Missing assent: a global systematic review of ethical practices in HIV research with men who have sex with men (MSM) under 18
Worawalan Waratworawan, T Charles Witzel, Sin How Lim, Thomas E. Guadamuz

TL;DR
This study reviews how ethical practices like informed assent are handled in HIV research involving young men who have sex with men under 18, finding significant gaps in proper procedures.
Contribution
The paper provides a global systematic review of ethical practices in HIV research with minors who have sex with men, highlighting underreported informed assent procedures.
Findings
Only 20% of studies included informed assent for minors.
Most studies were conducted in high-income countries, with no representation from low-income settings.
Only 7% of studies involved minors living with HIV.
Abstract
Ethical safeguards are critical in HIV research involving minors, especially vulnerable groups such as men who have sex with men (MSM) under 18 years. This systematic review explores how informed assent and consent practices are reported, guided by the 2016 Council for International Organizations of Medical Sciences (CIOMS) guidelines. A systematic review was conducted of peer-reviewed studies from 2010 to 2023 involving MSM under 18 years, using PubMed, Embase, and Scopus databases. Key ethical components were extracted and synthesized thematically. Of 410 articles screened, 65 met inclusion criteria. All included studies reported informed consent, but only 20% (n = 13) included informed assent. Most were conducted in high-income countries (64%), with no representation from low-income settings. Only 7% involved minors living with HIV. Quantitative methods were predominant (82%), and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
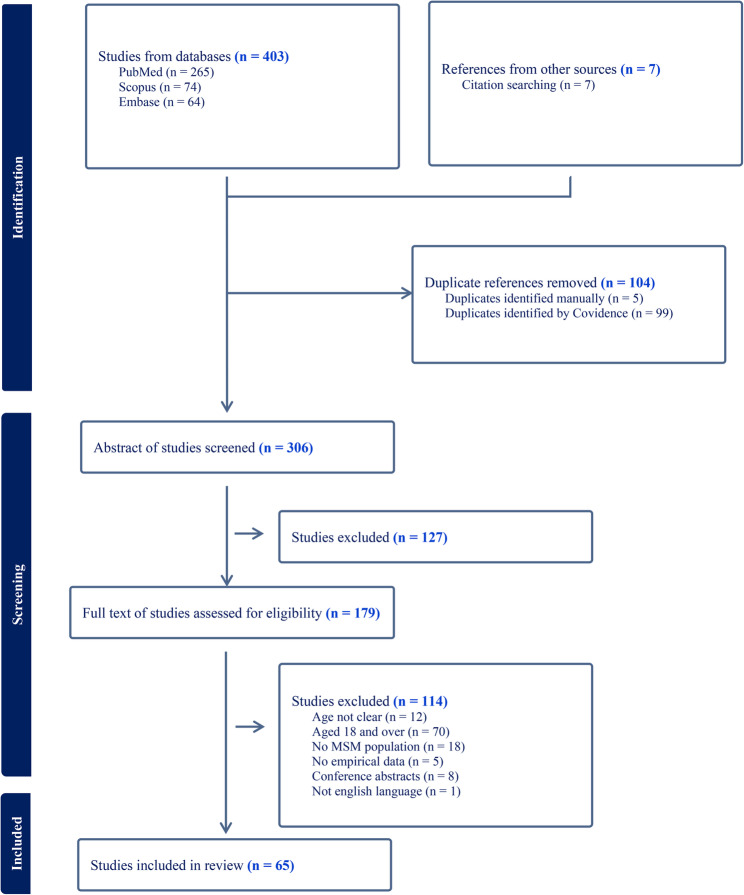 Figure 1
Figure 1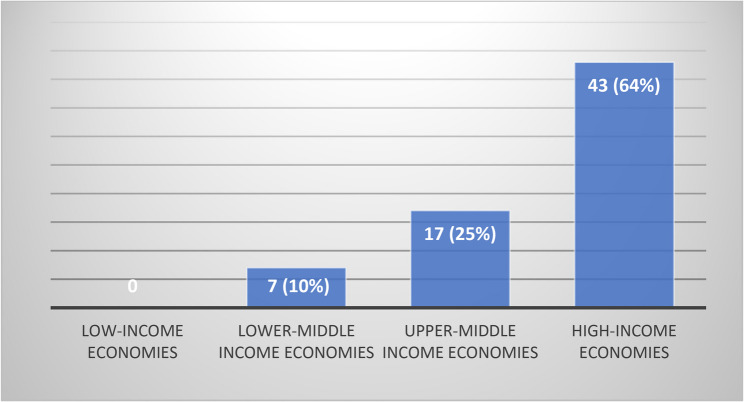 Figure 2
Figure 2- —Mahidol University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · Ethics in Clinical Research · HIV, Drug Use, Sexual Risk
Introduction
Despite progress in HIV treatment and prevention, the scale of the epidemic remained alarming. In 2023, approximately 9.3 million people were still living with HIV without access to treatment. Globally, around 630,000 people died of AIDS-related illnesses in that year alone, including 76,000 children under the age of 15, accounting for one in every eight AIDS-related deaths. HIV prevention efforts showed uneven progress. Key populations, such as men who have sex with men, transgender individuals, people who inject drugs, as well as youth, remained underserved in access to effective prevention services [1].
Given these ongoing challenges and disparities, HIV research continued to receive substantial funding support [2–6], recognizing that the epidemic required multidisciplinary responses and cross-sector collaboration. A large number of HIV studies were conducted using both observational and interventional methods [7, 8], exploring diverse areas such as HIV prevention [8, 9], HIV testing [10–13], care, and retention [14]. Much HIV research focused on key populations, including men who have sex with men (MSM), transgender women, people who use drugs, people in prisons and other closed settings [15–20], as well as migrant workers [21–23], people from minority ethnic backgrounds [24–26], and young people [27, 28].
Adolescents became a key target population in HIV interventions, particularly young MSM, who experienced overlapping vulnerabilities due to both their age and sexual orientation. Indeed, young MSM often faced complex social contexts, including stigma and discrimination, lack of family support, limited access to LGBTQ+-friendly healthcare services, and insufficient knowledge and skills related to HIV prevention. These challenges were compounded in countries where same-sex relationships were criminalized. For instance, as of 2022, 31 out of 54 African countries, including Nigeria, Uganda, and Malawi, still enforced laws against consensual same-sex acts, which further restricted access to HIV prevention and care services [29]. Such legal barriers contributed to broader obstacles in accessing preventive measures such as HIV pre-exposure prophylaxis (PrEP) and regular HIV testing. These challenges may be further amplified in low-income countries, where factors such as sociocultural stigma [30, 31], criminalization of same-sex relationships [29], and limited research infrastructure present substantial barriers to conducting ethical research involving MSM minors. The criminalization of homosexuality in many low-income settings [29] can heighten risks for both participants and researchers, potentially discouraging ethical review boards or institutions from approving such research. Moreover, restrictive legal environments may prohibit the enrollment of sexual minority minors without parental permission, even in contexts where such disclosure could place youth at risk. These factors may partly explain the absence of studies involving MSM minors in low-income settings. Within this context, research involving vulnerable populations such as young MSM had to prioritize ethical considerations, particularly with regard to protecting participants’ rights, safety, and well-being, which are core principles essential to conducting research responsibly and with integrity [30–32].
All ethically conducted research needed to protect participants from harm and had to outline how participants’ information would be safeguarded from improper use. In HIV research, this process had to be conducted with considerable sensitivity, since it dealt with an issue linked with experiences of stigma, discrimination, and potential mental health impacts, especially among MSM minors [33–36]. Therefore, the recruitment and enrollment process for research participants was critical, as these processes required a careful balance of risks and benefits, as well as the use of accessible language when describing project details. In many settings, researchers also had to ensure that their participants were of legal age to participate, especially MSM minors. Furthermore, when conducting research with MSM minors, participants needed to be given sufficient time to decide whether or not to take part. Sometimes, it was necessary to obtain parental consent, a waiver of parental permission, or even a proxy. Various consent options could be applied when conducting research with MSM minors, including parental or guardian consent, informed assent with parental permission, waivers, and proxy permission. Each of these approaches had different ethical and legal considerations, which had to be carefully evaluated based on the study context and jurisdiction (Table 1). These practices demonstrated the researchers’ care for the participants’ safety, while also ensuring that minors were protected and cared for while engaging in the study process without coercion.
Table 1. Types of assent/consent [38–42]Type of Assent/ConsentDefinitionStrengthsChallengesParental/guardian permissionRequires explicit permission from a parent or legal guardian before a minor can participateEnsures legal and ethical compliance; protects minors from potential risksMay discourage participation due to stigma, confidentiality concerns, or lack of parental/guardian supportInformed Assent + Parental permissionThe minor agrees to participate (assent), but legal authorization is still required from a parent/guardianGives minors a voice in decision-making; maintains legal protectionSimilar challenges as parental/guardian permission, including potential reluctance to disclose sensitive topics such as sexual identity, sexual activities, violence and substance useInformed Assent + Proxy PermissionThe minor agrees to participate (assent), and designated individual (not a parent/legal guardian) is authorized to provide permission on behalf of the minorProvides an alternative when parental permission is not feasible or appropriateMay raise ethical and legal concerns regarding who qualifies as a proxy and their decision-making power. Some IRB/ethics committees allow proxy permission instead of parental permission but still prioritize the protection of minors by requiring a responsible adult to assist in decision-makingInformed Assent + Waiver of Parental permissionThe minor agrees to participate (assent), and parental permission is waived by the ethics board when the research poses minimal or less than minimal risk and requiring parental permission may increase risk or harm to the minor. In some studies, additional supportive processes may be implemented—such as involving a minor advocate to help the minor make an informed decision about participationEmpowers minors, respects their autonomy, facilitates participation in sensitive research, and enhances confidentialityRequires institution oversight (IRB/ethics committee approval); may be contested for legal or ethical reasons. Typically allowed for low-risk studies or case-by-case in sensitive contexts (e.g., sexual identity, family violence)Emancipated or Mature Minor ConsentIn specific legal or ethical contexts, minors who are legally emancipated or deemed mature (e.g., married, parenting, homeless, or financially independent) may consent to participate in research without parental permissionRespects the legal and lived autonomy of minors who function independently; reduces barriers for vulnerable populations to participate in research that may benefit themLegal definitions vary by country or jurisdiction; requires careful documentation and justification; may still need ethics committee oversight
In practice, researchers were often concerned about how to truly preserve the rights of MSM minors while respecting their autonomy. Overly strict consent procedures, such as requiring parental permission, could have negatively affected participation and eroded trust among young MSM. This included cases where participants lived in unsupportive or violent households, did not wish to disclose their sexual orientation, or believed they had the capacity to make their own decisions. In some cases, participants distrusted their family members, making parental permission a significant barrier. When such procedures were applied without consideration for participants’ specific contexts, they hindered efforts to foster youth autonomy. In addition, lengthy procedures, complex language, or culturally insensitive materials alienated young MSM from the research process. These barriers made research feel inaccessible or difficult to understand, thereby undermining trust and reducing equitable youth participation. These challenges highlighted the need for ethically appropriate and context-sensitive approaches that both protected the rights of MSM minors and addressed Institutional Review Boards’ (IRBs) concerns about risk and participant safety [37].
The aim of this review article is to examine the consent/assent processes used when conducting HIV research with MSM under age 18 years.
Methods
The protocol for this study was registered with the PROSPERO international prospective register of systematic reviews (registration number: CRD420251067134). This review article is carried out according to the five steps to conducting a systematic review outlined by Kahn et al. 2003 to ensure the review process is executed properly and systematically, as well as meets the review objectives [43].
- Step 1: Framing questions for a review
- Step 2: Identifying relevant work
- Step 3: Assessing the quality of studies
- Step 4: Summarizing the evidence
- Step 5: Interpreting the findings
Framing questions for a review
This review explores the strategies and consent/assent processes used in HIV research involving MSM youths under 18. The research question was framed to address a critical gap in the literature regarding how researchers navigate legal, ethical, and practical challenges in obtaining consent for this population. Specifically, this review examines the question: ‘What strategies and considerations do researchers employ in the consent process when conducting HIV studies involving MSM minors?
Identifying relevant work
We conducted a comprehensive literature search across three databases (PubMed, Embase, and Scopus), covering studies published between 2010 and 2023. A combination of keywords [44–46] and Medical Subject Headings (MeSH) terms was used to capture studies at the intersection of HIV, MSM, youth, and ethical processes. Specifically, the search included terms related to HIV (“HIV”, “Acquired Immunodeficiency Syndrome”, “Human Immunodeficiency Virus”), population terms (“Men who have sex with men”, “Bisexual men”, “Gay”), age-related terms (“Adolescent”, “Youth”, “Minor”, “Teenager”, “Under 18”), and ethical terms (“Consent”, “Assent”). An example of a complete search string used in PubMed was:
(((((((((AIDS) OR (“acquired immunodeficiency syndrome”)) OR (HIV)) OR (“human immunodeficiency virus”)) AND ((((“men who have sex with men”) OR (“bisexual men”)) OR (gay)) OR (“MSM”))) AND ((((((adolescent) OR (youth)) OR (minor)) OR (teenager)) OR (“Under eighteen”)) OR (“Under 18”))) AND ((consent) OR (assent)) AND ((humans[Filter]) AND (english[Filter]) AND (2010:2023[pdat]))) NOT (review)) NOT (“systematic review”)) NOT (“meta-analysis”).
The year 2010 was chosen as the starting point because it represented a transitional period in the field with increasing focus on biomedical prevention options and widespread availability of effective HIV treatment globally, allowing for an examination of research conducted over the past decade and a half while capturing the evolution of consent processes and ethical considerations leading into the present era. This systematic review focuses exclusively on English-language publications concerning human subjects, while excluding literature reviews and protocol papers. To facilitate this process, the Covidence program was employed to screen for duplicate entries. Initially, one researcher reviewed the titles and abstracts to identify relevant studies. Following PRISMA 2020 guidance [47], which permits single-reviewer screening with secondary verification, full-text screening was primarily conducted by a single reviewer (WW). To ensure accuracy and consistency, a second reviewer (TG) independently assessed a random 10% of the articles. In cases where multiple articles were available for the same study, WW and TG jointly selected the report that contained the most detailed information on consent and assent procedures. All steps in the screening process were conducted using the Covidence program [48].
According to the search results obtained from the three databases using the aforementioned search queries, PubMed generated 265 articles, while Embase and Scopus produced 64 and 74 articles respectively, additional with 7 references searched for a total of 410 articles.
Assessing the quality of studies
The researcher assessed the quality of studies using the Mixed Methods Appraisal Tool (MMAT) checklist, a tool specifically designed to evaluate the methodological quality of studies across qualitative, quantitative, and mixed-methods designs. This checklist played a crucial role in examining the rigor, clarity, and potential biases in each study, ensuring the reliability and validity of the review’s findings. The MMAT was particularly suitable for this systematic review, as it provides a comprehensive evaluation of different study methodologies through five key questions. The first author (WW) scored all papers using Microsoft Excel. The senior author (TG) checked 10% of these for accuracy. Based on the MMAT score of 0–5, studies were categorized as follows: those with a score of 0–2 were rated as low quality, studies scoring 3–4 were classified as moderate quality, and studies with a score of 5 were considered to be of high quality [49–51].
Summarizing the evidence
Two researchers (WW and TG) developed a table to extract key information on the consent process in HIV-related research involving MSM youths under 18. The data extraction was organized into two separate tables. The first table captures study characteristics, including research aims and objectives, study design, inclusion criteria, MSM definition, recruitment venues, incentives, and cohort retention strategies. The second table focuses on participant age, consent/assent processes, parental permission waivers, justifications for waiver requests, guardian or proxy involvement, and additional protection measures for participants. (see “Results” section).
Interpreting the findings
The purpose of this review article was to provide an overview of studies related to the consent process in HIV research involving young men who have sex with men (MSM) under the age of 18. The results included a summary of studies conducted over the past 15 years, detailing their methodologies and the consent processes utilized. Following, we highlight the importance of the consent process and identify key associated challenges.
Results
Four hundred and ten articles were returned from a search of 3 databases and references from other sources, after screening, 179 articles were identified that potentially met the selection criteria. After a full-text screening review, 65 of these articles were found to meet study inclusion. Below the results are presented in 3 topics as follows: (1) study characteristics; (2) study design and methodology; and (3) the consent/assent processes (Fig. 1).
Fig. 1. Prisma flow diagram
Characteristics of studies
According to the World Bank’s [117] income level, more than half (n = 42, 64%) of the identified studies among MSM under the age of 18 took place in high-income countries [52–58, 60–63, 65–67, 70, 72–74, 77, 78, 80–82, 84, 88, 89, 91–95, 97–105, 108, 113]. Most of the studies were conducted in the United States, where 28 articles (43%) were published [52, 54, 56–58, 62, 63, 65–67, 70, 77, 80–82, 84, 89, 91, 92, 94, 95, 98, 99, 101–103, 105, 113]. The United Kingdom followed with 4 articles (6%), while Canada contributed 3 articles (4%) [61, 73, 93]. Additionally, there were 2 articles each from Australia (3%) [72, 97] and France (3%) [69, 85], and 1 article each from the Netherlands (1%) [55], New Zealand (1%) [53], and Switzerland (1%) [60]. Among upper-middle-income economies (17 articles, 26%), China had the highest number of studies, with 13 articles (20%) [59, 64, 75, 79, 85, 87, 96, 106, 109, 111, 112, 114, 115], followed by Brazil with 2 articles (3%) [107, 116], and Thailand (1%) [69] and South Africa (1%) [76] each with 1 article. In lower-middle-income economies, there were a total of 6 articles (9%), three of which were from India (4%) [71, 83, 86], while Nigeria (1%) [68], Pakistan (1%) [110], and Vietnam (1%) [90] each had 1 article. No studies on HIV involving young men who have sex with men (YMSM) under the age of 18 were found from low-income countries (See Fig. 2).
Fig. 2. World Bank countries distribution of included studies
In this review, the term MSM (men who have sex with men) is generally defined as gay or bisexual men, or more broadly, as men who engage in sexual activities with other men. However, the operational definition of “sex” varied across studies. Some studies defined sex strictly as anal sex only (14 articles) [63, 66, 70, 75, 77, 79, 81, 85, 87, 104, 106, 108, 111, 112], while others included both anal and oral sex (6 articles) [59, 64, 71, 83, 86, 96].
Most of the studies used a broad definition, categorizing men simply as male without providing a specific definition (35 articles) [52–58, 60, 65, 68, 71, 72, 74, 75, 78, 81, 83, 84, 86, 88–90, 93–95, 97–100, 102, 107, 109, 112, 115, 116]. In contrast, 21 articles defined men as those assigned male at birth or as cisgender males [59, 62–64, 66, 67, 70, 77, 79, 80, 82, 85, 87, 92, 96, 101, 105, 106, 111, 113, 114]. Four studies included a wider definition that encompassed trans men or trans women [61, 104, 108, 110]. Five articles provided no clear information about the definition of men or males, only referring to “LGBTQ", "LGBT+", "LGBQA", "gay men", or "sexual minorities" [69, 73, 76, 91, 103] (See Table 2).
Table 2. Characteristics of the included studies (N = 65)No.YearAuthorsCountryObjectives^a^Study design and inclusion criteriaMSM definition^b^Recruitment VenueIncentivesCohort retention^c^MMAT score12015Alexander et al. [52]USATo explore the process of adolescent decision-making on participation in an HIV vaccine clinical trialDesign: QualitativeParticipants: N = 33 (19 MSM), aged 16–19 years, HIV-negativeDescription: Participants underwent a simulated HIV vaccine trial consent process and subsequently completed in-person semi-structured interviewsSetting: In-person (across four urban U.S. sites)1) Male2) Sexually active MSM who had sex with males1) Community-based organizations (CBOs)2) Health clinics3) Youth groups4) Community eventsNo information providedN/A5/522010Azariah et al. [53]New ZealandTo collect data on STI and HIV diagnoses in a sample of MSM who visited the Auckland Sexual Health Service, as well as to investigate possible risk factorsDesign: Quantitative (observational cross-sectional study)Participants: N = 87 MSM, aged 15–66 yearsDescription: Clinic-based questionnaire (participant or clinician completed); onsite HIV/STI testingSetting: In-person (clinics)1) Male2) Ever had sex with a manAuckland Sexual Health Service (ASHS)No information providedN/A3/532016Bares et al. [54]USATo expand Testing and Linkage to Care (X-TLC) aimed to expand routine HIV testing programs for disproportionately affected populations on the South Side of ChicagoDesign: Quantitative (quasi-experimental)Participants: N = 67,153 minority men and women, MSM, aged 16–78 yearsDescription: HIV testing & linkage-to-care, routine and point-of-care HIV testing comparisonSetting: In-person (clinics)Men who have sex with menRecruitment involved routine, opt-in testing in high-prevalence communities at clinics, hospitals, and EDs.No information providedN/A2/542017Bartelsman et al. [55]NetherlandsTo evaluate whether the HTW (HIV Testing Week 2015) was an effective strategy for increasing HIV testing and detecting new infections among the targeted risk groupsDesign: Quantitative (quasi-experimental)Participants: N = 1,231 high-risk groups (304 MSM), aged 16–81 yearsDescription: Self-administered questionnaire and free HIV rapid/self-testingSetting: In-person testing at hospitals, GP clinics, STI clinic, outreach sites; home-based via online platformMen who have sex with menRecruitment took place at hospitals, GP clinics, STI clinics, outreach locations, community sites, and via home-based testing.No information providedN/A2/552010Begier et al. [56]USATo anonymously assess HIV prevalence among individuals entering New York City jails and approximate the percentage of cases that were previously undiagnosedDesign: Quantitative (observational cross-sectional study)Participants: 6,411 prisoners (47 MSM), aged 16 years and aboveDescription: Information was collected through a standardized medical intake questionnaire by health care workersSetting: In-person (Jail)Men who have sex with menJailNo information providedN/A3/562018Bhatia et al. [57]USATo describe the outcomes of this implementation approach in the context of a PrEP continuum that has been developedDesign: Quantitative (observational longitudinal cohort study)Participants: N = 137 walk-in patients from STI clinics (126 MSM), aged 12 years and older, all HIV-negativeDescription: Clinical data extracted from STI clinic records and PrEP partner sites (no self-administered questionnaire used)Setting: In-person (public STI clinics; follow-up conducted by partner PrEP clinics)Men who have sex with menChicago Department of Public Health (CDPH) STI Clinics.No information providedN/A2/572018Bonett et al. [58]USATo describe the process of constructing paradata measures based on the intervention’s theoretical framework, as well as to investigate whether participants’ sociodemographic traits are related to their overall and feature-specific use and engagement with the interventionDesign: Quantitative (Experimental)Participants: 130 MSM, aged 15–24) yearsDescription: Online intervention to promote HIV testingSetting: OnlineMen who have sex with men1) Community-based organizations2) Social media and dating apps (e.g., Grindr, Facebook)Electronic gift card (10 at each follow-up)Electronic gift card (10 at each follow-up)3/582018Cao et al. [59]China1) To examine the relationship between online STI information seeking and offline STI physician visits among YMSM2) To examine the role of social media as a source of STI information and as a method of linking care to STI healthcare providersDesign: Quantitative (observational cross-sectional study)Participants: N = 503 MSM, aged 16–30 years old, all had visited a physician within the past 24 monthsDescription: Nationwide online surveySetting: Online1) Male at birth/cisgender male2) Had anal or oral sex with menOnline via gay apps: WeChat, Blued, Qingtong, SESHA small phone credit reimbursement (~7.50 USD)N/A3/592016Clerc et al. [[60](#CR60)]SwitzerlandTo examine HCV awareness (risk factors, disease course, and treatment) among MSM attending screening clinics and meeting places in southwest Switzerland against behavioral risk factors reported and examined HCV seroprevalence among MSMDesign: Quantitative (observational cross-sectional study)Participants: 654 MSM, aged 16–80 yearsDescription: Self-administered questionnaire under field worker supervision, followed by on-site rapid HCV testingSetting: In-person (MSM clinics and indoor/outdoor meeting venues)Men who have sex with men1) Distribution from community-based organizations (CBOs) and health clinics2) MSM meeting venues: indoor (e.g., saunas, sex clubs) and outdoor (e.g., Pride events, cruising areas)No information providedN/A3/5102019Closson et al. [[61](#CR61)]CanadaTo understand differences in HIV prevention awareness, access to health care, and service utilization between MSM, as well as factors associated with attendance in HIV leadership programmingDesign: Quantitative (Observational longitudinal cohort study)Participants: *N* = 698 GBM, aged ≥ 16 yearsDescription: Assessed real-world uptake, effectiveness, and impact of HIV leadership programs. Data were collected every 6 months via computer-assisted self-interview (CASI).Setting: In-person data collection at a study office in Vancouver’s West End, Canada1) Men/transmen2) Reported having sex with another manRecruitment was conducted using Respondent-Driven Sampling (RDS) in Metro Vancouver, Canada.Monetary incentives (50 for each visit and additional 50 for each visit and additional 10 for recruitment of a new participant)4/5112022Cordoba et al. [[62](#CR62)]USAThis study aimed to examine if restrictive state policies requiring parental consent for HIV testing impact testing rates among young men who have sex with men (YMSM) in the USADesign: Quantitative (observational cross-sectional study)Participants: *N* = 612 MSM, aged 13–17 years, HIV negativeDescription: Secondary data analysis from an mHealth HIV prevention trialSetting: Online1) Male at birth2) Self-identify as male or non-binary3) Sexually attracted to male1) Local outreach- Active recruitment in community organizations/events- Passive recruitment using flyers2) Internet outreach via paid and targeted ads on social media platforms (IG, FB, Snapchat)N/AN/A3/5122011Dorell et al. [[63](#CR63)]USATo evaluate the associations between health care and HIV infection, as well as to identify missing HIV/STI testing opportunitiesDesign: Quantitative (Observational unmatched case-control study)Participants: *N* = 125 MSM, aged 16–25 years, both HIV-positive and HIV-negativeDescription: Self-administered computerized questionnaireSetting: In-person (clinics, campuses, clubs, malls, community events)1) Cisgender male2) Self-reported having anal sex with a man1) Case recruitment: Identified through the HIV/AIDS Reporting System (HARS)2) Control recruitment: Recruited from local venues (e.g., STD clinics, colleges, bars, malls, and community events) in Jackson, MississippiElectronic gift card (25)N/A4/5132017Duan et al. [64]ChinaTo explore patterns of recreational drug use among men who have sex with men (MSM) in Shenzhen, focusing on preferred substances and their associations with HIV and syphilis infectionsDesign: Quantitative (observational cross-sectional study)Participants: N = 1935 MSM, aged 16–79 yearsDescription: Self-administered computer-based questionnaire and laboratory testing for HIV and syphilisSetting: In-person (Shenzhen CDC and MSM community venues)1) Male at birth2) Having had sexual contact (oral or anal sex) with other males1. Time-Location Sampling (TLS) – Bars, saunas2. Respondent-Driven Sampling (RDS) – Participants recruit others3. Snowball Sampling – Referrals through social networksMonetary incentives (10 for the recruitment of a new participant)Monetary incentives (10 for the recruitment of a new participant)3/5142016Fisher et al. [65]USATo examine the attitudes of sexual and gender minority youth (SGMY) toward guardian permission for a pre-exposure prophylaxis (PrEP) adherence trial and their preparedness to provide informedDesign: Mixed methods (primarily qualitative with supportive quantitative survey items)Participants: N = 60 (self-identified sexually active SGMY), aged 14–17, HIV negativeDescription: Online questionnaire and asynchronous online focus group discussions (FGDs)Setting: OnlineMen who have a sexual experience or romantic interest in the male partnersPaid Facebook advertisements targeted at youth whose profiles indicated romantic interest in same gender personsNoN/A4/5152018Fisher et al. [66]USATo investigate adolescent men who have sex with men (AMSM) attitudes toward participating in oral/injectable PrEP RCTs in order to influence future study protections of youth’s rights and welfareDesign: Quantitative (observational cross-sectional study)Participants: N = 198 MSM, aged 14–17 years, HIV-negativeDescription: Self-administered online questionnaireSetting: Online1) Cisgender male2) Being attracted to males3) Reporting at least one lifetime male anal sex partnerUsing Facebook advertisementsElectronic gift card (30)N/A3/5162020Fisher et al. [[67](#CR67)]USATo give experimental information on AMSM’s competence to consent to a randomized clinical trial assessing the safety and efficacy of oral and injectable PrEP and to inform IRB decisions on waiver of guardian permissionDesign: Quantitative (observational cross-sectional study)Participants: *N* = 214 MSM, aged 14–19 years, HIV-nagativeDescription: self-administrated online questionnaireSetting: Online1) Assigned male at birth2) Reported attraction to or sexual experience with male partnersRecruited from online social media advertisements on Facebook and InstagramElectronic gift card (30)N/A3/5172022Folayan et al. [68]NigeriaTo enhance population health by identifying effective ways to strengthen enablers and reduce obstacles to healthcare accessDesign: Quantitative (observational cross-sectional study)Participants: N = 2119 (1,272 MSM), aged 13–72 yearsDescription: Self-administered online questionnaire across 9 high HIV-prevalence states in NigeriaSetting: OnlineMen who have sex with other men1) Snowballing2) Crowdsourcing by placing calls through to community members and making contact using social media platforms like Facebook, WhatsApp, and email to reach eligible participants3) Through the National Umbrella Network for the target populationsNo information providedN/A3/5182021Fongkaew et al. [69]ThailandTo garner evidence, especially young people’s perspectives, to support tailored HIV preventive interventionsDesign: QualitativeParticipants: N = 25 (20 MSM, 5 TGW), aged 16–20 yearsDescription: Four Focus Group Discussions (FGDs), segmented by ageSetting: In-person (three semi-urban provinces in eastern Thailand)No information provided (use “gay men”)Recruited from high schools and universities in three semi-urban provinces by contacting teachers known to be LGBT allies and student clubs involving LGBT members10N/A5/5192018Frye et al. [[70](#CR70)]USATo report the findings of a preliminary research phase of a bigger study aimed at informing the development of a communication technology-based intervention to increase consistent HIV testing among this age groupDesign: QualitativeParticipants: *N* = 30 (28 MSM), aged 16–29 years, HIV-negative or unknown statusDescription: In-depth interviews (IDI)Setting: In-person (New York City metropolitan area)1) Male at birth2) Report insertive or receptive anal intercourse with a man or transgender woman1) Participants were recruited via platforms like Facebook and Craigslist2) Face-to-face recruitment took place at community events like kiki balls and The Piers in NYCElectronic gift card (30)N/A5/5202014Godbole et al. [71]IndiaTo identify the prevalence and predictors of bisexual behavior among MSM attending TI sites, as well as the risk factors for HIV infection among MSMDesign: Quantitative (observational cross-sectional study)Participants: N = 4,682 MSM, aged 18–49 years (propose design 15 years)Description: Participants completed a one-page, 11-item questionnaire administered by trained counsellors and provided capillary blood samples for anonymous HIV testingSetting: In-person (19 drop-in centers across four Indian states)1) Male2) Had anal and/or oral sex with another maleRecruitment was conducted at 19 sites across four Indian states: Goa, Maharashtra, Gujarat, and Madhya Pradesh.No information providedN/A3/5212022Gosset et al. [72]FranceTo assess the proportion and the characteristics of the participants who distributed HSTs, as well as the characteristics of people who received HSTsDesign: Quantitative (observational cross-sectional study)Participants: N = 283 (267 MSM); aged ≥ 15 years; 86 were HIV-positiveDescription: Participants were recruited from a sexual health center and asked to distribute HIV self-tests to people in their networksSetting: In-person (Sexual Health Center, Paris, France)Men who have sex with other menLGBT + community-based a sexual health centerNo information providedN/A3/5222015Hadland et al. [73]CanadaTo investigate the relationship between childhood maltreatment and the risk of suicide attempts among street-involved youthDesign: Quantitative (observational longitudinal cohort study)Participants: N = 660 street youth; aged 14–26 yearsDescription: Interviewer-administered questionnaire and self-administered Childhood Trauma Questionnaire (CTQ)Setting: In-person (storefront location in downtown Vancouver, Canada)No information provided (Use “Lesbian/gay/bisexual/transgender”)Neighborhoods where street youth were known to congregate, with snowball samplingNoN/A4/5232017Hammoud et al. [74]AustraliaTo report findings from an online prospective study on legal and illegal substance use among gay and bisexual men (GBM), and to assess baseline prevalence within the sampleDesign: Quantitative (observational longitudinal cohort study)Participants: N = 2,250 MSM; 16–81 yearsDescription: Nationwide sample (Australia); self-administered online questionnaireSetting: Online1) Male2) Identifying as a gay/homosexual or bisexual man or3) Had sex with at least one manThe Flux study website was the main recruitment platform. Most participants joined via targeted Facebook ads.No information providedNo3/5242018He et al. [75]ChinaTo investigate factors linked to drug use and HIV infection among MSM in Hangzhou, China, with a focus on determinants associated with emerging substances like methamphetamine, ketamine, ecstasy, and rush poppersDesign: Quantitative (observational cross-sectional study)Participants: N = 555 MSM;; aged ≥ 16 years; HIV-negative or unknown status at baselineDescription: Face-to-face questionnaire interviews followed by on-site HIV testingSetting: In-person (community-based in Hangzhou, China)1) Male2) Had anal sex with menSnowball samplingMonetary incentives (30)N/A3/5252017Hogg et al. [[76](#CR76)]South AfricaTo examine adolescents’ knowledge regarding the origin of HIV? AIDS and correlates of beliefs surrounding conspiracy in Soweto, South AfricaDesign: Quantitative (observational cross-sectional study)Participants: *N* = 830 adolescents; 14–19 years; male and femaleDescription: Interviewer-administered structured questionnaire via iPad or desktop computerSetting: In-person (Kganya Motsha Adolescent Centre and Perinatal HIV Research Unit, Soweto, South Africa)No information provided (Use “No: Heterosexual”)1) Kganya Motsha Adolescent Centre2) the Perinatal HIV research Unit’s Bosha Bophelo Adolescent Health study (BBAHS)Participants were given an honorarium of 50 ZAR (2.67) for transportation and associated participation costsN/A3/5262017Hosek et al. [77]USATo investigate the safety and adherence to PrEP, and changes in sexual risk behavior among adolescent men who have sex with men (MSM)Design: Quantitative (Experimental; open-label phase 2 study)Participants: N = 78 MSM; aged 15–17 years, HIV-negative at baselineDescription: Self-administered computerized questionnaires, clinical STI testing, and biological sampling (e.g., dried blood spots for drug levels)Setting: In-person (adolescent medicine clinics in 6 US cities)1) Male at birth2) Anal intercourse with a male partner1) Online social media advertisements2) Distribution from community-based organizations (CBOs)Mobile phone top-up (75)N/A3/5272023Huang et al. [78]AustraliaThis study evaluates the proportion of attendees at a sexual health service who opted in or out of SHAVEDesign: Quantitative (Observation longitudinal cohort study)Participants: N = 18,582 (7,611 MSM); aged ≥ 16 years oldDescription: On-site computer-assisted self-interview (CASI), completed digitally by clients while physically present at the Melbourne Sexual Health Centre, prior to seeing a clinician.Setting: In-person (Melbourne Sexual Health Centre (MSHC), Australia)1) Men who have sex with men2) Men who have sex with men and womenMelbourne Sexual Health Centre (MSHC) between March 2021 and June 2022No information providedNo3/5282019Jin et al. [79]ChinaTo determine the feasibility of the Easy Test in increasing access and uptake of HIV testing and treatment services among MSM, and to identify demographic and behavioral predictors of program uptake in order to guide future implementationDesign: Quantitative (observational cross-sectional study)Participants: N = 879 MSM; aged ≥ 16 years old, HIV-negative or unknown statusDescription: Self-administered online questionnaire and home-delivered HIV self-testing kits with image upload for result confirmationSetting: Online1) Male at birth2) Had engaged in anal sex with a manOnline Social Media Advertisements (WeChat, QQ, and Blued)Free test kitN/A3/5292023Kaufman et al. [80]USAThis study is a usability test of a mobile app designed for the mentors of African American YMSM to increase mentors’ knowledge of and confidence in talking about HIV prevention and related topics with menteesDesign: Mixed methodsParticipants: N = 16 YMSM; aged 15–24 yearsDescription: Pre- and post- surveys to assess changes in HIV-related knowledge, confidence, and mentoring practices. After using the UrbanMentorHub app, participants also joined FGD to share feedback on app usability, mentoring experience, and suggested improvements.Setting: In-person (Baltimore and Philadelphia), online (due to COVID-19)1) Cisgender male2) Had sexual interest in males or reported having sex with men1) Community events2) Posted on social media sites3) Advertised on radio shows, newspapers, and gay dating apps4) Respondent-driven sampling (RDS)50N/A4/5302022Knopf et al. [[81](#CR81)]USATo explore how factors such as consent requirements, gender, sexual orientation, and characteristics of clinical trials influence minors’ willingness to participate in biomedical HIV prevention studiesDesign: Quantitative (quasi-experimental)Participants: *N* = 129 LGBTQ; aged 14–17 years old; HIV-negative or unknown statusDescription: Participants completed simulated consent procedures and self-administered surveys using QualtricsSetting: In-person (clinical and community facilities)1) Male2) Have anal sex with another man1) Research locations: Baltimore (MD), Chicago (IL), Denver (CO), and Tampa (FL)2) Recruitment tools: Flyers displayed in clinics and handed out at community events (e.g., Pride), along with outreach via social media platforms3) In-person engagement: Participant recruitment conducted directly at youth health centers and local community-based organizations50N/A3/5312017Knopf et al. [82]USATo investigate autonomous consent and study experiences among minor and adult Project PrEPare participants, a Phase II safety study of PrEP for HIV prevention. (Project PrEPare was the first biomedical HIV prevention study in the United States to allow minors to consent autonomously for enrollment if such consent was consistent with local statutes)Design: Mixed methodsParticipants: N = 58 MSM; aged 15–22 yearsDescription: Self-administered online questionnaire and in-depth interviews (IDIs). The questionnaire was completed online; interviews were conducted via phone or videoconference.Setting: Online1) Male at birth/cisgender male2) Men who engage in sexual acts with other menResearch staff from the 10 participating Adolescent Medicine Trials Network (ATN) centers contacted eligible participants, all of whom had previously taken part in Project PrEPare, a Phase II HIV prevention study.No information providedN/A4/5322020Kumar et al. [83]IndiaTo compare the factors associated with HIV infection among multi-risk MSM who use any substance to those who do not use any substanceDesign: Quantitative (observational cross-sectional study)Participants: N = 23,081 MSM; aged 16–80 yearsDescription: Data were collected through computer-assisted personal interviews (CAPI), and blood samples were obtained via dried blood spot (DBS) for HIV testing.Setting: In-person (community-based across 108 districts in India)1) Male2) Had anal, or oral sex with a male/hijra partner4,067 hotspots in 108 districts across IndiaNo information providedN/A3/5332014Lally et al. [84]USA1) To assess the effectiveness of supplementary brochures using persuasive content to enhance understanding of HIV vaccine trials, especially addressing themes related to preventive misconception2) To examine how numeracy, health literacy, and impulsivity in decision-making relate to participants’ comprehension of key elements in an HIV vaccine trialDesign: Mixed methodsParticipants: N = 120 women and men who were sexually active with men; aged 16–19 yearsDescription: Participants completed questionnaires and were randomized to receive no brochure, a one-sided, or two-sided brochure about HIV vaccine trials. A subset also joined follow-up interviews.Setting: In-person (four Adolescent Trials Network (ATN) sites in the U.S.)Men who were sexually active with menFour Adolescent Trials Network (ATN) sitesNo information providedN/A4/5342017Li et al. [85]ChinaTo investigate whether peer norms and self-efficacy act as mediators in the observed relationshipDesign: Quantitative (observational cross-sectional study)Participants: N = 1,042 MSM; aged ≥ 16 yearsDescription: A nationwide, self-administered online questionnaire assessing community engagement, condom use peer norms, self-efficacy, and condom use behaviors using validated instrumentsSetting: Online1) Male at birth2) Having had anal sex with a man at least once during their lifetime1) A popular online social networking platform: Danlan.org2) Weibo and WeChatNo information providedN/A3/5352015Mahapatra et al. [86]IndiaTo produce scientific insights by analyzing socio-demographic and behavioral factors linked to HIV risk among MSM in West Bengal, based on HSS dataDesign: Quantitative (observational cross-sectional study)Participants: N = 1,237 MSM; aged 15–49 yearsDescription: Structured, interviewer-administered questionnaire assessing socio-demographic and behavioral characteristics; anonymous HIV testing was performed following national guidelinesSetting: In-person (drop-in center across five districts in West Bengal, India)1) Male2) Had anal or oral sex with a male partnerDistribution from community-based organizations (CBOs)No information providedN/A3/5362018Mao et al. [87]China1) To describe patterns of sex tourism among Chinese MSM identified as having elevated HIV risk2) To identify socio-demographic and behavioral factors associated with sex tourism among MSM in ChinaDesign: Quantitative (observational cross-sectional study)Participants: N = 1,189 MSM; aged ≥ 16 yearsDescription: Self-administered online questionnaire conducted nationwide through gay-focused online platformsSetting: Online1) Male at birth2) Had anal sex with men1) Danlan.org, an online gay portal2) A gay mobile dating app BlueD3) Weibo and WeChatNo information providedN/A3/5372022Marchant et al. [88]UKTo implement an HIV testing strategy in emergency departments using existing biochemistry samples, aiming to increase testing uptake without altering routine clinical workflowsDesign: Quantitative (observational cross-sectional study)Participants: N = 78,333 (males and females who get HIV test); aged ≥ 16 yearsDescription: HIV testing was initially opt-in and later transitioned to an opt-out approach with notional consent, utilizing biochemistry samples from routine ED blood draws.Setting: In-person (Emergency Department of a large teaching hospital in London)Men who have sex with menOTP-out HIV testing programNo information providedN/A3/5382021Mata et al. [89]USATo explore the sexual learning experiences of bisexual male youth and their preferences regarding sexuality educationDesign: Mixed methodsParticipants: N = 56 bi-male youth; aged 14–17 years; HIV-negative or unknown statusDescription: Data were collected through an online survey and semi-structured interviews exploring participants’ experiences with and preferences for sexuality education.Setting: In-person (e.g., at community-based LGBTQ + organizations) and online (via phone or video conferencing), depending on participant location and preference.1) Male2) Identified as bisexual, pansexual, or queer1) In-person (e.g., at community-based organizations serving LGBTQ youth)2) On social media (e.g., Facebook, Instagram)30 Amazon giftN/A4/5392020Michel et al. [[90](#CR90)]VietnamTo identify the profiles of young people who use drugs (YPUD) and their HIV risk exposure in Vietnam’s three major cities, Haiphong, Hanoi, and Ho Chi Minh City (HCMC), to design a community-based HIV prevention interventionDesign: Quantitative (observational cross-sectional study)Participants: *N* = 584 YPUD; aged 16–24 yearsDescription: Structured questionnaire administered by trained interviewersSetting: In-person interviews conducted in community settingsMen who have sex with men1) Respondent-driven sampling (RDS)2) Peer recruitmentParticipants received VND 150,000 (7.50 USD) for their participation and VND 50,000 (2.50 USD) for each YPUD they helped recruitAll participants received VND 100,000 for coming backto get their screening results3/5402017Mustanski et al. [[91](#CR91)]USAUnderstanding teenagers’ perspectives on parental permission and the risks and benefits of participating in HIV research is critical to informing evidence-based IRB decisionsDesign: Mixed methodParticipants: *N* = 74 sexual and gender minority adolescents; aged 14–17 yearsDescription: Online focus group discussions and pre/post surveys exploring views on HIV research participation and parental permission.Setting: Online1) Sexual minority (e.g., lesbian, gay, bisexual, queer, questioning)2) Gender minority (e.g., transgender, nonbinary, genderqueer) were romantically interested in or had sex with cisgender male partnersPaid Facebook advertisementsa 30 gift cardN/A4/5412020Nelson et al. [92]USATo assess the differences between Adolescent Sexual Minority Males (ASMM) with and without legal capacity to consent to HIV testing and treatment and to describe associations between legal capacity to consent and testing behavior; and to explore whether ASMM who have tested believe that parental/guardian consent was requiredDesign: Quantitative (observational cross-sectional study)Participants: N = 127 Adolescent Sexual Minority Males; aged 14–17 yearsDescription: A self-administered online questionnaire collected data on demographics, sexual behavior, HIV testing history, and perceptions of legal consent and confidentiality.Setting: Online1) Cisgender males2) Self-identified as gay/bisexual, or reported male-male attraction or sexual contactOnline social media advertisements (Instagram, Facebook)Electronic gift card (15)N/A3/5422019Nelson et al. [[93](#CR93)]CanadaTo examine the prevalence of HIV, STIs, and HIV/STI co-infections in a community-recruited, non-probability sample of MSM and to examine whether past histories of STIs were associated with current HIV infectionDesign: Quantitative (observational cross-sectional study)Participants: *N* = 487 Black men (86 MSM); aged ≥ 16 yearsDescription: Participants completed a self-administered, computer-assisted survey (ACASI) and provided biological specimens for HIV and STI testing.Setting: In-person (three community health centers across Toronto)1) Male2) Reported having sex with menDistribution from community-based organizations (CBOs) and health clinicsNo information providedN/A3/5432017Osorio et al. [[94](#CR94)]USATo assess an opt-out inpatient HIV screening program that was provided using admission orders written by physician house staff. These data were compared to the number of HIV tests and diagnoses performed in the ED as part of physician-ordered HIV testing based on signs and symptomsDesign: Quantitative (observational cross-sectional study)Participants: *N* = 39,435 admitted patients and house staff medical; aged 13–64 yearsDescription: Self-administered questionnaire. Participants completed surveys assessing their experiences, understanding, and attitudes toward inpatient opt-out HIV screening.Setting: In-person (teaching hospital in the United States)Men who have sex with menUniversity of California, San DiegoNo information providedN/A3/5442013Ott et al. [[95](#CR95)]USATo address preventive misconception—where participants overestimate the level of protection they receive by participating in a prevention trialDesign: QualitativeParticipants: *N* = 33 adolescents; aged 16–19 years; male, female and MSM; HIV-negativeDescription: Explored adolescents’ understanding of clinical trial concepts—such as experiment, placebo, and randomisation—and their perceptions related to preventive misconception in the context of a simulated HIV vaccine trial.Setting: In-person (four Adolescent Medicine Trials Network (ATN) sites)1) Male2) Reported having sex with men1) Community agencies2) Youth programmes3) Clinics4) Gay pride eventsNo information providedN/A5/5452019Pan et al. [[96](#CR96)]ChinaTo explore key factors influencing HIV testing decisions among men who have sex with men (MSM) in ChinaDesign: Mixed methodsParticipants: *N* = 803 MSM; aged ≥ 16 years; HIV-negativeDescription: A self-administered online questionnaire, including a discrete choice experiment (DCE), was used to assess HIV testing preferences. FGDs were conducted to identify key service attributes for the DCE design.Setting: Online1) Male at birth2) Had anal or oral sex with another man1) Online social media advertisements2) Distribution from community-based organizations (CBOs)- 15 USD for FGD- Mobile phone top-up (7.50) for pilot test surveyN/A4/5462020Peuchant et al. [[97](#CR97)]FranceTo assess how common LGV is among French MSM using HIV PrEP who test positive for anorectal Chlamydia trachomatisDesign: Quantitative (observational cross-sectional study)Participants: *N* = 486 MSM; aged 17–69 years, tested positive for anorectal Chlamydia trachomatis and were using PrePDescription: Prescribing clinicians completed a standardized questionnaire covering demographic, clinical, biological, and behavioral dataSetting: In-person (30 hospitals and 10 STI screening centers throughout metropolitan France)Men who have sex with men30 hospitals and 10 STI screening centers throughout metropolitan FranceNo information providedN/A3/5472018Philbin et al. [[98](#CR98)]USATo explore the association between incarceration and transactional sex among HIV-infected YMSMDesign: Quantitative (observational cross-sectional study)Participants: *N* = 97 MSM living with HIV; aged 18–24 yearsDescription: Online survey collecting data on incarceration history, transactional sex, sociodemographic factors, drug use, and HIV care status.Setting: Online1) Identified as male2) Reported having sex with a manAdolescent Medicine Trials Network (ATN) clinical sites25N/A3/5482021Phillips et al. [99]USATo assess whether the offer of a single, free HIV self-testing kit led to increased HIV diagnoses with linkage to careDesign: Quantitative (Observational cross-sectional study)Participants: N = 29,992 adolescents (10,111 MSM); aged ≤ 17 yearsDescription: Pooled data from The 2017 local Youth Risk Behavior Survey (YRBS), assessing associations between HIV testing and state-level minor consent laws, with analysis stratified by sex and sexual behaviorSetting: In-person (school-based survey across 25 U.S. jurisdictions, YRBS 2017)1) Male2) Reported sex with both males and females or same-sex sexual contactHigh schools across 25 U.S. jurisdictions by departments of education or healthA free BioSURE self-testing kitNo3/5492013Pollard et al. [100]UKTo address this deficit by investigating the motivations and attitudes towards opt-out testing among different groups recruited from the community in a geographical area of high prevalence of HIV in the UKDesign: QualitativeParticipants: N = 31 (15 women, 16 lesbian/gay/bisexual); aged ≥ 16 yearsDescription: Community-based focus groups discussing opt-out HIV testingSetting: In-person (Brighton community centers)Men who have sex with men1) Local community and voluntary organizations2) Advertisements in the local press3) Word of mouth4) Interested individuals emailed or telephoned through the researcher£20 recompenseN/A5/5502017Puckett et al. [101]USATo investigate negative urgency (the tendency to act impulsively in response to negative emotional experiences), positive urgency (the tendency to act impulsively in response to positive emotional experiences), and sensation seeking as independent moderators of the association of IH with binge drinking, drug use, and condomless anal sexDesign: Quantitative (observational longitudinal study)Participants: N = 450 MSM; aged 16–20 yearsDescription: Self-administered online questionnaires conducted at four time points (baseline, 6, 12, and 18 months)Setting: Online1) Male at birth2) Identified as gay/bisexual or had sex with a man1. Targeted in-person outreach at community venues and schools2. Online recruitment via geo-social networking applications (e.g., Grindr, Jack’d)3. Distribution through community-based organizations (CBOs)4. Incentivized peer recruitment (i.e., snowball sampling)Monetary incentives (45 at each follow-up)Monetary incentives (45 at each follow-up)3/5512020Rendina et al. [102]USATo extend prior research by monitoring trends in belief accuracy regarding the U = U message among sexual minority men (SMM), identifying related factors, and examining links between these beliefs and perceived HIV transmission risk during condomless anal sex (CAS) with undetectable partnersDesign: Quantitative (observational cross-sectional study)Participants: N = 111,747 sexual minority men; aged 13–88 yearsDescription: Online survey conducted in the U.S., with participants recruited via social media, dating apps, and sexual networking websitesSetting: Online1) Male2) Report male-identified casual or main partners, or identify as a sexual minority1) Targeted digital ads on social media platforms, including pop-ups and inbox messages within popular geolocation-based dating apps2) Banner advertisements placed on web-based platforms used for sexual or dating networkingNo incentiveN/A3/5522021Rice et al. [103]USATo present the results of a quasi-experimental design that compares a PCA model delivered in drop-in centers with 3 study arms: (1) PCA selection based on AI; (2) PCA selection based on popularity, operationalized as Youth Experiencing Homelessness (YEH) with the highest DC; and (3) an observation-only comparison group (OBS)Design: Quantitative (quasi-experimental, 3-arm study)Participants: N = 713 (Youth experiencing homelessness); aged 16–24 yearsDescription: Online questionnaire and intervention conducted at 3 drop-in centers to compare the effectiveness of peer-led HIV prevention interventionsSetting: Online and in-person (drop-in centers)No information provided (use “LGBQ”)Recruited from 3 different drop-in centers in LA60N/A4/5532022Rodger et al. [[104](#CR104)]UKAim to assess whether the offering single, free HIV self-testing kit led to increased HIV diagnoses with linkage to careDesign: Quantitative (observational longitudinal study)Participants: *N* = 10,111 MSM; aged ≥ 16 yearsDescription: Online recruitment and data collection via sexual and social networking platforms; participants randomly allocated (3:2) to receive a free HIV self-test kit or no offerSetting: Online1) Being a man (including transgender men)2) Reported ever having anal intercourse with a manOnline through sexual and social networking site including Grindr, Hornet, Recon, Scruff and community FB also using AdsA free BioSURE self-testing kitNo4/5542023Schnall et al. [[105](#CR105)]USATo evaluate the practicality of HIV self-testing (HIV-ST) among very young MSM and analyze variations in test uptake based on demographics and parental consent requirementsDesign: Quantitative (quasi-experimental)Participants: *N* = 253 MSM; 14–21 years; HIV-negative or unknown statusDescription: Participants were contacted after completing a mobile HIV prevention intervention and offered a home HIV self-testing kit. Data collection was done via REDCap and video calls, including survey responses and test completion.Setting: Online (test kits mailed and procedures conducted virtually)1) Male at birth2) Self-identify as male3) Report sexual interest in other men4) Has either kissed another man or plan on having sex with a man in the next yearMyPEEPS Mobile Trial program40 electronic gift cardN/A3/5552019Smith et al. [106]ChinaTo compare latent class analysis (LCA) results from two online samples of HIV-negative Chinese MSM, aiming to identify more generalizable class structures and evaluate how sampling methods influence the validity of findingsDesign: Quantitative (observational cross-sectional study)Participants: (1) Nationwide online sample (N = 582 MSM, HIV-negative or untested, urban only) and (2) Guangzhou sentinel surveillance sample (N = 604 MSM, HIV-negative)Description: Self-reported behavioral surveys; HIV/syphilis testing in Guangzhou sampleSetting: Online and in-person (clinic)1) Male at birth2) Reported ever having had anal intercourse with another man1) Nationwide: Banner ads on BlueD app and danlan.org2) Guangzhou: Banner ads on gztz.org with in-clinic HIV/STI testingNo information providedN/A3/5562023Soares et al. [107]BrazilTo outline the process of PrEP uptake and identify factors associated with PrEP initiation among adolescent MSM and transgender women (TGW) in BrazilDesign: Quantitative (observational cross-sectional study)Participants: N = 903 adolescents (86.8% is MSM); aged 15–19 yearsDescription: Analyzed baseline data from an observational cohort (PrEP1519) to assess factors associated with same-day oral PrEP initiation among adolescent MSM and TGWSetting: Online and in-person (three urban PrEP clinics in São Paulo, Salvador, and Belo Horizonte, Brazil)1) Male2) Had sexual practices with cisgender men, and/or TGW1) Peer-educator-led outreach via schools, LGBTQIA + NGOs2) Social media (Instagram, Facebook, WhatsApp)3) Hookup apps (Grindr, Tinder, Badoo)No information providedN/A3/5572023Sullivan et al. [108]UKTo determine the size and characteristics of the population attending sexual health services (SHS) in England, assess their need and duration of need for PrEP, and evaluate both uptake and duration of PrEP useDesign: Quantitative (implementation trial with longitudinal follow-up)Participants: N = 24,268; aged ≥ 16 years; HIV-negativeDescription: Real-world implementation trial with data collected through electronic case report forms and national surveillance datasets (GUMCAD)Setting: In-person (sexual health clinics across England)1) Cisgender males and transgender men and transgender women2) Has anal intercourse with men157 sexual health services (SHS) across EnglandNo information providedN/A4/5582019Taklual et al. [109]ChinaTo evaluate the effect of route of transmission on the genotype distribution of HPgV, to determine the prevalence rate, and to identify the dominant genotypes among the two high-risk populationsDesign: Quantitative (observational cross-sectional study)Participants: N = 201 (131 MSM and 70 IDUs); all co-infected with HIV-1; aged ≥ 15 yearsDescription: Participants were randomly selected HIV-1 co-infected MSM and IDUs. Data were collected via structured face-to-face interviews using a pre-tested questionnaire, and blood samples were taken for HPgV RNA genotyping.Setting: In-person (Guangdong Dermatology Hospital, China)Men who have sex with menGuangdong Dermatology Hospital, ChinaNo information providedN/A3/5592021Usman et al. [110]PakistanTo evaluate how acceptable oral PrEP is among MSM and transgender women (TW) in PakistanDesign: Quantitative (observational cross-sectional study)Participants: 347 MSM and TGW; aged over 13 years; HIV negativeDescription: A structured, pre-tested online questionnaire administered among MSM and TW in Pakistan.Setting: Online1) Men or transgender2) Have sex with other man/TGW1) Snowball sampling2) Community groups on Facebook and Instagram 3) Community-based organizations (CBOs)No information providedN/A3/5602018Wang et al. [111]ChinaTo examine social norm patterns and condom-use self-efficacy among Chinese MSM, and analyze their relationship with consistent condom use across partner typesDesign: Quantitative (observational cross-sectional study)Participants: N = 1,597 MSM; aged ≥ 16 yearsDescription: Description: Online questionnaire covered socio-demographics, consistent condom use, condom use social norms, and self-efficacy.Setting: Online1) Male at birth2) Engaged in anal sex with a man at least once during their lifetime1) Danlan.org – the largest online platform serving the gay community in China2) Associated digital platforms including the Blued dating app, as well as social media channels like Weibo and WeChatNo information providedN/A3/5612018Wu et al. [112]ChinaTo investigate how MSM looked at HIV and investigate the psychometric properties of the Chinese IPQ-RDesign: Quantitative (observational cross-sectional study)Participants: N = 225 MSM living with HIV; aged ≥ 16 yearsDescription: Structured questionnaire administered through face-to-face interviews by trained peer interviewersSetting: In-person (community organizations)1) Male2) Reported having had anal sex with at least one man in the last 12 monthsRecruited and distributed via outreach lists maintained by CBOs, which had prior service engagement with MSM living with HIVMonetary incentives (7.8)N/A3/5622016Ybarra et al. [[113](#CR113)]USATo reflect on ethical considerations encountered during the implementation of Guy2Guy, a text-based HIV prevention and sexual health program, within an RCT involving sexual minority male adolescentsDesign: Quantitative (Experimental, RCT)Participants: *N* = 302 sexual minority males; aged 14–18 yearsDescription: Self-administered online questionnaires and follow-up surveys; intervention involved “Guy2Guy” – a text messaging–based HIV prevention and healthy sexuality programSetting: Online1) Male at birth/cisgender male2) Self-identified as gay, bisexual, or queerOnline social media advertisementsElectronic gift card (45)N/A4/5632016Zhao et al. [114]ChinaTo assess how common recreational drug use is and examine links between poppers use and HIV/STI testing history, use of gay dating apps, and sexual behaviorsDesign: Quantitative (observational cross-sectional study)Participants: N = 1,424 MSM; age ≥ 16 yearsDescription: Data were collected via a self-administered online questionnaire covering drug use, sexual behaviors, app use, HIV/STI testing, and demographics.Setting: Online1) Male at birth2) Have sex with other menRecruited via gay community websites and other online platforms.No information providedN/A3/5642012Zhao et al. [115]ChinaTo assess the seroprevalence of HCV, HBV, and syphilis, and identify associated risk factors among HIV-1-infected individuals in Shandong, China, using data from participants tested between 2000 and 2010Design: Quantitative (observational cross-sectional study)Participants: N = 2087 HIV-positive patients; aged 1–84 yearsDescription: Trained medical staff administered a standardized questionnaire on demographics and risk behaviors, and collected blood samples for STI testing (hepatitis B, C, and syphilis) after HIV diagnosisSetting: In-person (multiple sites under the supervision of the Shandong Provincial Center for Disease Control and Prevention (CDC), China)Men who have sex with menHIV-positive individuals confirmed by the Shandong CDC between 2000 and 2010.No information providedN/A4/5652023Zucchi et al. [116]BrazilTo examine legal and ethical issues surrounding adolescent involvement in HIV research and how these may impact their best interestsDesign: Quantitative (observational cross-sectional study)Participants: N = 347 MSM and TGW; aged 15–17 yearsDescription: Analyzed ethical and legal barriers to enrolling adolescents (15–17) in a Brazilian PrEP project, using ethics reviews, court rulings, and participant data to assess impacts of parental consent requirements on inclusion of vulnerable youth.Setting: In-person (Public health services in three major Brazilian cities—São Paulo, Salvador, and Belo Horizonte)1) Male2) Engage in sexual activity with other malesRecruited in person through public health services in São Paulo, Salvador, and Belo Horizonte.No information providedN/A5/5^a^Study objectives are based upon the information gathered from selected studies^b^Since the definition of MSM from selected studies may differ, the definition of MSM from each are provided^c^Cohort retention means strategies for each selected study to retain participants for the longitudinal research
Only five studies specifically focused on minors MSM living with HIV. These were conducted in three countries: two in the United States [63, 98], two in China [112, 115], and one in France. The studies from the United States explored the relationship between healthcare access and HIV infection, including missed opportunities for HIV/STI testing [63], as well as the association between incarceration and transactional sex among HIV-positive YMSM [98]. The studies from China examined various health concerns, such as attitudes toward living with HIV [112] and the prevalence of co-infections like hepatitis B, hepatitis C, and syphilis [115]. The study in France focused on the distribution of HIV self-testing kits (HIVST) and the characteristics of both those who distributed and those who received them [72] (see Table 2).
Design and methodology of studies
Most studies (53 articles, 82%) were quantitative, which were divided into (a) 36 (55%) observational cross-sectional studies, (b) 8 (12%) observational longitudinal studies, most of which collected data via questionnaires, (c) 8 (12%) experimental/quasi experimental studies, the majority of which were HIV testing interventions (4 articles; 6%), HIV prevention (3 articles; 4%), PrEP (1 article; 1%) and (d) one case control study (1%). Aside from these quantitative studies, five qualitative studies (7%) related to HIV testing and HIV vaccines were also conducted. Furthermore, there were seven articles (10%) on PrEP, HIV testing, and HIV prevention that used mixed methods (See Table 2).
Online recruitment was mainly employed to access MSM minors through online platforms and applications [59, 67, 77, 79, 85, 87, 92, 96, 101, 104, 111, 113, 114], as well as through recruitment hotspots and drop-in centers located in public areas, including hospitals, health centers, and prisons. According to most studies, community networks, such as community-based organizations (CBOs), play a crucial role in helping researchers connect with MSM minors [52, 58, 60, 62, 72, 77, 81, 86, 89, 93, 95, 96, 100, 101, 110]. They also contribute significantly to public relations, dissemination of information, and improving accessibility to MSM minors, who are often regarded as a hard-to-reach and underserved population.
A total of 29 studies (43%) offered compensation in various forms, including gift cards, cash, online shopping gift codes, mobile top-ups, and online/VISA e-gift cards. Some studies increased compensation over time [58, 61, 101]. To attract more participants, additional compensation was provided to those who invited others to join the project [61, 64, 90]. In a PrEP study conducted in the USA, the maximum compensation for each participant was a mobile phone top-up valued at 75 [[77](#CR77)]. Furthermore, participants in a study examining the relationship between internalized homophobia, substance use, and condomless sex in the USA received monetary incentives that started at 70 at baseline, with an additional 45 given at each follow-up [[101](#CR101)]. Most compensation ranged from 25 to $30 (See Table 2).
Quality assessment
The majority of studies were rated as moderate quality (91%), with 6% rated as high quality, and no studies were classified as low quality. All qualitative studies were rated as high quality (100%), while all quantitative descriptive studies were rated as moderate quality (100%). Frequent methodological limitations contributing to the moderate rating included challenges related to sample representativeness and nonresponse bias. For mixed methods studies, all (100%) were rated as moderate quality, primarily due to limited reporting on how inconsistencies between quantitative and qualitative data were addressed. In quantitative non-randomized studies, 91% were rated as moderate, largely due to unclear reporting of blinding procedures for outcome assessors (see Table 3).
Table 3. Study design and quality assessment (MMAT)Study DesignLow Quality (n)Moderate Quality (n)High Quality (n)Total (n)1. Qualitative552. Quantitative Randomized Control (Trials)443. Quantitative non-randomized111124. Quantitative Descriptive37375. Mixed Methods77Total059665
Consent/assent process
In this review and section, we distinguished between assent, an ethical process specific to minors, and standard consent procedures for adults, as well as studies that applied both. We also considered cases involving parental or guardian permission or proxy decision-makers. Table 1 summarizes the definitions, strengths, and limitations of each consent and assent model. Details of how each study applied these approaches are presented in Tables 4 and 5. The findings under the Consent/Assent Process section are presented in three parts: (1) Consent processes (2) Assent processes and (3) Parental permission processes.
Table 4. Details of the consent/assent processesNo.YearAuthorsAge of participantsConsent^c^Assent^d^Waiver of Parental permissionReasons for waiver requestGuardian InvolvementProxy involvementaAdditional protection activities^b^12015Alexander et al. [52]16–19Informed consentNoYesNo information providedNoNo1. Adolescents reviewed a simulated HIV vaccine trial consent form2. Research staff guided participants through key elements: purpose, procedures, risks, benefits, and compensation3. Participants were encouraged to ask questions as part of the standard consent process22010Azariah et al. [53]15–66Verbal informed consentNoNo information providedNo information providedNoNoNo32016Bares et al. [54]16–78Verbal informed consentNoNo information providedNo information providedNoNo1. The research team provided a patient education sheet explaining the rationale for HIV screening and associated risk factors2. The sheet included explanations for both positive and negative test results3. Contact information was included for the X-TLC program, as well as testing resources from the State of Illinois and the CDC42017Bartelsman et al. [55]16–81Written informed consentNoNo information providedNo information providedNoNoNo52010Begier et al. [56]16 upWritten informed consentNoNo information providedNo information providedNoNoNo62018Bhatia et al. [57]12 upConsentNoNo information providedNo information providedNoNoNo72018Bonett et al. [58]15–24Online informed consentNoNo information providedNo information providedNoNoNo82018Cao et al. [59]16–30Online informed consentNoNo information providedNo information providedNo information providedNo information providedNo92016Clerc et al. [60]16–80Verbal informed consentNoNo information providedNo information providedNoNoNo102019Closson et al. [61]16 upWritten informed consentNoNo information providedNo information providedNoNoNo112022Cordoba et al. [62]13–17Written informed assentYes (written informed assent)YesNo information providedNoNoSome state policy explicitly included HIV testing among STI service available to minors without parental permission122011Dorell et al. [63]16–25Written informed consentNoNo information providedNo information providedNoNoNo132017Duan et al. [64]16–79Written informed consentNoNo information providedNo information providedNoNoNo142016Fisher et al. [65]14–17Verbal consentNoYesNo information providedNoNoNo152018Fisher et al. [66]14 upIndependent consentNoYesNo information providedNoNoNo162020Fisher et al. [67]14–19Online informed consentNoYesNo information providedNoNoNo172022Folayan et al. [68]13–72Online informed consentYesYesNo information providedNo information providedNo information providedNo182021Fongkaew et al. [69]16–20Written informed consentNoNo (provided parental consent)NoYesNoNo192018Frye et al. [70]16–29Written informed consentYes (Written informed assent)No information providedNo information providedNoMinor advocate1. Participants under 18 were considered mature minors and provided written informed assent2. Before assent, each minor met with a minor advocate—a neutral staff member not involved in the study3. The advocate’s role was to support the minor; discussions were confidential and not shared with study staff202014Godbole et al. [71]15–49Written informed consentYes (Written informed assent)No information providedNo information providedNoNoNo212022Gosset et al. [72]15 or olderOnline informed consentNoNo information providedNo information providedNo information providedNo information providedNo222015Hadland et al. [73]14–26Written informed consentNoYesNo information providedNo information providedNo information providedNo232017Hammoud et al. [74]16–81Online informed consentNoNo information providedNo information providedNoNoNo242018He et al. [75]16 upWritten informed consentNoNo information providedNo information providedNoNoNo252017Hogg et al. [76]14–19Online informed consentNoNo information providedNo information providedNo information providedNo information providedNo262017Hosek et al. [77]15–17Written informed consentNoYesNo information providedNoNoNo272023Huang et al. [78]16 or olderConsentNoNo information providedNo information providedNo information providedNo information providedNo282019Jin et al. [79]16 upOnline informed consentNoNo information providedNo information providedNoNoNo292023Kaufman et al. [80]15–24Written informed consentNoNo information providedNo information providedNo information providedNo information providedNo302022Knopf et al. [81]14–17Online informed consentNoYesNoNo information providedNo information providedNo312017Knopf et al. [82]17–25Online informed consent/Verbal informed consentNoNo information providedNo information providedNoNo1. Used Likert-type questions to evaluate the consent process2. Measured how informed participants felt3. Assessed perceived support during decision-making4. Evaluated whether participation was voluntary322020Kumar et al. [83]15 upWritten informed consentNoNo information providedNo information providedNoNoNo332014Lally et al. [84]16–19Online informed consentNo information providedYesThis study as participation included only minimal riskNo information providedNo information providedNo342017Li et al. [85]16 or olderOnline informed consentNoNo information providedNo information providedNo information providedNo information providedNo352015Mahapatra et al. [86]15–49Written informed consentYes (Written informed assent)No (consent from the next to kin, caretakers, or guardian on behalf of the minors)NoGuardianKin, CaretakersNo362018Mao et al. [87]16 or olderOnline informed consentNoNo information providedNo information providedNo information providedNo information providedNo372022Marchant et al. [88]18–59ConsentNoNo information providedNo information provideNo information provideNo information provideNo382021Mata et al. [89]14–17Online informed consentYesYesNo information providedNo information providedNo information providedNo392020Michel et al. [90]16–24Written informed consentNoNo information providedNo information providedNoNoNo402017Mustanski et al. [91]14–17Online informed consentYes (Online inform consent)YesIRBs can approve waivers of parental permission requirements when studies are not otherwise feasible or when parental permission may not protect the adolescents. Adolescents’ perspectives represent a critical lens through which to examine these issues.No information providedNo information providedNo412020Nelson et al. [92]14–17Online informed consentNoYesNo information providedNoNo1. Capacity to consent assessed using four comprehension questions2. Questions covered study procedures, risks, and benefits3. Participants had up to three attempts to answer correctly4. Those unable to answer all correctly were deemed ineligible422019Nelson et al. [93]16 upWritten informed consentNoNo information providedNo information providedNoNoNo432017Osorio et al. [94]13–64Verbal informed consentNoNo information providedNo information providedNoNoNo442013Ott et al. [95]16–19Written informed consentNoYesNo information providedNoNo452019Pan et al. [96]16 upOnline informed consentNoNo information providedNo information providedNoNoNo462020Peuchant et al. [97]17–69written informed consentNoNo information providedNo information providedNoNoNo472018Philbin et al. [98]13–24Written informed consentNoNo information providedNo information providedNo information providedNo information providedNo482021Phillips et al. [99]16 or olderOnline informed consentNoNo information providedNo information providedNo information providedNo information providedNo492013Pollard et al. [100]16–65No information providedNoNo information providedNo information providedNo information providedNo information providedNo502017Puckett et al. [101]16–20Informed consentYes (Informed assent)YesNo information providedNoNoNo512020Rendina et al. [102]13 or oderOnline informed consentYesYesNo information provideNo information provideNo information provideNo522021Rice et al. [103]16–24ConsentNoNo information providedNo information providedNo information providedNoNo532022Rodger et al. [104]16 or olderOnline informed consentNoNo information providedNo information providedNoNoNo542023Schnall et al. [105]14–21Online informed consentYesNo (parental e-consent)No information providedNo information providedNo information providedNo552019Smith et al. [106]16 or olderConsentNoNo information providedNo information providedNo information providedNo information providedNo562023Soares et al. [107]15–19Written informed consentYes (Written)YesNo information providedNo information providedNo information providedNo572023Sullivan et al. [108]16 or olderWritten informed consentNoNo information providedNo information providedNo information providedNo information providedNo582019Taklual et al. [109]15 or olderWritten informed consentNoNo information providedNo information providedNo information providedNo information providedNo592021Usman et al. [110]18–67Online informed consentNoNo information providedNo information providedNoNoNo602018Wang et al. [111]16 or olderOnline informed consentNoNo information providedNo information providedNo information providedNo information providedNo612018Wu et al. [112]16 upWritten informed consentNoNo information providedNo information providedNoNoNo622016Ybarra et al. [113]14–18Informed consentYes (Informed assent)YesNo information providedNoNo1. Enrollment conducted via phone to assess minors’ understanding of assent.2. Assent form written in simple, age-appropriate language; capacity to consent assessed to ensure understanding of risks and voluntariness.3. Waiver of parental permission obtained from both IRBs due to minimal risk and sensitivity of the study.4. Self-safety assessment developed to help youth evaluate whether it was safe for them to participate.5. Step-by-step privacy instructions provided (e.g., setting a phone password) to enhance participant confidentiality.632016Zhao et al. [114]16 or olderWritten informed consentNoNo information providedNo information providedNo information providedNo information providedNo642012Zhao et al. [115]1–84Informed consentNoNo information providedNo information providedQuestionnaires were completed by guardians for participants with developmental, physical, or cognitive limitationsNoNo652023Zucchi et al. [116]15–17ConsentYesNo (parental consent were adopted across sites)No information providedNo information providedNo information providedNo^a^Proxy involvement refers an adult person that is not a legal guardian to give permission and helps minors make decisions^b^Additional activities are organized in selected HIV research studies to protect minors, minimize harms, prevent risk, and protect their rights^c^Informed consent as stated in the paper ^d^Informed assent as stated in the paper
Table 5. Summary table of consent and assent practices (n = 65 studies)Consent/Assent PracticeNumber of StudiesReferencesReported use of any informed consent process64[52–116] exclude [100]Used online consent forms22[58, 67, 68, 72, 74, 76, 79, 81, 82, 84, 85, 87, 89, 91, 92, 96, 99, 102, 104, 105, 110, 111]Did not distinguish between minors and adults in consent51[52–116] exclude [62, 68, 70, 71, 86, 89, 91, 100–102, 105, 107, 113, 116]Used comprehension questions check as part of consent1[92]Used participant-centered tools (e.g., safety self-assessments)2[82, 113]Included pre-participation discussions1[54]Reported a distinct assent process for minors13[62, 68, 70, 71, 86, 89, 91, 101, 102, 105, 107, 113, 116]Used written assent forms4[62, 70, 71, 107]Included minor-specific protections (e.g., simplified language, privacy tools)3[70, 92, 113]Involved minor advocates1[70]Reported waiver of parental permission18[52, 62, 65–68, 73, 77, 81, 84, 89, 91, 92, 95, 101, 102, 107, 113]Provided justification for parental permission waiver2[84, 91]Required parental permission3[69, 86, 116]Mentioned guardian or kin involvement1[86]Reported variation in parental permission by region1[116]
Consent processes
Out of all 65 studies reviewed, 64 reported implementing a consent process. Among these, 22 studies employed an online form of informed consent [58, 67, 68, 72, 74, 76, 79, 81, 82, 84, 85, 87, 89, 91, 92, 96, 99, 102, 104, 105, 110, 111]. In most studies, the consent process was presented collectively for all participants, with no clear distinction between adults and minors. Furthermore, a distinct procedure for obtaining assent from minors was typically not described; rather, studies generally reported that consent had been obtained from all participants.
However, one study [92] required participants to complete a comprehension questionnaire prior to enrollment. Participants had to answer all questions correctly, and those who failed to do so three times were deemed ineligible to participate. This study included a process specifically designed for minors, as all participants were under the age of 18. Two studies also introduced participant-centered tools, such as self-safety assessments, to enhance informed decision-making [82, 113]. Additionally, some studies offered pre-participation discussion sessions, allowing potential participants to reflect on the study’s details before providing consent [54] (See Tables 4 and 5).
Assent processes
Only thirteen studies involving minors under the age of 18 included an assent process [62, 68, 70, 71, 86, 89, 91, 101, 102, 105, 107, 113, 116]. Four of these used written informed assent [62, 70, 71, 107], and three studies [70, 92, 113] applied a distinct and protection process specifically designed for minors. Innovative strategies were identified in some studies to support minor participants’ autonomy and understanding. One study used simplified language and included a self-safety assessment, along with instructions on configuring phone security settings to promote participant safety and privacy [113]. In another study, minor advocates were engaged to support MSM minors under 18, minor advocates were not part of the research team and served as intermediaries to address participants’ concerns confidentially before enrollment [70] (See Tables 4 and 5).
Parental permission processes
Out of 65 studies, a waiver of parental permission was explicitly reported as required in only eighteen studies [52, 62, 65–68, 73, 77, 81, 84, 89, 91, 92, 95, 101, 102, 107, 113]. Only two studies provided justifications for requesting a waiver of parental permission—one citing minimal risk [84], and the other emphasizing the protection of minors [91].
Out of the 65 studies, only three required parental permission. These include a qualitative study that developed and evaluated a participatory sexual health program tailored to the needs of YMSM in Thailand [69], and a qualitative study conducted in India that explored the experiences and challenges faced by young MSM in accessing sexual and reproductive health services. Notably, only this study [86] explicitly mentioned the involvement of kin, caretakers, or guardians acting on behalf of minors. In addition, one quantitative study [116] examined the ethical and legal challenges of providing daily oral PrEP to adolescent MSM and transgender women aged 15–19 in Brazil. This study involved both quantitative data analysis and an in-depth review of decisions made by research ethics committees across different regions. Interestingly, the requirement for parental permission varied by location—some regions mandated it, while others granted a waiver, allowing adolescents to participate independently (See Tables 4 and 5).
Discussion
This review highlights key limitations in the ethical reporting of HIV research involving MSM minors. Most studies were conducted in high-income countries, particularly the United States, with little representation from low-income settings. This imbalance may reflect disparities in research infrastructure, legal constraints, or funding priorities, which have been similarly noted in prior reviews on adolescent research ethics [118]. In addition, sociocultural stigma [36, 119], criminalization of same-sex relationships [29], and heightened ethical and regulatory barriers to enrolling sexual minority minors may further limit research conducted in low-income settings. Notably, only three studies focused specifically on MSM minors living with HIV, despite growing evidence that this group experiences unique barriers to care, support, and participation in research [120].
The reviewed studies were predominantly quantitative and observational, with most using convenience sampling via social media or community venues. While these methods can facilitate access to hidden populations, they may underrepresent MSM minors who are most marginalized or disengaged from services [121]. A minority of studies used experimental designs or qualitative methods, and few clearly described peer referral processes or safeguards. Although 43% of studies reported offering incentives, few explained how these were delivered or ethically justified. This lack of detail raises concerns about potential undue influence, particularly among minors who may be economically or socially vulnerable. In such contexts, incentives may support recruitment but could also compromise voluntary participation if decision-making capacities are still developing [122].
The limited reporting on informed assent is particularly striking. Only thirteen studies explicitly mentioned an assent process for minors, and even among those, few tailored the process to age or developmental stage. This echoes findings by Soll et al. (2020) [118], who noted a similar lack of attention to assent procedures in adolescent health research. Despite ethical guidelines recommending that minors be given age-appropriate opportunities to provide informed agreement to participate (CIOMS, 2016) [123], our review suggests this standard is often underreported, if not entirely overlooked.
Furthermore, variability in how studies navigated parental permission, such as through formal waivers, proxy consent, or omission of detail, reflects broader inconsistencies in ethical oversight. For example, while 18 studies mentioned receiving IRB-approved waivers of parental permission, few explained the rationale or described how MSM minors were otherwise protected. These patterns may stem from ambiguous regulatory guidance, legal uncertainty surrounding minors’ autonomy, or assumptions that standard adult procedures suffice [124, 125].
Many studies applied consent procedures to minors similarly to adults, despite ethical guidelines recommending additional protections and the inclusion of assent for minors. However, only a limited number of studies provided detailed descriptions of how assent was obtained, which constrains transparency and limits opportunities for methodological learning or replication. This pattern suggests that minors’ perspectives and decision-making roles may not always be explicitly foregrounded in reporting practices. Existing literature highlights that well-designed assent processes can support trust, shared understanding between researchers and participants, and minors’ capacity to make informed decisions about research participation [126, 127]. Existing literature has suggested that assent may be appropriate for children as young as 10 years of age, depending on developmental capacity and context [128]. In digital research settings, interactive approaches such as question-and-answer formats have been proposed to enhance minors’ understanding of study procedures, risks, benefits, and their right to withdraw [45]. Ethical guidance further emphasizes the importance of age-appropriate language, sufficient time for comprehension, and context-sensitive protections when conducting research with minors [45, 129, 130]. Nevertheless, relatively few studies in this review reported implementing or describing such tailored approaches in detail [54, 70, 82, 92].
Nearly half of the studies included in this review (43%) reported providing compensation to participants, with amounts ranging from 75. Some studies also mentioned additional incentives for peer referrals. This observation raises potential ethical considerations, particularly in studies involving MSM minors. While compensation may encourage participation and help reduce dropout rates, especially among youth who are economically or socially marginalized, it may also raise concerns about undue influence, depending on the context. In HIV research, where participants may experience intersecting vulnerabilities related to stigma, economic disadvantage, and limited legal protections, the use of incentives calls for careful ethical reflection. Ensuring that participation is both voluntary and informed is essential, and compensation should not compromise participants’ ability to assess personal risks. This consideration is especially relevant for minors, whose autonomy and decision-making capacity are still developing. Some literature has noted that adolescents may perceive incentives differently depending on their individual circumstances; some may find them supportive, while others may feel uncertain or pressured [122]. In this review, few studies provided detailed descriptions of how incentives were presented within consent or assent procedures. Greater clarity in future reporting could support transparency and assist researchers and ethics committees in considering context-sensitive approaches.
Why is assent missing? While assent procedures were present in some studies, they were reported inconsistently and often lacked sufficient detail. This pattern suggests that the role of assent may be underreported or de-emphasized in published HIV research involving minors. Researchers working with vulnerable minors may encounter practical challenges when navigating ethical frameworks that vary across settings and are sometimes perceived as unclear or inconsistently applied [116]. Such variability may reflect efforts to maintain flexibility and allow for cultural and social sensitivity. At the same time, the limited reporting of assent procedures may also reflect cautious approaches to participant protection, potentially influenced by institutional or regulatory considerations. This observation raises an ethical question regarding how IRBs balance the protection of vulnerable participants with respect for minors’ emerging autonomy. This issue remains insufficiently examined in the current literature [116]. Additionally, a substantial proportion of the reviewed studies did not provide detailed descriptions of consent and assent procedures, which limits transparency and comparability across studies. This pattern may reflect assumptions that assent procedures are embedded within local ethical or cultural contexts, or that IRB approval implies adequate ethical oversight without the need for further reporting. Alternatively, authors may assume that such procedures are widely understood and therefore do not require explicit description. These possibilities highlight a gap in empirical reporting rather than definitive conclusions about intent or ethical commitment. Addressing the persistent lack of detailed reporting on assent procedures may therefore require broader, coordinated efforts, including international collaboration and shared ethical dialogue among researchers, ethics committees, and journal editors.
Strengths and limitations
This systematic review found that one in five studies involving MSM minors reported an assent process. This reporting gap highlights the need for clearer expectations in adolescent HIV research. To promote ethical rigor and transparency, journals and ethics committees should require explicit reporting of assent and consent methods. Addressing this gap can improve protections for adolescent participants and foster shared standards across research contexts. However, this study has several limitations. The search was conducted in only three databases and focused solely on English-language studies, which may have limited the comprehensiveness of the findings and introduced language bias. In addition, the search terms focused on MSM under the age of 18 years, meaning studies that did not explicitly state the inclusion of this group may have been missed. The review also excluded grey literature and unpublished materials, including internal IRB documents, which restricts the ability to fully assess ethical practices, particularly in settings where such information is not publicly accessible. Moreover, reporting on assent procedures was often limited or inconsistent across the included studies, which may have led to an underestimation of existing ethical practices that were implemented but not described in the published articles. Finally, most of the reviewed studies were conducted in high-income countries, limiting the generalizability of the findings to lower- and middle-income settings, which were underrepresented in this review. Developing an evidence base in these settings remains a critical priority.
Conclusion
These findings underscore significant gaps in research on HIV among MSM minors, particularly in low-income countries. Moreover, consent and assent processes were often reported with limited clarity, blurring distinctions between procedures for MSM minors and those aged 18 years and older. This lack of transparency may contribute to assumptions that identical consent procedures apply to both groups, despite important ethical differences. The limited and inconsistent reporting of assent procedures may reflect challenges related to ethical documentation, variability in legal frameworks, cultural norms surrounding minors, or differing IRB requirements across settings. As a result, assent procedures may be underreported or insufficiently described in published studies, rather than entirely absent. Given that only one in five studies involving MSM minors reported an assent process, this gap presents an opportunity for researchers, IRBs, and journal editors to strengthen transparency, promote shared ethical understanding, and support assent practices that appropriately respect both the protection and emerging autonomy of MSM minors in HIV research.
To promote ethical integrity and transparency in HIV research involving MSM minors, the following recommendations may be considered:
- Clearly report consent and assent procedures to support transparency and shared learning. Describe how minors were informed, how consent/assent was obtained, and whether waivers or proxies were used. Detailed reporting allows future researchers to build upon ethical practices in diverse contexts.
- Include underrepresented populations. Prioritize MSM minors living with HIV and those from under-resourced or legally restrictive environments to address research gaps.
- Tailor assent procedures to age and cultural context. Ensure that processes reflect minors’ developmental maturity and are sensitive to local norms.
- Use accessible, age-appropriate language. Design study materials that are clear and understandable for youth participants.
- Provide adequate time for questions and decisions. Allow minors space to process information and ask questions before enrolling.
- Justify the use of incentives. Clearly explain the rationale, method of delivery, and safeguards to ensure that incentives do not compromise voluntary participation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Global Fund. Results Report 2025. https://www.theglobalfund.org/en/results/. Accessed 25 January 2026.
- 2UNAIDS. UNAIDS calls for greater and sustained funding commitments to support its work in leading global efforts to end AIDS by 2030 n.d. https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2021/november/20211119_funding-dialogue. Accessed 25 January 2026.
- 3CDC. CDC awards $117 Million to Advance Innovation and Health Equity in Federal Initiative to End HIV 2021. https://archive.cdc.gov/www_cdc_gov/media/releases/2021/p 0727-end-hiv.html. Accessed 25 January 2026.
- 4CDC, CDC's HIV, Viral Hepatitis, STD, and Tuberculosis Prevention Budget 2024. https://www.cdc.gov/nchhstp/budget-funding/index.html. Accessed 25 January 2026.
- 5The U.S. Department of Health and Human Services. Funding Opportunities n.d. https://www.hiv.gov/topics/funding. Accessed 25 January 2026.
- 6Marshall A, Cahill S. Barriers and opportunities for the mental health of LGBT older adults and older people living with HIV: a systematic literature review. Aging Ment Health. 2021;1–10. 10.1080/13607863.2021.2003300.10.1080/13607863.2021.200330034784488 · doi ↗ · pubmed ↗
- 7UNFPA. HIV & AIDS. United Nations Population Fund 2016. https://www.unfpa.org/hiv-aids. Accessed 25 January 2026.
- 8Missing men living with HIV n.d. https://www.unaids.org/en/resources/presscentre/featurestories/2022/january/20220124_missing-men-living-with-hiv. Accessed 25 January 2026.