules including a DHL module, platform development, and iterative usability testing. Milestones are indicated by target quarters (Q). WP = work package; MS = milestone; Q = quarter
Participants
Informal caregivers of PlwD and experts are the study participants in the various data collections. Family members, partners, friends, neighbors or other close individuals are included as informal caregivers who provide unpaid, home-based care and support for a PlwD. This includes assistance with daily living activities, emotional support, coordination of care, and navigating health-related information and services. Experts in this context are individuals who have extensive experience with the perspectives of informal caregivers of PlwD and their situation – either from the perspective of self-help groups, associations, or professional expertise in research and care. Participants must be over 18 years of age, with all genders being considered. Only individuals who possess sufficient proficiency in the German language will be included. A diagnosed psychiatric disorder will serve as an exclusion criterion.
The samples and sample sizes in relation to the form of data collection are listed below:
- A total of 25 semi-structured interviews will be conducted with informal caregivers of PlwD, focusing on the topic of DHL.
- Three focus group discussions will be conducted to evaluate the translation and cultural adaptation of the iSupport modules. One group will include eight informal caregivers of PlwD, while two additional groups will each include eight experts. Informal caregivers and experts will participate in separate focus groups. This is to promote open and unbiased discussions. It is also to minimize potential hierarchically driven inhibitions.
- The think-aloud sessions to pilot the platform will be conducted with 15 informal caregivers of PlwD and five experts. The group of informal caregivers is divided into three subgroups: approximately five informal caregivers with high DHL, five with moderate DHL, and five with low DHL. Participant classification will be based on results obtained using the GR-eHEALS [37].
Participants will be recruited using a combination of digital and analogue recruitment approaches to enhance the inclusion of informal caregivers with varying levels of DHL. In addition to online recruitment via social media channels, newsletters, and official communications of the Department of Health Services Research at Ruhr University Bochum, the German Alzheimer Society e.V., We care – Interest group and self-help group for family caregivers e.V. (Wir pflegen NRW e.V.), and Last Aid Germany gGmbH, analogue recruitment pathways will be deliberately intensified. Printed project flyers and calls for participation will be disseminated through the affiliated member societies, which will be explicitly asked to approach potential participants directly. Snowball sampling will be strategically employed to specifically reach informal caregivers with lower DHL. Participating caregivers with higher DHL will be encouraged to share study information within their personal offline networks (e.g., self-help groups, caregiver support groups, dementia cafés), thereby facilitating access to caregivers with lower digital affinity. Additionally, a press release issued by Ruhr University Bochum was disseminated via regional media outlets. In particular, radio dissemination proved to be a relevant channel for reaching informal caregivers with limited digital engagement. Furthermore, the dissemination of study information by the technical product developer Ergosign GmbH enables access to individuals outside of traditional care-specific networks.
Overall, the combined recruitment strategy aims to mitigate recruitment bias toward informal caregivers with higher DHL and to improve the representation of informal caregivers with lower DHL, while ensuring a diverse study sample. Sample diversity will be actively promoted through the targeted recruitment of informal caregivers with varying sociodemographic backgrounds, genders, caregiving contexts, and levels of DHL. The key characteristics will be systematically assessed using validated questionnaire measures. This approach enables a transparent description of the achieved sample, a critical reflection on potential selection effects, and the ongoing monitoring of sample composition, allowing recruitment strategies to be adjusted if necessary to enhance diversity.
Data collection
As part of the recruitment process, a contact list will be compiled containing basic contact information (name, address, email address, telephone number). This data will be collected via a contact form completed by prospective informal caregivers and experts during initial outreach. The completed forms will be returned to the research team by post or via e-mail. Prior to this, verbal consent will be obtained regarding data storage and inclusion in the contact list. For better understanding and traceability, data collection is structured according to the three interrelated steps:
- Interviews: In advance, sociodemographic data will be collected using a standardized paper-based questionnaire. Additionally, the GR-eHEALS [37] will be surveyed. The interview guides will be developed by the authors based on existing models of DHL and research findings on DHL. Following a narrative stimulus regarding the caregiving situation (“Please tell us about the care situation with your family member with dementia.”), the interview will first focus on participants’ experiences with digital health services (e.g. “Please tell us about a situation in which you experienced challenges when searching for health and/or care-related topics on the Internet.”). It will then explore their needs and expectations in the context of DHL (e.g. “What should a website look like or what should it contain to make it easily accessible and easy to use for you?”). Particular attention will be given to the technical features and devices participants use to access digital services (e.g. “Which digital devices (e.g., PC, tablet, smartphone) do you use, and which form of media (e.g., video, podcast, text) do you prefer?”). In addition, participants will be asked about their personal needs and preferences in engaging with the digital platform (e.g. “If a digital platform like the one we're planning enables communication with other informal caregivers, what form would be most helpful to you?“). Data collection is scheduled for summer 2025. Interviews will last approximately 45 to 60 minutes and will be conducted according to participants’ preferences – either in person, via Zoom, or by telephone. Remote sessions will be conducted using end-to-end encrypted Zoom connections, without using the platform's built-in recording function. All interviews will be audio-recorded using an external recording device. Transcription will be carried out by a transcription agency.
- Focus group discussions: The authors will develop the discussion guide for the evaluation in focus group discussions based on the experiences in the cultural adaptation and translation process. In the focus groups, participants will discuss the linguistic design and comprehensibility of the information (e.g. “How would you assess the terms and phrases used in terms of dementia-sensitive language?”), as well as critical passages from the cultural adaptation (e.g. “How would you assess the description of the types of dementia in terms of their precision and current status?”), the first draft of the DHL module (e.g. “What additional content would you like to see in this module?”), and possible designs for the interactive elements and implementations of previously text-based content in more appealing didactic formats (e.g. “How useful and relevant to everyday life did you find the examples and quiz questions?”). Data collection is scheduled for summer 2025. Each focus group will last approximately 60 to 90 minutes. The focus groups will be conducted at Ruhr University Bochum and will be audio-recorded using an external recording device.
- Think-aloud sessions: The think-aloud sessions will be conducted to assess the usability (including accessibility) of the iSupport Deutschland platform by capturing participants’ cognitive and behavioral responses during task-based interactions. In advance, sociodemographic data (e.g., year of birth, gender, occupation) will be collected using a standardized paper-based questionnaire. Informal caregivers will also complete the German version of GR-eHEALS [37] in this context. The sociodemographic questionnaire and GR-eHEALS will be administered in paper format. Participants will then be asked to verbalize their thoughts in a cognitive walkthrough while completing structured tasks designed to reflect typical usage scenarios and to uncover potential usability barriers. Verbalizations, gestures, facial expressions, and system interactions will be documented. Immediately following each cognitive walkthrough, a post-session interview will be conducted using a semi-structured interview guide. Interviews will be audio-recorded using an external recording device. After the post-session interviews, participants will be asked to complete the SUS [39] and the short version of the user experience questionnaire (UEQ-S) [40]. Participants may complete the questionnaires either independently or together with the researcher, depending on their preference. All completed questionnaires will be collected immediately following the post-session interview. For remote interviews, the questionnaires will be sent and returned by post. Data collection is scheduled for spring 2026. Each session will last approximately 60 min and will be conducted either in person or remotely via Zoom, depending on participant preference. Remote sessions will use end-to-end encrypted Zoom connections (without using the platform’s built-in recording function), with screen recordings captured locally on the researcher’s computer using the open-source software OBS Studio [41]. In all sessions, verbalizations and user interactions will be audio-recorded using an external recording device.
Data handling
The contact details are only collected and stored for the purpose of contacting the study participants and for the payment of the expense allowance within the described project and within the described project duration.
Video and audio files as well as the data sets of the socio-demographic data and questionnaires of the informal caregivers and experts are pseudonymized so that an assignment to the contact data is no longer possible without the use of a coding list. The original documents of the questionnaires will be stored in a locked cabinet after digitization (scans) and pseudonymization until the end of the project. An external provider will transcribe the audio data verbatim. The transcribed and pseudonymized data will be organized using MAXQDA software [42] for qualitative analysis. The software IBM SPSS Statistics [36] will be used to analyze the quantitative data.
Data analysis
The pseudonymized transcripts and screen recordings from the interviews, focus group discussions, and think-aloud sessions will be analyzed using a structuring content analysis [43]. Qualitative content analysis is the appropriate approach for the analysis of communicative content in a rule-based manner. An inductive-deductive approach is employed to explore the unknown field of research, while existing assumptions are examined on a case-by-case basis. The coding of the respective data will be carried out by two coders to ensure reliability, collegial validation, and intersubjective traceability.
The usability tests will be analyzed with the aim of capturing participants’ cognitive and emotional responses to the interaction design, content, and visual-aesthetic layout of the iDEM-Support platform. Quantitative data from the SUS, UEQ-S, and GR-eHEALS will be analyzed using descriptive statistics to characterize usability, user experience, and digital health literacy within the study sample. No inferential or subgroup analyses are planned.
Ethics and consent to participate
Ethical approval for the study was obtained from the Ethics Committee of the Ruhr University Bochum, based in Bad Oeynhausen, Germany, in 2025 (Nr. 2025 − 1343).
Participation in the study requires written informed consent. In accordance with the principle of ongoing consent, participants are reminded during the study that their participation is voluntary. They can withdraw their consent at any time without giving reasons and without any disadvantages. While the study topics are not expected to pose inherent risks, participants may disclose sensitive information, potentially causing temporary emotional strain. Safeguarding measures will be implemented, and contact information for follow-up support will be provided. The study team will monitor adverse events continuously, with early termination considered if risks are higher than anticipated. Overall, anticipated risks are minimal and limited to short-term emotional reactions during the data collection, with no expected medium- or long-term burdens.
Discussion
iDEM-Support will represent the first implementation of the WHO iSupport program in a German-language version tailored to the specific needs of informal caregivers of PlwD in Germany. The iSupport Deutschland platform will be a further refinement of iSupport by incorporating interactive features and a module on DHL, thereby enhancing its potential to empower informal caregivers. The study design reflects lessons learned from prior implementations in other countries [28–30, 33] and is shaped by a participatory development approach to ensure alignment with the target group’s needs and preferences.
The iSupport platform has demonstrated positive effects in previous studies, including improvements in emotional well-being, reductions in stress and burden, and a decreased risk of mental health problems among informal caregivers of PlwD [19, 20]. iDEM-Support aims to expand these outcomes through additional interactive and peer-exchange components. The platform’s digital nature ensures location-independent access, which is an important advantage for this target group. This aligns with the result of Etxeberria’s et al. (2021) study, which showed a high acceptance of digital interventions among informal caregivers [27]. A particular innovation of iDEM-Support is the development of a DHL module, enabling informal caregivers to find, understand, evaluate, and apply digital health information. Informed by established instructional design principles and evidence from the fields of health literacy and digital education, the module supports both knowledge acquisition and self-efficacy. Importantly, the module’s scope extends beyond dementia-specific content and caregiving roles, offering broader utility for patients in earlier stages of dementia and informal caregivers as well as relatives without caregiver role or professional caregivers. This approach ensures a high degree of user-centeredness, aiming for strong usability and a positive user experience [44], which should also be enabled by accessibility. Thus, the expected improvements in DHL can be a valuable contribution to public health by fostering the competent use of digital health information – in particular by maintaining the digital infrastructure of the iSupport Deutschland platform beyond the study period and thus ensuring long-term availability. The insights gained may inform similar adaptations in other national contexts. To ensure visibility and uptake within the scientific community, scientific results will be disseminated through presentations at academic conferences and publications in national and international journals.
Despite its expected strengths, the project has certain limitations. The recruitment strategy may favor informal caregivers who are more open to digital formats, potentially underrepresenting those with lower DHL or a fundamental lack of digital access. Nonetheless, the project contributes essential insights into user-centered design and the development of scalable, accessible digital interventions for informal caregivers – especially within a healthcare landscape increasingly shaped by digital transformation. Valuable findings are also likely to emerge from the subsequent proof of concept in the RCT.
iDEM-Support aims to address the critical gap in (self-)support for informal caregivers of PlwD. Using digital technologies, the study will provide valuable insights into the effects of internet-based information and communication technologies for informal caregivers of PlwD, including online training and support programs. Thus, the platform offers a promising way to reduce the burden on informal caregivers, thereby delaying the institutionalization of PlwD and strengthening informal care structures in an evolving digital healthcare landscape.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Federal Statistical Office of Germany. Ergebnisse der 14. koordinierten Bevölkerungsvorausberechnung. 2019. www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Bevoelkerungsvorausberechnung/Tabellen/variante-1-2-3-altersgruppen.html. Accessed 16 Jun 2025.
- 2World Health Organization. i Support version 1.0. Adaptation and Implementation Guide. 2019. https://www.who.int/publications/i/item/9789241515863.
- 3Alzheimer’s Disease International. Dementia statistics. 2025. https://www.alzint.org/about/dementia-facts-figures/dementia-statistics/. Accessed 16 Jun 2025.
- 4Radtke R. Anzahl der Demenzkranken in Deutschland nach Alter und Geschlecht 2023. 2024. https://de.statista.com/statistik/daten/studie/246028/umfrage/anzahl-der-demenzkranken-in-deutschland-nach-alter-und-geschlecht/#statistic Container. Accessed 16 Jun 2025.
- 5Rummel B. System Usability Scale – jetzt auch auf Deutsch. 2016. https://blogs.sap.com/2016/02/01/system-usability-scale-jetzt-auch-auf-deutsch/.