Ultrasound-Guided Regional Anesthesia: A Narrative Review of Techniques, Safety, and Clinical Applications
Fadi A Jamaleddin Ahmad, Joshua A Herrera, Joanna M Saldanha, Akbar Khan, Waleed Nasir, Miriam L Otim, Asjad Y Amin, Nosakhare R Asemota, Sadiq Bhadmus, Farah AlShammari, Aditya Vikkiraman, Izatullah Kamran

TL;DR
This review explores how ultrasound-guided regional anesthesia improves pain management by making nerve blocks safer, more accurate, and effective, while reducing opioid use and recovery time.
Contribution
The paper highlights recent advancements in UGRA techniques, including the use of additives and AI, to improve safety and efficacy in clinical settings.
Findings
UGRA reduces opioid consumption and speeds up post-surgery recovery by improving the accuracy of nerve blocks.
Real-time imaging and updated protocols help minimize risks like nerve damage and toxicity.
AI and robotics in UGRA enhance precision and may increase the standardization and accessibility of the technique.
Abstract
Ultrasound-guided regional anesthesia (UGRA) has changed how we manage pain by allowing doctors to visualize nerves and other structures in real time, making the process more accurate, effective, and safe while also reducing risk. This narrative review examines the latest advancements in UGRA techniques, evaluating their efficacy and safety, particularly for peripheral nerve and truncal plane blocks, their potential to diminish opioid consumption, and their clinical applications in perioperative care. This review followed the Scale for the Assessment of Narrative Review Articles (SANRA) quality assessment guidelines and searched six databases for studies published from January 2015 to October 2025, including trials, meta-analyses, cohort studies, reviews, and technical reports. This review aims to give doctors, anesthesia experts, and researchers the newest information and methods about…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
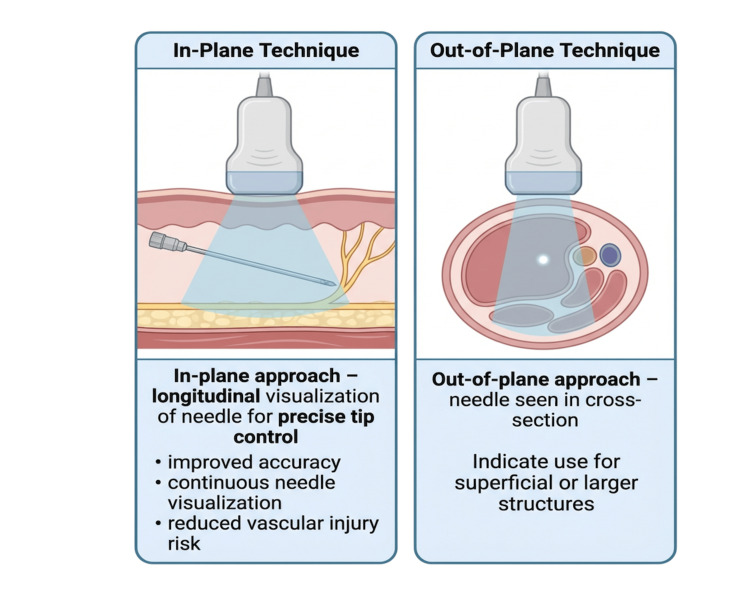 Figure 1
Figure 1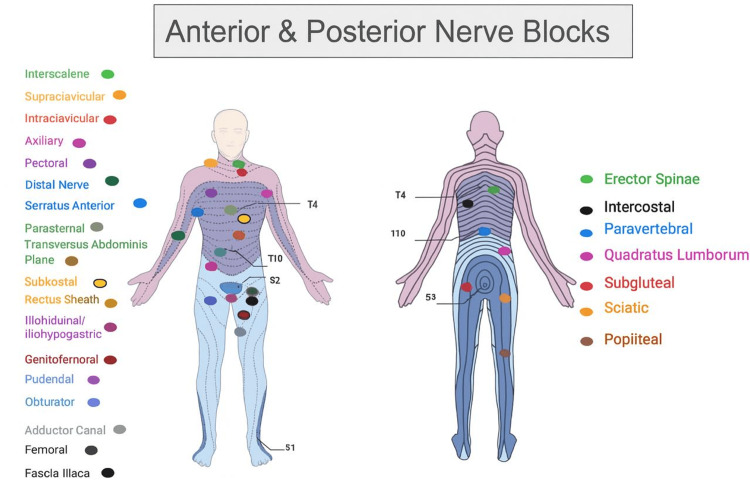 Figure 2
Figure 2| Category | Description |
| Study design | Narrative review |
| Objective of the search | To summarize current evidence on ultrasound-guided regional anesthesia (UGRA), including techniques, pharmacology, safety, complications, and emerging technologies |
| Databases searched | MEDLINE (PubMed), Embase (Ovid), Cochrane Library, Web of Science, Google Scholar |
| Time period covered | January 2015 to October 2025 |
| Search strategy | Database-specific adaptations of structured search strings using MeSH terms and keywords |
| Key search terms | “Ultrasonography,” “ultrasound-guided,” “regional anesthesia,” “nerve block,” “peripheral nerve block,” “analgesia,” “local anesthetic,” “opioid,” “postoperative pain,” “complications,” “local anesthetic systemic toxicity,” “needle visualization,” “block safety” |
| Inclusion criteria | Human studies; adult and pediatric populations; clinical trials; observational studies; systematic reviews; meta-analyses; technical reviews; and case reports related to UGRA |
| Exclusion criteria | Non-English publications; animal or cadaveric studies; abstracts without full text; studies not focused on ultrasound-guided techniques |
| Rationale for inclusion approach | Broad inclusion is used to capture the multidisciplinary and evolving nature of UGRA across clinical practice |
| Study selection process | Titles and abstracts screened by authors; relevant full texts reviewed for inclusion |
| Nature of review | Narrative review (not a systematic review or meta-analysis) |
| Rationale for narrative design | Heterogeneity in study design, outcomes, and evolving technologies precluded quantitative synthesis; the narrative approach allowed clinical integration |
| Methodological limitations | Potential publication bias, exclusion of non-English studies, lack of formal risk-of-bias assessment, and variability among included studies |
| Criterion | Score (0–2) | Brief justification |
| Justification of importance | 2 | Clearly establishes the clinical relevance and timeline of UGRA innovations. |
| Statement of aims | 2 | Objectives clearly defined: Evidence, methodology, and uses of UGRA (2015-2025). |
| Literature search | 1 | Six databases, transparent inclusion/exclusion criteria. |
| Referencing | 2 | 139 current and relevant sources up to 2025, correctly formatted. |
| Scientific reasoning | 1.5 | Logical synthesis but lacks bias assessment or quantitative pooling. |
| Presentation of data | 1.5 | Well-structured with tables/figures; lacks formal grading of evidence. |
| Total score | 10/12 | Excellent-quality narrative review with minor methodological limitations. |
| Probes | Shape | Depth | Application |
| Linear array | Rectangular-shaped & flat | High frequency, ranging from 3 MHz to 19 MHz & penetrates to a depth of up to 10 cm | Visualize superficial structures & help with the administration of superficial regional anesthesia |
| Phased array | Square-shaped & small | Low frequency, ranging from 1 to 5 MHz | Visualize a single point (e.g., ribs) by directing the beams to a single point in proximity |
| Curvilinear array | Curved & not flat | Low frequency, ranging from 1 to 5 MHz, and penetrates up to 30cm in depth | Visualize deep structures (e.g., transabdominal ultrasounds) |
| Agent | Block Type | Recommended dosage | Onset | Effects of toxicity |
| Ropivacaine | US-guided median nerve block (trigger thumb) | ED₅₀: 0.9 mL (1–3 years), 1.4 mL (3–6 years); ED₉₅: ~1.5–1.7 mL (0.2%) | Minutes | No adverse events reported at these doses |
| Levobupivacaine | US-guided TAP block | 0.2% at 0.2 mL/kg or 0.1% at 0.4 mL/kg (~0.4 mg/kg), adults only | Tmax ~17 min | Median peak plasma ~0.315 µg/mL; no toxicity observed |
| Ropivacaine | US-guided TAP block (lower abdominal surgery) | ~150–200 mg total dose (adult; weight-dependent; ≤3 mg/kg) | Peak plasma ~30 min | Mean peak plasma ~2.54 µg/mL; unbound ~0.14 µg/mL; no clinical toxicity |
| Bupivacaine | US-guided axillary brachial plexus block | 0.25–0.375% bupivacaine ± epinephrine; ~3–5 mL per nerve (adults) | ~10–20 min; duration ~4–12 h | Serum levels may approach toxic thresholds with high-volume dosing; adherence to weight-based dosing reduces risk |
| Adjuvant | Dose/route | Effect on block duration | Mechanism & benefit | Risks |
| Dexamethasone | 4–10 mg, perineural or IV | Prolongs by 4–8 hours | Anti-inflammatory, reduces nociceptive transmission | Neurotoxicity debated; perineural vs. IV efficacy similar in some studies |
| Dexmedetomidine | 0.5–1 µg/kg perineural | Prolongs duration, faster onset | α2-agonist causing vasoconstriction and sedation | Bradycardia, sedation, hypotension |
| Clonidine | ~1–2 µg/kg or fixed dose | Moderate prolongation | α2-agonist | Sedation, hypotension; less potent than dexmedetomidine |
| Epinephrine | 5 μg/mL | Slight prolongation | Vasoconstriction, a marker for intravascular injection | Possible ischemia in end-arterial areas |
| Step | Action/Recommendation | Details/Notes |
| 1. Stop injection | Discontinue the local anesthetic immediately | Request assistance and prepare for emergency management |
| 2. Airway & oxygenation | Prioritize airway management and provide supplemental oxygen | Prevent hypoxia and acidosis, which exacerbate LAST |
| 3. Seizure control | Administer benzodiazepines or propofol | Use propofol only if cardiovascularly stable |
| 4. Lipid emulsion therapy (ILE) | Initiate 20% lipid emulsion | Bolus: 1.5 mL/kg over 2–3 min. Infusion: 0.25 mL/kg/min & repeat as needed; continue for ≥10 min after hemodynamic stabilization |
| 5. Avoid substitutes | Do not use propofol in place of ILE | Propofol has insufficient lipid content and a higher risk of adverse effects |
| 6. Cardiovascular support (Modified ACLS) | Manage cardiovascular collapse per advanced cardiac life support (ACLS) with modifications | Avoid: vasopressin, calcium channel blockers, beta-blockers. Use low-dose epinephrine (<1 mcg/kg) to minimize worsening LAST |
| 7. Post-stabilization monitoring | Transfer to ICU for prolonged observation | Monitor for rebound toxicity as lipid emulsion is metabolized |
| Aspect | Summary | Key Points/Evidence |
| Nerve injury risk | Permanent neurological injury after UGRA is rare, reported at a 0.1–0.4% incidence. Risk increases with pre-existing neuropathies, advanced age, or connective tissue disorders. | Proper pre-procedural neurological exam and ultrasound-guided needle control are essential to reduce direct nerve trauma. |
| Patient-related risk factors | Conditions like diabetic or chemotherapy-induced neuropathy and Ehlers–Danlos syndrome heighten vulnerability to nerve injury. | Careful screening and documentation before the block are advised. |
| Intraneural injection | Previously avoided, but recent studies show low-pressure, subepineural injections may be safe under expert supervision. | Controlled intraneural techniques can enhance block efficacy but require awake or lightly sedated patients to detect paresthesia. |
| Injection pressure monitoring | High injection pressure (>15 psi) indicates needle misplacement (in fascicle, tendon, or vessel). Real-time pressure monitoring prevents intraneural injury. | Combining ultrasound visualization with pressure manometry forms a dual-safety approach. |
| Preventive strategies | Stop injection immediately if high resistance or pain occurs; reassess under ultrasound before resuming. | Reduces risk of neuropraxia and ischemic injury during peripheral nerve blocks. |
| Block | Description/Indications | Technique/Key Anatomy | Advantages/Considerations |
| Interscalene block (ISB) | Standard for postoperative analgesia after shoulder surgeries; targets superior trunk (C5–C6) of brachial plexus | Ultrasound-guided (UG) identification of anterior/middle scalene muscles and C5–C7 roots ("traffic light" sign); needle in-plane lateral-to-medial toward C5–C6 sheath; low volume (5–10 mL) reduces risk of hemidiaphragmatic paresis (HDP) | Excellent shoulder analgesia; risk of HDP, but ipsilateral extra-fascial injection reduces phrenic nerve involvement |
| Supraclavicular block (SCB) | “Spinal of the arm”; dense anesthesia for the upper limb (mid-humerus and below); ideal for trauma and emergency surgery | UG at supraclavicular fossa; use the first rib as a safety backstop; needle advanced lateral-to-medial toward plexus; subclavian artery and pleura as landmarks | Fast onset, comprehensive anesthesia; less phrenic nerve risk than ISB; pleural puncture avoided with correct technique; low volumes reduce HDP |
| Infraclavicular block (ICB) | For surgeries below the elbow; suitable for catheter placement for prolonged analgesia | Targets the brachial plexus cords around the axillary artery under the pectoral muscles; a single injection behind the artery or the costoclavicular approach for tighter cord packing | Long-lasting analgesia; low pneumothorax/phrenic risk; ideal for COPD/obese patients; continuous catheters stabilize well; costoclavicular variant provides faster onset |
| Axillary block | Distal brachial plexus block for forearm, wrist, and hand surgeries; ideal for outpatients and those with respiratory disease | Inject around the axillary artery to block the median, ulnar, radial, and musculocutaneous nerves; ultrasound-guided multiple injections improve efficacy | Safe (away from pleura/phrenic nerve); minimal respiratory risk; excellent for ambulatory settings; multiple injections yield better success |
| Distal nerve blocks (median, ulnar, radial, musculocutaneous) | Target individual nerves at the elbow/wrist for selective sensory anesthesia and motor preservation | UG injections (3–5 mL per nerve); typically used for precision procedures or rescue blocks | Motor-sparing; low anesthetic volume minimizes toxicity; superior to IV regional anesthesia for carpal tunnel; highly safe and targeted |
| Block | Description/Indications | Technique/Key anatomy | Advantages/Considerations |
| Paravertebral block (PVB) | Effective postoperative analgesia for thoracic & breast surgeries; blocks sympathetic & somatosensory signals for unilateral chest/abdominal pain | Inject local anesthetic near spinal nerves; the needle is advanced straight (no tilt) and redirected caudally to avoid pleural puncture | Safer than an epidural (less hemodynamic instability, nausea, urinary retention) |
| Erector spinae plane (ESP) block | For thoracic & abdominal somatic and visceral pain; also effective for acute and chronic cancer, acute pain | Inject local anesthetic into the fascia of the erector spinae near the transverse process (ultrasound-guided); spreads cephalocaudally to paravertebral/epidural/intercostal spaces | Simple, versatile, low complication rate; ~3.4 mL per dermatome |
| Pectoral nerve blocks (PECS I/II) | Analgesia for chest wall surgeries (e.g., mastectomy, axillary dissection, and port placement) | PECS I: Inject between pectoralis minor & major at the 3rd rib; PECS II: Between pectoralis major & serratus anterior | Blocks lateral & medial pectoral nerves; effective and easy with ultrasound |
| Serratus anterior plane block (SA) | For trauma (e.g., rib fractures) and thoracic wall pain | Inject LA between latissimus dorsi & serratus anterior, or beneath SA above intercostal muscles; identify thoracodorsal artery via Doppler | Blocks intercostobrachial, lateral cutaneous (T3–T9), long thoracic & thoracodorsal nerves |
| Intercostal nerve block (ICB) | Pain relief post-thoracic surgery & chest trauma | LA is injected into the intercostal space outside the parietal pleura at appropriate levels | Reduces respiratory complications; risk of systemic absorption causing hypotension/CNS effects; lasts 6–8 hours |
| Parasternal & interfascial plane blocks (PIFB, TTP) | Regional analgesia for chest wall pain (surgery, trauma, respiratory distress) | LA injected between muscles, not targeting anterior cutaneous branches; includes parasternal intercostal plane block | Good alternative to neuraxial blocks (paravertebral, epidural, spinal), especially in cardiac surgery or anticoagulated patients |
| Block | Description/Indications | Technique/Key anatomy | Advantages/Considerations |
| Transversus abdominis plane (TAP) blocks (subcostal, lateral, posterior) | Used for abdominal surgeries (laparoscopic cholecystectomy, hysterectomy, varicocelectomy, nephrectomy); reduces postoperative pain, opioid use, and nausea | Injection between internal oblique and transversus abdominis; variants: subcostal (upper abdomen), lateral (flank), posterior (near lumbar triangle) | Improves pain control, ambulation, and sleep; subcostal and combined approaches are superior to single TAP |
| Rectus sheath (RS) block | Used in hernia, abdominal, and prostate surgeries | LA injection into the posterior rectus sheath under ultrasound guidance, bilateral for midline incisions | Reduces pain, opioid use, nausea, and vomiting postoperatively; effective for both open and laparoscopic procedures |
| Quadratus lumborum (QL) blocks (QL1, QL2, transmuscular) | Used in abdominal, hip, and renal surgeries; also used for chronic pain relief | QL1: lateral (superficial to QL). QL2: posterior (between QL & thoracolumbar fascia). QL transmuscular: between QL & psoas major; ultrasound-guided | Provides visceral and somatic analgesia; long duration; effective for chronic and postoperative pain; combination with fascia iliaca block enhances recovery; comparable to epidural in pediatrics |
| Ilioinguinal/iliohypogastric (II/IH), genitofemoral (GF) & pudendal (PN) blocks | Used in unilateral hernia repair, prostatectomy, hemorrhoid repair, and urethroplasty; also for obstetric analgesia | II/IH: between the internal oblique and the transversus abdominis. Triple block: includes II/IH + GF + PNB: near ischial spine or transperineal; all under ultrasound guidance | II/IH is more effective than wound infiltration; triple block is superior to spinal alone; PNB improves pain scores vs. caudal and local infiltration and reduces opioid use and recovery time |
| Obturator nerve (ON) block (anterior & posterior approaches) | Prevents adductor jerk during transurethral resection of bladder tumor (TURBT); treats hip/knee pain and spasticity | Anterior: between adductor brevis & longus. Posterior: between adductor brevis & magnus; ultrasound or nerve stimulator guided | Using spinal and ONB nerve stimulators enhances surgical safety in TURBT, reduces spasm and pain, and provides safe and precise ultrasound-guided techniques for reflex inhibition. |
| Block | Description/Indications | Technique/Key anatomy | Advantages/Considerations |
| Femoral & fascia iliaca compartment blocks (emphasizing the suprainguinal approach) | Used for femoral neck fractures, hip arthroplasty, and revision surgeries; provides pre- and postoperative analgesia | Ultrasound-guided injection into the fascia iliaca compartment (suprainguinal approach improves spread to femoral and lateral femoral cutaneous nerves); often combined with spinal anesthesia | Effective analgesia, reduced opioid use, safe for elderly trauma patients; suprainguinal technique enhances block coverage, and may be an alternative to spinal morphine (needs further study) |
| Adductor canal (saphenous) block | Provides analgesia for knee and medial leg procedures such as total knee arthroplasty (TKA) | Ultrasound-guided injection into the adductor canal near the femoral artery under the sartorius blocks the saphenous nerve | Preserves quadriceps motor function; safer (low vascular puncture risk); excellent for early ambulation post-TKA |
| Sciatic nerve & ankle blocks (subgluteal, popliteal) | Analgesia for foot, ankle, and posterior leg surgeries; useful in pediatric patients for compliance and pain control | Ultrasound-guided at the subgluteal or popliteal level; for ankle block, targets tibial, deep/superficial peroneal, sural, and saphenous nerves | Effective perioperative analgesia: heating ropivacaine (30°C) accelerates onset and improves quality; duration similar to ankle block; enhances efficiency without added risk |
| IPACK & posterior knee analgesia strategies | Pain control after total knee arthroplasty (TKA); complements the adductor canal and femoral blocks | Injection between the popliteal artery and the posterior knee capsule (ultrasound-guided); ~20 mL ropivacaine is sufficient | Reduces opioid use; preserves motor function of tibial and peroneal nerves; comparable efficacy to suprainguinal fascia iliaca block; safe addition to multimodal analgesia |
| Step | Phase/Title | Key points |
| 1 | Preoperative planning & assessment | Evaluate the patient’s injuries, surgical type, and suitability for regional anesthesia, and educate the patient on ERAS expectations and pain management plan |
| 2 | Ultrasound-guided regional anesthesia (UGRA) | Identify the appropriate block for the surgical site, and prepare the POCUS setup for airway and vascular guidance |
| 3 | Intraoperative management | Administer multimodal analgesia (regional + non-opioid systemic), and minimize intraoperative opioid dosing |
| 4 | Postoperative phase (PACU) | Monitor block effectiveness and pain control, and observe for complications (PONV, respiratory depression, and hypotension) |
| 5 | ERAS pathway integration | Implement early oral intake and mobilization, continue multimodal analgesia regimen, and encourage physiotherapy involvement (orthopedic cases) |
| 6 | Clinical outcome | Reduced length of stay via faster recovery, minimized opioid use and side effects, improved sleep, comfort, and satisfaction, and lower postoperative complication rates |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Pain Management and Treatment · Pain Management and Opioid Use
Introduction and background
Ultrasound-guided regional anesthesia (UGRA) has revolutionized healthcare, replacing landmark and nerve-stimulation techniques. Real-time visualization of nerves with non-invasive imaging enhances block precision, safety, and success rates. It helps anesthesiologists verify needle placement and assess anesthetic dispersion, improving efficacy and reducing risks such as nerve injury and intravascular injection [1].
Ultrasound guidance has been the global standard in regional anesthesia since 2015. This has led to new techniques and uses. Its consistent outperformance of traditional methods in perioperative pain management is an important development. UGRA offers important clinical advantages over landmark and nerve-stimulator techniques, including safety, accuracy, and effectiveness [2]. Ultrasound allows for the real-time visualization of structures, puncture sites, and the distribution of anesthesia, thereby improving safety and accuracy. As UGRA is wide-ranging and rapidly evolving, covering technical methods, drug use, safety issues, and new technologies, a narrative review approach was chosen to gather current information and provide useful advice for doctors and trainees.
Review
Methodology
Literature Review, Study Selection, and Inclusion & Exclusion Criteria
This review searched six major databases, including MEDLINE (PubMed), Embase (Ovid), Cochrane Library, Web of Science, Scopus, and Google Scholar, and conducted author screening from August 2025 to October 2025. Table 1 below was adapted to highlight the literature search strategy and methodology sequence. This narrative review aims to provide a general overview of clinical and technical information on UGRA, rather than to conduct a detailed statistical analysis or a systematic review. Also, one seminal background article was added to the introduction, which does not affect the authors' inclusion dates as outlined in Table 1. No formal risk-of-bias assessment or study selection flow diagram was performed.
Quality Assessment
Each author independently screened the assigned studies, with discrepancies resolved through discussion in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA) quality assessment standards, as explained in Table 2.
Objective of the Review
This narrative review highlights the clinical applications, safety, and technical aspects of UGRA. It will cover commonly used techniques and agents in UGRA, as well as measures to reduce complications. In addition, it will discuss innovations in UGRA that may further enhance its safety and efficacy.
Fundamentals of ultrasound for regional anesthesia
Equipment & Probes: Image Optimization
Ultrasound-guided local anesthesia allows real-time needle placement and reduces complications like insufficient blockade or toxicity. Table 3 lists various types of clinical ultrasound probes, each with distinct configurations and frequencies [3].
Needle Visualization Techniques
Two primary visualization methods are in-plane and out-of-plane, as shown in Figure 1. In-plane offers a longitudinal view for accuracy, while out-of-plane positions the probe perpendicular to the needle. Probe choice and depth affect visibility. Out-of-plane suits superficial or large structures, but in-plane is preferred for precise needle-tip control to avoid vessel damage [4].
Ultrasound-guided needle visualization techniques: in-plane and out-of-plane approaches.This illustration compares the in-plane and out-of-plane ultrasound-guided needle approaches. The in-plane technique allows longitudinal visualization of the needle shaft and tip, facilitating precise needle control and improved safety. The out-of-plane technique visualizes the needle in cross-section and is commonly used for superficial or larger anatomical targets. The selection of technique depends on anatomical location, depth, and procedural requirements.Image credit: Created by the authors using BioRender (scientific illustration software).
Asepsis, Ergonomics, and Probe Handling
To prevent infections from the ultrasound probe or gel, use a disposable sleeve or alternatives such as surgical gowns, gloves, or non-lubricated condoms, which are cost-effective and accessible. The sterile cover should extend from the probe to the cable to prevent contamination. It should be sterilized after each use with a high-level disinfectant, such as ortho-phthalaldehyde, hydrogen peroxide, glutaraldehyde, or peracetic acid [5]. The anesthetist should maintain proper posture for comfort, correctly position the patient for the nerve block, and adhere to aseptic protocols to ensure patient safety. The probe is manipulated through five maneuvers: sliding, tilting, rotating, rocking, and applying pressure to improve nerve and needle visibility [6].
Pharmacology & peri-block management
Local Anesthetics: Agents, Concentration/Volume Strategies, and Toxicity Thresholds
In UGRA, selecting the appropriate local anesthetic and dose is crucial for both safety and effectiveness. Common amide anesthetics are ropivacaine, bupivacaine, and levobupivacaine, which are preferred because they last longer and are less likely to cause harm. The concentration and volume vary by block type. Hydrodissection with saline before injecting local anesthetic has been shown to accelerate the onset and spread of infraclavicular blocks [7]. Toxicity levels can vary among individuals, but it is important to stick to the maximum doses and inject slowly while checking [8]. Table 4 lists common anesthetic agents, their recommended doses for adults and children, and any reported side effects [9-12].
Adjuvants (Dexamethasone, Dexmedetomidine, Clonidine, Epinephrine): Evidence & Controversies
Adjuvants extend block duration and enhance analgesia, but their efficacy and safety differ. Table 5 lists common UGRA adjuvants with their pros and cons [13-19].
Dexamethasone is the most effective adjunct. Studies show that dexamethasone helps maintain pain relief longer with erector spinae and serratus anterior plane blocks, leading to better results. Adding dexmedetomidine to ropivacaine for an erector spinae plane block makes pain relief and recovery better, but it also raises the risk of sedation and bradycardia [17]. Clonidine, once common, has been replaced mainly by dexmedetomidine due to its weaker analgesic effects and less favorable side effect profile [18]. Epinephrine primarily narrows blood vessels, which slows its absorption and indicates that it was injected into a blood vessel; it can also extend the duration of analgesia.
Single-Shot vs. Continuous Catheters: Indications, Pump Settings, and Troubleshooting
Single-shot blocks provide reliable pain relief for short- to medium-duration procedures and are widely used for their simplicity [20]. Continuous catheter techniques provide extended analgesia, especially in shoulder and thoracic surgery, allowing the titration of local anesthetics. Infusions typically use low-concentration ropivacaine (0.1-0.2%) at 4-8 mL/hr, allowing patient-controlled boluses [21]. Programmed intermittent bolus (PIB) regimens may improve spread and analgesic quality, though the evidence remains evolving [15]. Catheter complications include dislodgement, infection, anesthetic toxicity, and technical difficulties; careful monitoring is essential.
Monitoring, Sedation, and Documentation Standards
Safe UGRA requires appropriate patient monitoring, including an electrocardiogram (ECG), pulse oximetry, and blood pressure monitoring. To keep the patient able to talk to the doctor, sedation should be kept to a minimum so that nerve irritation or systemic toxicity can be found early. Keeping a close watch on the patient after the block is crucial for spotting signs of local anesthetic systemic toxicity (LAST), with observation time based on the block's risk, and for quickly addressing any problems that arise. Documentation must capture block details, drug doses, onset time, adverse events, and analgesic outcomes to guide clinical care and quality assurance. In the context of continuous catheters, regular assessment of the catheter site and infusion parameters is essential for patient safety [21].
Safety, complications, and risk reduction
LAST: Prevention, Recognition, and Lipid Rescue Algorithm
Prevention of LAST: UGRA reduces the amount of local anesthetic needed, lowering the risk of toxicity by visualizing the needle tip and anesthetic spread [22,23]. Intravascular injection is common and causes severe LAST; real-time visualization is crucial to prevent it. Using levobupivacaine or ropivacaine, which have better cardiac safety and higher toxicity thresholds than bupivacaine, is a vital risk-reduction measure [24].
Procedural vigilance involves gentle, frequent aspiration during injection (not always reliable), administering small doses (3-5 mL) of local anesthetic with pauses to monitor the patient, and using an intravascular marker like epinephrine (1:200,000 or 5 mcg/mL) for early warning through increased heart rate [25,26]. Nerve stimulation as an adjunct provides safety; a sudden loss of motor response after a test dose can indicate intravascular placement [26].
Recognition of LAST: Early recognition of LAST is crucial for prompt treatment and preventing irreversible cardiovascular collapse. Clinicians must be vigilant for subtle prodromal signs, particularly neurological ones, such as metallic taste, perioral numbness, tinnitus, lightheadedness, or visual disturbance [27]. High suspicion is crucial during or after a local anesthetic injection. Talking with an awake patient is the best way to monitor for early detection.
Lipid rescue algorithm: The way we treat LAST has changed significantly with the use of intravenous lipid emulsion (ILE) therapy, which helps remove lipid-soluble local anesthetics from the blood and heart tissue. The American Society of Regional Anesthesia and Pain Medicine (ASRA) has formulated a definitive algorithm that must be readily accessible wherever regional blocks are administered and in cases of suspected LAST [28], as presented in Table 6.
Nerve Injury Risk, Intraneural Injection, and Monitoring Injection Pressure
Preventive efforts can lead to improved outcomes, lower post-procedure complications, and increased patient satisfaction. Table 7 outlines key aspects to consider during needle insertion and summarizes the key points for each step.
Vascular Puncture/Hematoma: Anticoagulation/Antiplatelet Considerations
Vascular puncture can be prevented by careful pre-procedural scanning and needle visualization. A thorough B-mode and color Doppler ultrasound should identify the target nerve and map nearby arteries and veins before needle insertion. Keeping the needle tip visible, preferably in-plane, is vital throughout. Hydrodissection can also help move vessels out of the needle path [7]. When aspirating blood, retract the needle and press for 5-10 minutes, then observe for an additional five minutes; this method is suitable for superficial blocks.
The management of patients on antithrombotic medications requiring regional anesthesia is complex. It must be guided by the latest societal recommendations, primarily from the ASRA and the European Society of Anaesthesiology and Intensive Care (ESAIC). The most recent guidelines emphasize a patient-specific, multidisciplinary risk-benefit analysis [33]. The key point of the guidelines is stratifying risk by block site. Superficial blocks, such as femoral, popliteal, sciatic, and transversus abdominis plane blocks, carry a much lower risk of serious [34].
Infection Prevention for Single-Shot and Catheter Techniques
Single-shot nerve blocks aim for surgical asepsis, which means the person performing the procedure must wash their hands for two minutes, wear sterile gloves, use a single-use ultrasound cover, and apply sterile gel. Continuous peripheral nerve blocks carry a higher risk of infection because they involve indwelling foreign objects. Strict aseptic standards, often with a full-body drape, are essential during insertion. A study comparing catheter-over-needle and catheter-through-needle techniques found that infection rates were the same for both. However, one design showed greater dislodgement, which can indirectly increase the risk of infection if reinsertion or site complications occur, thereby increasing the risk of contamination [35]. Post-insertion catheter care involves using sterile, transparent dressings to allow daily site checks for signs of inflammation, such as erythema, edema, or purulence. There is no proof that using peripheral nerve catheters with routine prophylactic antibiotics is advantageous. If signs of infection (local signs, fever, elevated WBC count) occur, remove the catheter, culture the tip, and initiate appropriate antibiotics. Studies on continuous blocks, like erector spinae and paravertebral catheters, show low infection rates when strict protocols are followed [36].
Pneumothorax, Diaphragmatic Paresis, and Urinary Retention Risks
Pneumothorax commonly occurs with blocks near the lung apex, like supraclavicular and paravertebral blocks. Its incidence has decreased with the use of ultrasound, enabling operators to identify the pleural line and avoid needle contact [37]. Symptoms may be immediate (such as sharp pain or cough) or delayed (including dyspnea or tachycardia). Diagnosis requires suspicion and is confirmed with a chest X-ray or ultrasound.
Hemidiaphragmatic paralysis is a common result, not a problem, of the interscalene brachial plexus block, which happens because of phrenic nerve involvement. It occurs in nearly all patients with standard volumes (>15 mL), making the block relatively contraindicated in those with severe respiratory issues who cannot tolerate approximately 25% decrease in lung capacity. Recent studies focus on mitigation strategies [38].
Urinary retention is associated with neuraxial anesthesia (spinal, epidural) due to the S2-S4 nerve block, which affects bladder function. It is rare after peripheral nerve blocks, but it can happen with extensive bilateral lower limb blocks or risk factors like benign prostatic hyperplasia. Falls are a risk after femoral or sciatic nerve blocks, particularly in outpatient surgery, due to the resulting motor weakness. Patients need education on weight-bearing, knee brace use, and clear instructions until the motor block subsides. Knowing the anatomy of each block helps prevent and manage these effects [35,39].
Quality Assurance, Incident Reporting, and Credentialing
A quality assurance program actively monitors and improves a regional anesthesia service using key performance indicators (KPIs), such as block success rates, complication rates, and patient satisfaction. These KPIs include surgical anesthesia, postoperative analgesia, LAST rate, nerve injury, infection, and block failures [29]. Periodic morbidity and mortality reviews, as well as departmental audits, review complex cases and complications in a non-punitive, educational setting, which are invaluable for collective learning and system improvement [40].
A key reactive element of a safety culture is voluntary, non-punitive incident reporting, including near-miss incidents that could have caused harm but did not due to chance or intervention. These reports reveal hidden flaws in equipment, communication, or protocols, often underlying safety issues [29].
Credentialing and privileging should ensure that clinicians performing UGRA possess the necessary skills and competencies. An integrated credentialing career map must include several steps: didactic education, which provides a basic understanding of ultrasound physics, sonic anatomy, pharmacology, and complication management; simulation-based training, which involves practical training in a non-hazardous setting with phantoms and high-fidelity simulators to develop needle skills, scan interpretation, and the treatment of rare emergencies, such as LAST; and proctored practice, in which a set number of critical blocks must be conducted with the direct oversight of a competent, experienced mentor with documented competence through various complexities [29].
Upper extremity blocks (brachial plexus & distal)
Upper-extremity blocks are highlighted in Table 8 [38-48], which illustrates the types of regional blocks and their visual landmarks (Figure 2). Descriptions and indications, technique/key anatomy, and advantages/considerations for performing UGRA per block are also provided.
Landmark for the anterior and posterior nerve blocks.Image credit: Created by the authors using BioRender (scientific illustration software).
Thoracic & truncal blocks
Thoracic and truncal blocks are outlined in Table 9 [49-56], showing the types of regional blocks. Their visual landmarks are displayed in Figure 2, along with descriptions, indications, techniques/key anatomy, and advantages or considerations for performing UGRA with each block.
Abdominal wall & pelvic blocks
Abdominal and pelvic blocks are summarized in Table 10 [57-68], which lists the types of regional blocks and their corresponding visual landmarks (Figure 2). The descriptions, indications, technique, key anatomy, and advantages or considerations for performing UGRA per block are also provided.
Lower extremity blocks
Lower-extremity blocks are highlighted in Table 11 [69-82], which illustrates the types of regional blocks and their visual landmarks, as shown in Figure 2. Descriptions and indications, technique/key anatomy, and advantages/considerations for performing UGRA per block are also provided.
Cost-effectiveness, workflow, and role within Enhanced Recovery After Surgery (ERAS) pathways across specialties
While UGRA may require additional equipment, training, and higher costs, the improved postoperative efficiency offsets these long-term expenses. Despite higher initial costs, UGRA enhances post-anesthesia care unit (PACU) throughput, reduces length of stay (LOS), and minimizes complications, resulting in broader cost benefits. A retrospective study found that ERAS protocols decreased hospital stay from 3.0 to 2.1 days (p < 0.0001) [83].
The combination of point-of-care ultrasound (POCUS) with techniques like focused assessment with sonography for trauma (FAST) has improved anesthesiology by making it possible to assess the airway, heart function, and trauma accurately. While successful outcomes depend on training, rapid detection of injury supports intervention, making POCUS essential in perioperative management [84]. These workflow and cost improvements align with ERAS protocols, which involve multiple disciplines and evidence-based approaches to optimize outcomes from preoperative to postoperative care. As shown in Table 12 [83-86], combining UGRA and POCUS with ERAS helps maintain stable clinical outcomes, improves hospital efficiency, and saves money in the long run.
Emerging technologies
Artificial Intelligence (AI)-Assisted Image Recognition and Probe Guidance
AI aids image recognition and improves nerve block teaching. A trial showed AI significantly reduced paresthesia (11 (4.12%) vs. 36 (14.06%), P = 0.000093) and injection pain (2.25% vs. 6.64%, P = 0.025). AI reduces nerve injury and boosts trainee confidence [87]. AI is an emerging topic with the potential to improve accuracy and decrease side effects.
Needle-Tracking Enhancements and Pressure-Sensing Injectables
Adding features like needle-tracking enhancers, pressure-sensing injectables, and UGRA can improve needle placement and tracking. A study showed that the catheter-over-needle (CON) method was more effective than the catheter-through-needle (CTN) method in ultrasound-guided femoral nerve blocks, reducing procedure time and leakage [88].
Robotics
UGRA could influence robotics by enabling minimally invasive procedures with fewer side effects and shorter hospital stays. One study indicated that bilateral low deep serratus anterior plane (DSAP) blocks alleviate postsurgical pain and cut opioid use after trans-subxiphoid robotic thymectomy [89]. Another study found that ultrasound transversus abdominal plane (US-TAP) wound infiltration combined with ultrasound transversus abdominal block is safe and effective for patients undergoing robotic prostatectomy and pelvic lymph node dissection [90].
Limitations of the evidence base
Despite covering UGRA, this review has limitations. As a narrative review, it lacks quantitative synthesis and a risk-of-bias assessment, thereby limiting causal inference. Though using six databases, publication and selection bias cannot be ruled out due to reliance on author judgment. Only English studies from January 2015 to October 2025 were included, potentially excluding relevant non-English or out-of-date research, thereby increasing selection bias. The review aimed to cover different clinical settings, but variability in study design, agents, and techniques affects comparability. Many studies were single-center, small, or observational and did not fully reflect real-world variability. Particularly for new technologies such as AI and robotics, there is a dearth of research on long-term outcomes, including recovery and chronic pain. Rapid tech evolution may render some conclusions outdated; future well-designed systematic reviews are needed. Furthermore, human trials involving AI, 3D/ultra-high-frequency ultrasound, Doppler technology, augmented reality, and robotics are scarce. Existing studies mainly involve cadavers or lack sufficient sample sizes to validate accuracy. The available evidence is limited by design variability, inconsistent reporting of outcomes, small sample sizes, and a focus on observational studies, all of which hinder direct comparisons and definitive conclusions.
Conclusions
UGRA has emerged as an essential component of modern perioperative management, maximizing precision, safety, and analgesic efficacy across a variety of clinical settings. This narrative review focuses on the clinical applications, pharmacological considerations, and safety issues of modern UGRA, emphasizing its role in reducing opioid consumption and improving perioperative recovery profiles. Although evidence endorses its clinical utility, variability in techniques complicates direct comparisons among interventions. Advances in ultrasound technology, education, and supplementary techniques will continue to improve clinical outcomes in UGRA. Future studies should emphasize standardized outcome measures and comparative effectiveness studies to define best practices in UGRA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ultrasound guidance in regional anesthesia: state of the art review through challenging clinical scenarios Local Reg Anesth Sites BD Antonakakis JG 114220092291586010.2147/lra.s 3444 PMC 3417939 · doi ↗ · pubmed ↗
- 2Easier and safer regional anesthesia and peripheral nerve block under ultrasound guidance Korean J Pain Jeon YH 122920162683966310.3344/kjp.2016.29.1.1PMC 4731544 · doi ↗ · pubmed ↗
- 3Ultrasound physics and instrumentation Stat Pearls Grogan SP Mount CA Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 570593/34033355 · pubmed ↗
- 4Advancements in needle visualization enhancement and localization methods in ultrasound: a literature review Art Int Surg Kimbowa A Pieters A Tadayon P 14916942024
- 5Aseptic handling of ultrasound probe: an easy solution Indian J Crit Care Med Paliwal B Bhatia P Kothari N Mohammed S 5545552020162768863510.4103/0972-5229.190373 PMC 5027752 · doi ↗ · pubmed ↗
- 6Assessing the clinical impact of emergency physician-performed ultrasound-guided peripheral nerve blocks in a level 1 trauma center: a retrospective analysis J Emerg Trauma Shock Bhoi S Gopinath B Khandelwal U 1932001720243991145910.4103/jets.jets_8_24PMC 11792750 · doi ↗ · pubmed ↗
- 7Effects of hydrodissection on anesthesia characteristics in ultrasound guided infraclavicular brachial plexus blockade Medicine (Baltimore) Er S Baskan S Akcay M Akcay F Zengin M 0101202210.1097/MD.0000000000029241 PMC 927642935687774 · doi ↗ · pubmed ↗
- 8Local anesthetic systemic toxicity CMAJ Antel R Ingelmo P 0194202210.1503/cmaj.220835 PMC 951215836162843 · doi ↗ · pubmed ↗