Rare pediatric Galeazzi lesion with progressive wrist deformity
Sarah Kerler, Johannes Fuchs, Jörg Grünert, Samuel Christen

TL;DR
A rare childhood wrist injury called Galeazzi lesion can cause long-term deformity and limited function if not diagnosed early, but corrective surgery using 3D imaging can restore function even when treatment is delayed.
Contribution
Demonstrates successful use of 3D imaging and corrective osteotomy to treat a delayed pediatric Galeazzi lesion with progressive deformity.
Findings
Undiagnosed Galeazzi injuries in childhood can lead to severe forearm rotation deficits and progressive deformity.
Multiplanar corrective osteotomy guided by 3D CT imaging significantly improved wrist function in a delayed case.
Advanced imaging enables accurate correction of complex deformities even in long-standing injuries.
Abstract
Galeazzi injuries are rare in early childhood and may be missed at initial presentation. Undiagnosed instability of the distal radioulnar joint can lead to progressive deformity and functional impairment. We report a rare case of Galeazzi injury in early childhood that led to progressive wrist malalignment during growth. Over the years this resulted in a severe restriction of forearm rotation. Using computed tomography–based three-dimensional analysis, a multiplanar corrective osteotomy was planned with reference to the contralateral healthy side. The procedure reduced the initial supination deficit of 120° to 20° and restored excellent wrist function. Missed Galeazzi injuries in early childhood can result in progressive deformity and significant long-term functional limitations. Advanced three-dimensional imaging enables accurate analysis of complex deformities and facilitates…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1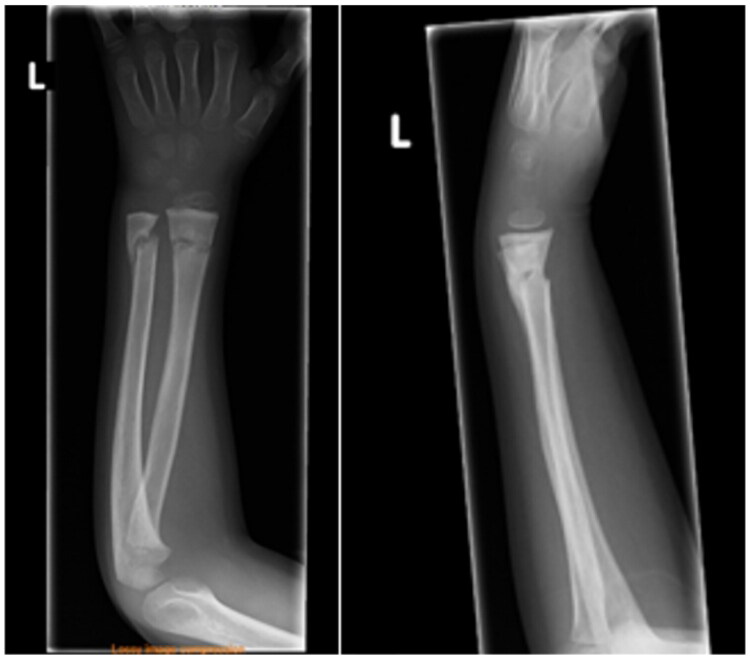 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5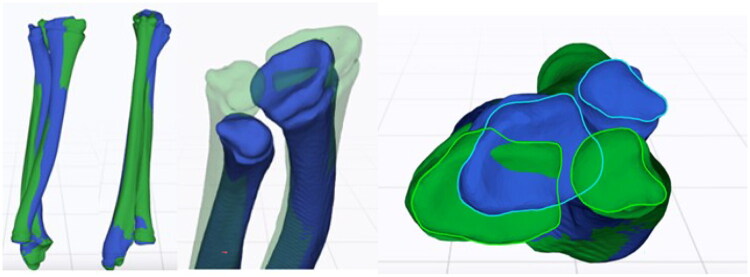 Figure 6
Figure 6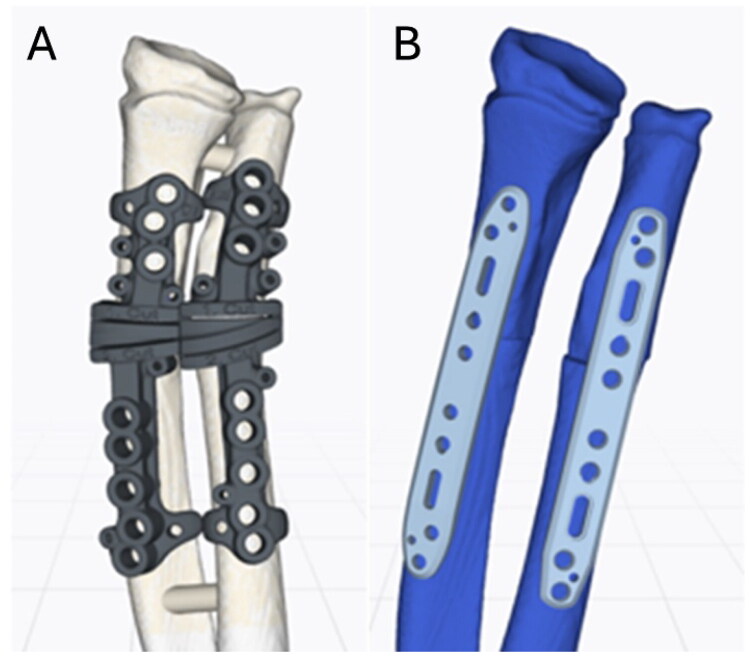 Figure 7
Figure 7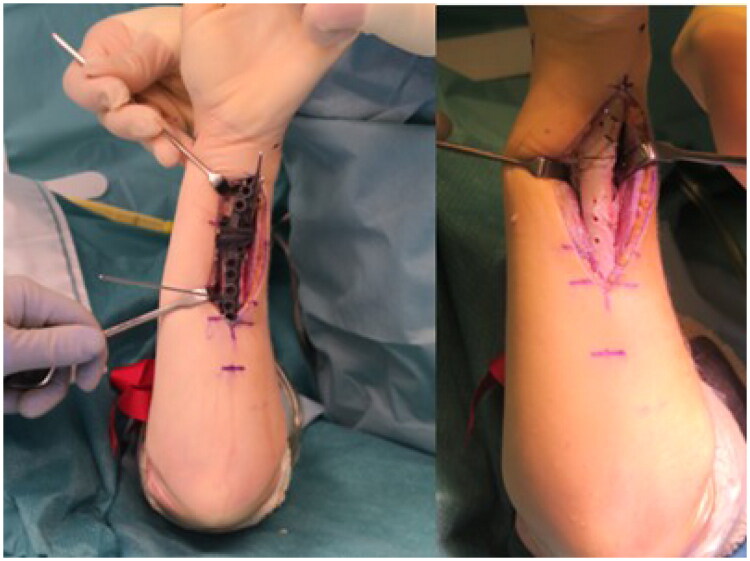 Figure 8
Figure 8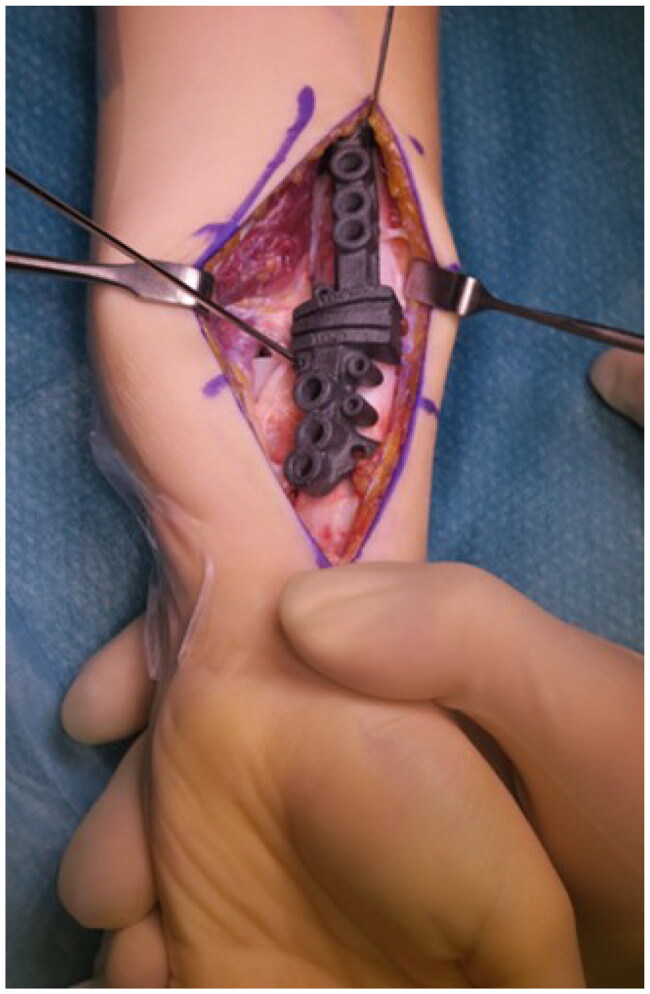 Figure 9
Figure 9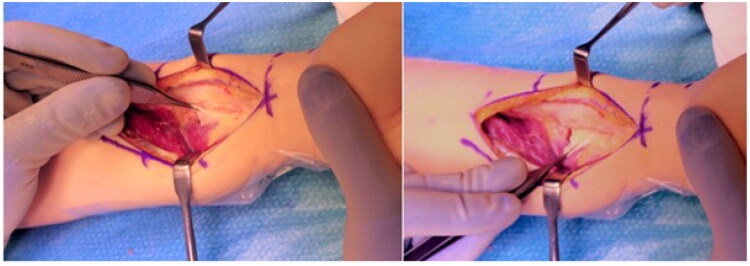 Figure 10
Figure 10 Figure 11
Figure 11Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Elbow and Forearm Trauma Treatment · Bone fractures and treatments
Introduction
In 1934, the Italian surgeon Riccardo Galeazzi first described, based on 18 cases, the biomechanics and pathology of a combined injury involving a distal third radial shaft fracture with simultaneous (typically dorsal) dislocation of the distal radioulnar joint (DRUJ) [1,2]. While the incidence of Galeazzi fractures in adults accounts for approximately 7% of all distal forearm fractures, these injuries are considerably rare in children, occurring in only 0.3–2.8% of the cases [3–6]. The relatively high elasticity and tensile strength of ligamentous structures generally protect the pediatric wrist from dislocations in general. The so-called Galeazzi-equivalent injury, which combines a distal radius fracture with severely displaced distal ulnar epiphysiolysis, is slightly more common in children [2,6–8]. Ulnar dislocation with distal metaphyseal fractures of both bones is extremely rare and reported only in isolated pediatric cases [5,9,10].
Patients/materials and methods
A 12-year-old boy presented to our pediatric hand surgery clinic with progressive restriction of forearm rotation of his left wrist following an injury in early childhood.
At the age of 4, he suffered a severely displaced distal forearm fracture of the left arm after a fall from 3 meters (Figure 1). The fracture was initially managed at an external hospital with closed reduction and immobilization in an elbow cast for 4 weeks, followed by a forearm cast for an additional 2 weeks. Radiological follow-up at 4 weeks demonstrated only a slight dorsal tilt of the ulna (Figure 2).
X-rays before (A) and after (B) closed reduction of the fully displaced forearm fracture.
X-ray follow-up 4 weeks after trauma.
At 24-month follow-up, a supination deficit of 45° was documented, while pronation remained unrestricted. Conventional radiographs revealed progressive dorsal angulation of the ulna with subluxation of the distal radioulnar joint (DRUJ) (Figure 3). As the patient was asymptomatic and spontaneous correction during growth was expected, a watchful waiting strategy was adopted.
2-year follow-up showing a progressive dorsal angulation and subluxation of the distal ulna.
Over the years, the motion restriction progressively worsened. Due to increasing limitations in daily activities and the patient’s desire to pursue a manual profession, he presented to our pediatric hand surgery clinic for a second opinion. Wrist supination was now limited to −30° (total deficit of 120°), while at the same time a hyperpronation of +20° could be observed. Furthermore, wrist flexion was restricted by 20° (Figure 4). Conventional radiographs revealed marked dorsal angulation of the distal ulna with DRUJ dislocation (Figure 5).
Clinical finding at initial presentation in our outpatient clinic 8 years after trauma. Range of motion: Pronation-Supination 90°-0°-90° (right) vs. 110°–30°–0° (left), Flexion-Extension 80°-0°-80° (right) vs. 60°-0°-80° (left).
X-ray 8 years after injury showing marked angulation of both forearm bones and dorsal dislocation of the ulna in the DRUJ.
Comparative 3D analysis using computed tomography of both forearms revealed multidirectional deformities of the distal third of both radius and ulna (Figure 6). A multiplanar corrective osteotomy of both bones was planned using the CMX system (Medartis AG, Basel, Switzerland) with patient-specific surgical guides (Figure 7).
Three-dimensional analysis and surgical planning (Medartis AG, Basel, Switzerland), blue: affected side, green: mirrored contralateral side.
Preoperative planning of patient-specific drilling and cutting guides (A), and osteosynthesis with standard plate fixation in corrected alignment (B).
Surgical technique
Given the inability to supinate the forearm, the ulnar osteotomy was performed as the first step after predrilling the screw holes according to the guide (Figure 8). Afterwards the forearm could be repositioned to allow access to the distal radius via a modified Henry approach. For guide placement, the flexor pollicis longus muscle had to be detached from the radial shaft.
Guide positioning on the ulna using K-wire fixation (A). Predrilled screw holes and wedge osteotomy after removal of the guide (B).
Following the wedge osteotomy of the radius both bones were reduced and osteosynthesized with standard forearm shaft plates (Radius Ulna Shaft System 2.8, Medartis AG, Basel, Switzerland). The reduction was obtained by means of the screw hole placement defined by the guide, consistent with the preoperative planning ([Figures 7, 8, 9](#F0007 F0008 F0009)).
Positioning and temporary fixation of the radial guide after exposure of the bony references.
After bony correction, supination remained limited to 0°, prompting an additional soft-tissue release. In the distal third of the shaft, a thick fibrous scar formation of the interosseous membrane could be identified. In addition, the pronator quadratus muscle had been replaced by scarred residue (Figure 10). After excision of the scar tissue and further soft-tissue release, supination improved to +40° (Figure 11). An above-elbow plaster splint was applied with the forearm positioned in maximal supination.
Pronounced thick scarring of the distal interosseous membrane and the pronator quadratus muscle residue.
Postoperative result showing an achieved supination of 40° (in redressing cast).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Galeazzi R. Über ein besonderes Syndrom bei Verletzungen im Bereich der Umeramnknochen [On a special syndrome in injuries of the forearm bones]. Arch Orthop Trauma Surg. 1935;35:557–562.
- 2Sebastin SJ, Chung KC. A historical report on Riccardo Galeazzi and the management of Galeazzi fractures. J Hand Surg Am. 2010;35(11):1870–1877. doi: 10.1016/j.jhsa.2010.08.032.21050967 PMC 4411960 · doi ↗ · pubmed ↗
- 3Alajmi T. Galeazzi fracture dislocations: an illustrated review. Cureus. 2020;12(7):e 9367. doi: 10.7759/cureus.9367.32850236 PMC 7444983 · doi ↗ · pubmed ↗
- 4Walsh HP, Mc Laren CA, Owen R. Galeazzi fractures in children. J Bone Joint Surg Br. 1987;69(5):730–733. doi: 10.1302/0301-620X.69B 5.3680332.3680332 · doi ↗ · pubmed ↗
- 5Eberl R, Singer G, Schalamon J, et al. Galeazzi lesions in children and adolescents: treatment and outcome. Clin Orthop Relat Res. 2008;466(7):1705–1709. doi: 10.1007/s 11999-008-0268-6.18443894 PMC 2505249 · doi ↗ · pubmed ↗
- 6Little JT, Klionsky NB, Chaturvedi A, et al. Pediatric distal forearm and wrist injury: an imaging review. Radiographics. 2014;34(2):472–490. doi: 10.1148/rg.342135073.24617692 · doi ↗ · pubmed ↗
- 7Letts M, Rowhani N. Galeazzi-equivalent injuries of the wrist in children. J Pediatr Orthop. 1993;13(5):561–566. doi: 10.1097/01241398-199313050-00001.8376552 · doi ↗ · pubmed ↗
- 8Chae SB, Kwon JB. Pronation type Galeazzi-equivalent fracture: a rare case report (CARE-compliant). Medicine (Baltimore). 2019;98(52):e 18429. doi: 10.1097/MD.0000000000018429.31876721 PMC 6946214 · doi ↗ · pubmed ↗